
Relationship between Patient Preferences, Attitudes to Treatment, Adherence, and Quality of Life in New Users of Teriflunomide

 ,
,
Abstract
:1. Introduction
2. Results
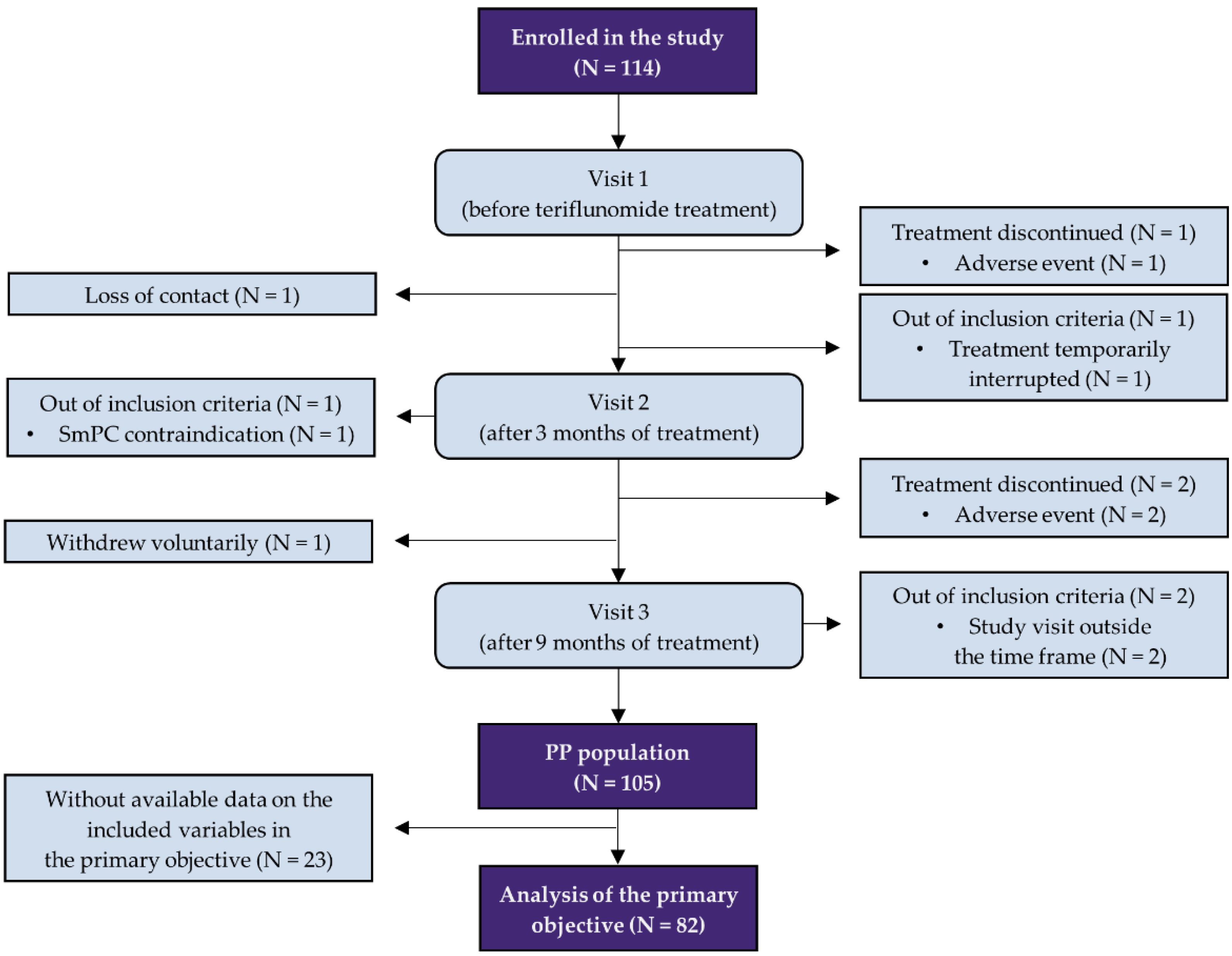
2.1. Primary Objective
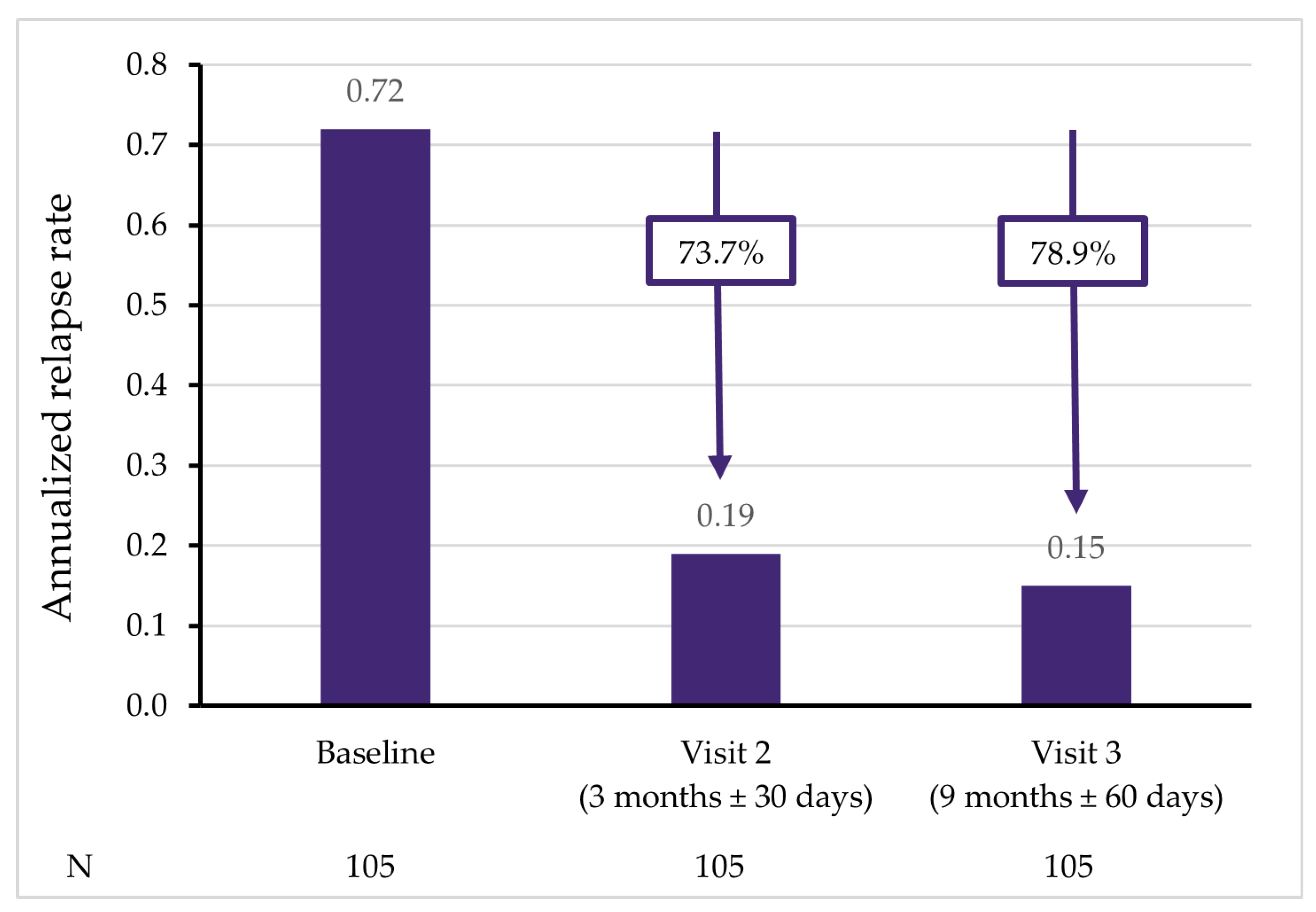
2.2. Disease Activity and Disability
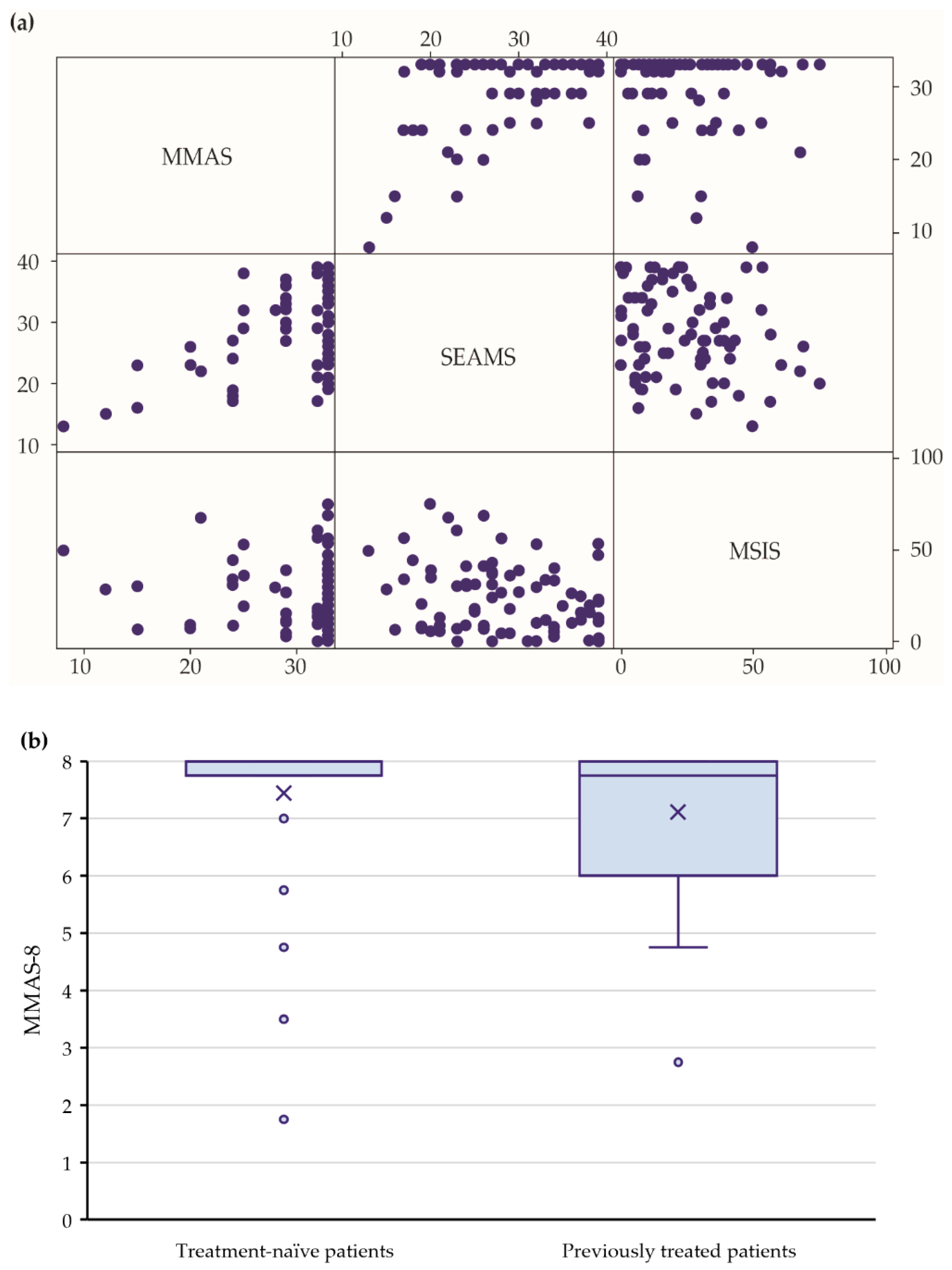
2.3. Quality of Life and Adherence
2.4. Attitudes toward Treatment and Preferences
2.5. Safety
3. Discussion
4. Materials and Methods
4.1. Study Design and Standards
4.2. Subject Eligibility
4.3. Parameters
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wallin, M.T.; Culpepper, W.J.; Nichols, E.; Bhutta, Z.A.; Gebrehiwot, T.T.; Hay, S.I.; Khalil, I.A.; Krohn, K.J.; Liang, X.; Naghavi, M.; et al. Global, regional, and national burden of multiple sclerosis 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 269–285. [Google Scholar] [CrossRef] [Green Version]
- Simpson, S.; Blizzard, L.; Otahal, P.; Van der Mei, I.; Taylor, B. Latitude is significantly associated with the prevalence of multiple sclerosis: A meta-analysis. J. Neurol. Neurosurg. Psychiatry 2011, 82, 1132–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, D.; Zhang, C.; Zhao, X.; Zhang, Y.; Dai, Q.; Li, Y.; Chu, L. Teriflunomide for multiple sclerosis. Cochrane Database Syst. Rev. 2016, 3, 8. Available online: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD009882.pub3/full (accessed on 7 December 2021). [CrossRef] [PubMed]
- Nicholas, J.A.; Edwards, N.C.; Edwards, R.A.; Dellarole, A.; Grosso, M.; Phillips, A.L. Real-world adherence to, and persistence with, once- and twice-daily oral disease-modifying drugs in patients with multiple sclerosis: A systematic review and meta-analysis. BMC Neurol. 2020, 20, 281. [Google Scholar] [CrossRef] [PubMed]
- Munsell, M.; Frean, M.; Menzin, J.; Phillips, A.L. An evaluation of adherence in patients with multiple sclerosis newly initiating treatment with a self-injectable or an oral disease-modifying drug. Patient Prefer. Adherence 2016, 11, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Zhou, T.; Guan, H.; Wang, L.; Zhang, Y.; Rui, M.; Ma, A. Health-Related Quality of Life in Patients With Different Diseases Measured With the EQ-5D-5L: A Systematic Review. Front. Public Health 2021, 9, 675523. [Google Scholar] [CrossRef]
- Aubagio European Public Assessment Report EMEA/H/002514-IG1386, Updated 27/08/2021. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/aubagio (accessed on 7 December 2021).
- Vermersch, P.; Czlonkowska, A.; Grimaldi, L.M.; Confavreux, C.; Comi, G.; Kappos, L.; Olsson, T.P.; Benamor, M.; Bauer, D.; Truffinet, P.; et al. Teriflunomide versus subcutaneous interferon beta-1a in patients with relapsing multiple sclerosis: A randomised, controlled phase 3 trial. Mult. Scler. J. 2014, 20, 705–716. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, P.; Wolinsky, J.S.; Confavreux, C.; Comi, G.; Kappos, L.; Olsson, T.P.; Benzerdjeb, H.; Truffinet, P.; Wang, L.; Miller, A.; et al. Randomized trial of oral teriflunomide for relapsing multiple sclerosis. N. Engl. J. Med. 2011, 365, 1293–1303. [Google Scholar] [CrossRef] [Green Version]
- Confavreux, C.; O’Connor, P.; Comi, G.; Freedman, M.S.; Miller, A.E.; Olsson, T.P.; Wolinsky, J.S.; Bagulho, T.; Delhay, J.-L.; Dukovic, D.; et al. Oral teriflunomide for patients with relapsing multiple sclerosis (TOWER): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol. 2014, 13, 247–256. [Google Scholar] [CrossRef]
- Miller, A.E.; Wolinsky, J.S.; Kappos, L.; Comi, G.; Freedman, M.S.; Olsson, T.P.; Bauer, D.; Benamor, M.; Truffinet, P.; O’Connor, P.W.; et al. Oral teriflunomide for patients with a first clinical episode suggestive of multiple sclerosis (TOPIC): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol. 2014, 13, 977–986. [Google Scholar] [CrossRef]
- Bayas, A.; Mäurer, M. Teriflunomide for the treatment of relapsing–remitting multiple sclerosis: Patient preference and adherence. Patient Prefer. Adherence 2015, 9, 265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visser, L.A.; Louapre, C.; Uyl-de Groot, C.A.; Redekop, W.K. Patient needs and preferences in relapsing-remitting multiple sclerosis: A systematic review. Mult. Scler. Relat. Disord. 2020, 39, 101929. [Google Scholar] [CrossRef] [PubMed]
- Vermersch, P.; Suchet, L.; Colamarino, R.; Laurendeau, C.; Detournay, B. An analysis of first-line disease-modifying therapies in patients with relapsing-remitting multiple sclerosis using the French nationwide health claims database from 2014–2017. Mult. Scler. Relat. Disord. 2020, 46, 102521. [Google Scholar] [CrossRef] [PubMed]
- Lahdenperä, S.; Soilu-Hänninen, M.; Kuusisto, H.; Atula, S.; Junnila, J.; Berglund, A. Medication adherence/persistence among patients with active multiple sclerosis in Finland. Acta Neurol. Scand. 2020, 142, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Prosperini, L.; Cortese, A.; Lucchini, M.; Boffa, L.; Borriello, G.; Buscarinu, M.C.; Capone, F.; Centonze, D.; De Fino, C.; De Pascalis, D.; et al. Exit strategies for “needle fatigue” in multiple sclerosis: A propensity score-matched comparison study. J. Neurol. 2020, 267, 694–702. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Liao, Q.; Wen, H.; Zhang, Y. Disease modifying therapies in relapsing-remitting multiple sclerosis: A systematic review and network meta-analysis. Autoimmun. Rev. 2021, 20, 102826. [Google Scholar] [CrossRef]
- Buron, M.D.; Chalmer, T.A.; Sellebjerg, F.; Frederiksen, J.; Góra, M.K.; Illes, Z.; Kant, M.; Mezei, Z.; Petersen, T.; Rasmussen, P.V.; et al. Comparative effectiveness of teriflunomide and dimethyl fumarate: A nationwide cohort study. Neurology 2019, 92, e1811–e1820. [Google Scholar] [CrossRef]
- Kalincik, T.; Havrdova, E.K.; Horakova, D.; Izquierdo, G.; Prat, A.; Girard, M.; Duquette, P.; Grammond, P.; Onofrj, M.; Lugaresi, A.; et al. Comparison of fingolimod, dimethyl fumarate and teriflunomide for multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2019, 90, 458–468. [Google Scholar] [CrossRef] [Green Version]
- Hillert, J.; Tsai, J.A.; Nouhi, M.; Glaser, A.; Spelman, T. A comparative study of teriflunomide and dimethyl fumarate within the Swedish MS Registry. Mult. Scler. 2022, 28, 13524585211019648. [Google Scholar] [CrossRef]
- de Sèze, J.; Devy, R.; Planque, E.; Delabrousse-Mayoux, J.P.; Vandhuick, O.; Kabir, M.; Gherib, A. Fatigue in teriflunomide-treated patients with relapsing remitting multiple sclerosis in the real-world Teri-FAST study. Mult. Scler. Relat. Disord. 2021, 47, 102659. [Google Scholar] [CrossRef]
- Nazareth, T.; Friedman, H.S.; Navaratnam, P.; Herriott, D.A.; Ko, J.J.; Barr, P.; Sasane, R. Persistency, medication prescribing patterns, and medical resource use associated with multiple sclerosis patients receiving oral disease-modifying therapies: A retrospective medical record review. BMC Neurol. 2016, 16, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermersch, P.; Oh, J.; Cascione, M.; Oreja-Guevara, C.; Gobbi, C.; Travis, L.H.; Myhr, K.-M.; Coyle, P.K. Teriflunomide vs injectable disease modifying therapies for relapsing forms of MS. Mult. Scler. Relat. Disord. 2020, 43, 102158. [Google Scholar] [CrossRef] [PubMed]
- Pust, G.E.A.; Untiedt, B.; Weierstall-Pust, R.; Randerath, J.; Barabasch, A.; Rahn, A.C.; Heesen, C. Medication beliefs in first-line and second-line treated multiple sclerosis patients. Mult. Scler. Relat. Disord. 2020, 42, 102144. [Google Scholar] [CrossRef] [PubMed]
- Yoon, E.L.; Cheong, W.L. Adherence to oral disease-modifying therapy in multiple sclerosis patients: A systematic review. Mult. Scler. Relat. Disord. 2019, 28, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Kołtuniuk, A.; Chojdak-Łukasiewicz, J. Adherence to Therapy in Patients with Multiple Sclerosis—Review. Int. J. Environ. Res. Public. Health 2022, 19, 2203. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Hobart, J.; Lamping, D.; Fitzpatrick, R.; Riazi, A.; Thompson, A. The Multiple Sclerosis Impact Scale (MSIS-29): A new patient-based outcome measure. Brain 2001, 124, 962–973. [Google Scholar] [CrossRef]
- De las Cuevas, C.; Peñate, W. Psychometric properties of the eight-item Morisky Medication Adherence Scale (MMAS-8) in a psychiatric outpatient setting. Int. J. Clin. Health Psychol. IJCHP 2015, 15, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Risser, J.; Jacobson, T.A.; Kripalani, S. Development and psychometric evaluation of the Self-efficacy for Appropriate Medication Use Scale (SEAMS) in low-literacy patients with chronic disease. J. Nurs. Meas. 2007, 15, 203–219. [Google Scholar] [CrossRef]
- Svarstad, B.L.; Chewning, B.A.; Sleath, B.L.; Claesson, C. The Brief Medication Questionnaire: A tool for screening patient adherence and barriers to adherence. Patient Educ. Couns. 1999, 37, 113–124. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Mean (±SD)/Number (%) |
|---|---|
| Number of patients | 105 |
| Female | 59 (56.2%) |
| Age (years) | 41.2 (±10.6) |
| Diagnosis of CIS | 68 (64.8%) |
| Diagnosis of RRMS | 37 (35.2%) |
| Time from diagnosis (years) | 3.5 (±5.5) |
| Time from diagnosis for previously treated patients (years) 1 | 7.2 (±6.1) |
| Time from diagnosis for DMT-naïve patients (years) 1 | 0.2 (±0.2) |
| DMT-naïve patients | 55 (52.4%) |
| One previous DMT | 37 (35.2%) |
| Two or more previous DMTs | 13 (12.4%) |
| Duration of previous treatment (years) 2 | 3.8 (±4.5) |
| Baseline BMI | 25.1 (±4.4) |
| MMAS-8 [Decreasing] 1 | Unadjusted 2 | Adjusted 2 | |||
|---|---|---|---|---|---|
| OR (95% CI) 3 | p-Value 3 | OR (95% CI) 3 | p-Value 3 | ||
| SEAMS [pointwise] 1 | 0.93 (0.87–0.99) | 0.026 | 0.92 (0.86–0.99) | 0.032 |  |
| BMQ [ambivalent] 1,4 | 1.90 (0.73–4.97) | 0.190 | 1.95 (0.61–6.18) | 0.259 | |
| BMQ [indifferent & skeptical] 1 | 2.31 (0.45–12.00) | 0.318 | 2.05 (0.33–12.54) | 0.439 | |
| MSIS-29 total [pointwise] 1 | 1.01 (0.98–1.03) | 0.668 | 0.98 (0.95–1.02) | 0.344 | |
| Sex [female] | 0.77 (0.32–1.82) | 0.547 | 0.61 (0.21–1.82) | 0.378 | |
| Previous DMT [yes] | 3.21 (1.30–7.91) | 0.011 | 4.66 (1.67–13.04) | 0.003 | |
| Difference of EDSS [pointwise] 1 | 1.27 (0.67–2.41) | 0.465 | 1.93 (0.88–4.21) | 0.100 | |
| Clinical Outcomes 2 | Baseline | Visit 2 | Visit 3 |
|---|---|---|---|
| Mean Length of Follow-Up | Teriflunomide Initiation | 2.9 ± 0.25 months | 8.8 ± 0.5 months |
| Number of patients with at least 1 relapse (%) | 66 (62.9%) | 4 (3.8%) | 8 (7.6%) |
| Number of patients hospitalized for relapse (%) | 31 (29.5%) | 0 (0.0%) | 1 (1.0%) |
| ARR | 0.72 (0.57–0.91) | 0.19 (0.12–0.29) | 0.15 (0.09–0.25) |
| ARR relative decrease | - | 73.7% | 78.9% |
| EDSS | 1.97 (±0.99) | 1.97 (±1.04) | 2.03 (±0.99) |
| MSIS-29 3 | 26.62 (±20.40) | 25.58 (±20.10) | 25.49 (±19.88) |
| MMAS-8 3 | - | 7.61 (±0.82) | 7.39 (±1.22) |
| VAS 3 | - | 96.21 (±14.52) | 95.60 (±14.22) |
| SEAMS 3 | - | - | 28.53 (±7.20) |
| BMQ accepting 3 | - | - | 60 (60.6%) |
| BMQ ambivalent 3 | - | - | 31 (31.3%) |
| BMQ indifferent 3 | - | - | 6 (6.1%) |
| BMQ skeptical 3 | - | - | 2 (2.0%) |
| Patient preferences (oral dosage) 3 | 101 (98.1%) | 104 (100.0%) | 104 (100.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Štrosová, D.; Tužil, J.; Turková, B.V.; Pilnáčková, B.F.; de Souza, L.L.; Doležalová, H.; Rašková, M.; Dufek, M.; Doležal, T. Relationship between Patient Preferences, Attitudes to Treatment, Adherence, and Quality of Life in New Users of Teriflunomide. Pharmaceuticals 2022, 15, 1248. https://doi.org/10.3390/ph15101248
Štrosová D, Tužil J, Turková BV, Pilnáčková BF, de Souza LL, Doležalová H, Rašková M, Dufek M, Doležal T. Relationship between Patient Preferences, Attitudes to Treatment, Adherence, and Quality of Life in New Users of Teriflunomide. Pharmaceuticals. 2022; 15(10):1248. https://doi.org/10.3390/ph15101248
Chicago/Turabian StyleŠtrosová, Daniela, Jan Tužil, Barbora Velacková Turková, Barbora Filková Pilnáčková, Lada Lžičařová de Souza, Helena Doležalová, Michaela Rašková, Michal Dufek, and Tomáš Doležal. 2022. "Relationship between Patient Preferences, Attitudes to Treatment, Adherence, and Quality of Life in New Users of Teriflunomide" Pharmaceuticals 15, no. 10: 1248. https://doi.org/10.3390/ph15101248