
Incident Type 2 Diabetes Risk of Selective Estrogen Receptor Modulators in Female Patients with Breast Cancer


Abstract
:1. Introduction
2. Results
2.1. Characteristics of Study Patients
2.2. Study Outcomes: SERM Users Versus Non-Users
2.3. T2DM Risk per SERM Agent and Treatment Duration
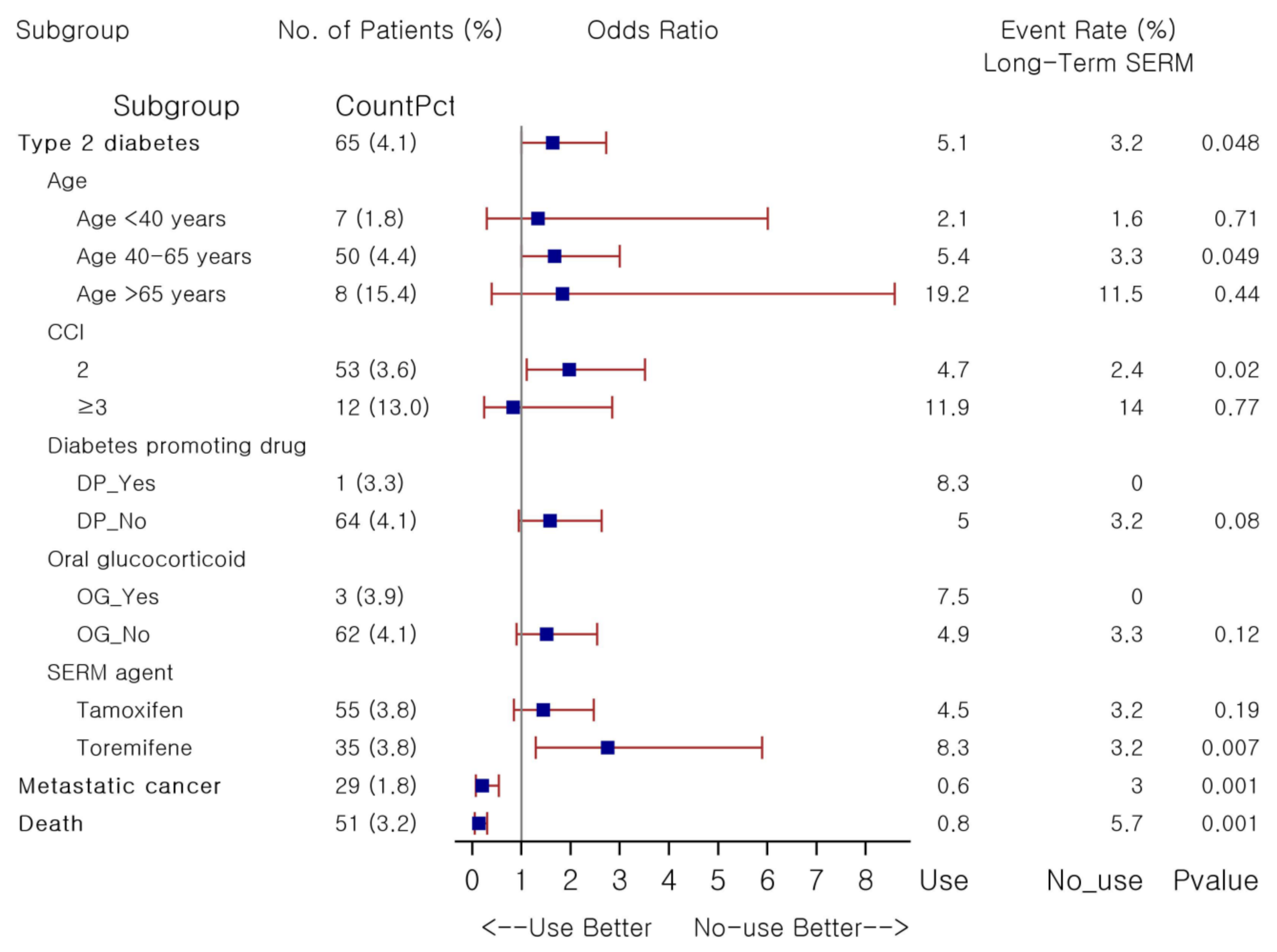
2.4. T2DM Risk with Long-Term Use of SERM
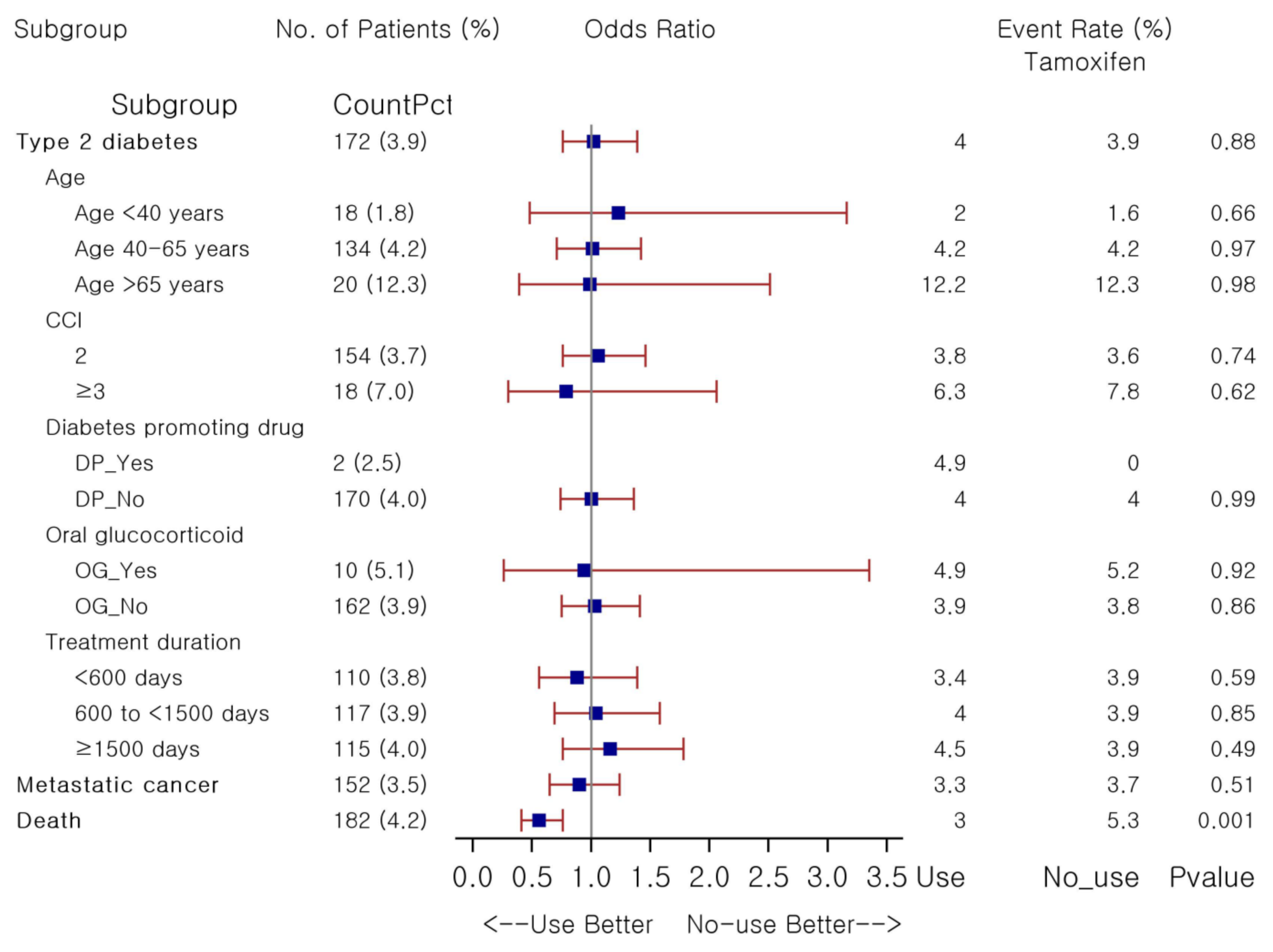
2.5. T2DM Risk with Tamoxifen
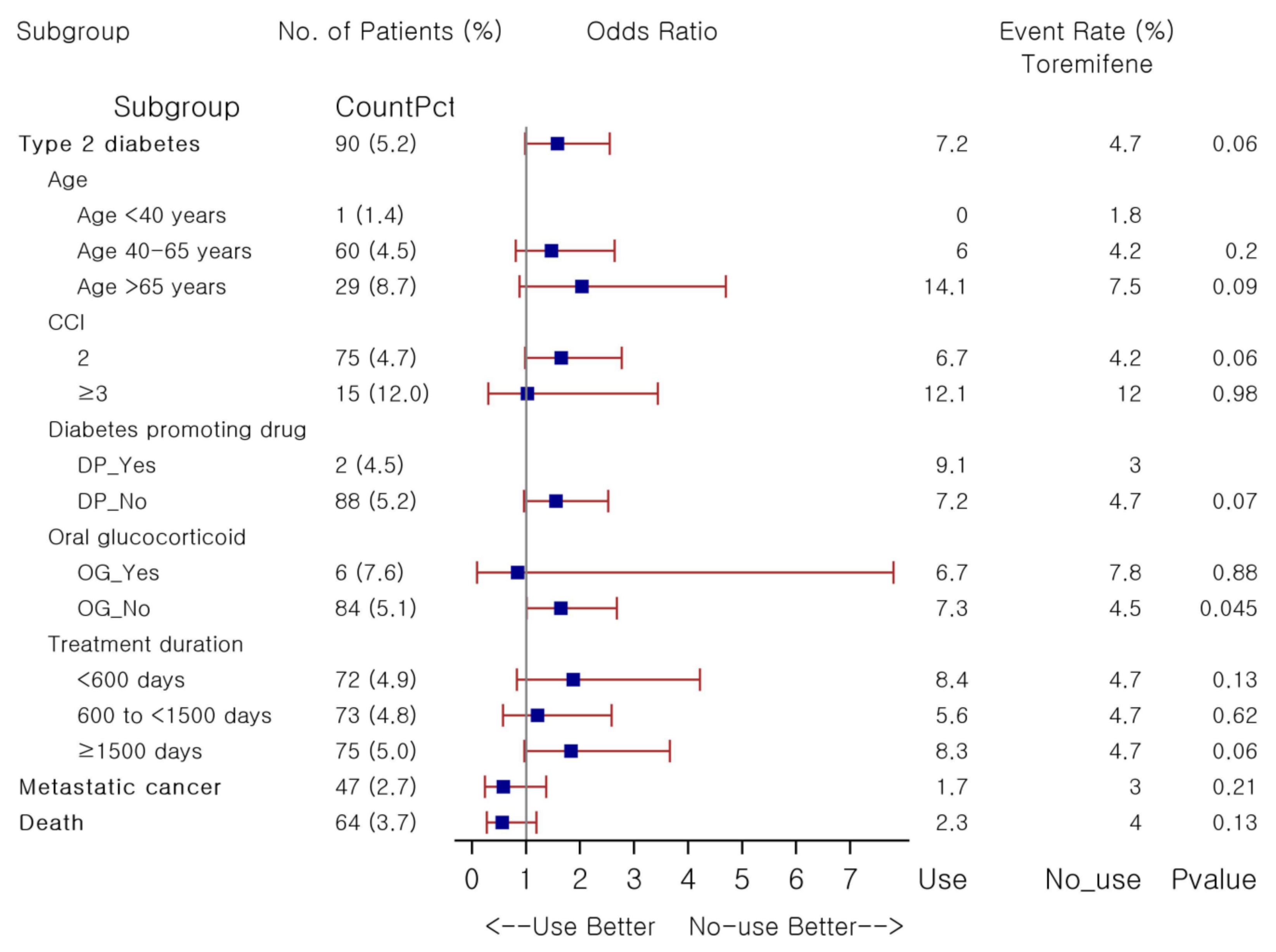
2.6. T2DM Risk with Toremifene
3. Discussion
4. Materials and Methods
4.1. Study Design and Cohort
4.2. Study Medications and Variables
4.3. Study Outcomes
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Redaniel, M.T.; Jeffreys, M.; May, M.T.; Ben-Shlomo, Y.; Martin, R.M. Associations of type 2 diabetes and diabetes treatment with breast cancer risk and mortality: A population-based cohort study among British women. Cancer Causes Control 2012, 23, 1785–1795. [Google Scholar] [CrossRef]
- Peairs, K.S.; Barone, B.B.; Snyder, C.F.; Yeh, H.-C.; Stein, K.B.; Derr, R.L.; Brancati, F.L.; Wolff, A. Diabetes Mellitus and Breast Cancer Outcomes: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2011, 29, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Noh, Y.; Jeon, S.-M.; Shin, S. Association between glucose-lowering treatment and cancer metastasis among patients with preexisting type 2 diabetes and incident malignancy. Int. J. Cancer 2019, 144, 1530–1539. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Kim, D.J.; Shin, S. Incident cancer risk in dipeptidyl peptidase-4 inhibitor-treated patients with type 2 diabetes mellitus. Cancer Manag. Res. 2019, 11, 7427–7438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipscombe, L.L.; Goodwin, P.J.; Zinman, B.; McLaughlin, J.R.; Hux, J.E. Increased prevalence of prior breast cancer in women with newly diagnosed diabetes. Breast Cancer Res. Treat. 2006, 98, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Bordeleau, L.; Lipscombe, L.; Lubinski, J.; Ghadirian, P.; Foulkes, W.; Neuhausen, S.; Ainsworth, P.; Pollak, M.; Sun, P.; Narod, S.A.; et al. Diabetes and breast cancer among women with BRCA1 and BRCA2 mutations. Cancer 2011, 117, 1812–1818. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund & American Institute for Cancer Research. Worldwide Cancer Data. Available online: https://www.wcrf.org/dietandcancer/worldwide-cancer-data/ (accessed on 28 June 2021).
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef]
- Loibl, S.; Poortmans, P.; Morrow, M.; Denkert, C.; Curigliano, G. Breast cancer. Lancet 2021, 397, 1750–1769. [Google Scholar] [CrossRef]
- Giordano, S.H.; Buzdar, A.U.; Smith, T.L.; Kau, S.-W.; Yang, Y.; Hortobagyi, G.N. Is breast cancer survival improving? Cancer 2004, 100, 44–52. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology. Breast Cancer Version 5.2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 2 July 2021).
- Mirkin, S.; Pickar, J.H. Selective estrogen receptor modulators (SERMs): A review of clinical data. Maturitas 2015, 80, 52–57. [Google Scholar] [CrossRef]
- Lipscombe, L.L.; Fischer, H.D.; Yun, L.; Gruneir, A.; Austin, P.; Paszat, L.; Anderson, G.M.; Rochon, P.A. Association between tamoxifen treatment and diabetes: A population-based study. Cancer 2012, 118, 2615–2622. [Google Scholar] [CrossRef]
- Yan, H.; Yang, W.; Zhou, F.; Li, X.; Pan, Q.; Shen, Z.; Han, G.; Newell-Fugate, A.; Tian, Y.; Mejeti, R.; et al. Estrogen Improves Insulin Sensitivity and Suppresses Gluconeo-genesis via the Transcription Factor Foxo1. Diabetes 2019, 68, 291–304. [Google Scholar] [CrossRef] [Green Version]
- Nadal, A.; Alonso-Magdalena, P.; Soriano, S.; Quesada, I.; Ropero, A.B. The pancreatic beta-cell as a target of estrogens and xenoestrogens: Implications for blood glucose homeostasis and diabetes. Mol. Cell. Endocrinol. 2009, 304, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauvais-Jarvis, F.; Manson, J.E.; Stevenson, J.C.; Fonseca, V.A. Menopausal Hormone Therapy and Type 2 Diabetes Preven-tion: Evidence, Mechanisms, and Clinical Implications. Endocr. Rev. 2017, 38, 173–188. [Google Scholar] [CrossRef] [Green Version]
- Lima, M.T.M.; De Carvalho, K.P.; Mazzutti, F.S.; de Almeida Maia, M.; Canto, P.P.L.; Paiva, C.E.; Maia, Y.C.D.P. Temporal influence of endocrine therapy with tamoxifen and chemotherapy on nutritional risk and obesity in breast cancer patients. BMC Cancer 2017, 17, 578. [Google Scholar] [CrossRef] [PubMed]
- Kharroubi, A.T.; Darwish, H.M. Diabetes mellitus: The epidemic of the century. World J. Diabetes 2015, 6, 850–867. [Google Scholar] [CrossRef]
- Clemons, M.; Danson, S.; Howell, A. Tamoxifen (‘Nolvadex’): A review. Cancer Treat. Rev. 2002, 28, 165–180. [Google Scholar] [CrossRef]
- Bae, S.Y.; Kim, S.; Lee, J.H.; Lee, H.-C.; Lee, S.K.; Kil, W.H.; Kim, S.W.; Lee, J.E.; Nam, S.J. Poor prognosis of single hormone receptor- positive breast cancer: Similar outcome as triple-negative breast cancer. BMC Cancer 2015, 15, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vigneri, P.; Frasca, F.; Sciacca, L.; Pandini, G.; Vigneri, R. Diabetes and cancer. Endocr.-Relat. Cancer 2009, 16, 1103–1123. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, T.A. Diabetes and cancer. QJM Int. J. Med. 2010, 103, 905–915. [Google Scholar] [CrossRef] [Green Version]
- De Bruijn, K.M.; Arends, L.R.; Hansen, B.; Leeflang, S.; Ruiter, R.; van Eijck, C.H. Systematic review and meta-analysis of the association between diabetes mellitus and incidence and mortality in breast and colorectal cancer. BJS 2013, 100, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Shao, S.; Gill, A.A.; Zahm, S.H.; Jatoi, I.; Shriver, C.D.; McGlynn, K.A.; Zhu, K. Diabetes and Overall Survival among Breast Cancer Patients in the U.S. Military Health System. Cancer Epidemiol. Biomark. Prev. 2017, 27, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szmuilowicz, E.; Stuenkel, C.A.; Seely, E.W. Influence of menopause on diabetes and diabetes risk. Nat. Rev. Endocrinol. 2009, 5, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Chlebowski, R.T.; Shi, J.; Barac, A.; Haque, R. Aromatase inhibitor and tamoxifen use and the risk of venous throm-boembolism in breast cancer survivors. Breast Cancer Res. Treat. 2019, 174, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Mustonen, M.V.; Pyrhonen, S.; Kellokumpu-Lehtinen, P.L. Toremifene in the treatment of breast cancer. World J. Clin. Oncol. 2014, 5, 393–405. [Google Scholar] [CrossRef]
- Hong, J.; Huang, J.; Shen, L.; Zhu, S.; Gao, W.; Wu, J.; Huang, O.; He, J.; Zhu, L.; Chen, W.; et al. A prospective, randomized study of Toremifene vs. tamoxifen for the treatment of premenopausal breast cancer: Safety and genital symptom analysis. BMC Cancer 2020, 20, 663. [Google Scholar] [CrossRef]
- Gu, R.; Jia, W.; Zeng, Y.; Rao, N.; Hu, Y.; Li, S.; Wu, J.; Jin, L.; Chen, L.; Long, M.; et al. A comparison of survival outcomes and side effects of toremifene or tamoxifen therapy in premenopausal estrogen and progesterone receptor positive breast cancer patients: A retrospective cohort study. BMC Cancer 2012, 12, 161. [Google Scholar] [CrossRef] [Green Version]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG); Davies, C.; Godwin, J.; Gray, R.; Clarke, M.; Cutter, D.; Darby, S.; McGale, P.; Pan, H.C.; Taylor, C.; et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: Patient-level meta-analysis of randomised trials. Lancet 2011, 378, 771–784. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | SERM Use (n = 2522) | Non-Use (n = 2522) | p-Value |
|---|---|---|---|
| Age (years), mean ± SD | 46.2 ± 9.7 | 49.2 ± 10.8 | |
| <40 | 510 (20.2) | 509 (20.2) | 1.00 |
| 40–65 | 1866 (74.0) | 1867 (74.0) | |
| >65 | 146 (5.8) | 146 (5.8) | |
| CCI, mean ± SD | 2.1 ± 0.3 | 2.1 ± 0.3 | |
| 2, n (%) | 2361 (93.6) | 2369 (93.9) | 0.64 |
| ≥3, n (%) | 161 (6.4) | 153 (6.1) | |
| Comorbidity | |||
| Cardiovascular disease | 84 (3.3) | 87 (3.4) | 0.82 |
| ESRD | 2 (0.1) | 4 (0.2) | 0.41 |
| Stroke | 9 (0.4) | 14 (0.6) | 0.30 |
| Venous thrombosis | 2 (0.1) | 1 (0.0) | 0.56 |
| Fasting glucose | 100.6 ± 21.4 | 101.8 ± 21.1 | 0.06 |
| HbA1c | 6.8 ± 1.5 | 6.5 ± 1.4 | 0.10 |
| Comedication | |||
| Aromatase inhibitor | 22 (0.9) | 15 (0.6) | 0.25 |
| Diabetes promoting drug | 51 (2.0) | 50 (2.0) | 0.92 |
| Oral glucocorticoid | 113 (4.5) | 113 (4.5) | 1.00 |
| Estrogen | 2 (0.1) | 0 (0.0) | 0.16 |
| Progesterone | 24 (1.0) | 22 (0.9) | 0.77 |
| Adjuvant chemotherapy | 106 (4.2) | 106 (4.2) | 1.00 |
| SERM agent | |||
| Tamoxifen | 2176 (86.3) | - | - |
| Toremifene | 346 (13.7) | - |
| Outcomes | SERM Use (n = 2522) | Non-Use (n = 2522) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Type 2 diabetes | 112 (4.4) | 103 (4.1) | 1.09 (0.83–1.43) | 0.53 |
| Age | ||||
| <40 | 10/510 (2.0) | 8/509 (1.6) | 1.25 (0.49–3.20) | 0.64 |
| 40–65 | 83/1866 (4.4) | 80/1867 (4.3) | 1.04 (0.76–1.42) | 0.81 |
| >65 | 19/146 (13.0) | 15/146 (10.3) | 1.31 (0.64–2.68) | 0.47 |
| CCI | ||||
| 2 | 100/2,361 (4.2) | 91/2369 (3.8) | 1.11 (0.83–1.48) | 0.49 |
| ≥3 | 12/161 (7.5) | 12/153 (7.8) | 0.95 (0.41–2.18) | 0.90 |
| Diabetes promoting drug | ||||
| Yes | 3/51 (5.9) | 0/50 (0.0) | - | - |
| No | 109/2471 (4.4) | 103/2472 (4.2) | 1.06 (0.81–1.40) | 0.67 |
| Oral glucocorticoid | ||||
| Yes | 6/113 (5.3) | 5/113 (4.4) | 1.21 (0.36–4.09) | 0.76 |
| No | 106/2409 (4.4) | 98/2409 (4.1) | 1.09 (0.82–1.44) | 0.57 |
| Metastatic cancer | 78 (3.1) | 81 (3.2) | 0.96 (0.70–1.32) | 0.81 |
| Death | 74 (2.9) | 121 (4.8) | 0.60 (0.45–0.81) | 0.001 |
| Outcome | SERM Use | Non-Use | OR (95% CI) | p-Value |
|---|---|---|---|---|
| SERM agent | ||||
| Tamoxifen | 87/2185 (4.0) | 85/2185 (3.9) | 1.02 (0.76–1.39) | 0.88 |
| Toremifene | 25/346 (7.2) | 18/346 (5.2) | 1.42 (0.76–2.65) | 0.27 |
| Treatment duration (days) | ||||
| <600 | 32/808 (4.0) | 31/808 (3.8) | 1.03 (0.62–1.71) | 0.90 |
| 600 to <1500 | 40/934 (4.3) | 33/934 (3.5) | 1.22 (0.76–1.95) | 0.40 |
| ≥1500 | 40/789 (5.1) | 25/789 (3.2) | 1.63 (1.00–2.72) | 0.048 |
| Tamoxifen | 30/668 (4.5) | 25/789 (3.2) | 1.44 (0.84–2.47) | 0.19 |
| Toremifene | 10/121 (8.3) | 25/789 (3.2) | 2.75 (1.29–5.89) | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.-J.; Bak, K.; Yeo, Y.; Choi, Y.; Shin, S. Incident Type 2 Diabetes Risk of Selective Estrogen Receptor Modulators in Female Patients with Breast Cancer. Pharmaceuticals 2021, 14, 925. https://doi.org/10.3390/ph14090925
Choi Y-J, Bak K, Yeo Y, Choi Y, Shin S. Incident Type 2 Diabetes Risk of Selective Estrogen Receptor Modulators in Female Patients with Breast Cancer. Pharmaceuticals. 2021; 14(9):925. https://doi.org/10.3390/ph14090925
Chicago/Turabian StyleChoi, Yeo-Jin, Keunhyeong Bak, Yoon Yeo, Yongwon Choi, and Sooyoung Shin. 2021. "Incident Type 2 Diabetes Risk of Selective Estrogen Receptor Modulators in Female Patients with Breast Cancer" Pharmaceuticals 14, no. 9: 925. https://doi.org/10.3390/ph14090925