
An Experimental Medicine Investigation of the Effects of Subacute Pramipexole Treatment on Emotional Information Processing in Healthy Volunteers

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Study Sample
2.2. What Were the Side Effects of Pramipexole and Was Blinding Successful?
2.3. Did Pramipexole Treatment Influence Subjective State?
2.4. Did Pramipexole Treatment Induce a Positive Bias in Behavioural Measures of Emotional Information Processing?
2.4.1. Facial Expression Recognition Task (FERT)
2.4.2. Emotional Categorisation Task (ECAT)
2.4.3. Faces Dot Probe Task (FDOT)
2.4.4. Emotional Recall Task (EREC)
2.5. Did Pramipexole Treatment Affect Neural Measures of Emotional Information Processing?
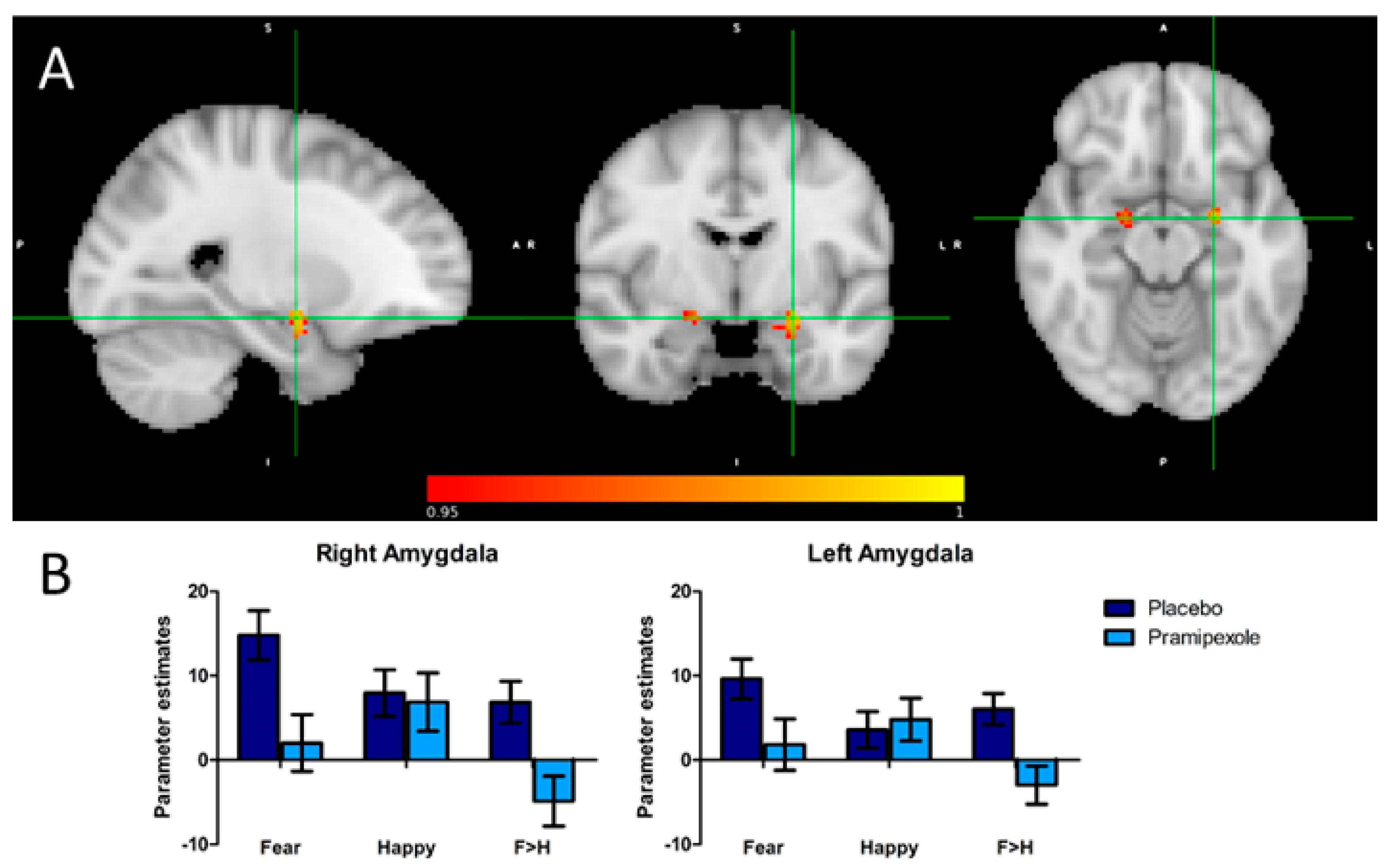
2.5.1. Effect of Treatment on Amygdala Activity (Region of Interest Analysis)
2.5.2. Analyses Controlling for Potential Confounds
Arterial Spin Labelling (ASL)—Effect of Treatment on Whole Brain Perfusion
Effect of Treatment on Amygdala Perfusion (Region of Interest Analysis)
2.5.3. Behavioural Performance in the fMRI Task
3. Discussion
4. Materials and Methods
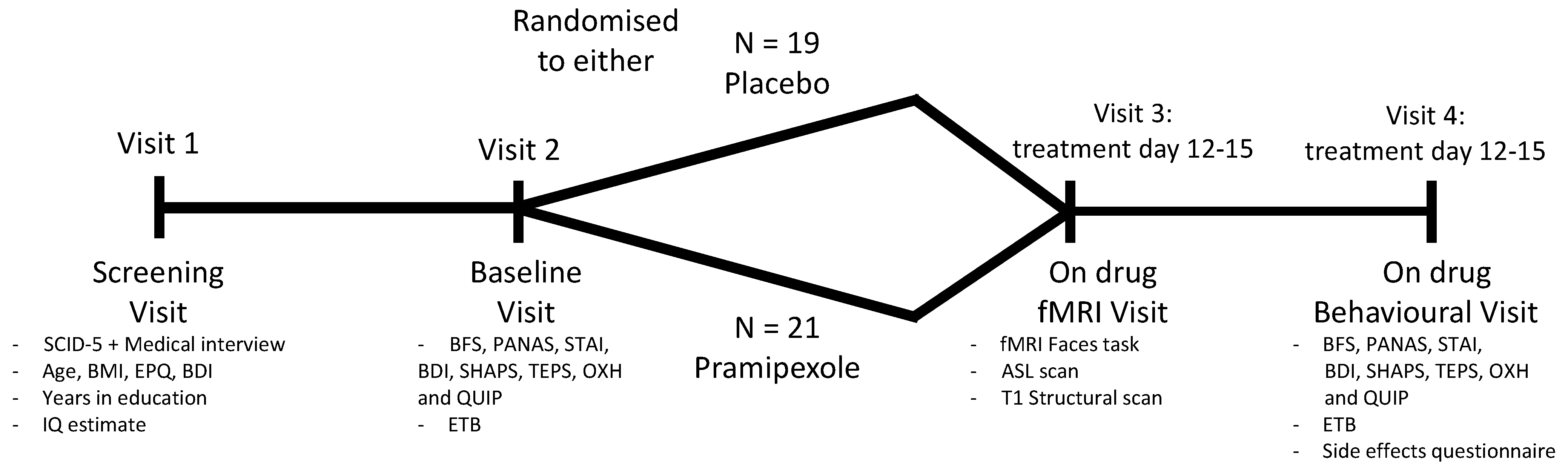
4.1. Participants
4.2. Study Design and Intervention
4.3. Assessment of Subjective State
4.4. Assessment of Side Effects and Blinding
4.5. Assessment of Behavioural Measures of Emotional Information Processing
4.5.1. Facial Expression Recognition Task (FERT)
4.5.2. Emotional Categorisation Task (ECAT)
4.5.3. Emotional Faces Dot Probe Task (FDOT)
4.5.4. Emotional Recall Task (EREC)
4.6. Assessment of Neural Activity during Emotional Information Processing
4.6.1. MRI Faces Task
4.6.2. Neuroimaging Protocol
fMRI—Faces Task
Structural
Arterial Spin Labelling (ASL)
4.7. Data Analysis
4.7.1. Analysis of Questionnaire and Behavioural Data
4.7.2. MRI Data Analysis
fMRI—Faces Task
Arterial Spin Labelling/Resting Brain Perfusion
Global Perfusion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y.; Leucht, S.; Ruhe, H.G.; Turner, E.H.; Higgins, J.P.T.; et al. Comparative Efficacy and Acceptability of 21 Antidepressant Drugs for the Acute Treatment of Adults with Major Depressive Disorder: A Systematic Review and Network Meta-Analysis. Lancet 2018, 391, 1357–1366. [Google Scholar] [CrossRef] [Green Version]
- Cowen, P. Backing into the Future: Pharmacological Approaches to the Management of Resistant Depression. Psychol. Med. 2017, 47, 2569–2577. [Google Scholar] [CrossRef] [Green Version]
- Dunlop, B.W.; Nemeroff, C.B. The Role of Dopamine in the Pathophysiology of Depression. Arch. Gen. Psychiatry 2007, 64, 327–337. [Google Scholar] [CrossRef]
- Romeo, B.; Blecha, L.; Locatelli, K.; Benyamina, A.; Martelli, C. Meta-Analysis and Review of Dopamine Agonists in Acute Episodes of Mood Disorder: Efficacy and Safety. J. Psychopharmacol. 2018, 32, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Tundo, A.; Filippis, R.; De Crescenzo, F. Pramipexole in the Treatment of Unipolar and Bipolar Depression: A Systematic Review and Meta-analysis. Acta Psychiatr. Scand. 2019, 140, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Piercey, M. Pharmacology of Pramipexole, a Dopamine D3-Preferring Agonist Useful in Treating Parkinson’s Disease. Clin. Neuropharmacol. 1998, 21, 141–151. [Google Scholar]
- Ostadhadi, S.; Imran Khan, M.; Norouzi-Javidan, A.; Dehpour, A.-R. Antidepressant Effect of Pramipexole in Mice Forced Swimming Test: A Cross Talk between Dopamine Receptor and NMDA/Nitric Oxide/CGMP Pathway. Biomed. Pharmacother. 2016, 81, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, N.; Choudhury, M.E.; Nishikawa, N.; Nagai, M.; Tujii, T.; Iwaki, H.; Kaneta, M.; Nomoto, M. Pramipexole Upregulates Dopamine Receptor D2 and D3 Expression in Rat Striatum. J. Pharm. Sci. 2012, 120, 133–137. [Google Scholar] [CrossRef] [Green Version]
- Castro-Hernández, J.; Afonso-Oramas, D.; Cruz-Muros, I.; Salas-Hernández, J.; Barroso-Chinea, P.; Moratalla, R.; Millan, M.J.; González-Hernández, T. Prolonged Treatment with Pramipexole Promotes Physical Interaction of Striatal Dopamine D3 Autoreceptors with Dopamine Transporters to Reduce Dopamine Uptake. Neurobiol. Dis. 2015, 74, 325–335. [Google Scholar] [CrossRef]
- Chernoloz, O.; El Mansari, M.; Blier, P. Long-Term Administration of the Dopamine D3/2 Receptor Agonist Pramipexole Increases Dopamine and Serotonin Neurotransmission in the Male Rat Forebrain. J. Psychiatry Neurosci. 2012, 37, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Lieberknecht, V.; Cunha, M.P.; Junqueira, S.C.; dos Santos Coelho, I.; de Souza, L.F.; dos Santos, A.R.S.; Rodrigues, A.L.S.; Dutra, R.C.; Dafre, A.L. Antidepressant-like Effect of Pramipexole in an Inflammatory Model of Depression. Behav. Brain Res. 2017, 320, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Mah, L.; Zarate, C.A.; Nugent, A.C.; Singh, J.B.; Manji, H.K.; Drevets, W.C. Neural Mechanisms of Antidepressant Efficacy of the Dopamine Receptor Agonist Pramipexole in Treatment of Bipolar Depression. Int. J. Neuropsychopharmacol. 2011, 14, 545–551. [Google Scholar] [CrossRef]
- McCabe, C.; Harwood, J.; Brouwer, S.; Harmer, C.J.; Cowen, P.J. Effects of Pramipexole on the Processing of Rewarding and Aversive Taste Stimuli. Psychopharmacology 2013, 228, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Roiser, J.P.; Elliott, R.; Sahakian, B.J. Cognitive Mechanisms of Treatment in Depression. Neuropsychopharmacology 2012, 37, 117–136. [Google Scholar] [CrossRef] [PubMed]
- Warren, M.B.; Pringle, A.; Harmer, C.J. A Neurocognitive Model for Understanding Treatment Action in Depression. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20140213. [Google Scholar] [CrossRef] [Green Version]
- Walsh, A.E.L.; Huneke, N.T.M.; Brown, R.; Browning, M.; Cowen, P.; Harmer, C.J. A Dissociation of the Acute Effects of Bupropion on Positive Emotional Processing and Reward Processing in Healthy Volunteers. Front. Psychiatry 2018, 9, 482. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y. Neuropsychological Mechanism Underlying Antidepressant Effect: A Systematic Meta-Analysis. Mol. Psychiatry 2015, 20, 311–319. [Google Scholar] [CrossRef]
- Browning, M.; Kingslake, J.; Dourish, C.T.; Goodwin, G.M.; Harmer, C.J.; Dawson, G.R. Predicting Treatment Response to Antidepressant Medication Using Early Changes in Emotional Processing. Eur. Neuropsychopharmacol. 2019, 29, 66–75. [Google Scholar] [CrossRef]
- Godlewska, B.R.; Browning, M.; Norbury, R.; Cowen, P.J.; Harmer, C.J. Early Changes in Emotional Processing as a Marker of Clinical Response to SSRI Treatment in Depression. Transl. Psychiatry 2016, 6, e957. [Google Scholar] [CrossRef] [Green Version]
- Shiroma, P.R.; Thuras, P.; Johns, B.; Lim, K.O. Emotion Recognition Processing as Early Predictor of Response to 8-Week Citalopram Treatment in Late-Life Depression: Emotion Recognition in Late-Life Depression. Int. J. Geriatr. Psychiatry 2014, 29, 1132–1139. [Google Scholar] [CrossRef]
- Browning, M.; Bilderbeck, A.C.; Dias, R.; Dourish, C.T.; Kingslake, J.; Deckert, J.; Goodwin, G.M.; Gorwood, P.; Guo, B.; Harmer, C.J.; et al. The Clinical Effectiveness of Using a Predictive Algorithm to Guide Antidepressant Treatment in Primary Care (PReDicT): An Open-Label, Randomised Controlled Trial. Neuropsychopharmacology 2021, 46, 1307–1314. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; Placentino, A.; Carletti, F.; Landi, P.; Allen, P.; Surguladze, S.; Benedetti, F.; Abbamonte, M.; Gasparotti, R.; Barale, F.; et al. Functional Atlas of Emotional Faces Processing: A Voxel-Based Meta-Analysis of 105 Functional Magnetic Resonance Imaging Studies. J. Psychiatry Neurosci. 2009, 34, 418–432. [Google Scholar]
- Grier, J.B. Nonparametric Indexes for Sensitivity and Bias: Computing Formulas. Psychol. Bull. 1971, 75, 424–429. [Google Scholar] [CrossRef]
- Vytal, K.; Hamann, S. Neuroimaging Support for Discrete Neural Correlates of Basic Emotions: A Voxel-Based Meta-Analysis. J. Cogn. Neurosci. 2010, 22, 2864–2885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capitão, L.P.; Chapman, R.; Murphy, S.E.; Harvey, C.-J.; James, A.; Cowen, P.J.; Harmer, C.J. A Single Dose of Fluoxetine Reduces Neural Limbic Responses to Anger in Depressed Adolescents. Transl. Psychiatry 2019, 9, 30. [Google Scholar] [CrossRef] [Green Version]
- Murphy, S.E.; Mackay, C.E. Using MRI to Measure Drug Action: Caveats and New Directions. J. Psychopharmacol. 2011, 25, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Martens, M.; McConnell, F.K.; Filippini, N.; Mackay, C.; Harrison, P.; Tunbridge, E. Dopaminergic Modulation of Regional Cerebral Blood Flow: An Arterial Spin Labelling Study of Genetic and Pharmacological Manipulation of COMT Activity. NeuroImage 2021, 234, 117999. [Google Scholar] [CrossRef]
- Michels, L.; Scherpiet, S.; Stämpfli, P.; Herwig, U.; Brühl, A.B. Baseline Perfusion Alterations Due to Acute Application of Quetiapine and Pramipexole in Healthy Adults. Int. J. Neuropsychopharmacol. 2016, 19, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, A.D.; Calder, A.J.; McGowan, S.W.; Grasby, P.M. Selective Disruption of the Recognition of Facial Expressions of Anger. Neuroreport 2002, 13, 881–884. [Google Scholar] [CrossRef] [PubMed]
- Capitão, L.P.; Murphy, S.E.; Browning, M.; Cowen, P.J.; Harmer, C.J. Acute Fluoxetine Modulates Emotional Processing in Young Adult Volunteers. Psychol. Med. 2015, 45, 2295–2308. [Google Scholar] [CrossRef] [PubMed]
- Schulte-Herbrüggen, O.; Vogt, M.A.; Hörtnagl, H.; Gass, P.; Hellweg, R. Pramipexole Is Active in Depression Tests and Modulates Monoaminergic Transmission, but Not Brain Levels of BDNF in Mice. Eur. J. Pharmacol. 2012, 677, 77–86. [Google Scholar] [CrossRef]
- Groenewold, N.A.; Opmeer, E.M.; de Jonge, P.; Aleman, A.; Costafreda, S.G. Emotional Valence Modulates Brain Functional Abnormalities in Depression: Evidence from a Meta-Analysis of FMRI Studies. Neurosci. Biobehav. Rev. 2013, 37, 152–163. [Google Scholar] [CrossRef]
- Fawcett, J.; Rush, A.J.; Vukelich, J.; Diaz, S.H.; Dunklee, L.; Romo, P.; Yarns, B.C.; Escalona, R. Clinical Experience with High-Dosage Pramipexole in Patients with Treatment-Resistant Depressive Episodes in Unipolar and Bipolar Depression. Am. J. Psychiatry 2016, 173, 107–111. [Google Scholar] [CrossRef] [Green Version]
- Hobbs, C.; Murphy, S.E.; Wright, L.; Carson, J.; Assche, I.V.; O’Brien, J.; Oyesanya, M.; Sui, J.; Munafò, M.R.; Kessler, D.; et al. Effect of Acute Citalopram on Self-Referential Emotional Processing and Social Cognition in Healthy Volunteers. BJPsych Open 2020, 6, e124. [Google Scholar] [CrossRef]
- Kanen, J.W.; Ersche, K.D.; Fineberg, N.A.; Robbins, T.W.; Cardinal, R.N. Computational Modelling Reveals Contrasting Effects on Reinforcement Learning and Cognitive Flexibility in Stimulant Use Disorder and Obsessive-Compulsive Disorder: Remediating Effects of Dopaminergic D2/3 Receptor Agents. Psychopharmacology 2019, 236, 2337–2358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, G.K.; Knolle, F.; Ersche, K.D.; Craig, K.J.; Abbott, S.; Shabbir, S.S.; Fineberg, N.A.; Suckling, J.; Sahakian, B.J.; Bullmore, E.T.; et al. Dopaminergic Drug Treatment Remediates Exaggerated Cingulate Prediction Error Responses in Obsessive-Compulsive Disorder. Psychopharmacology 2019, 236, 2325–2336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feld, G.B.; Besedovsky, L.; Kaida, K.; Münte, T.F.; Born, J. Dopamine D2-like Receptor Activation Wipes out Preferential Consolidation of High over Low Reward Memories during Human Sleep. J. Cogn. Neurosci. 2014, 26, 2310–2320. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.Q.; Glizer, D.; Vo, A.; Seergobin, K.N.; MacDonald, P.A. Pramipexole Increases Go Timeouts but Not No-Go Errors in Healthy Volunteers. Front. Hum. Neurosci. 2016, 10, 523. [Google Scholar] [CrossRef] [Green Version]
- Gallant, H.; Vo, A.; Seergobin, K.N.; MacDonald, P.A. Pramipexole Impairs Stimulus-Response Learning in Healthy Young Adults. Front. Neurosci. 2016, 10, 374. [Google Scholar] [CrossRef] [Green Version]
- Campbell-Meiklejohn, D.; Wakeley, J.; Herbert, V.; Cook, J.; Scollo, P.; Ray, M.K.; Selvaraj, S.; Passingham, R.E.; Cowen, P.; Rogers, R.D. Serotonin and Dopamine Play Complementary Roles in Gambling to Recover Losses. Neuropsychopharmacology 2011, 36, 402–410. [Google Scholar] [CrossRef] [Green Version]
- Martins, D.; Mehta, M.A.; Prata, D. The “Highs and Lows” of the Human Brain on Dopaminergics: Evidence from Neuropharmacology. Neurosci. Biobehav. Rev. 2017, 80, 351–371. [Google Scholar] [CrossRef]
- Walsh, A.E.L.; Browning, M.; Drevets, W.C.; Furey, M.; Harmer, C.J. Dissociable Temporal Effects of Bupropion on Behavioural Measures of Emotional and Reward Processing in Depression. Philos. Trans. R. Soc. B 2018, 373, 20170030. [Google Scholar] [CrossRef]
- Samuels, E.R.; Hou, R.H.; Langley, R.W.; Szabadi, E.; Bradshaw, C.M. Comparison of Pramipexole with and without Domperidone Co-Administration on Alertness, Autonomic, and Endocrine Functions in Healthy Volunteers. Br. J. Clin. Pharm. 2007, 64, 591–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonassi, A.; Ghilardi, T.; Gabrieli, G.; Truzzi, A.; Doi, H.; Borelli, J.L.; Lepri, B.; Shinohara, K.; Esposito, G. The Recognition of Cross-Cultural Emotional Faces Is Affected by Intensity and Ethnicity in a Japanese Sample. Behav. Sci. 2021, 11, 59. [Google Scholar] [CrossRef]
- Young, A.W.; Rowland, D.; Calder, A.J.; Etcoff, N.L.; Seth, A.; Perrett, D.I. Facial Expression Megamix: Tests of Dimensional and Category Accounts of Emotion Recognition. Cognition 1997, 63, 271–313. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M. Fast Robust Automated Brain Extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, M.; Bannister, P.; Brady, M.; Smith, S. Improved Optimization for the Robust and Accurate Linear Registration and Motion Correction of Brain Images. NeuroImage 2002, 17, 825–841. [Google Scholar] [CrossRef]
- Jenkinson, M.; Smith, S. A Global Optimisation Method for Robust Affine Registration of Brain Images. Med. Image Anal. 2001, 5, 143–156. [Google Scholar] [CrossRef]
- Andersson, J.L.R.; Jenkinson, M.; Smith, S. Non-Linear Registration Aka Spatial Normalisation; FMRIB Technical Report TR07JA2; FMRIB Centre: Oxford, UK, 2007. [Google Scholar]
- Andersson, J.L.R.; Jenkinson, M.; Smith, S. Non-Linear Optimisation; FMRIB Technical Report TR07JA1; FMRIB Centre: Oxford, UK, 2007. [Google Scholar]
- Winkler, A.M.; Ridgway, G.R.; Webster, M.A.; Smith, S.M.; Nichols, T.E. Permutation Inference for the General Linear Model. NeuroImage 2014, 92, 381–397. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Nichols, T.E. Threshold-Free Cluster Enhancement: Addressing Problems of Smoothing, Threshold Dependence and Localisation in Cluster Inference. NeuroImage 2009, 44, 83–98. [Google Scholar] [CrossRef] [Green Version]
- Chappell, M.A.; Groves, A.R.; Whitcher, B.; Woolrich, M.W. Variational Bayesian Inference for a Nonlinear Forward Model. IEEE Trans. Signal. Process. 2009, 57, 223–236. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Placebo (n = 19; 10 Male) | Pramipexole (n = 21; 10 Male) | |
|---|---|---|
| Age | 24.5 (6.9) | 22.5 (3.7) |
| Body mass index | 24.0 (2.9) | 22.4 (2.6) |
| Years in full-time education | 17.5 (3.1) | 16.8 (2.9) |
| IQ estimate (spot-the-word test) | 111.9 (7.6) | 108.3 (8.1) |
| Neuroticism (Eysenck personality questionnaire) | 4.3 (3.7) | 4.2 (3.7) |
| Psychoticism (Eysenck personality questionnaire) | 2.8 (2.1) | 2.5 (2.1) |
| Extraversion (Eysenck personality questionnaire) | 14.5 (3.7) | 14.7 (4.5) |
| Lie (Eysenck personality questionnaire) | 7.5 (3.4) | 9.5 (4.6) |
| Trait anxiety (state-trait anxiety inventory) | 32.1 (9.1) | 31.2 (9.1) |
| Depression at inclusion (Beck depression inventory) | 2.5 (4.0) | 1.6 (1.7) |
| Placebo | Pramipexole | Fisher’s Exact Test (Two-Sided) | |
|---|---|---|---|
| Sleeping problems | 26.3% | 33.3% | p = 0.74 |
| Abnormal dreaming | 21.1% | 19% | p = 1.00 |
| Headache | 21.1% | 23.8% | p = 1.00 |
| Dizziness | 10.5% | 33.3% | p = 0.13 |
| Somnolence | 21.1% | 45% | p = 0.18 |
| Nausea | 5.3% | 61.9% | p < 0.001 |
| Vomiting | 0.0% | 19% | p = 0.11 |
| Constipation | 5.3% | 4.8% | p = 1.00 |
| Fatigue | 21.1% | 23.8% | p = 1.00 |
| Impulse control problems | 5.3% | 9.5% | p = 1.00 |
| Hallucinations | 0.0% | 0.0% | - |
| Abnormal movements | 0.0% | 4.8% | p = 1.00 |
| Placebo | Pramipexole | ||||
|---|---|---|---|---|---|
| Baseline | On-Drug | Baseline | On-Drug | ANCOVA Results | |
| BFS | 13.8 (11.2) | 14.8 (14.2) | 11.7 (12.4) | 15.4 (14.7) | F(1.37) = 0.4, p = 0.51 |
| STAI state | 28.6 (6.1) | 29.1 (5.2) | 28.9 (6.5) | 27.8 (5.4) | F(1.37) = 1.2, p = 0.28 |
| BDI | 2.8 (3.3) | 2.7 (3.3) | 1.9 (2.5) | 2.9 (3.4) | F(1.36) = 0.9, p = 0.36 |
| PANAS pos. present | 32.5 (8.6) | 32.6 (7.9) | 36.4 (7.7) | 34.5 (8.3) | F(1.37) = 0.5, p = 0.50 |
| PANAS neg. present | 11.3 (1.3) | 11.8 (2.7) | 11.2 (1.5) | 11.0 (1.5) | F(1.37) = 2.1, p = 0.15 |
| PANAS pos. today | 32.9 (8.2) | 32.3 (8.1) | 36.8 (8.0) | 34.8 (9.1) | F(1.37) = 0.1, p = 0.73 |
| PANAS neg. today | 11.6 (1.7) | 11.8 (2.4) | 11.4 (2.0) | 11.4 (1.7) | F(1.37) = 0.4, p = 0.55 |
| PANAS pos. last week | 34.2 (7.6) | 34.6 (9.3) | 37.7 (9.2) | 37.0 (7.7) | F(1.37) < 0.001, p > 0.99 |
| PANAS neg. last week | 14.1 (4.1) | 12.6 (2.7) | 13.3 (2.8) | 12.7 (3.2) | F(1.37) = 0.1, p = 0.71 |
| SHAPS | 0.2 (0.7) | 0.3 (0.7) | 0.5 (1.0) | 0.7 (1.6) | F(1.37) = 0.3, p = 0.61 |
| TEPS total | 79.3 (8.2) | 79.2 (10.0) | 85.3 (10.0) | 82.1 (9.5) | F(1.37) = 0.7, p = 0.42 |
| TEPS anticipatory | 42.1 (4.9) | 42.3 (5.4) | 47.1 (6.1) | 44.6 (5.5) | F(1.37) = 0.8, p = 0.38 |
| TEPS consummatory | 37.3 (4.4) | 36.8 (5.4) | 38.1 (5.6) | 37.5 (5.9) | F(1.37) = 0.01, p = 0.91 |
| OXH | 132.4 (19.6) | 132.0 (19.7) | 134.8 (19.2) | 138.0 (18.4) | F(1.37) = 3.1, p = 0.08 |
| QUIP | 16.6 (11.2) | 13.8 (10.4) | 12.3 (8.3) | 8.7 (8.5) | F(1.37) = 1.0, p = 0.33 |
| Placebo | Pramipexole | |||
|---|---|---|---|---|
| Baseline | On-Drug | Baseline | On-Drug | |
| Facial expression recognition task (FERT) | ||||
| Hit rate (%) | ||||
| Anger | 55.6 (10.5) | 59.3 (7.7) | 53.3 (12.7) | 57.9 (14.3) |
| Disgust | 66.9 (9.6) | 67.5 (12.6) | 62.3 (15.8) | 62.1 (17.5) |
| Fear | 54.6 (15.2) | 61.1 (10.2) | 49.4 (17.2) | 55.6 (16.2) |
| Happiness | 80.3 (5.4) | 78.2 (5.3) | 77.2 (7.3) | 74.8 (5.5) |
| Sadness | 63.5 (8.5) | 65.1 (9.3) | 63.2 (12.5) | 61.2 (12.3) |
| Surprise | 68.9 (6.5) | 74.2 (5.5) | 67.4 (8.3) | 72.6 (6.8) |
| Neutral | 83.3 (12.4) | 90.6 (10.0) | 87.6 (12.6) | 87.6 (17.6) |
| False alarm rate (%) | ||||
| Anger | 1.7 (1.1) | 1.8 (1.9) | 1.7 (1.9) | 2.1 (2.1) |
| Disgust | 2.4 (1.7) | 1.9 (1.4) | 2.5 (2.0) | 2.2 (1.7) |
| Fear | 1.3 (0.9) | 1.2 (0.9) | 0.9 (1.2) | 1.2 (1.2) |
| Happiness | 0.5 (0.8) | 0.6 (0.8) | 0.5 (0.7) | 0.7 (0.8) |
| Sadness | 3.0 (2.4) | 2.8 (2.4) | 3.5 (3.3) | 3.5 (2.7) |
| Surprise | 2.5 (1.9) | 1.6 (1.4) | 3.4 (2.5) | 2.0 (2.1) |
| Non-identification rate (%) | ||||
| Anger | 33.8 (7.0) | 32.8 (8.3) | 35.6 (9.4) | 34.3 (11.3) |
| Disgust | 21.7 (5.2) | 18.2 (7.4) | 24.3 (7.2) | 22.1 (8.5) |
| Fear | 23.2 (2.5) | 22.5 (4.5) | 23.8 (6.1) | 22.4 (5.1) |
| Happiness | 16.8 (5.5) | 18.6 (5.2) | 19.3 (5.9) | 21.0 (4.8) |
| Sadness | 32.6 (7.7) | 31.8 (8.9) | 34.3 (11.9) | 35.0 (10.8) |
| Surprise | 25.8 (4.9) | 21.0 (5.3) | 27.0 (4.7) | 23.5 (4.1) |
| Reaction time (ms) | ||||
| Anger | 1429.6 (279.2) | 1356.6 (231.3) | 1396.9 (348.1) | 1274.1 (202.4) |
| Disgust | 1435.8 (247.4) | 1246.1 (194.0) | 1437.1 (307.3) | 1245.3 (165.6) |
| Fear | 1645.4 (325.7) | 1456.9 (314.7) | 1646.9 (446.1) | 1443.8 (316.5) |
| Emotional categorisation task (ECAT) | ||||
| Reaction time (ms) | ||||
| Positive | 724.9 (97.3) | 802.4 (120.0) | 748.0 (147.5) | 771.1 (126.1) |
| Negative | 835.3 (135.0) | 869.3 (153.9) | 799.0 (138.6) | 823.0 (171.1) |
| Faces dot probe task (FDOT) | ||||
| Vigilance bias score (ms) | ||||
| Masked positive | −7.7 (38.4) | −11.0 (54.1) | 8.1 (33.0) | 9.5 (37.5) |
| Masked negative | −3.4 (43.8) | −2.9 (32.1) | −16.1 (40.5) | −8.0 (28.1) |
| Unmasked positive | −4.9 (40.5) | 4.9 (35.6) | 4.0 (34.3) | −1.3 (40.3) |
| Unmasked negative | −0.1 (46.0) | −10.7 (33.7) | −12.0 (40.0) | −2.4 (31.3) |
| Emotional recall task (EREC) | ||||
| Hits (n correct) | ||||
| Positive | 4.4 (1.2) | 5.6 (2.7) | 5.6 (2.5) | 6.4 (3.2) |
| Negative | 3.5 (1.0) | 3.2 (2.1) | 4.0 (2.3) | 4.2 (2.2) |
| Intrusions (n wrong) | ||||
| Positive | 3.2 (2.8) | 7.9 (3.2) | 2.4 (2.7) | 8.9 (3.8) |
| Negative | 1.5 (1.6) | 4.4 (2.2) | 1.4 (1.7) | 5.1 (2.1) |
| Exclusion Criteria |
|---|
| Current or past psychiatric disorder (e.g., depression, bipolar disorder) |
| First-degree relative with a diagnosis of schizophrenia-spectrum or other psychotic disorder, or bipolar disorder |
| Body mass index not between 18 and 30 |
| History of unexplained hallucinations or impulse control problems (e.g., pathological gambling) |
| Severe medical condition not stabilized at the time of the experiment (e.g., cardiovascular disease, epilepsy, asthma) |
| Severe heart or blood vessel disease |
| Postural hypotension |
| Any history of seizures |
| Lactose intolerance |
| Any current or past physical illness that has the potential to significantly affect mental functioning (e.g., epilepsy, hypothyroidism, Parkinson’s disease, multiple sclerosis) |
| Pregnant or lactating woman |
| Sexually active woman who does not use any medically accepted method of contraception |
| Current or previous intake (last three months) of any medication that has a significant potential to affect mental functioning (e.g., benzodiazepines, antidepressants, neuroleptics) |
| Any intake of recreational drugs in the last 3 months (e.g., marijuana, ecstasy) |
| Regular alcohol consumption of more than 14 units a week or excessive alcohol consumption up to three days before the experiment |
| Regular smoker (> 5 cigarettes per day) |
| Excessive caffeine user (> 6 caffeinated drinks per day) |
| History of recurrent rashes or history of allergic reactions to relevant substances (e.g., pramipexole) |
| Previous participation in a study using the same or similar tasks |
| History of recurrent rashes or history of allergic reactions to relevant substances (e.g., pramipexole) |
| Previous participation in a study using the same or similar tasks |
| Any contraindication to magnetic resonance imaging (e.g., metallic implant, severe claustrophobia) |
| Current participation in another study |
| In the researcher’s opinion, participation in the study could be harmful or severely distressing to the participant (e.g., intolerance of side effects), or the participant is not able to follow instructions or complete study tasks |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martens, M.A.G.; Kaltenboeck, A.; Halahakoon, D.C.; Browning, M.; Cowen, P.J.; Harmer, C.J. An Experimental Medicine Investigation of the Effects of Subacute Pramipexole Treatment on Emotional Information Processing in Healthy Volunteers. Pharmaceuticals 2021, 14, 800. https://doi.org/10.3390/ph14080800
Martens MAG, Kaltenboeck A, Halahakoon DC, Browning M, Cowen PJ, Harmer CJ. An Experimental Medicine Investigation of the Effects of Subacute Pramipexole Treatment on Emotional Information Processing in Healthy Volunteers. Pharmaceuticals. 2021; 14(8):800. https://doi.org/10.3390/ph14080800
Chicago/Turabian StyleMartens, Marieke Annie Gerdine, Alexander Kaltenboeck, Don Chamith Halahakoon, Michael Browning, Philip J. Cowen, and Catherine J. Harmer. 2021. "An Experimental Medicine Investigation of the Effects of Subacute Pramipexole Treatment on Emotional Information Processing in Healthy Volunteers" Pharmaceuticals 14, no. 8: 800. https://doi.org/10.3390/ph14080800