
A Novel Regimen for Treating Melanoma: MCL1 Inhibitors and Azacitidine

 , ,
, ,
Abstract
:1. Introduction
2. Results
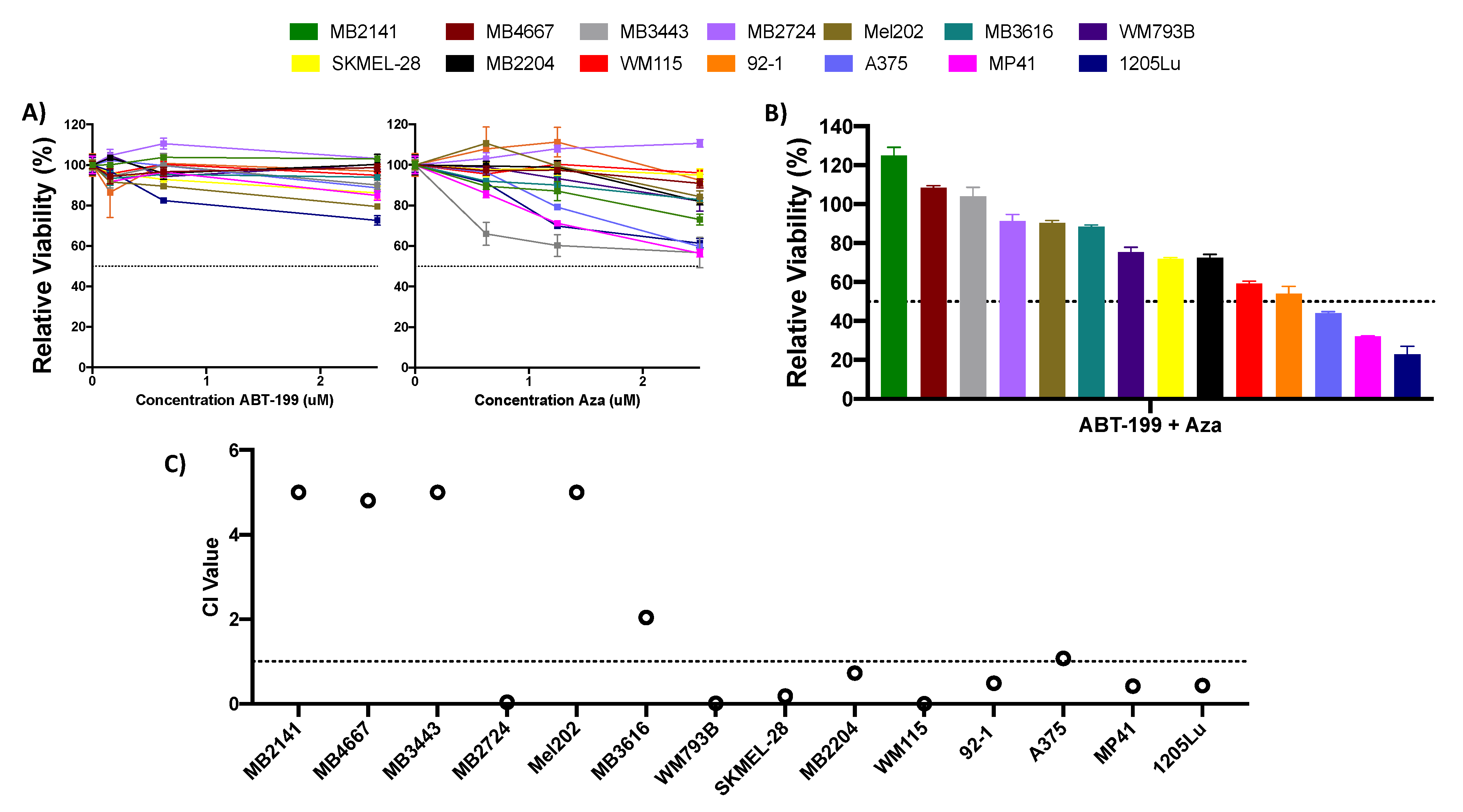
2.1. Single Agent or Combination of ABT-199 Plus Azacitidine Is Not Highly Effective at Reducing Melanoma Cell Viability
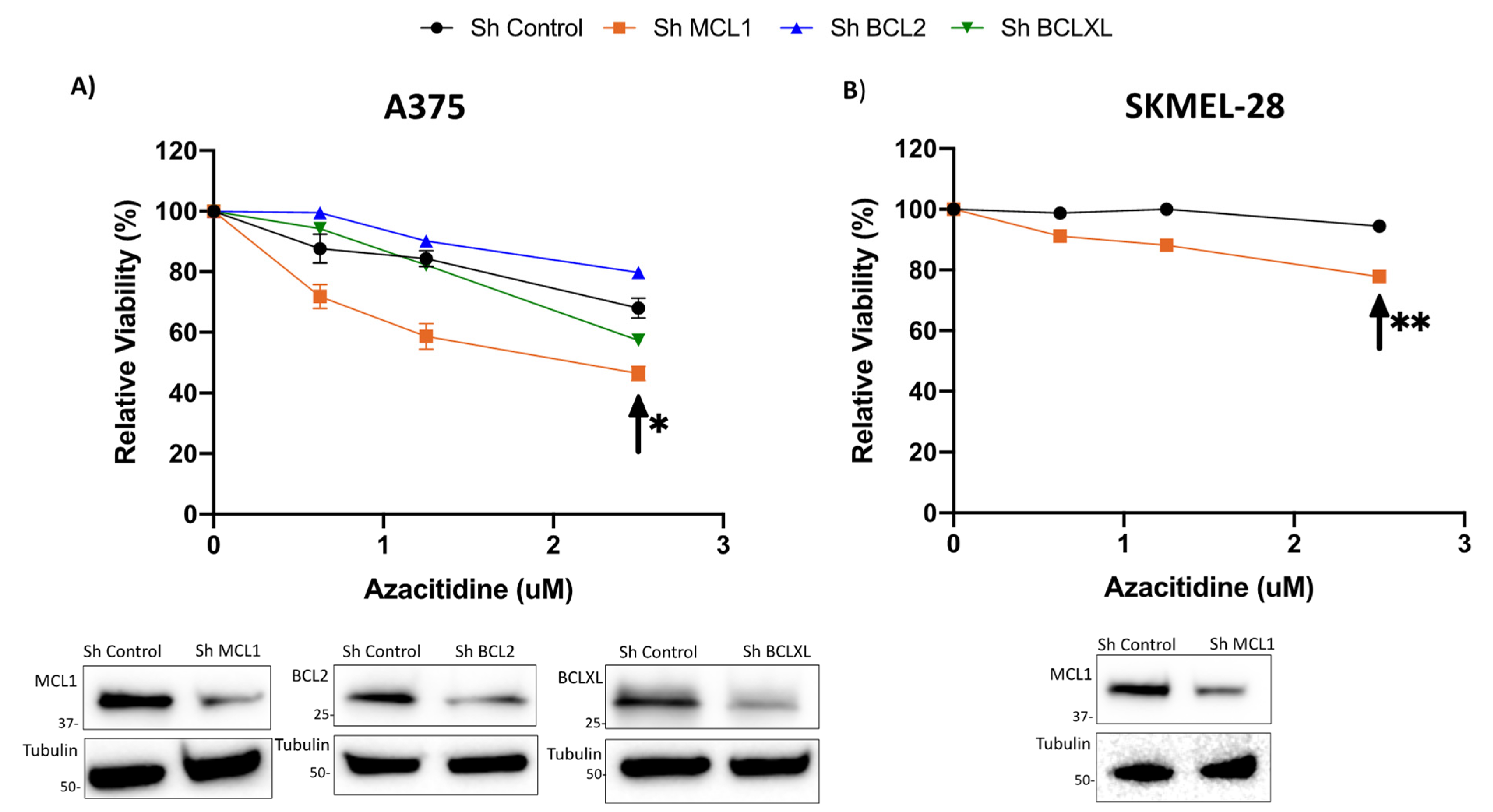
2.2. Knockdown of BCLXL or MCL1 Sensitizes Cells to Treatment with Azacitidine
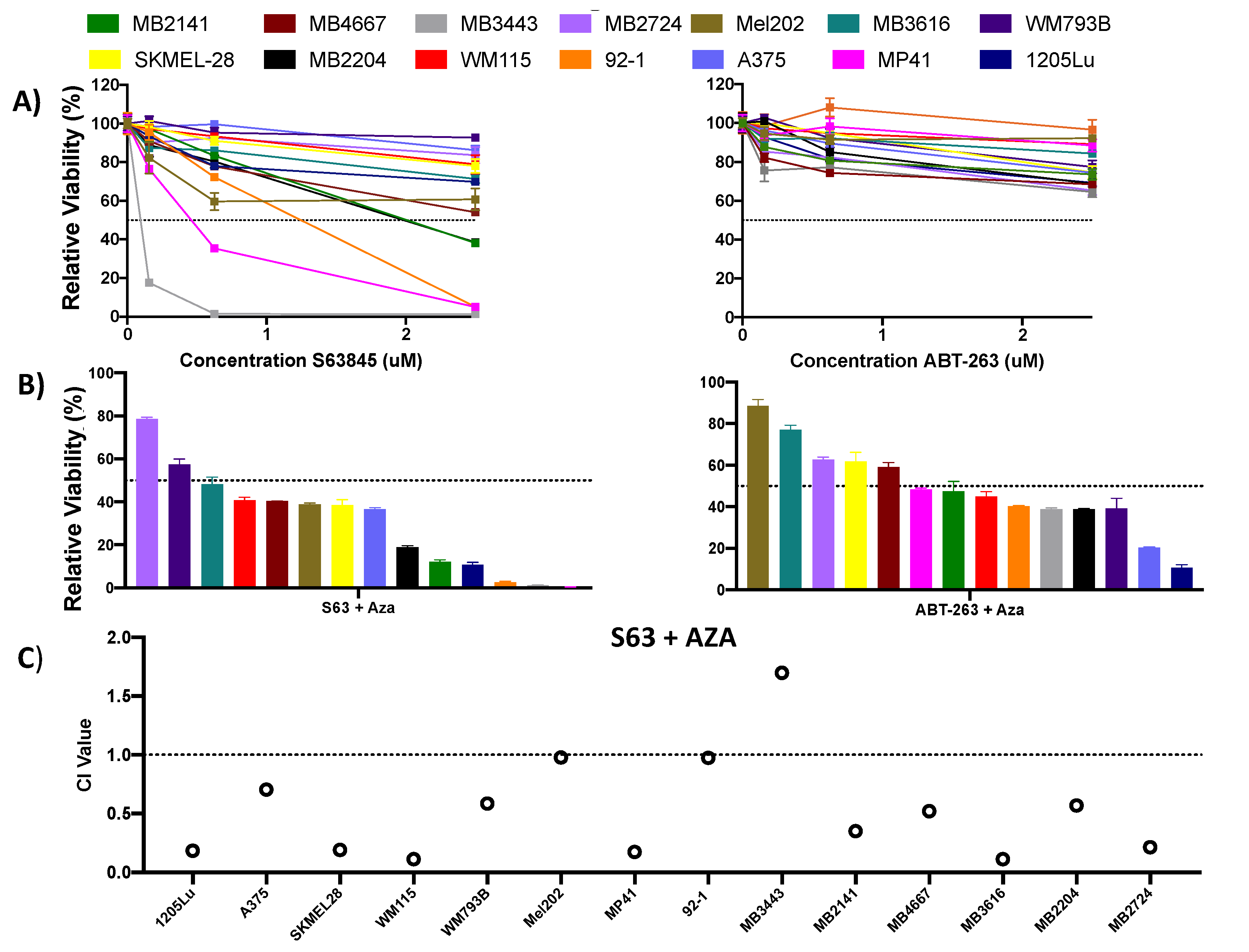
2.3. MCL1i, S63845 or Clinical Grade Version S64315/MIK665, in Combination with Azacitidine Effectively Reduces Cell Growth in Melanoma Cells from a Variety of Subtypes
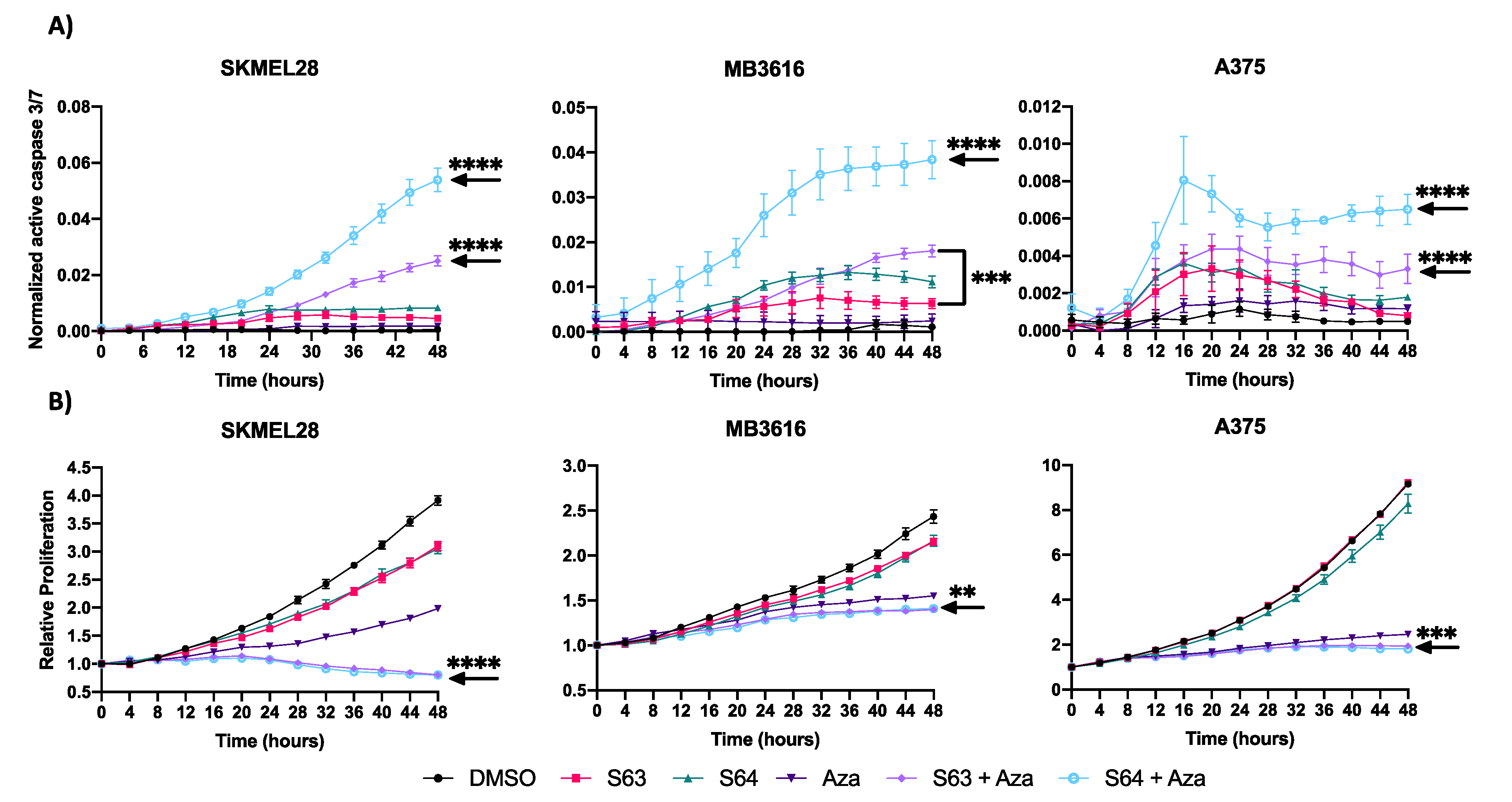
2.4. MCL1i Plus Azacitidine Induce Apoptosis and Reduce Proliferation in Melanoma Cell Lines
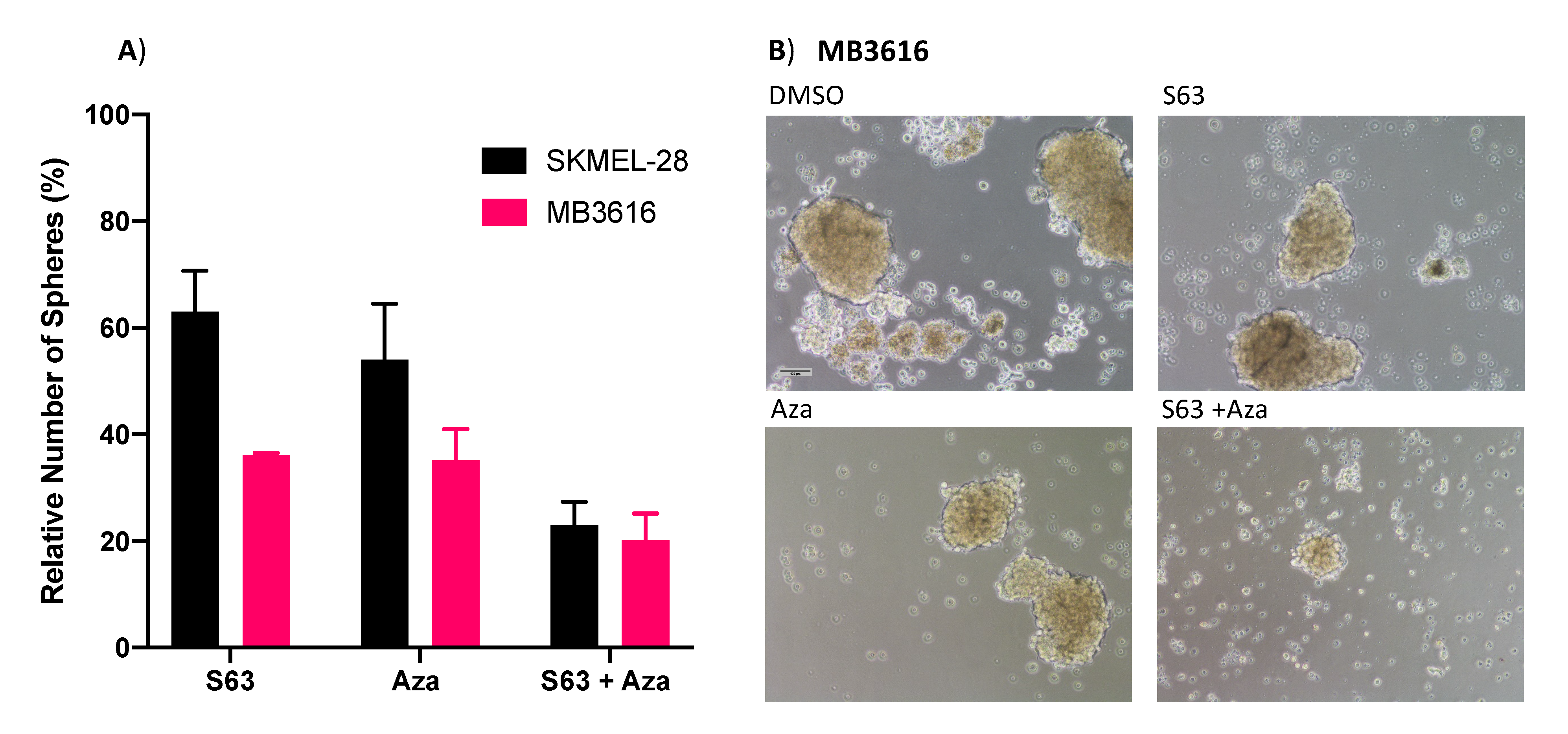
2.5. MCL1i Plus Azacitidine Decreases Sphere Formation of Melanoma Cell Lines
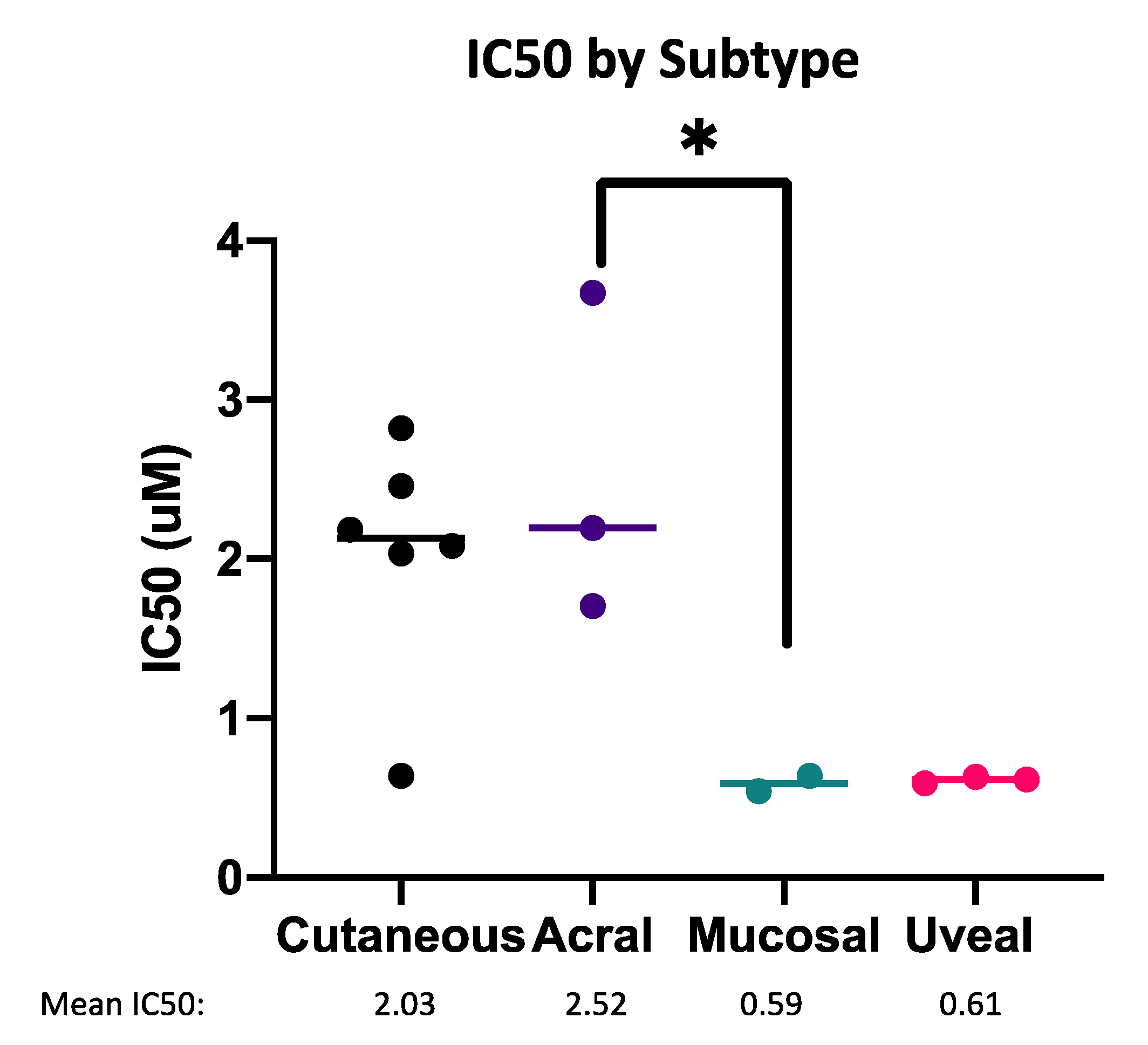
2.6. Sensitivity to MCL1i Plus Azacitidine Treatment May Be Stratified by Melanoma Subtype
2.7. Cell Death Induced by MCL1i Plus Azacitidine Is Not Dependent on BIM or NOXA
3. Discussion
4. Materials and Methods
4.1. Cell Lines and Patient Sample Derived Lines
4.2. Drugs and Dosages
4.3. Cell Viability, Proliferation and Apoptosis Assays
4.4. Immunoblot
4.5. Creation of Stable Knockdown Cell Lines
4.6. Primary Sphere Forming Assay
4.7. Statistical Analysis, Calculation of IC50 and CI Values
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Cancer Facts & Figures 2019; American Cancer Society: Atlanta, GA, USA, 2019. [Google Scholar]
- Cummins, D.L.; Cummins, J.M.; Pantle, H.; Silverman, M.A.; Leonard, A.L.; Chanmugam, A. cutaneous malignant melanoma. Mayo Clin. Proc. 2006, 81, 500–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Zhang, X.; Wang, G.; Cui, X. Triple Combination Therapy With PD-1/PD-L1, BRAF, and MEK Inhibitor for Stage III–IV Melanoma: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 2088. [Google Scholar] [CrossRef]
- Giugliano, F.; Crimini, E.; Tarantino, P.; Zagami, P.; Uliano, J.; Corti, C.; Trapani, D.; Curigliano, G.; Ascierto, P.A. First Line Treatment of BRAF Mutated Advanced Melanoma: Does One Size Fit All? Cancer Treat. Rev. 2021, 99, 102253. [Google Scholar] [CrossRef]
- Yang, J.; Manson, D.K.; Marr, B.P.; Carvajal, R.D. Treatment of Uveal Melanoma: Where Are We Now? Ther. Adv. Med. Oncol. 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Yde, S.S.; Sjoegren, P.; Heje, M.; Stolle, L.B. Mucosal Melanoma: A Literature Review. Curr. Oncol. Rep. 2018, 20, 28. [Google Scholar] [CrossRef]
- Shoushtari, A.N.; Munhoz, R.R.; Kuk, D.; Ott, P.A.; Johnson, D.B.; Tsai, K.K.; Rapisuwon, S.; Eroglu, Z.; Sullivan, R.J.; Luke, J.J.; et al. The Efficacy of Anti-PD-1 Agents in Acral and Mucosal Melanoma. Cancer 2016, 122, 3354–3362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, D.B.; Peng, C.; Abramson, R.G.; Ye, F.; Zhao, S.; Wolchok, J.D.; Sosman, J.A.; Carvajal, R.D.; Ariyan, C.E. Clinical Activity of Ipilimumab in Acral Melanoma: A Retrospective Review. Oncologist 2015, 20, 648–652. [Google Scholar] [CrossRef] [Green Version]
- Edmunds, S.C.; Cree, I.A.; Dí Nícolantonío, F.; Hungerford, J.L.; Hurren, J.S.; Kelsell, D.P. Absence of BRAF Gene Mutations in Uveal Melanomas in Contrast to Cutaneous Melanomas. Br. J. Cancer 2003, 88, 1403–1405. [Google Scholar] [CrossRef] [Green Version]
- Yeh, I.; Jorgenson, E.; Shen, L.; Xu, M.; North, J.P.; Shain, A.H.; Reuss, D.; Wu, H.; Robinson, W.A.; Olshen, A.; et al. Targeted Genomic Profiling of Acral Melanoma. J. Natl. Cancer Inst. 2019, 111, 1068–1077. [Google Scholar] [CrossRef]
- Cruz, F.; Rubin, B.P.; Wilson, D.; Town, A.; Schroeder, A.; Haley, A.; Bainbridge, T.; Heinrich, M.C.; Corless, C.L. Absence of BRAF and NRAS Mutations in Uveal Melanoma. Cancer Res. 2003, 63, 5761–5766. [Google Scholar] [PubMed]
- Juárez-Salcedo, L.M.; Desai, V.; Dalia, S. Venetoclax: Evidence to Date and Clinical Potential. Drugs Context 2019, 8, 212574. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Pratz, K.; Pullarkat, V.; Jonas, B.A.; Arellano, M.; Becker, P.S.; Frankfurt, O.; Konopleva, M.; Wei, A.H.; Kantarjian, H.M.; et al. Venetoclax Combined with Decitabine or Azacitidine in Treatment-Naive, Elderly Patients with Acute Myeloid Leukemia. Blood 2019, 133, 7–17. [Google Scholar] [CrossRef] [Green Version]
- DiNardo, C.D.; Jonas, B.A.; Pullarkat, V.; Thirman, M.J.; Garcia, J.S.; Wei, A.H.; Konopleva, M.; Döhner, H.; Letai, A.; Fenaux, P.; et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. New Engl. J. Med. 2020, 383, 617–629. [Google Scholar] [CrossRef]
- Jones, C.L.; Stevens, B.M.; D’Alessandro, A.; Reisz, J.A.; Culp-Hill, R.; Nemkov, T.; Pei, S.; Khan, N.; Adane, B.; Ye, H.; et al. Inhibition of Amino Acid Metabolism Selectively Targets Human Leukemia Stem Cells. Cancer Cell 2018, 34, 724–740. [Google Scholar] [CrossRef] [Green Version]
- Pollyea, D.A.; Stevens, B.M.; Jones, C.L.; Winters, A.; Pei, S.; Minhajuddin, M.; D’Alessandro, A.; Culp-Hill, R.; Riemondy, K.A.; Gillen, A.E.; et al. Venetoclax with Azacitidine Disrupts Energy Metabolism and Targets Leukemia Stem Cells in Patients with Acute Myeloid Leukemia. Nat. Med. 2018, 24, 1859–1866. [Google Scholar] [CrossRef]
- Lee, E.F.; Harris, T.J.; Tran, S.; Evangelista, M.; Arulananda, S.; John, T.; Ramnac, C.; Hobbs, C.; Zhu, H.; Gunasingh, G.; et al. BCL-XL and MCL-1 Are the Key BCL-2 Family Proteins in Melanoma Cell Survival. Cell Death Dis. 2019, 10, 1–14. [Google Scholar] [CrossRef]
- Mukherjee, N.; Lu, Y.; Almeida, A.; Lambert, K.; Shiau, C.-W.; Su, J.-C.; Luo, Y.; Fujita, M.; Robinson, W.A.; Robinson, S.E.; et al. Use of a MCL-1 Inhibitor Alone to de-Bulk Melanoma and in Combination to Kill Melanoma Initiating Cells. Oncotarget 2016, 8, 46801. [Google Scholar] [CrossRef]
- Mukherjee, N.; Skees, J.; Todd, K.J.; West, D.A.; Lambert, K.A.; Robinson, W.A.; Amato, C.M.; Couts, K.L.; Van Gulick, R.; MacBeth, M.; et al. MCL1 Inhibitors S63845/MIK665 plus Navitoclax Synergistically Kill Difficult-to-Treat Melanoma Cells. Cell Death Dis. 2020, 11, 443. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Haass, N.K. Microenvironment-Driven Dynamic Heterogeneity and Phenotypic Plasticity as a Mechanism of Melanoma Therapy Resistance. Front. Oncol. 2018, 8, 173. [Google Scholar] [CrossRef]
- Villani, V.; Sabbatino, F.; Ferrone, C.R.; Ferrone, S. Melanoma Initiating Cells: Where Do We Stand? Melanoma Manag. 2015, 2, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, N.; Schwan, J.V.; Fujita, M.; Norris, D.A.; Shellman, Y.G. Alternative Treatments for Melanoma: Targeting BCL-2 Family Members to De-Bulk and Kill Cancer Stem Cells. J. Invest. Dermatol. 2015, 135, 2155–2161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukherjee, N.; Amato, C.M.; Skees, J.; Todd, K.J.; Lambert, K.A.; Robinson, W.A.; Van Gulick, R.; Weight, R.M.; Dart, C.R.; Tobin, R.P.; et al. Simultaneously Inhibiting BCL2 and MCL1 Is a Therapeutic Option for Patients with Advanced Melanoma. Cancers 2020, 12, 2182. [Google Scholar] [CrossRef] [PubMed]
- Stecca, B.; Santini, R.; Pandolfi, S.; Penachioni, J.Y. Culture and Isolation of Melanoma-Initiating Cells. Curr. Protoc. Stem Cell Biol. 2013, 24, 3.6.1–3.6.12. [Google Scholar] [CrossRef]
- Mukherjee, N.; Strosnider, A.; Vagher, B.; Lambert, K.A.; Slaven, S.; Robinson, W.A.; Amato, C.M.; Couts, K.L.; Bemis, J.G.T.; Turner, J.A.; et al. BH3 Mimetics Induce Apoptosis Independent of DRP-1 in Melanoma. Cell Death Dis. 2018, 9, 1–12. [Google Scholar] [CrossRef]
- Johnson, S.; Chen, H.; Lo, P.-K. In Vitro Tumorsphere Formation Assays. Bio Protoc 2013, 3, e325. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Roberto, M.; Panebianco, M.; Botticelli, A.; Mazzuca, F.; Marchetti, P. Drug Resistance of BRAF-Mutant Melanoma: Review of up-to-Date Mechanisms of Action and Promising Targeted Agents. Eur. J. Pharmacol. 2019, 862, 172621. [Google Scholar] [CrossRef]
- Gide, T.N.; Wilmott, J.S.; Scolyer, R.A.; Long, G.V. Primary and Acquired Resistance to Immune Checkpoint Inhibitors in Metastatic Melanoma. Clin. Cancer Res. 2018, 24, 1260–1270. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.; Carvajal, R.D. Novel Approaches to the Systemic Management of Uveal Melanoma. Curr. Oncol. Rep. 2020, 22, 104. [Google Scholar] [CrossRef] [PubMed]
- Middleton, M.R.; McAlpine, C.; Woodcock, V.K.; Corrie, P.; Infante, J.R.; Steven, N.M.; Evans, T.R.J.; Anthoney, A.; Shoushtari, A.N.; Hamid, O.; et al. Tebentafusp, A TCR/Anti-CD3 Bispecific Fusion Protein Targeting Gp100, Potently Activated Antitumor Immune Responses in Patients with Metastatic Melanoma. Clin. Cancer Res. 2020, 26, 5869–5878. [Google Scholar] [CrossRef]
- Alkermes Announces FDA Orphan Drug Designation for Nemvaleukin Alfa for Treatment of Mucosal Melanoma | Alkermes Plc. Available online: https://investor.alkermes.com/news-releases/news-release-details/alkermes-announces-fda-orphan-drug-designation-nemvaleukin-alfa (accessed on 14 June 2021).
- Nemvaleukin for Mucosal Melanoma Granted FDA’s Orphan Drug Status. Available online: https://www.targetedonc.com/view/nemvaleukin-for-mucosal-melanoma-granted-fda-s-orphan-drug-status (accessed on 14 June 2021).
- Rajaii, F.; Asnaghi, L.; Enke, R.; Merbs, S.L.; Handa, J.T.; Eberhart, C.G. The Demethylating Agent 5-Aza Reduces the Growth, Invasiveness, and Clonogenicity of Uveal and Cutaneous Melanoma. Invest. Ophthalmol. Vis. Sci. 2014, 55, 6178–6186. [Google Scholar] [CrossRef] [Green Version]
- DiNardo, C.D.; Tiong, I.S.; Quaglieri, A.; MacRaild, S.; Loghavi, S.; Brown, F.C.; Thijssen, R.; Pomilio, G.; Ivey, A.; Salmon, J.M.; et al. Molecular Patterns of Response and Treatment Failure after Frontline Venetoclax Combinations in Older Patients with AML. Blood 2020, 135, 791–803. [Google Scholar] [CrossRef]
- Chacón, M.; Pfluger, Y.; Angel, M.; Waisberg, F.; Enrico, D. Uncommon Subtypes of Malignant Melanomas: A Review Based on Clinical and Molecular Perspectives. Cancers 2020, 12, 2362. [Google Scholar] [CrossRef]
- Basurto-Lozada, P.; Molina-Aguilar, C.; Castaneda-Garcia, C.; Vázquez-Cruz, M.E.; Garcia-Salinas, O.I.; Álvarez-Cano, A.; Martínez-Said, H.; Roldán-Marín, R.; Adams, D.J.; Possik, P.A.; et al. Acral Lentiginous Melanoma: Basic Facts, Biological Characteristics and Research Perspectives of an Understudied Disease. Pigment Cell Melanoma Res. 2021, 34, 59–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabbie, R.; Ferguson, P.; Molina-Aguilar, C.; Adams, D.J.; Robles-Espinoza, C.D. Melanoma Subtypes: Genomic Profiles, Prognostic Molecular Markers and Therapeutic Possibilities. J. Pathol. 2019, 247, 539–551. [Google Scholar] [CrossRef]
- Newell, F.; Wilmott, J.S.; Johansson, P.A.; Nones, K.; Addala, V.; Mukhopadhyay, P.; Broit, N.; Amato, C.M.; Van Gulick, R.; Kazakoff, S.H.; et al. Whole-Genome Sequencing of Acral Melanoma Reveals Genomic Complexity and Diversity. Nat. Commun. 2020, 11, 5259. [Google Scholar] [CrossRef]
- Slominski, A.; Tobin, D.J.; Shibahara, S.; Wortsman, J. Melanin Pigmentation in Mammalian Skin and Its Hormonal Regulation. Physiol. Rev. 2004, 84, 1155–1228. [Google Scholar] [CrossRef]
- Nishimura, E.K.; Granter, S.R.; Fisher, D.E. Mechanisms of Hair Graying: Incomplete Melanocyte Stem Cell Maintenance in the Niche. Science 2005, 307, 720–724. [Google Scholar] [CrossRef] [Green Version]
- McGill, G.G.; Horstmann, M.; Widlund, H.R.; Du, J.; Motyckova, G.; Nishimura, E.K.; Lin, Y.-L.; Ramaswamy, S.; Avery, W.; Ding, H.-F.; et al. Bcl2 Regulation by the Melanocyte Master Regulator Mitf Modulates Lineage Survival and Melanoma Cell Viability. Cell 2002, 109, 707–718. [Google Scholar] [CrossRef] [Green Version]
- Yamamura, K.; Kamada, S.; Ito, S.; Nakagawa, K.; Ichihashi, M.; Tsujimoto, Y. Accelerated Disappearance of Melanocytes in Bcl-2-Deficient Mice. Cancer Res. 1996, 56, 3546–3550. [Google Scholar]
- Hird, A.W.; Tron, A.E. Recent Advances in the Development of Mcl-1 Inhibitors for Cancer Therapy. Pharmacol. Ther. 2019, 198, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Kotschy, A.; Szlavik, Z.; Murray, J.; Davidson, J.; Maragno, A.L.; Le Toumelin-Braizat, G.; Chanrion, M.; Kelly, G.L.; Gong, J.-N.; Moujalled, D.M.; et al. The MCL1 Inhibitor S63845 Is Tolerable and Effective in Diverse Cancer Models. Nature 2016, 538, 477–482. [Google Scholar] [CrossRef]
- Brennan, M.S.; Chang, C.; Tai, L.; Lessene, G.; Strasser, A.; Dewson, G.; Kelly, G.L.; Herold, M.J. Humanized Mcl-1 Mice Enable Accurate Preclinical Evaluation of MCL-1 Inhibitors Destined for Clinical Use. Blood 2018, 132, 1573–1583. [Google Scholar] [CrossRef] [Green Version]
- Ruth, M.C.; Xu, Y.; Maxwell, I.H.; Ahn, N.G.; Norris, D.A.; Shellman, Y.G. RhoC Promotes Human Melanoma Invasion in a PI3K/Akt-Dependent Pathway. J. Investig. Dermatol. 2006, 126, 862–868. [Google Scholar] [CrossRef] [Green Version]
- Reuland, S.N.; Goldstein, N.B.; Partyka, K.A.; Cooper, D.A.; Fujita, M.; Norris, D.A.; Shellman, Y.G. The Combination of BH3-Mimetic ABT-737 with the Alkylating Agent Temozolomide Induces Strong Synergistic Killing of Melanoma Cells Independent of P53. PLoS ONE 2011, 6, e24294. [Google Scholar] [CrossRef]
- Reuland, S.N.; Goldstein, N.B.; Partyka, K.A.; Smith, S.; Luo, Y.; Fujita, M.; Gonzalez, R.; Lewis, K.; Norris, D.A.; Shellman, Y.G. ABT-737 Synergizes with Bortezomib to Kill Melanoma Cells. Biol. Open 2011, 1, 92–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukherjee, N.; Almeida, A.; Partyka, K.A.; Lu, Y.; Schwan, J.V.; Lambert, K.; Rogers, M.; Robinson, W.A.; Robinson, S.E.; Applegate, A.J.; et al. Combining a GSI and BCL-2 Inhibitor to Overcome Melanoma’s Resistance to Current Treatments. Oncotarget 2016, 7, 84594–84607. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, N.; Reuland, S.N.; Lu, Y.; Luo, Y.; Lambert, K.; Fujita, M.; Robinson, W.A.; Robinson, S.E.; Norris, D.A.; Shellman, Y.G. Combining a BCL2 Inhibitor with the Retinoid Derivative Fenretinide Targets Melanoma Cells Including Melanoma Initiating Cells. J. Investig. Dermatol. 2015, 135, 842–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukherjee, N.; Lambert, K.A.; Norris, D.A.; Shellman, Y.G. Enrichment of melanoma stem-like cells via sphere assays. In Methods in Molecular Biology; Springer: Berlin, Germany, 2021; Volume 2265, pp. 185–199. [Google Scholar]
- Chou, T.-C. Theoretical Basis, Experimental Design, and Computerized Simulation of Synergism and Antagonism in Drug Combination Studies. Pharmacol. Rev. 2006, 58, 621–681. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cell/MB Line | Genotype | Subtype |
|---|---|---|
| A375 | BRAF V600E | Cutaneous |
| 1205Lu | BRAF V600E | Cutaneous |
| SKMEL-28 | BRAF V600E | Cutaneous |
| WM793B | BRAF V600E | Cutaneous |
| WM115 | BRAF V600D | Superficial spreading |
| MB2141 | EML4-ALK | Mucosal |
| MB3443 | NRAS Q61H | Mucosal |
| MB3616 | NRAS Q61K | Superficial spreading |
| MB4667 | NRAS Q61R | Acral |
| MB2724 | Triple WT (BRAF, NRAS, NF) | Acral |
| MB2204 | Triple WT (BRAF, NRAS, NF) | Acral |
| Mel202 | SF3B1 R625G, GNAQ Q209L, R210K | Uveal |
| 92-1 | GNAQ Q209L | Uveal |
| MP46 | GNAQ Q209P | Uveal |
| MP41 | GNAQ Q209L | Uveal |
| MB Line | Primary or Metastatic | Sample Collection Site | Pigmentation Status of Tumor |
|---|---|---|---|
| MB2141 | Metastatic | Subcutaneous | Unknown |
| MB3616 | Metastatic | Brain | Unknown |
| MB2724 | Metastatic | Lymph node | Unknown |
| MB3443 | Metastatic | Neck | Amelanotic |
| MB4667 | Metastatic | Subcutaneous | Amelanotic |
| MB2204 | Metastatic | Subcutaneous | Amelanotic |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dart, C.R.; Mukherjee, N.; Amato, C.M.; Goulding, A.; MacBeth, M.; Van Gulick, R.; Couts, K.L.; Lambert, J.R.; Norris, D.A.; Robinson, W.A.; et al. A Novel Regimen for Treating Melanoma: MCL1 Inhibitors and Azacitidine. Pharmaceuticals 2021, 14, 749. https://doi.org/10.3390/ph14080749
Dart CR, Mukherjee N, Amato CM, Goulding A, MacBeth M, Van Gulick R, Couts KL, Lambert JR, Norris DA, Robinson WA, et al. A Novel Regimen for Treating Melanoma: MCL1 Inhibitors and Azacitidine. Pharmaceuticals. 2021; 14(8):749. https://doi.org/10.3390/ph14080749
Chicago/Turabian StyleDart, Chiara R., Nabanita Mukherjee, Carol M. Amato, Anabel Goulding, Morgan MacBeth, Robert Van Gulick, Kasey L. Couts, James R. Lambert, David A. Norris, William A. Robinson, and et al. 2021. "A Novel Regimen for Treating Melanoma: MCL1 Inhibitors and Azacitidine" Pharmaceuticals 14, no. 8: 749. https://doi.org/10.3390/ph14080749