
Development of Wearable Devices for Collecting Digital Rehabilitation/Fitness Data from Lower Limbs

 , and
, and
Abstract
:1. Introduction
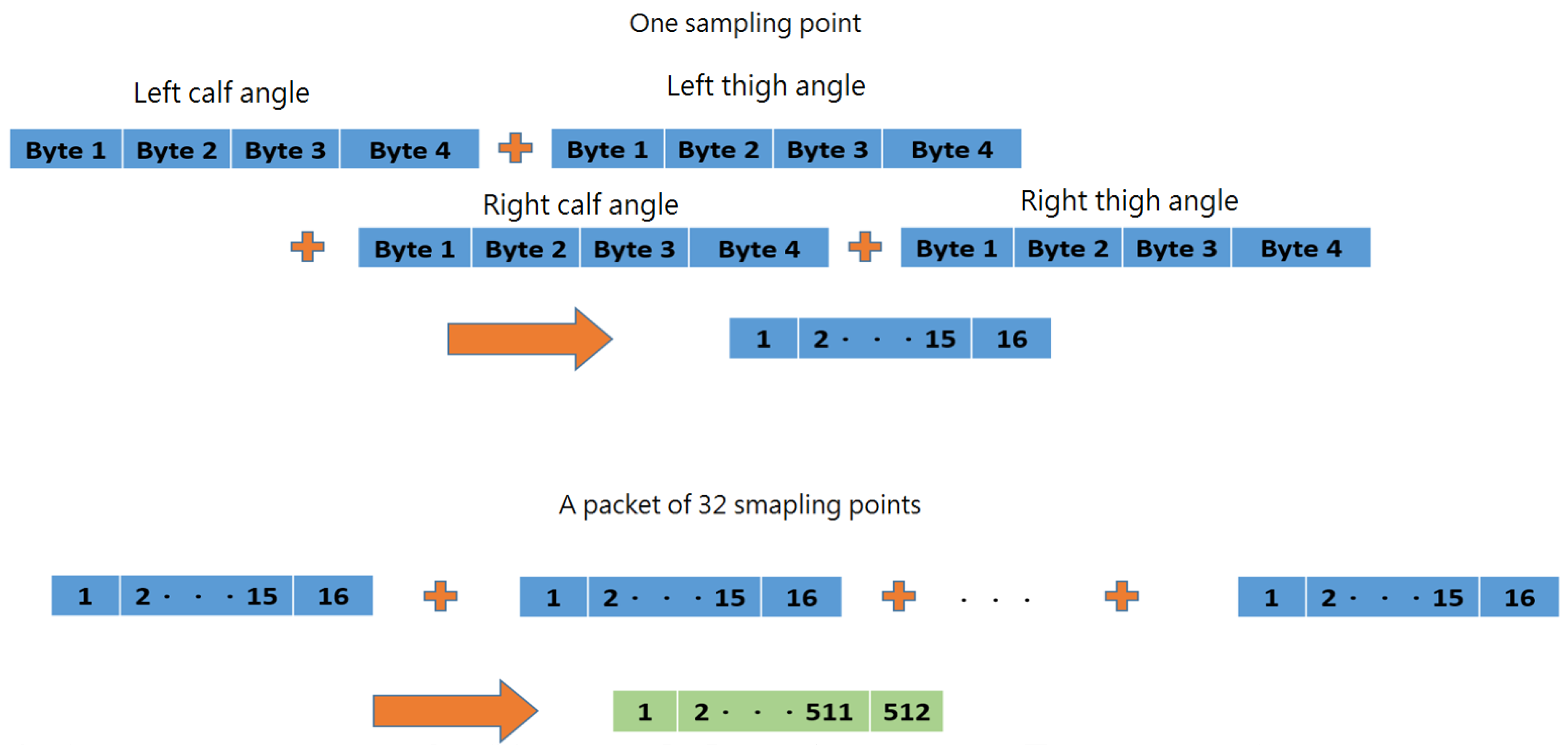
- Cost-effective RF modules were developed to implement the proposed system for transmitting the motion data from each IMU at a sampling rate of 60 Hz, while most other systems used Wi-Fi or Bluetooth. RF communication provides more reliable data acquisition than Bluetooth or Wi-Fi in crowded environments where several Wi-Fi and Bluetooth networks coexist.
- A custom do-it-yourself IMU-based system that does not use commercial IMU systems is presented.
- The developed system was tested in the laboratory environment in real time using a 3D avatar to represent 3D movement.
- A pre-trained machine learning model deployed on the smartphone can instantly obtain FAR (fitness activity recognition) results and display fitness activity data such as repetitions, intensity, energy consumption, and exercise duration, leveraging the data generated by users during fitness/rehabilitation to provide instantaneous and personalized insights.
- A DTW algorithm was integrated into the system for scoring the similarity in two motions.
2. Materials and Methods
2.1. Hardware
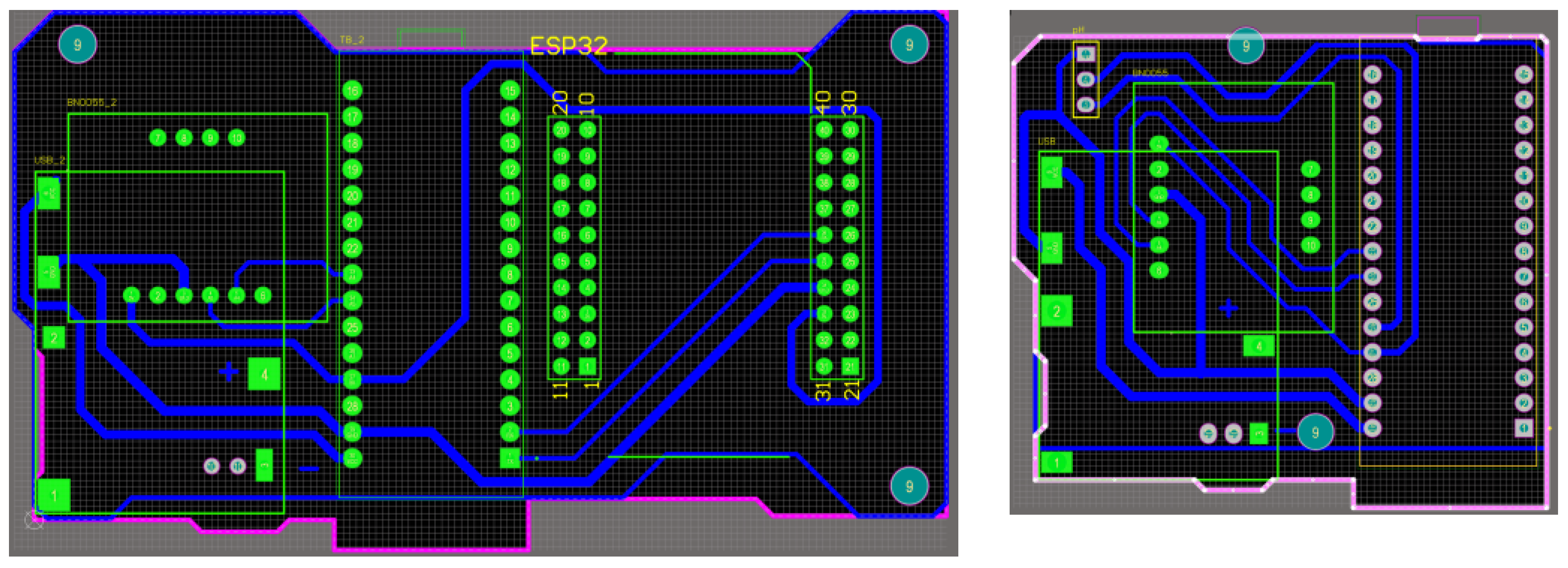
- Microcontroller unit (MCU) with BLE: It controls the reading of IMU data, programs algorithms to convert values, and exchanges data through Bluetooth. ESP32 (Espressif Systems, Shanghai, China) is used in this system.
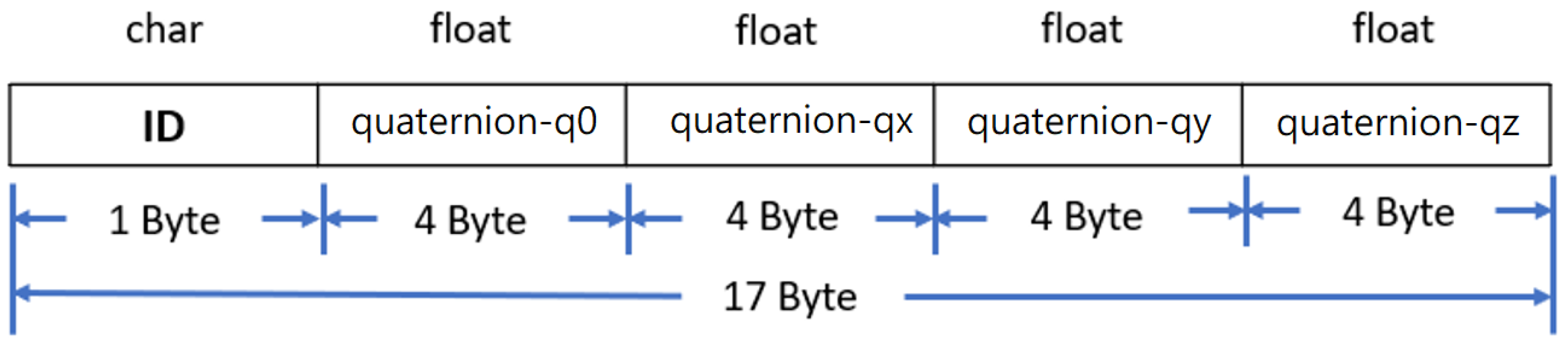
- Inertial measurement unit (IMU): It captures the spatial coordinate vector data (quaternion) of motion attitude (9 axes including 3-axis acceleration, 3-axis angular velocity, and 3-axis geomagnetism). BNO055 (Bosch Sensortec GmbH, Reutlingen, Germany) is used in this system, which can also output stable quaternion data in addition to 9-axis data.
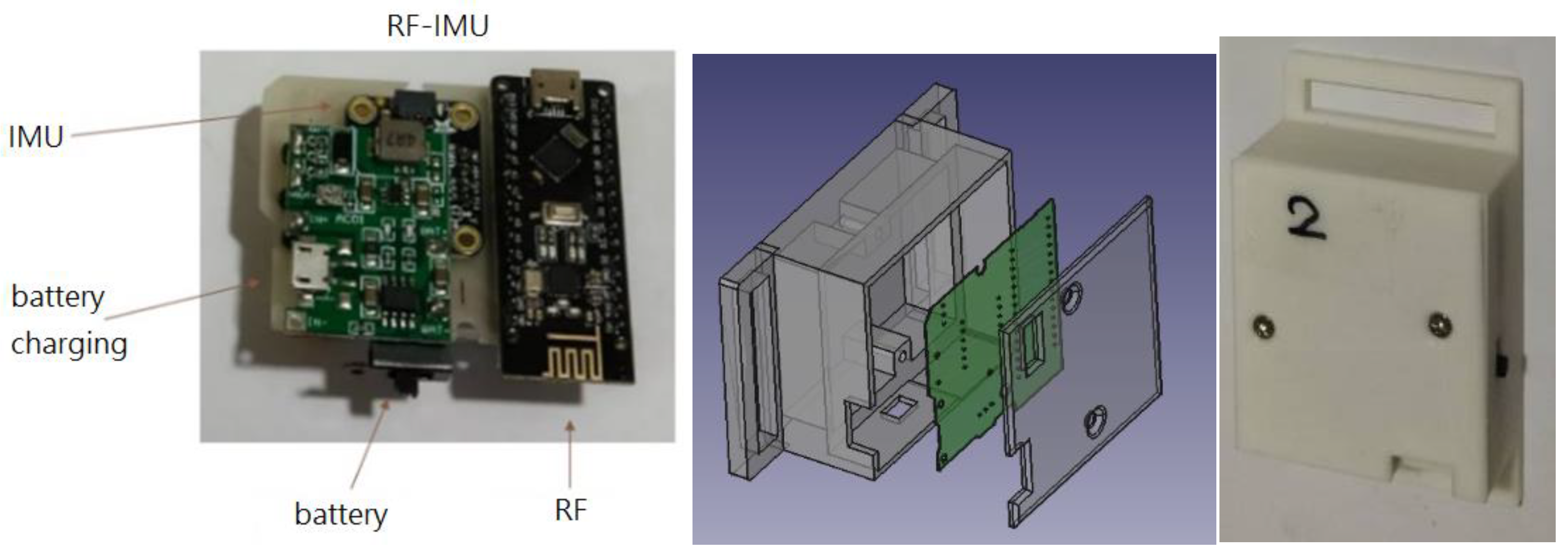
- RF with MCU: RF-Nano (Arduino Nano R3 + nRF24L01) is used in this system to transmit data wirelessly using RF. It combines the simplicity and compatibility of Arduino Nano R3′s ATmega328 with the usefulness of the nRF24L01+ (Nordic Semiconductor ASA, Trondheim, Norway) 2.4 GHz radio transceiver in one single board [23]. nRF24L01+ is a compact 2.4 GHz transceiver chip featuring an integrated baseband protocol engine known as Enhanced ShockBurst™, ideal for energy-efficient wireless applications [24]. Engineered to function within the globally recognized ISM frequency band of 2.400–2.4835 GHz, nRF24L01+ offers versatility and reliability. The specifications of the MCU in RF-Nano are identical to the Arduino Nano R3 development board. The nRF24L01+ chip is connected to the ATmega328P chip directly on the board. This means there are SPI pins on the GPIO that you can no longer use for other purposes. These pins are listed in Table 1. The MCU is connected to the IMU via the I2C to read the motion data.
- Lithium battery charging module: It provides power for each individual module.
2.2. Software
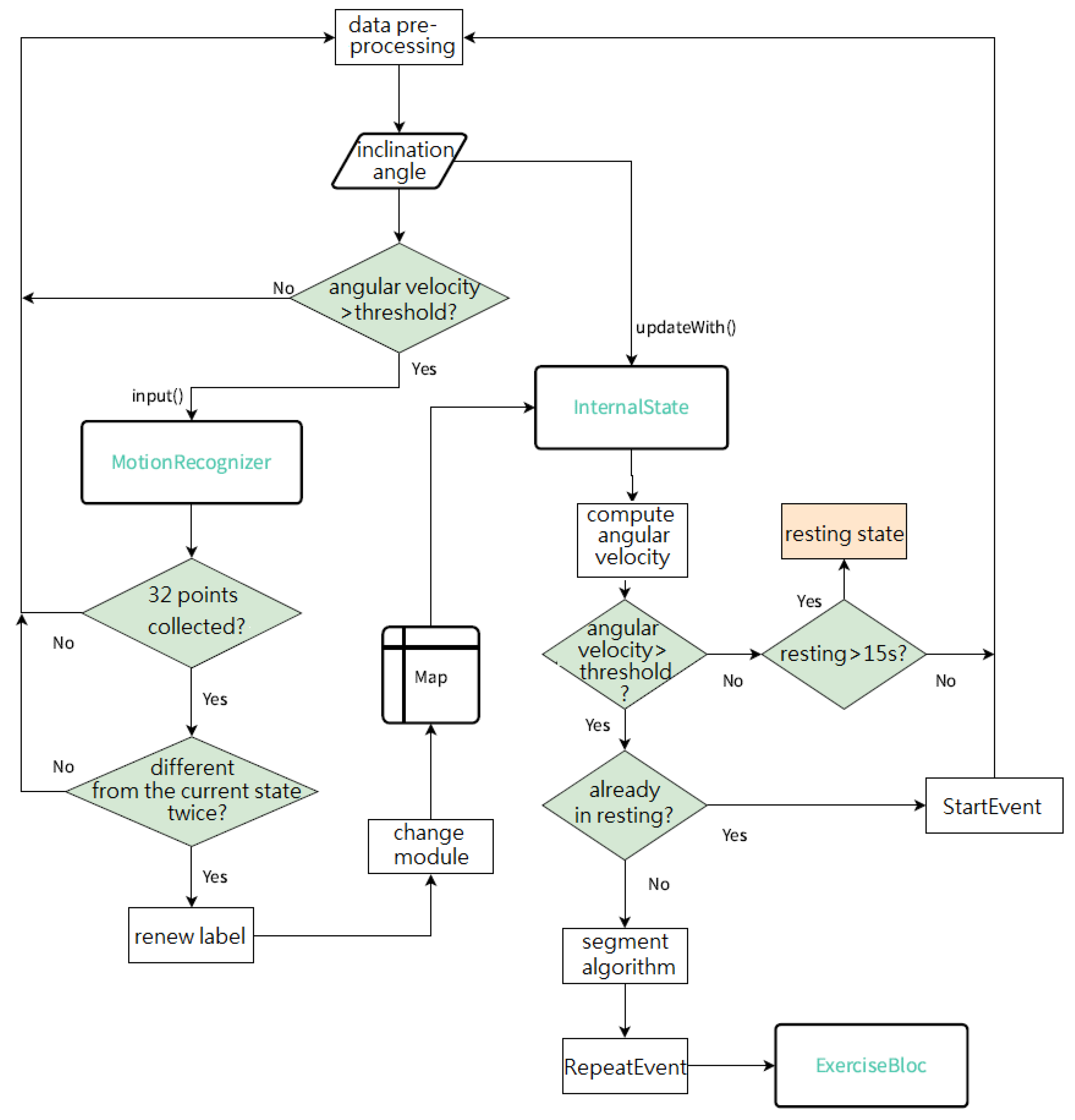
2.2.1. MotionRecognizer
2.2.2. InternalState
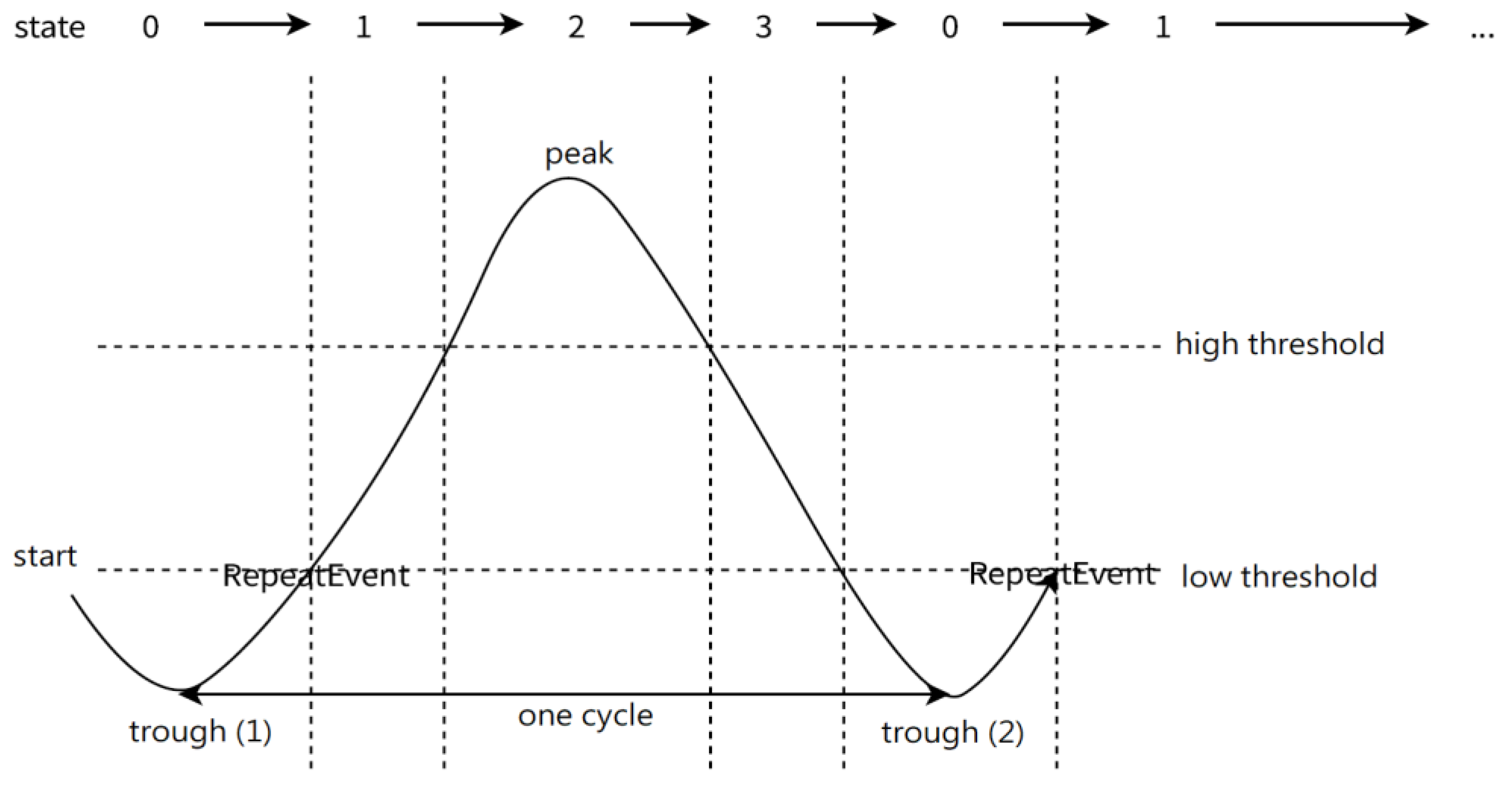
2.2.3. Segment Algorithm
2.2.4. ExerciseBloc
2.2.5. Dynamic Time Warping (DTW) [25]
3. Results
3.1. Hardware
3.2. Real-Time Motion Display Interface
- A humanoid avatar screen, as shown in Figure 16: This screen automatically displays the real-time humanoid avatar movements and fitness activity data, including the current activity recognition result, number of sets, number of repetitions, calories consumed, and accumulative exercise time. The activity recognition is based on the TensorFlow Lite model deployed on the smartphone.
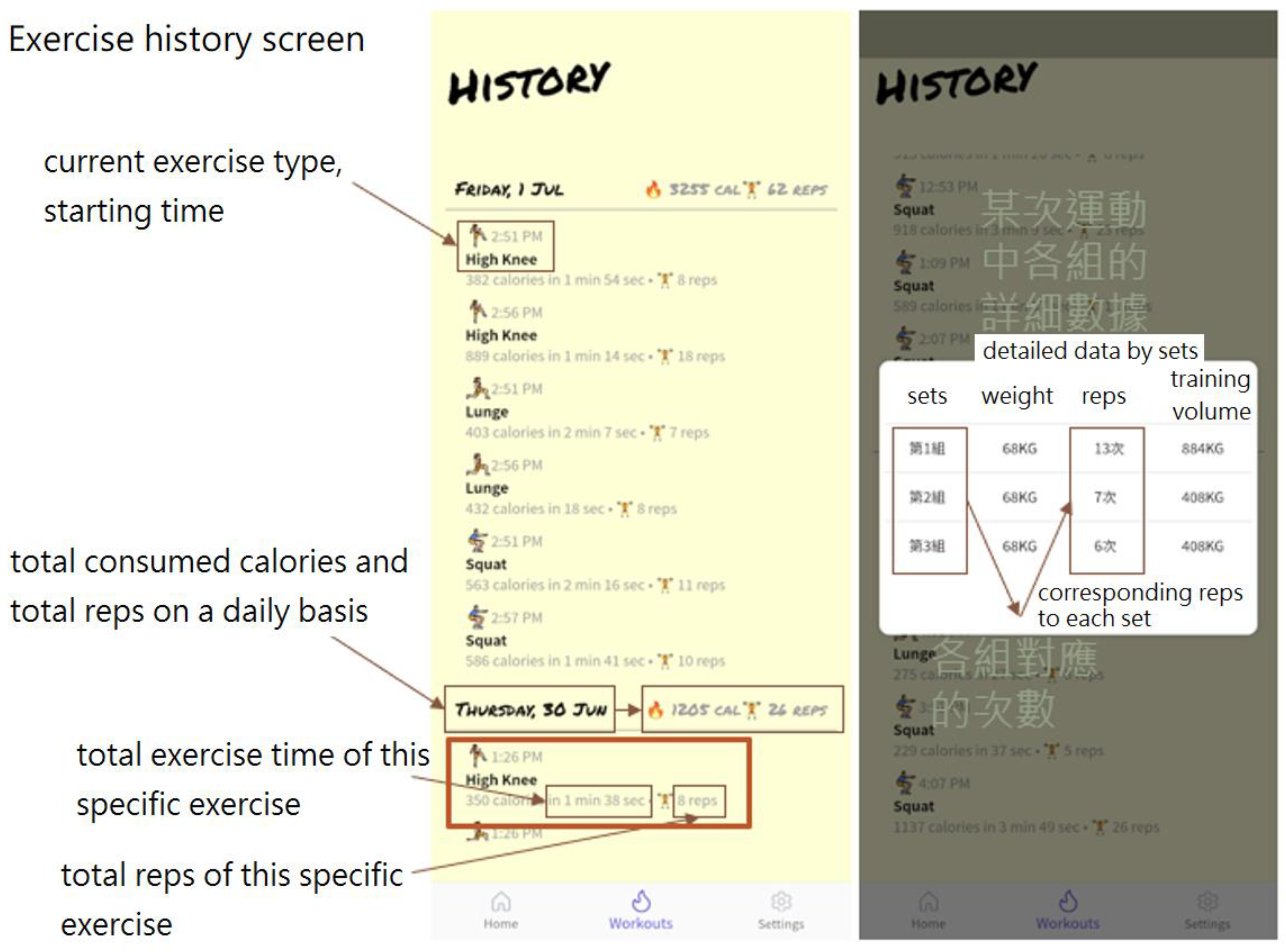
- An exercise history screen, as shown in Figure 17: This screen allows the user to view the historical exercise records on a daily basis or on a specific exercise.
3.3. Fitness Activity Recognition (FAR)-LSTM
3.4. DTW
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Report on Disability. Available online: http://www.who.int/disabilities/world_report/2011/en/ (accessed on 25 November 2022).
- Rehabilitation Treatment for Stroke, Taichung Veterans General Hospital. 28 June 2023. Available online: https://www.vghtc.gov.tw/UnitPage/RowViewDetail?WebRowsID=320a1b6f-2d3f-4a49-9fa2-7e72195e62a0&UnitID=642b65b8-ac30-4ef9-86de-dc3af9211d3e&CompanyID=e8e0488e-54a0-44bf-b10c-d029c423f6e7&UnitDefaultTemplate=1 (accessed on 19 November 2023).
- G.W.H.O. Rehabilitation 2030 Initiative. 2017. Available online: https://www.who.int/initiatives/rehabilitation-2030 (accessed on 24 January 2024).
- Komaris, D.-S.; Tarfali, G.; O’flynn, B.; Tedesco, S. Unsupervised IMU-based evaluation of at-home exercise programmes: A feasibility study. BMC Sports Sci. Med. Rehabil. 2022, 14, 28. [Google Scholar] [CrossRef]
- Health Quality Ontario. Physiotherapy Rehabilitation after Total Knee or Hip Replacement: An Evidence-based Analysis. Ont. Health Technol. Assess. Ser. 2005, 5, 1–91. [Google Scholar]
- Jordan, K.M.; Arden, N.K.; Doherty, M.; Bannwarth, B.; Bijlsma, J.W.J.; Dieppe, P.; Gunther, K.; Hauselmann, H.; Herrero-Beaumont, G.; Kaklamanis, P.; et al. EULAR Recommendations 2003: An evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann. Rheum. Dis. 2003, 62, 1145–1155. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Molina, G.; Reichenbach, S.; Zhang, B.; LaValley, M.; Felson, D.T. Effect of Therapeutic Exercise for Hip Osteoarthritis Pain: Results of a Meta-analysis. Arthritis Care Res. 2008, 59, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- ITU Internet Report 2005: The Internet of Things. Available online: https://www.itu.int/net/wsis/tunis/newsroom/stats/The-Internet-of-Things-2005.pdf (accessed on 25 November 2022).
- Vishnu, S.; Ramson, S.J.; Jegan, R. Internet of Medical Things (IoMT)—An overview. In Proceedings of the 2020 5th International Conference on Devices, Circuits and Systems (ICDCS), Coimbatore, India, 5–6 March 2020. [Google Scholar]
- Fox, J.; Donnellan, A.; Doumen, L. The Deployment of an IoT Network Infrastructure, as a Localised Regional Service. In Proceedings of the 2019 IEEE 5th World Forum on Internet of Things (WF-IoT), Limerick, Ireland, 15–18 April 2019. [Google Scholar]
- Firouzi, F.; Rahmani, A.M.; Mankodiya, K.; Badaroglu, M.; Merrett, G.V.; Wong, P.; Farahani, B. Internet-of-Things and Big Data for Smarter Healthcare: From Device to Architecture, Applications and Analytics. Future Gener. Comput. Syst. 2018, 78, 583–586. [Google Scholar] [CrossRef]
- Pulkkis, G.; Karlsson, J.; Westerlund, M.; Tana, J. Secure and Reliable Internet of Things Systems for Healthcare. In Proceedings of the IEEE 5th International Conference on Future Internet of Things and Cloud (FiCloud), Prague, Czech Republic, 21–23 August 2017. [Google Scholar]
- Xu, B.; Xu, L.-D.; Cai, H.; Xie, C.; Hu, J.; Bu, F. Ubiquitous Data Accessing Method in IoT-Based Information System for Emergency Medical Services. IEEE Trans. Ind. Inform. 2014, 10, 1578–1586. [Google Scholar]
- Chang, C.S.; Wu, T.H.; Wu, Y.C.; Han, C.C. Bluetooth-Based Healthcare Information and Medical Resource Management Systgem. Sensors 2023, 23, 5389. [Google Scholar] [CrossRef]
- Chen, C.J.; Lin, Y.T.; Lin, C.C.; Chen, Y.C.; Lee, Y.J.; Wang, C.Y. Rehabilitation System for Limbs using IMUs. In Proceedings of the 2020 21st International Symposium on Quality Electronic Design (ISQED), Santa Clara, CA, USA, 25–26 March 2020. [Google Scholar]
- Wu, Y.C.; Lin, S.X.; Lin, J.Y.; Han, C.C.; Chang, C.S.; Jiang, J.X. Development of AI Algorithm for Weight Training Using Inertial Measurement Units. Appl. Sci. 2022, 12, 1422. [Google Scholar] [CrossRef]
- Lin, Y.T.; Chen, C.J.; Kuo, P.Y.; Lee, S.H.; Lin, C.C.; Lee, Y.J.; Li, Y.T.; Chen, Y.C.; Wang, C.Y. An IMU-aided Fitness System. In Proceedings of the 2021 IEEE 34th International System-on-Chip Conference (SOCC), Las Vegas, NV, USA, 14–17 September 2021. [Google Scholar]
- Schlage, N.; Kitzig, A.; Stockmanns, G.; Naroska, E.; Schlage, N.; Kitzig, A.; Stockmanns, G.; Naroska, E. Development of a Mobile, Cost-effective and Easy to Use Inertial Motion Capture System for Monitoring in Rehabilitation Applications. Curr. Dir. Biomed. Eng. 2021, 7, 586–589. [Google Scholar] [CrossRef]
- Xsens Dots Precision Motion Tracking. Available online: https://www.xsens.com/xsens-dot (accessed on 26 January 2024).
- Qualisys. Available online: https://www.qualisys.com/ (accessed on 26 January 2024).
- KneTex. Available online: https://knetex.hsnr.de/ (accessed on 26 January 2024).
- Müller, P.N.; Müller, A.J.; Achenbach, P.; Stefan Göbel, S. IMU-Based Fitness Activity Recognition Using CNNs for Time Series Classification. Sensors 2024, 24, 742. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://flowduino.com/2021/08/24/arduino-nano-r3-nrf24l01-rf-nano/ (accessed on 5 March 2024).
- Available online: https://infocenter.nordicsemi.com/pdf/nRF24L01P_PS_v1.0.pdf?cp=10_4_0_0 (accessed on 5 March 2024).
- Alizadeh, E. An Introduction to Dynamic Time Warping. Available online: https://builtin.com/data-science/dynamic-time-warping (accessed on 30 January 2024).
- Tedesco, S.; Torre, O.M.; Belcastro, M.; Torchia, P.; Alfieri, D.; Khokhlova, L.; Komaris, S.D.; O’Flynn, B. Design of a Multi-Sensors Wearable Platform for Remote Monitoring of Knee Rehabilitation. IEEE Access 2022, 10, 98309–98328. [Google Scholar] [CrossRef]
- InBody. Available online: https://inbodyusa.com/ (accessed on 1 February 2024).























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GPIO Pin Number (Nano R3) | nRF24L01+ SPI |
|---|---|
| D9 | CE (Chip Enable) |
| D10 | CS/CSN (Chip Select) |
| D11 | MOSI |
| D12 | MISO |
| D13 | SCK |
| Participant No. | Accuracy |
|---|---|
| 1 | 0.94 |
| 2 | 0.99 |
| 3 | 0.99 |
| 4 | 0.95 |
| 5 | 1.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-J.; Chang, C.-S.; Wu, Y.-C.; Han, C.-C.; Cheng, Y.-Y.; Chen, H.-M. Development of Wearable Devices for Collecting Digital Rehabilitation/Fitness Data from Lower Limbs. Sensors 2024, 24, 1935. https://doi.org/10.3390/s24061935
Huang Y-J, Chang C-S, Wu Y-C, Han C-C, Cheng Y-Y, Chen H-M. Development of Wearable Devices for Collecting Digital Rehabilitation/Fitness Data from Lower Limbs. Sensors. 2024; 24(6):1935. https://doi.org/10.3390/s24061935
Chicago/Turabian StyleHuang, Yu-Jung, Chao-Shu Chang, Yu-Chi Wu, Chin-Chuan Han, Yuan-Yang Cheng, and Hsian-Min Chen. 2024. "Development of Wearable Devices for Collecting Digital Rehabilitation/Fitness Data from Lower Limbs" Sensors 24, no. 6: 1935. https://doi.org/10.3390/s24061935