
Detecting Movement Changes in Children with Hemiparesis after Upper Limb Therapies: A Responsiveness Analysis of a 3D Bimanual Protocol
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical and Regulatory Considerations
2.2. Participants
2.3. Interventions
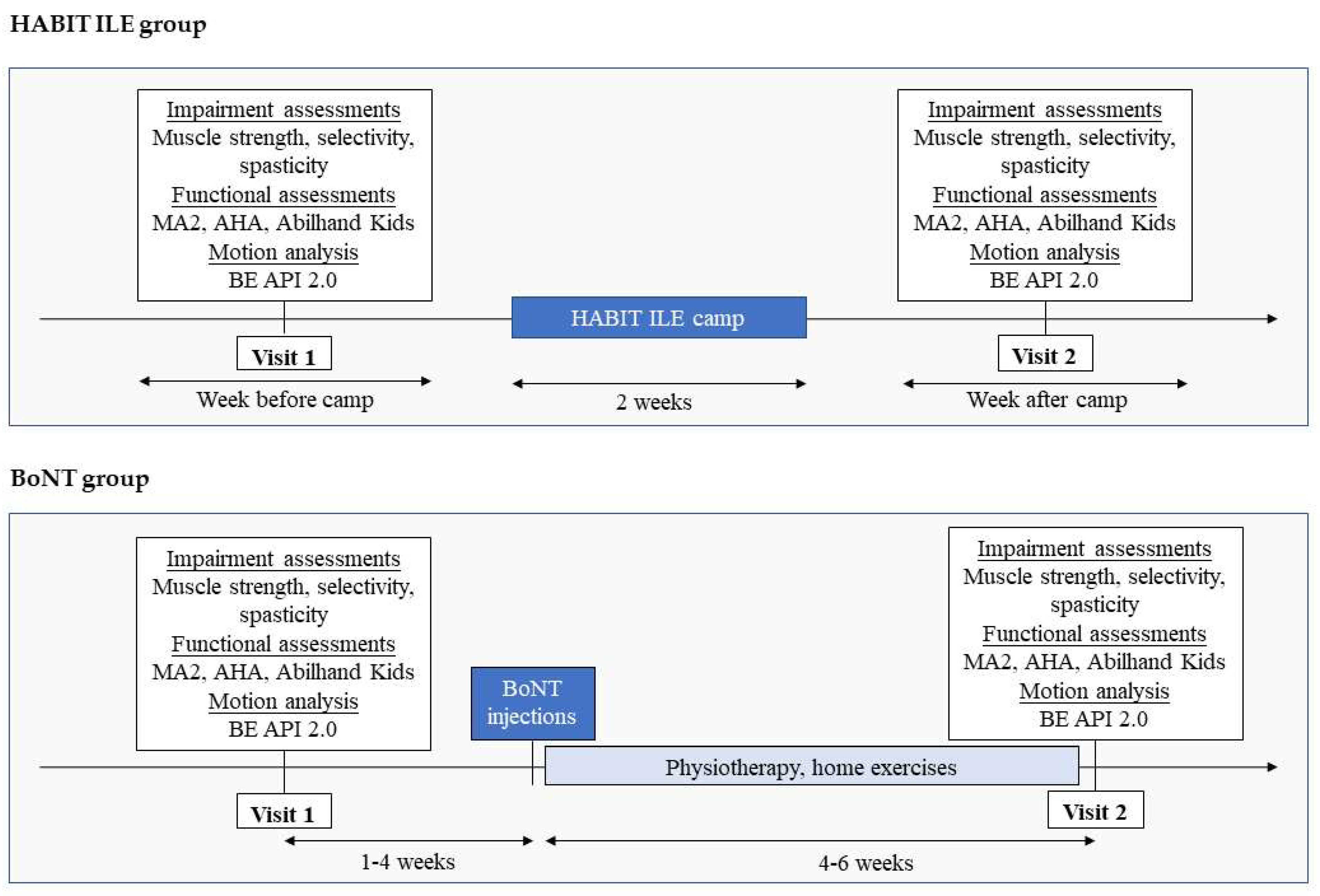
2.4. Study Schedule
2.5. Clinical Assessments
2.6. 3D Motion Analysis
2.6.1. BE API 2.0 Protocol
2.6.2. Motion Capture and Data Processing
2.6.3. Data Analysis
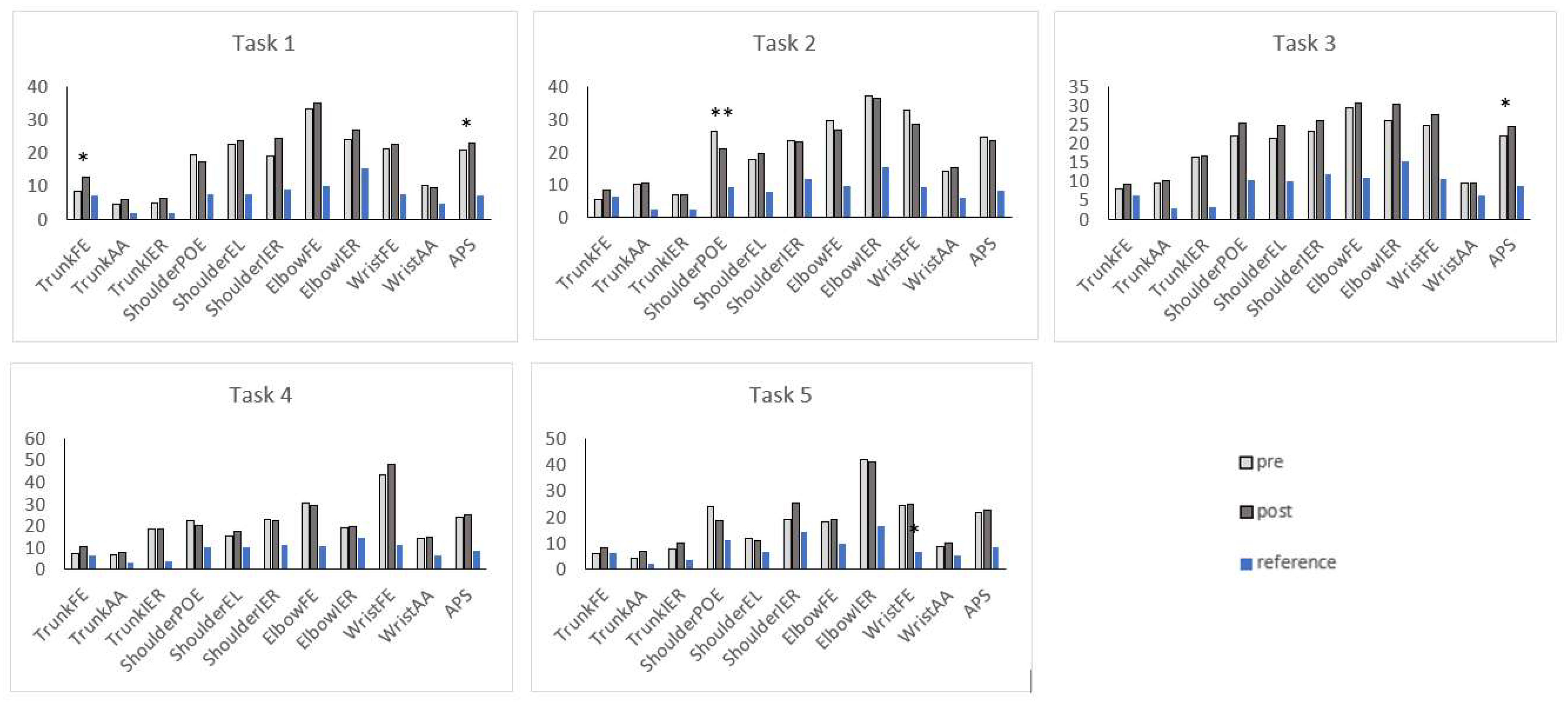
- The Arm Variable Scores (AVS) [29] were calculated using the root-mean-square error (RMSE) between the point-by-point comparison of each joint angle of each child and the mean value for the same joint angle from a reference database of 20 typically developing children (TDC) included in a previous study [16]. A total of 10 AVS were calculated for each task: the trunk (flexion/extension, abduction/adduction, axial rotation), the shoulder (plane of elevation, elevation, rotation), the elbow (flexion/extension, pronation/supination), and the wrist (flexion/extension, abduction/adduction). The global AVS of each joint angle was calculated by averaging the AVS values for the five tasks.
- The Arm Profile Score (APS) is a kinematic index that reflects the total movement deviation of the UL during each task [29]. It was calculated by averaging the RMSE of the 10 joint angles during each task (10 AVS) and compared to the reference population (TDC group). The global APS was calculated by averaging the APS values for the five tasks.
- The kinematic waveforms of each DoF were calculated by computing the mean angular value of the four cycles at each time point of the time-normalized (0–100%) movement cycles for each task.
2.7. Number of Participants
2.8. Statistical Analysis
3. Results
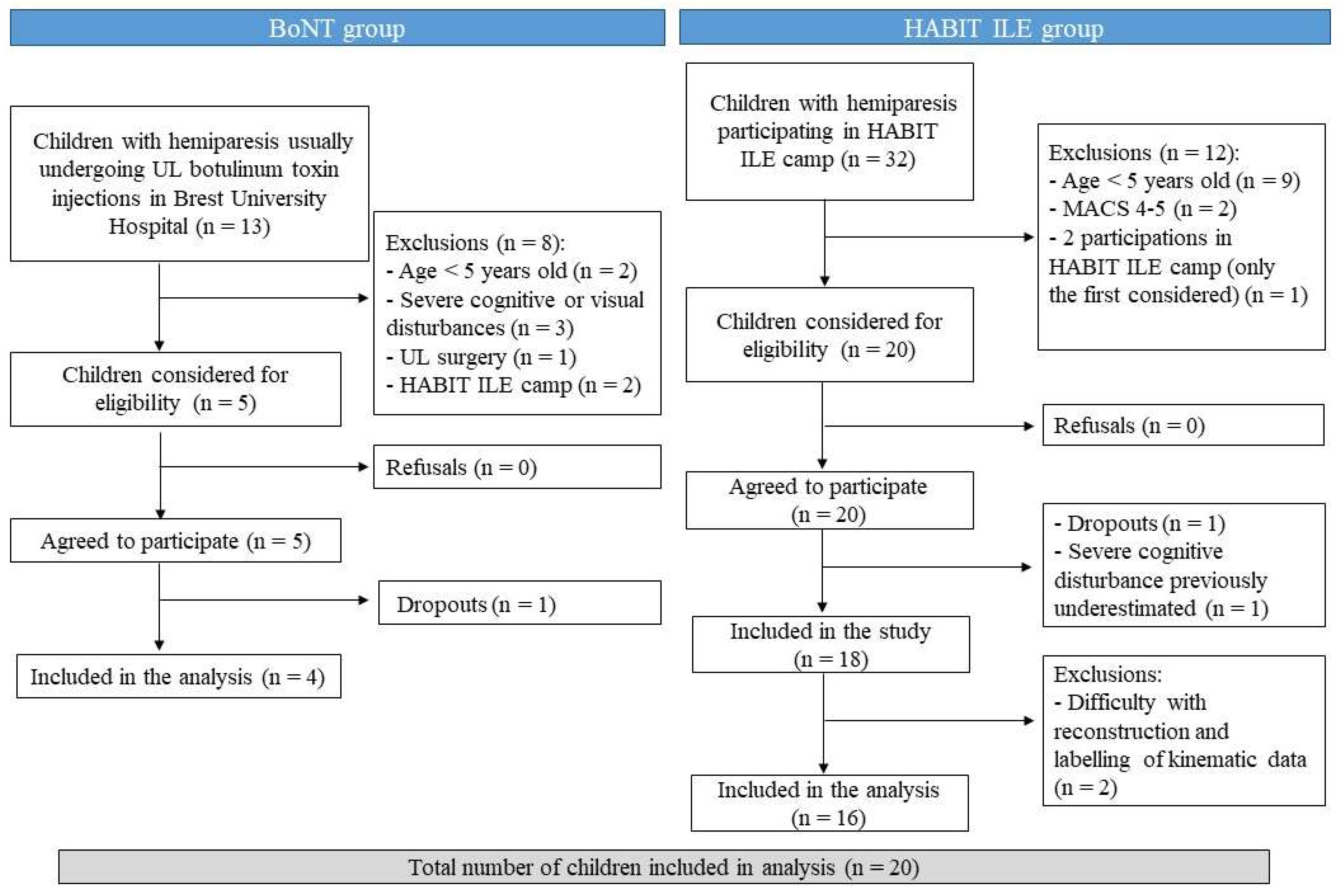
3.1. Participants
3.2. Comparison of Clinical Scores Pre- and Post-Intervention
3.2.1. Individual Analysis
3.2.2. Group Analysis (HABIT ILE Group)
3.3. Comparison of Kinematic Movement Patterns of the Impaired UL Pre- and Post-Intervention
3.3.1. Individual Analysis
3.3.2. Group Analysis (HABIT ILE Group)
3.4. Comparison of IOC and SPARC of the Impaired UL Pre- and Post-Intervention
3.4.1. Individual Analysis
3.4.2. Group Analysis (HABIT ILE Group)
3.5. Correlations between Changes in Kinematics and Clinical Assessment Scores
4. Discussion
4.1. Different Kinematic Changes Detected in Each Child after the Interventions
4.2. Proximal Kinematic Changes Post-Intervention Detected by the Group Level Analysis
4.3. No Change Detected in Quality of Movement Post-Intervention
4.4. Relationship between Changes in Movement Deviations and Function
4.5. Limits
4.6. Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, T.-N.; Howe, T.-H.; Liang, K.-J.; Chang, T.-W.; Shieh, J.-Y.; Chen, H.-L. Bimanual motor performance in everyday life activities of children with hemiplegic cerebral palsy. Eur. J. Phys. Rehabil. Med. 2021, 57, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Namara, M.M.; Paton, M.C.B.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef] [PubMed]
- Krumlinde-Sundholm, L.; Holmefur, M.; Kottorp, A.; Eliasson, A.-C. The Assisting Hand Assessment: Current evidence of validity, reliability, and responsiveness to change. Dev. Med. Child. Neurol. 2007, 49, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Arnould, C.; Penta, M.; Renders, A.; Thonnard, J.-L. ABILHAND-Kids: A measure of manual ability in children with cerebral palsy. Neurology 2004, 63, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Hebda-Boon, A.; Tan, X.-L.; Tillmann, R.; Shortland, A.P.; Firth, G.B.; Morrissey, D. The impact of instrumented gait analysis on decision-making in the interprofessional management of cerebral palsy: A scoping review. Eur. J. Paediatr. Neurol. 2023, 42, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Fitoussi, F.; Diop, A.; Maurel, N.; Laasel, E.M.; Ilharreborde, B.; Penneçot, G.F. Upper limb motion analysis in children with hemiplegic cerebral palsy: Proximal kinematic changes after distal botulinum toxin or surgical treatments. J. Child. Orthop. 2011, 5, 363–370. [Google Scholar] [CrossRef]
- Mackey, A.H.; Miller, F.; Walt, S.E.; Waugh, M.-C.; Stott, N.S. Use of three-dimensional kinematic analysis following upper limb botulinum toxin A for children with hemiplegia. Eur. J. Neurol. 2008, 15, 1191–1198. [Google Scholar] [CrossRef]
- Simon-Martinez, C.; Mailleux, L.; Hoskens, J.; Ortibus, E.; Jaspers, E.; Wenderoth, N.; Feys, H. Randomized controlled trial combining constraint-induced movement therapy and action-observation training in unilateral cerebral palsy: Clinical effects and influencing factors of treatment response. Ther. Adv. Neurol. Disord. 2020, 13, 1756286419898065. [Google Scholar] [CrossRef]
- Hung, Y.-C.; Casertano, L.; Hillman, A.; Gordon, A.M. The effect of intensive bimanual training on coordination of the hands in children with congenital hemiplegia. Res. Dev. Disabil. 2011, 32, 2724–2731. [Google Scholar] [CrossRef]
- Hung, Y.-C.; Brandão, M.B.; Gordon, A.M. Structured skill practice during intensive bimanual training leads to better trunk and arm control than unstructured practice in children with unilateral spastic cerebral palsy. Res. Dev. Disabil. 2017, 60, 65–76. [Google Scholar] [CrossRef]
- Hung, Y.-C.; Ferre, C.L.; Gordon, A.M. Improvements in Kinematic Performance After Home-Based Bimanual Intensive Training for Children with Unilateral Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2018, 38, 370–381. [Google Scholar] [CrossRef] [PubMed]
- Smorenburg, A.R.P.; Ledebt, A.; Deconinck, F.J.A.; Savelsbergh, G.J.P. Practicing a matching movement with a mirror in individuals with spastic hemiplegia. Res. Dev. Disabil. 2013, 34, 2507–2513. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, M.; Loos, A.; Lempereur, M.; Brochard, S. Bimanual movements in children with cerebral palsy: A systematic review of instrumented assessments. J. Neuroeng. Rehabil. 2023, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.M.; Schneider, J.A.; Chinnan, A.; Charles, J.R. Efficacy of a hand-arm bimanual intensive therapy (HABIT) in children with hemiplegic cerebral palsy: A randomized control trial. Dev. Med. Child. Neurol. 2007, 49, 830–838. [Google Scholar] [CrossRef]
- Gaillard, F.; Cacioppo, M.; Bouvier, B.; Bouzille, G.; Newman, C.J.; Pasquet, T.; Bonan, I. Assessment of bimanual performance in 3-D movement analysis: Validation of a new clinical protocol in children with unilateral cerebral palsy. Ann. Phys. Rehabil. Med. 2020, 63, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, M.; Marin, A.; Rauscent, H.; Le Pabic, E.; Gaillard, F.; Brochard, S.; Bonan, I. A new child-friendly 3D bimanual protocol to assess upper limb movement in children with unilateral cerebral palsy: Development and validation. J. Electromyogr. Kinesiol. 2020, 55, 102481. [Google Scholar] [CrossRef]
- Bleyenheuft, Y.; Gordon, A.M. Hand-arm bimanual intensive therapy including lower extremities (HABIT-ILE) for children with cerebral palsy. Phys. Occup. Ther. Pediatr. 2014, 34, 390–403. [Google Scholar] [CrossRef]
- Bleyenheuft, Y.; Arnould, C.; Brandao, M.B.; Bleyenheuft, C.; Gordon, A.M. Hand and Arm Bimanual Intensive Therapy Including Lower Extremity (HABIT-ILE) in Children with Unilateral Spastic Cerebral Palsy: A Randomized Trial. Neurorehabil. Neural. Repair. 2015, 29, 645–657. [Google Scholar] [CrossRef]
- Masson, E. Traitements Médicamenteux de la Spasticité: Recommandations de Bonnes Pratiques Juin 2009. EM-Consulte n.d. Available online: https://www.em-consulte.com/article/247632/traitements-medicamenteux-de-la-spasticite-recomma (accessed on 29 July 2020).
- Hoare, B.; Imms, C.; Villanueva, E.; Rawicki, H.B.; Matyas, T.; Carey, L. Intensive therapy following upper limb botulinum toxin A injection in young children with unilateral cerebral palsy: A randomized trial. Dev. Med. Child. Neurol. 2013, 55, 238–247. [Google Scholar] [CrossRef]
- Bourke-Taylor, H. Melbourne Assessment of Unilateral Upper Limb Function: Construct validity and correlation with the Pediatric Evaluation of Disability Inventory. Dev. Med. Child. Neurol. 2003, 45, 92–96. [Google Scholar] [CrossRef]
- Bard, R.; Chaléat-Valayer, E.; Combey, A.; Bleu, P.E.; Perretant, I.; Bernard, J.-C. Upper limb assessment in children with cerebral palsy: Translation and reliability of the French version for the Melbourne unilateral upper limb assessment (test de Melbourne). Ann. Phys. Rehabil. Med. 2009, 52, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Paternostro-Sluga, T.; Grim-Stieger, M.; Posch, M.; Schuhfried, O.; Vacariu, G.; Mittermaier, C.; Fialka-Moser, V. Reliability and validity of the Medical Research Council (MRC) scale and a modified scale for testing muscle strength in patients with radial palsy. J. Rehabil. Med. 2008, 40, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, A.; Livanelioglu, A.; Gunel, M.K. Reliability of Ashworth and Modified Ashworth scales in children with spastic cerebral palsy. BMC Musculoskelet. Disord. 2008, 9, 44. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, M.; Lempereur, M.; Marin, A.; Rauscent, H.; Crétual, A.; Brochard, S.; Bonan, I. Motor patterns of the impaired upper limb in children with unilateral cerebral palsy performing bimanual tasks. Clin. Biomech. 2022, 97, 105710. [Google Scholar] [CrossRef]
- Simon-Martinez, C.; Jaspers, E.; Mailleux, L.; Desloovere, K.; Vanrenterghem, J.; Ortibus, E.; Klingels, K. Negative Influence of Motor Impairments on Upper Limb Movement Patterns in Children with Unilateral Cerebral Palsy. A Statistical Parametric Mapping Study. Front. Hum. Neurosci. 2017, 11, 482. [Google Scholar] [CrossRef]
- Wu, G.; Van der Helm, F.C.; Veeger, H.D.; Makhsous, M.; Van Roy, P.; Anglin, C.; Buchholz, B. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion–Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Lempereur, M.; Leboeuf, F.; Brochard, S.; Rousset, J.; Burdin, V.; Rémy-Néris, O. In vivo estimation of the glenohumeral joint centre by functional methods: Accuracy and repeatability assessment. J. Biomech. 2010, 43, 370–374. [Google Scholar] [CrossRef]
- Jaspers, E.; Feys, H.; Bruyninckx, H.; Klingels, K.; Molenaers, G.; Desloovere, K. The Arm Profile Score: A new summary index to assess upper limb movement pathology. Gait Posture 2011, 34, 227–233. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Melendez-Calderon, A.; Roby-Brami, A.; Burdet, E. On the analysis of movement smoothness. J. Neuroeng. Rehabil. 2015, 12, 1–12. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Melendez-Calderon, A.; Burdet, E. A robust and sensitive metric for quantifying movement smoothness. IEEE Trans. Biomed. Eng 2012, 59, 2126–2136. [Google Scholar] [CrossRef]
- Butler, E.E.; Ladd, A.L.; LaMont, L.E.; Rose, J. Temporal–spatial parameters of the upper limb during a Reach & Grasp Cycle for children. Gait Posture 2010, 32, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, E.; Feys, H.; Bruyninckx, H.; Harlaar, J.; Molenaers, G.; Desloovere, K. Upper limb kinematics: Development and reliability of a clinical protocol for children. Gait Posture 2011, 33, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Anselmi, P.; Vidotto, G.; Bettinardi, O.; Bertolotti, G. Measurement of change in health status with Rasch models. Health Qual. Life Outcomes 2015, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Paradis, J.; Arnould, C.; Thonnard, J.L.; Houx, L.; Pons-Becmeur, C.; Renders, A.; Bleyenheuft, Y. Responsiveness of the ACTIVLIM-CP questionnaire: Measuring global activity performance in children with cerebral palsy. Dev. Med. Child. Neurol. 2018, 60, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Pataky, T.C. Generalized n-dimensional biomechanical field analysis using statistical parametric mapping. J. Biomech. 2010, 43, 1976–1982. [Google Scholar] [CrossRef]
- Pataky, T.C. One-dimensional statistical parametric mapping in Python. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 295–301. [Google Scholar] [CrossRef]
- Dralle, H.; Machens, A.; Basa, J.; Fatourechi, V.; Franceschi, S.; Hay, I.D.; Sherman, S.I. Cerebral palsy. Nat. Rev. Dis. Prim. 2016, 2, 15082. [Google Scholar] [CrossRef]
- Damiano, D.L. Meaningfulness of mean group results for determining the optimal motor rehabilitation program for an individual child with cerebral palsy. Dev. Med. Child. Neurol. 2014, 56, 1141–1146. [Google Scholar] [CrossRef]
- Cope, S.M.; Liu, X.-C.; Verber, M.D.; Cayo, C.; Rao, S.; Tassone, J.C. Upper limb function and brain reorganization after constraint-induced movement therapy in children with hemiplegia. Dev. Neurorehabilit. 2010, 13, 19–30. [Google Scholar] [CrossRef]
- Simon-Martinez, C.; Mailleux, L.; Jaspers, E.; Ortibus, E.; Desloovere, K.; Klingels, K.; Feys, H. Effects of combining constraint-induced movement therapy and action-observation training on upper limb kinematics in children with unilateral cerebral palsy: A randomized controlled trial. Sci. Rep. 2020, 10, 10421. [Google Scholar] [CrossRef]
- Saussez, G.; Brandão, M.B.; Gordon, A.M.; Bleyenheuft, Y. Including a Lower-Extremity Component during Hand-Arm Bimanual Intensive Training does not Attenuate Improvements of the Upper Extremities: A Retrospective Study of Randomized Trials. Front. Neurol. 2017, 8, 495. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, F.; Cretual, A.; Cordillet, S.; Le Cornec, C.; Gonthier, C.; Bouvier, B.; Rauscent, H. Kinematic motion abnormalities and bimanual performance in children with unilateral cerebral palsy. Dev. Med. Child Neurol. 2018, 60, 839–845. [Google Scholar] [CrossRef]
- Mailleux, L.; Jaspers, E.; Ortibus, E.; Simon-Martinez, C.; Desloovere, K.; Molenaers, G.; Feys, H. Clinical assessment and three-dimensional movement analysis: An integrated approach for upper limb evaluation in children with unilateral cerebral palsy. PLoS ONE 2017, 12, e0180196. [Google Scholar] [CrossRef]
- Butler, E.E.; Ladd, A.L.; Louie, S.A.; Lamont, L.E.; Wong, W.; Rose, J. Three-dimensional kinematics of the upper limb during a Reach and Grasp Cycle for children. Gait Posture 2010, 32, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, E.; Desloovere, K.; Bruyninckx, H.; Klingels, K.; Molenaers, G.; Aertbeliën, E.; Feys, H. Three-dimensional upper limb movement characteristics in children with hemiplegic cerebral palsy and typically developing children. Res. Dev. Disabil. 2011, 32, 2283–2294. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-C.; Chen, C.-L.; Kang, L.-J.; Wu, C.-Y.; Chen, F.-C.; Hong, W.-H. Improvement of upper extremity motor control and function after home-based constraint induced therapy in children with unilateral cerebral palsy: Immediate and long-term effects. Arch. Phys. Med. Rehabil. 2014, 95, 1423–1432. [Google Scholar] [CrossRef]
- Mohamed Refai, M.I.; Saes, M.; Scheltinga, B.L.; van Kordelaar, J.; Bussmann, J.B.; Veltink, P.H.; Van Beijnum, B.J.F. Smoothness metrics for reaching performance after stroke. Part 1: Which one to choose? J. Neuroeng. Rehabil. 2021, 18, 154. [Google Scholar] [CrossRef]
- Germanotta, M.; Iacovelli, C.; Aprile, I. Evaluation of Gait Smoothness in Patients with Stroke Undergoing Rehabilitation: Comparison between Two Metrics. Int. J. Environ. Res. Public Health 2022, 19, 13440. [Google Scholar] [CrossRef]
- Steenbergen, B.; Hulstijn, W.; de Vries, A.; Berger, M. Bimanual movement coordination in spastic hemiparesis. Exp. Brain Res. 1996, 110, 91–98. [Google Scholar] [CrossRef]
- Zhang, J.; Li, Y.; Xiao, W.; Zhang, Z.; Zhang, E. Non-iterative and Fast Deep Learning: Multilayer Extreme Learning Machines. J. Frankl. Inst. 2020, 357, 8925–8955. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion No. | Age (years) | Sex | Pathology | Cerebral Lesion | Impaired Side | MACS Level | Therapy | Therapy Modalities |
|---|---|---|---|---|---|---|---|---|
| 1 | 9 | F | Stroke | Haemorrhagic stroke (at 7 yo.) | Left | 3 | HABIT ILE | 65 h |
| 2 | 6 | F | CP | Ischaemic stroke | Right | 1 | HABIT ILE | 65 h |
| 3 | 5 | F | CP | Haemorrhagic stroke | Left | 1 | HABIT ILE | 65 h |
| 4 | 7 | M | CP | Ischaemic stroke | Right | 1 | HABIT ILE | 65 h |
| 5 | 5 | M | CP | / | Right | 2 | HABIT ILE | 65 h |
| 6 | 6 | F | CP | Ischaemic stroke | Right | 2 | HABIT ILE | 65 h |
| 7 | 8 | F | CP | Leukomalacia | Right | 1 | HABIT ILE | 65 h |
| 8 | 7 | F | CP | Ischaemic stroke | Right | 2 | HABIT ILE | 65 h |
| 9 | 6 | M | CP | Ischaemic stroke | Right | 1 | HABIT ILE | 65 h |
| 10 | 6 | F | CP | Ischaemic stroke | Right | 3 | HABIT ILE | 65 h |
| 11 | 6 | M | CP | Ischaemic stroke | Right | 2 | HABIT ILE | 65 h |
| 12 | 16 | F | CP | Ischaemic stroke | Right | 2 | BoNT | Triceps Brachii |
| 13 | 14 | F | CP | Ischaemic stroke | Left | 2 | BoNT | Pronators, ulnar & radial flexors, thumb opposors |
| 14 | 14 | M | CP | Ischaemic stroke | Right | 3 | BoNT | Biceps Brachii, pronators |
| 15 | 5 | F | CP | Schizencephaly | Right | 1 | HABIT ILE | 30 h |
| 16 | 6 | M | CP | Ischaemic stroke | Right | 1 | HABIT ILE | 65 h |
| 17 | 7 | F | CP | Malformation | Right | 2 | HABIT ILE | 65 h |
| 18 | 7 | F | CP | / | Right | 3 | HABIT ILE | 65 h |
| 19 | 12 | M | Stroke | Ischaemic stroke (at 10 yo) | Left | 3 | HABIT ILE | 65 h |
| 20 | 17 | M | CP | Ischaemic stroke | Left | 2 | BoNT | Biceps Brachii, pronators, ulnar & radial flexors |
| HABIT ILE Group | Pre-Intervention (n = 16) | Post- Intervention (n = 16) | Mean Difference [SD] | p-Value | Cohen’s d |
|---|---|---|---|---|---|
| Clinical outcomes | |||||
| Strength (/80) | 62.3 [9.3] | 65.9 [7.5] | 3.5 [5.6] | 0.03 | −0.63 |
| Spasticity (/80) | 3.3 [4.3] | 3.2 [3.6] | −0.1 [3.1] | 0.87 | 0.04 |
| Selectivity (/32) | 28.0 [4.8] | 29.7 [4.0] | 1.8 [2.2] | 0.01 | −0.96 |
| Functional outcomes | |||||
| AHA (AHA-units/100) | 54.6 [9] | 57.9 [8.6] | 3.3 [4.9] | 0.03 | −0.67 |
| MA2 (%) | 59.9 [17.8] | 67.6 [14.1] | 7.7 [18.1] | 0.17 W | −0.43 |
| Global Deviations | Pre-Intervention (°) | Post- Intervention (°) | Mean Difference [95% CI] | p-Value | Effect Size | |
|---|---|---|---|---|---|---|
| HI group | Trunk FE | 7.1 [2.4] | 9.7 [4.8] | 2.7 [0.4–5] | 0.03 | −0.62 |
| Trunk AA | 6.9 [1.6] | 8.2 [4.2] | 1.2 [−0.8–3.2] | 0.25 W | −0.34 | |
| Trunk IER | 10.7 [2.7] | 11.8 [3.5] | 1.3 [−0.8–3] | 0.24 | −0.31 | |
| Shoulder POE | 22.5 [6.4] | 20.5 [4.9] | −2 [−5.4–1.3] | 0.22 | 0.32 | |
| Shoulder El | 17.7 [5.6] | 19.1 [5.3] | 1.4 [−0.5–3.4] | 0.14 | −0.40 | |
| Shoulder IER | 21.5 [6.5] | 24.2 [8.9] | 2.7 [−1.4–6.9] | 0.43 W | −0.24 | |
| Elbow FE | 27.8 [7.2] | 28.3 [5.9] | 0.5 [−2.5–3.6] | 0.71 | −0.09 | |
| Elbow IER | 29.9 [8.1] | 31.1 [9.5] | 1.2 [−1–3.3] | 0.26 | −0.30 | |
| Wrist FE | 27.7 [9.2] | 30.3 [12.7] | 2.6 [−1.3–6.5] | 0.50 W | −0.21 | |
| Wrist AA | 11.6 [3.7] | 12 [4.6] | 0.4 [−1.5–2.2] | 0.63 W | 0.15 | |
| APS | 22.3 [3.2] | 23.7 [3.1] | 1.4 [0.3–2.5] | 0.02 | −0.68 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cacioppo, M.; Lempereur, M.; Houx, L.; Bouvier, S.; Bailly, R.; Brochard, S. Detecting Movement Changes in Children with Hemiparesis after Upper Limb Therapies: A Responsiveness Analysis of a 3D Bimanual Protocol. Sensors 2023, 23, 4235. https://doi.org/10.3390/s23094235
Cacioppo M, Lempereur M, Houx L, Bouvier S, Bailly R, Brochard S. Detecting Movement Changes in Children with Hemiparesis after Upper Limb Therapies: A Responsiveness Analysis of a 3D Bimanual Protocol. Sensors. 2023; 23(9):4235. https://doi.org/10.3390/s23094235
Chicago/Turabian StyleCacioppo, Marine, Mathieu Lempereur, Laetitia Houx, Sandra Bouvier, Rodolphe Bailly, and Sylvain Brochard. 2023. "Detecting Movement Changes in Children with Hemiparesis after Upper Limb Therapies: A Responsiveness Analysis of a 3D Bimanual Protocol" Sensors 23, no. 9: 4235. https://doi.org/10.3390/s23094235