
Motion Smoothness-Based Assessment of Surgical Expertise: The Importance of Selecting Proper Metrics

Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Environment
2.2. Participants
2.3. Tasks
- (1)
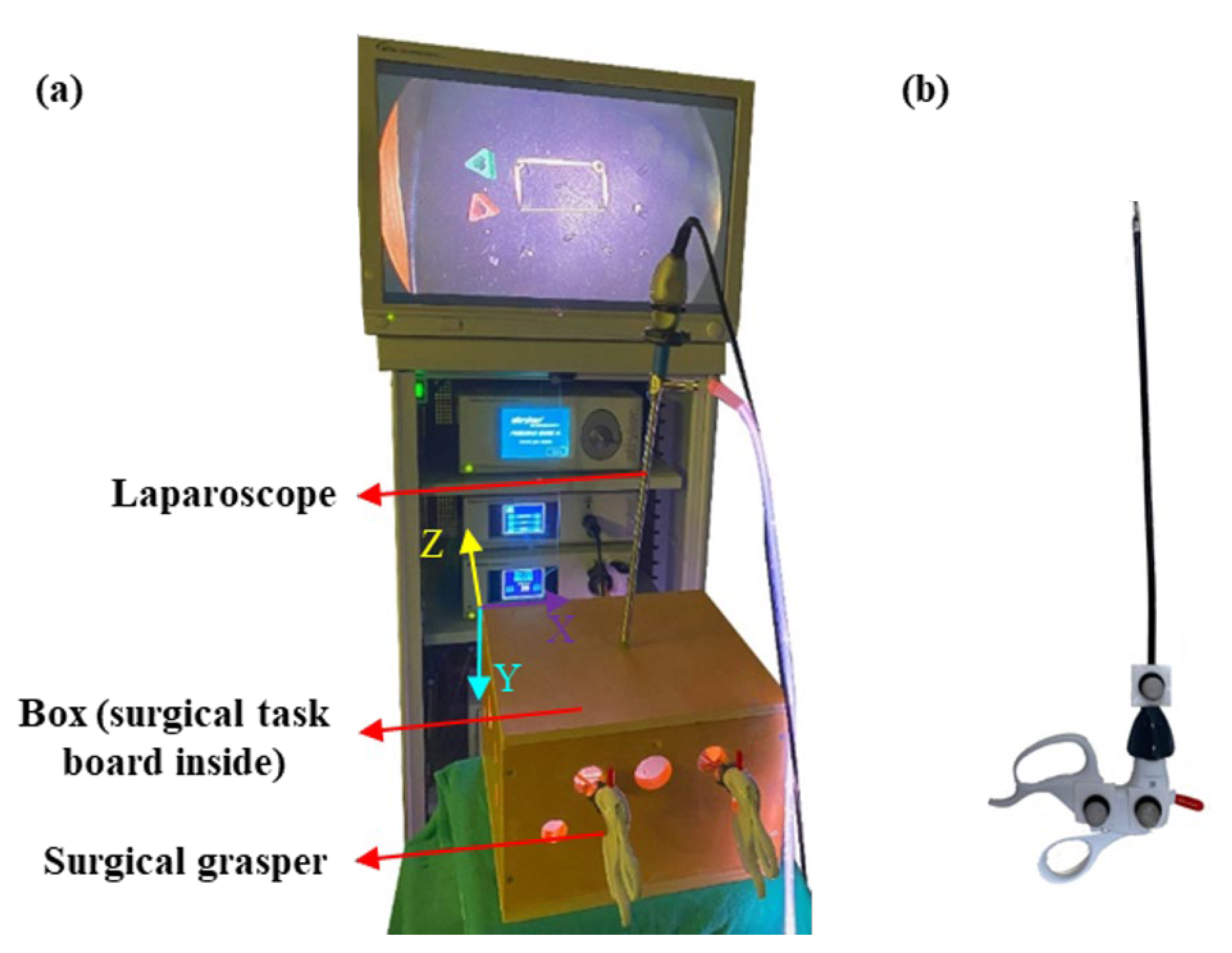
- Peg transfer task: The participants grasped a peg (1.6 × 1.4 × 1.6 cm) from a pin on the task board inside a box (Figure 1a) using the laparoscopic grasper (Ethicon Endo-Surgery, Cincinnati, OH, USA) held in the non-dominant hand. After that, they delivered the peg to the grasper held in the dominant hand, moved it to the target (a pin 10 cm away from the initial pin), and dropped it there. Then, the same procedure was conducted for the second peg. Once the two pegs were placed on the dominant hand’s side, the participants conducted the reverse procedure in order to transfer the pegs back to the original position. The peg transfer task is included in the Fundamentals of Laparoscopic Surgery (FLS) curriculum [25].
- (2)
- Bimanual peg transfer task: Using both surgical graspers held in the dominant and non-dominant hands, the participants grasped the two pegs simultaneously from the non-dominant hand’s side, moved them to the targets (pins 10 cm away from the initial pins’ position), and dropped them there. Afterwards, participants grasped the pegs from the dominant hand’s side and moved them back to the initial positions. This task required a high level of bimanual coordination.
- (3)
- Rubber band translocation task: A rubber band was placed around four pins on the task board, and participants grasped the rubber band with two laparoscopic graspers, translocated the rubber band to the distal pins (5.5 cm away from the initial pins), released the rubber band, re-grasped it, and moved it back to the original position. This task was included as it had tool–tissue interaction that could affect surgical performance. This task also required a high level of bimanual coordination.
2.4. Motion Tracking of Surgical Tooltip
2.5. Motion Smoothness Derivation Algorithms
- (1)
- Mean tooltip motion jerk (J) was defined as the mean value of the magnitude of the tooltip motion jerk (the third time derivative of the tooltip position).
- (2)
- Logarithmic dimensionless tooltip motion jerk (DJ) was derived from tooltip motion jerk converted into a dimensionless metric via normalizing by tooltip path length (PL) and task duration (T). The term in Table 1 has a dimension of ; hence, it is normalized using . This normalization is in accordance with [10,14,24]. Since dimensionless motion jerk values had different orders of magnitude across the skill levels, logarithmic values were used to report the results. To derive this metric, we required the tooltip path length, computed by integrating the tooltip velocity magnitude with respect to time.
- (3)
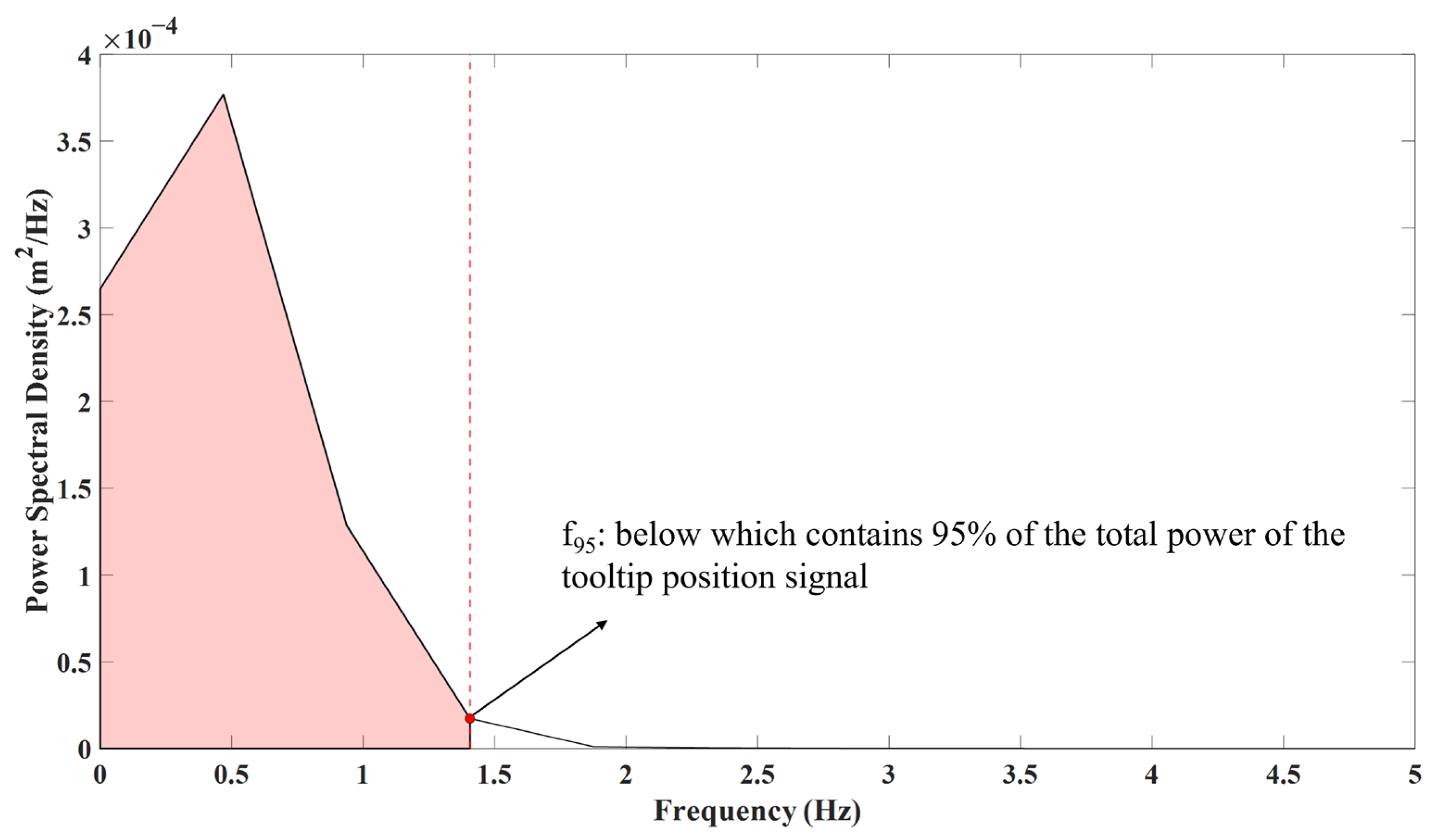
- The 95% tooltip motion frequency (f95%) was calculated in the frequency domain, as opposed to the first two metrics above that were calculated in the time domain. To calculate f95%, we converted the tooltip position data into the frequency domain using the power spectral density of the tooltip position. The power spectral density of the tooltip position was calculated by the pwelch function (10 s Hamming windows and 50% overlap) of MATLAB 2020, implementing Welch’s method. Then, we identified the frequency below which contained 95% of the total power of the tooltip position (Figure 2). We intended not to include the high-frequency and low-amplitude content of the tooltip position signal in the motion smoothness metric calculation, which resulted from the measurement noise. Therefore, we considered 95% of the total power of the tooltip position to derive the motion smoothness metric, neglecting the area under the power spectral density generated from the measurement noise (5%).
2.6. Statistical Analysis
3. Results
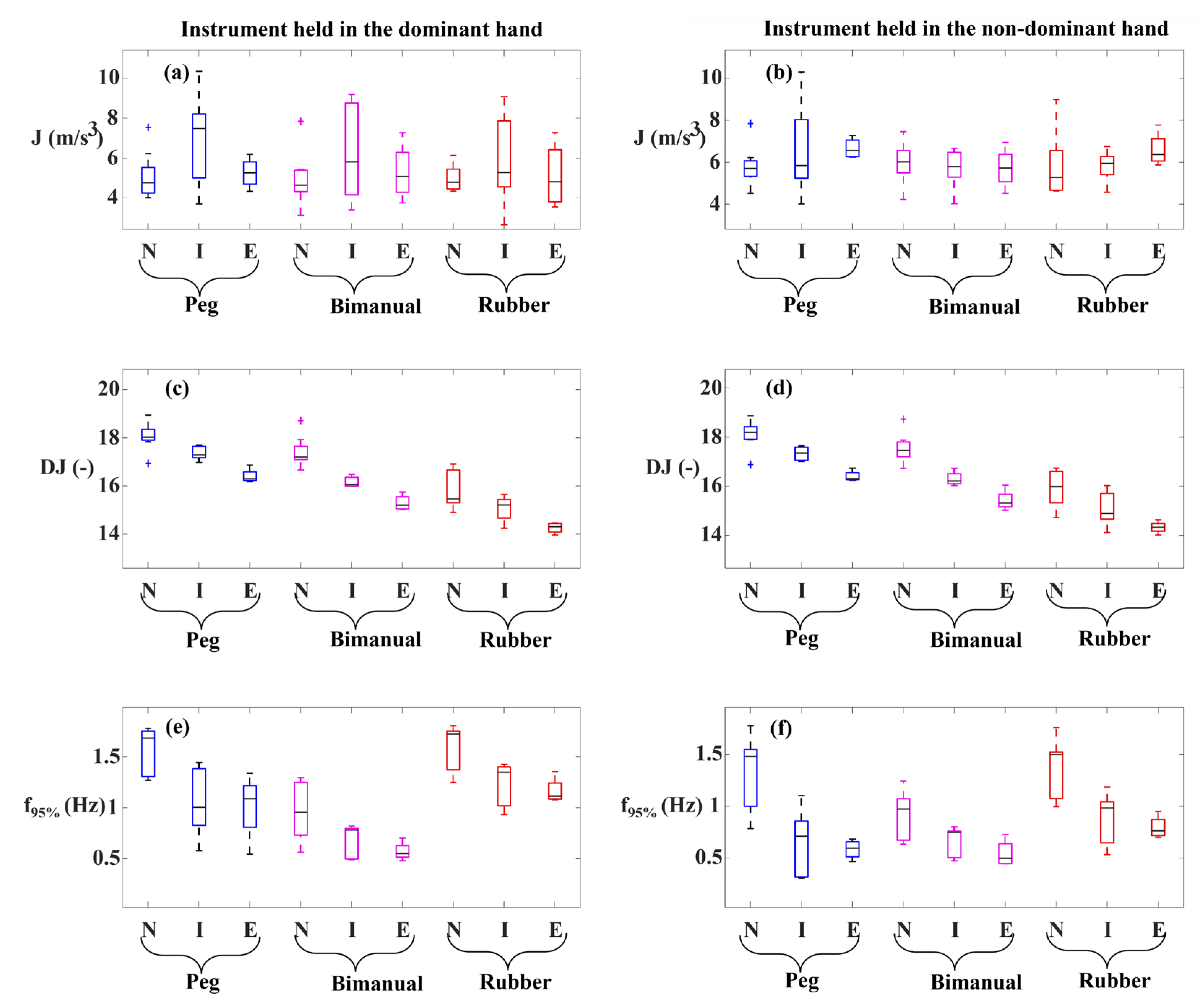
3.1. Mean Tooltip Motion Jerk
3.2. Logarithmic Dimensionless Tooltip Motion Jerk
3.3. The 95% Tooltip Motion Frequency
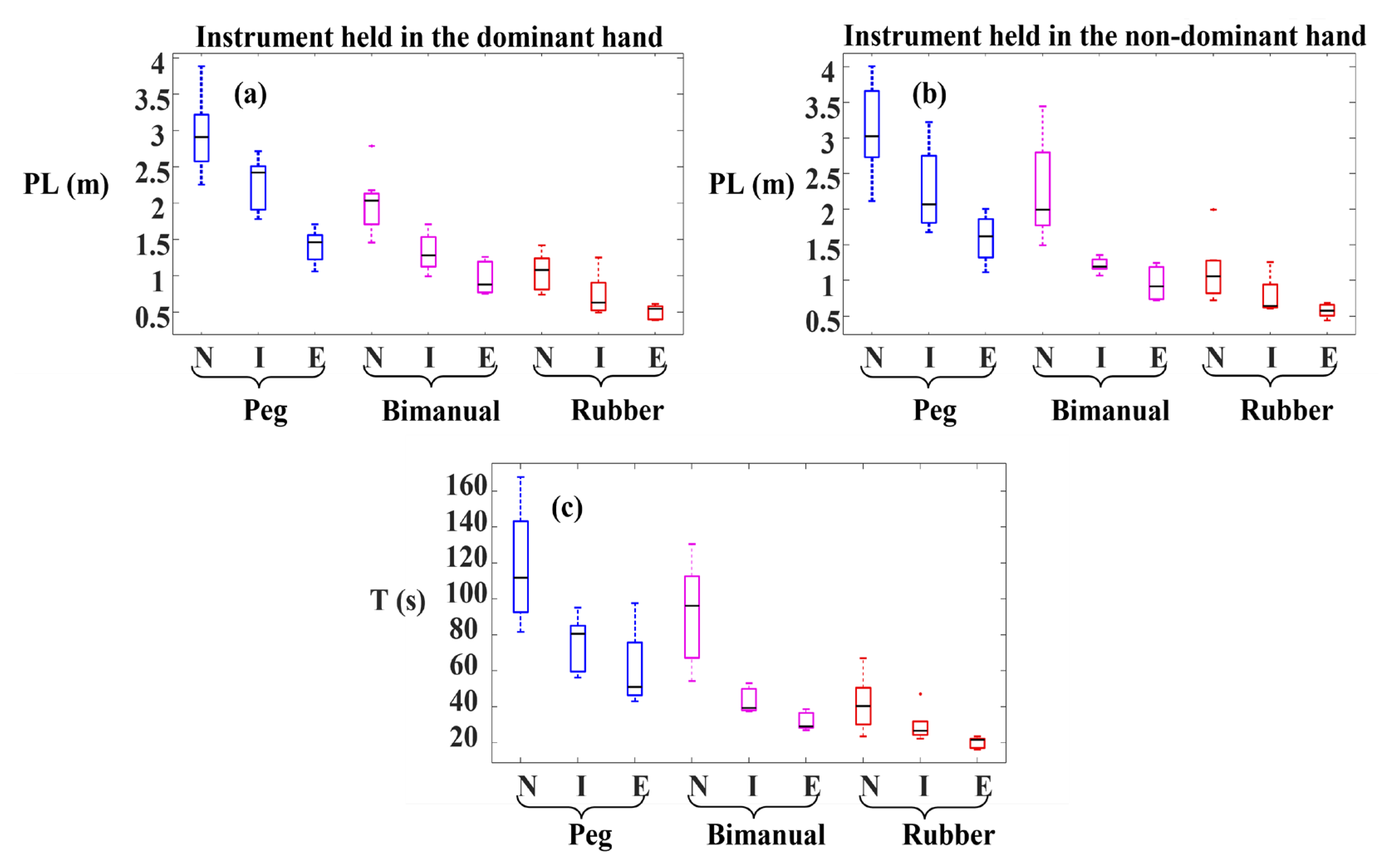
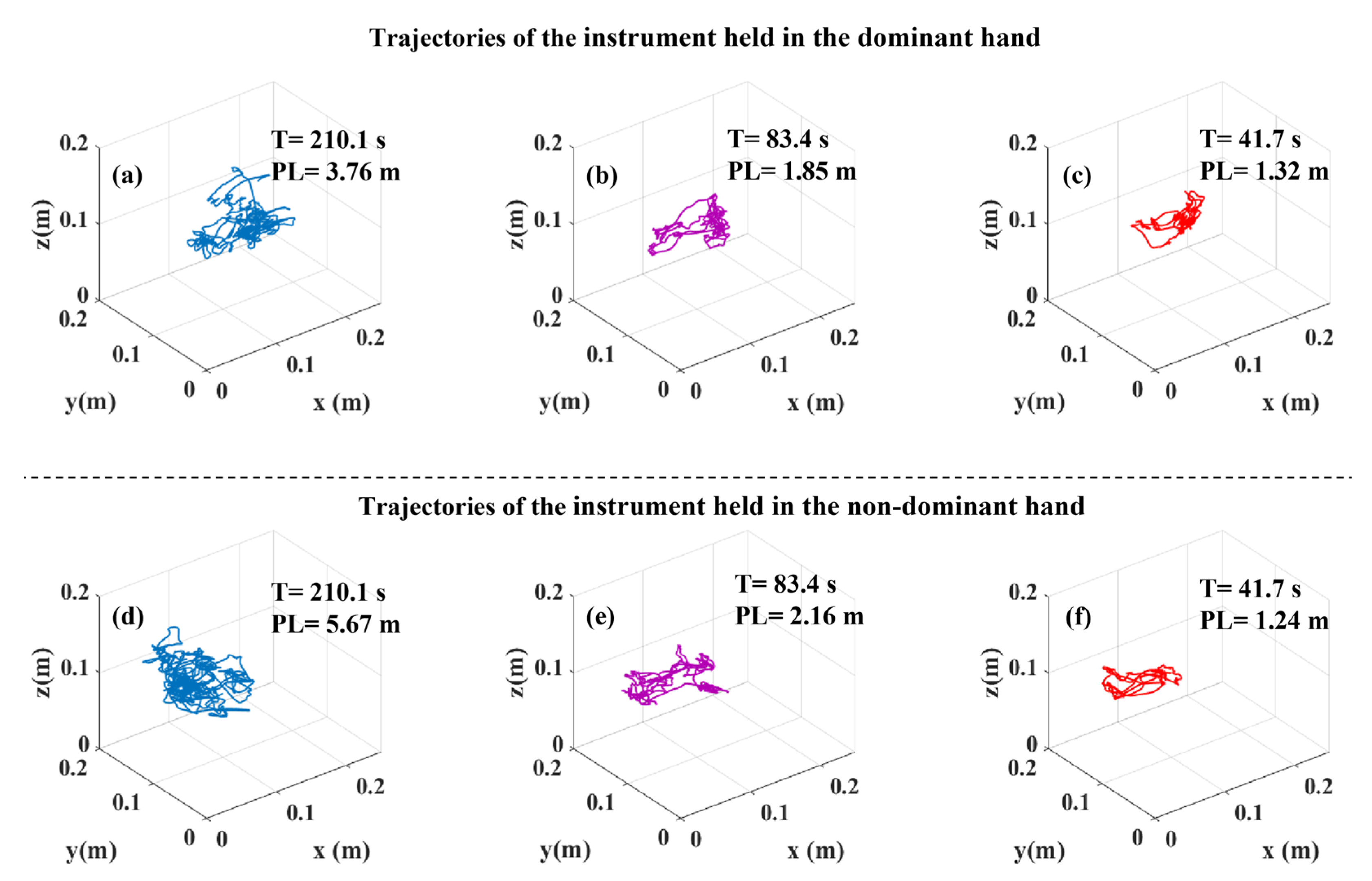
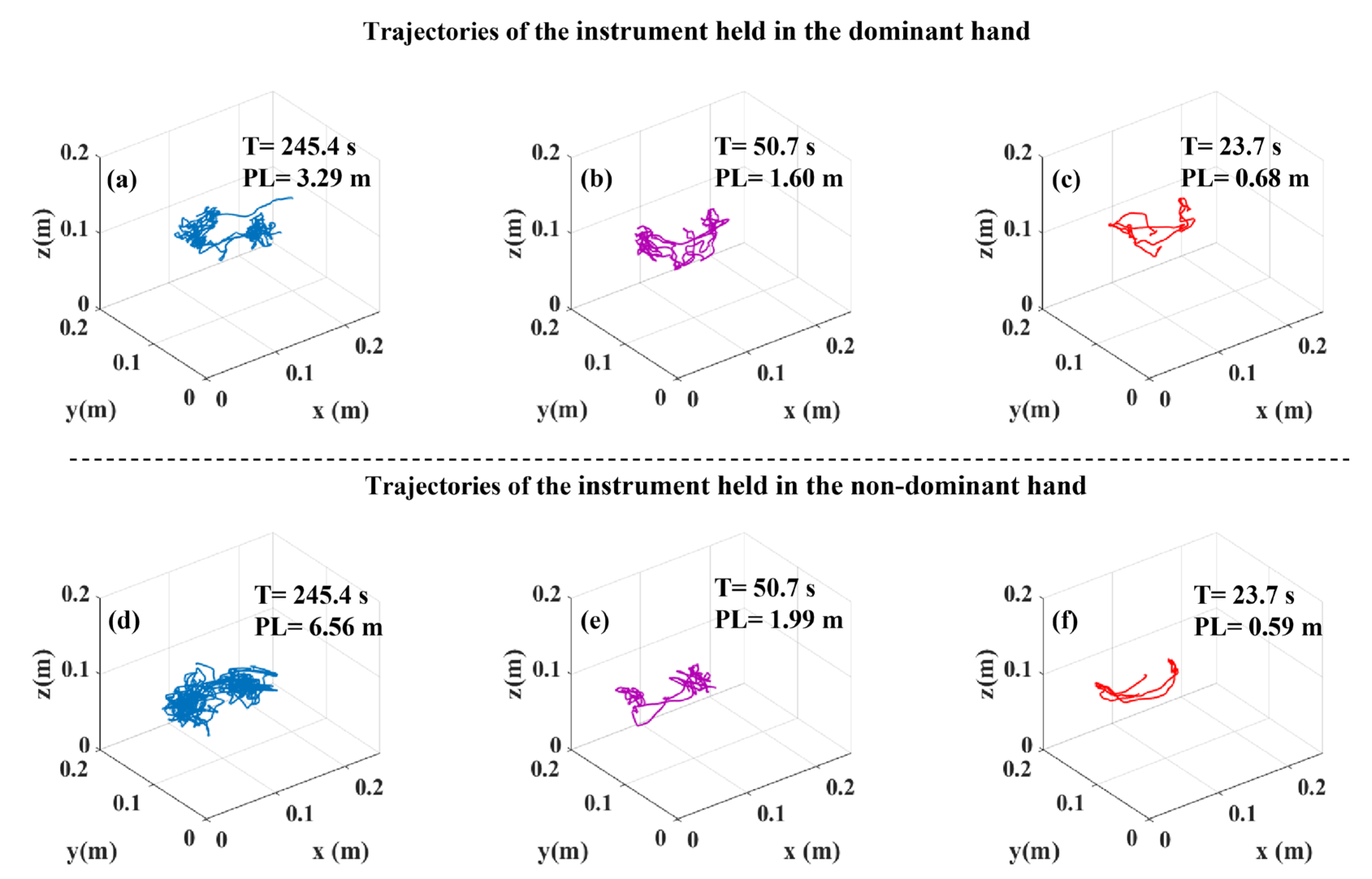
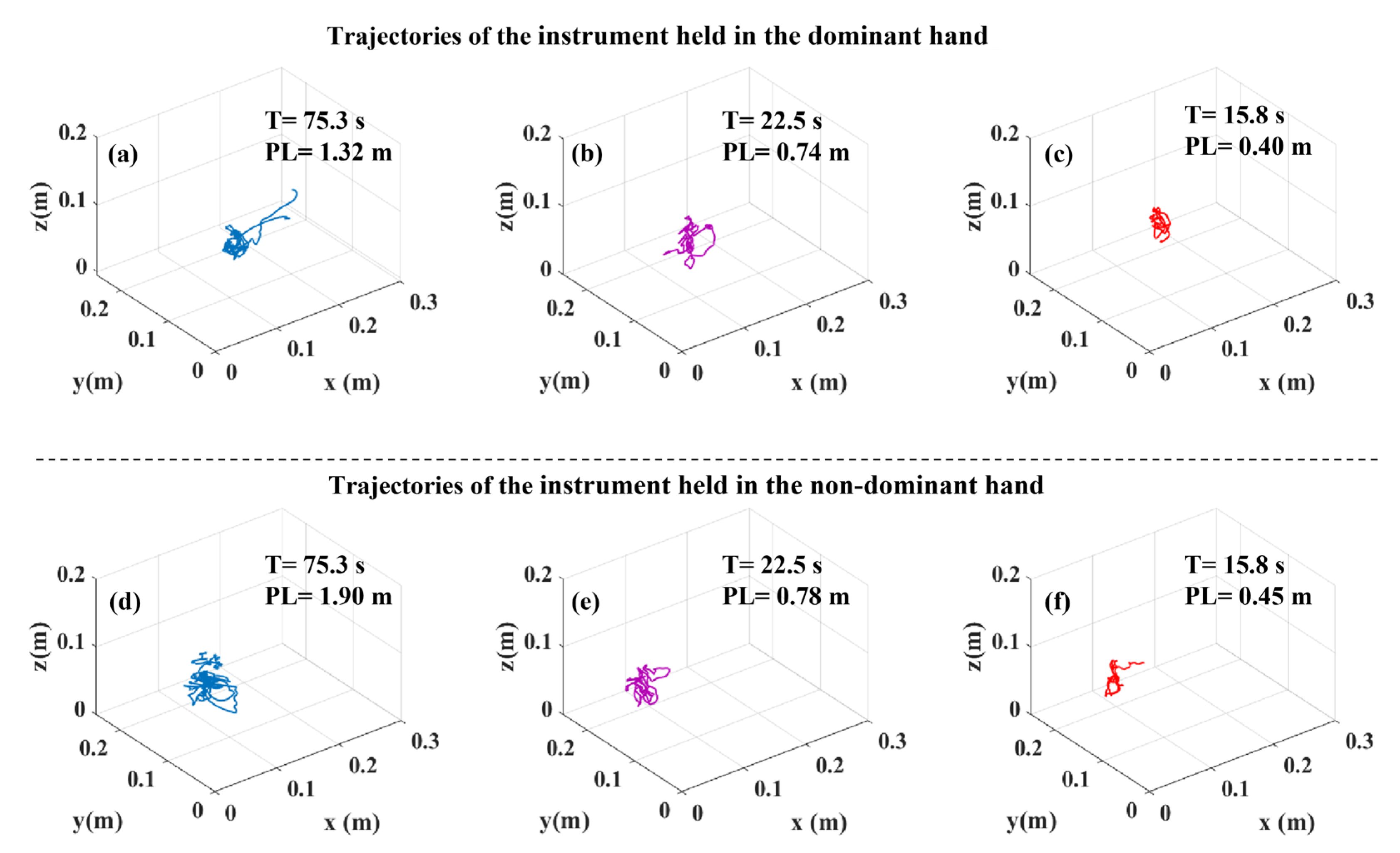
3.4. Tooltip Path Length and Task Duration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siddaiah-Subramanya, M.; To, H.; Haigh, C. The psychosocial impact of surgical complications on the operating surgeon: A scoping review. Ann. Med. Surg. 2021, 67, 102530. [Google Scholar] [CrossRef]
- Zhan, C.; Miller, M.R. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA 2003, 290, 1868–1874. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, M.G. Evidence that surgical performance predicts clinical outcomes. World J. Urol. 2020, 38, 1595–1597. [Google Scholar] [CrossRef] [PubMed]
- Grantcharov, T.P.; Bardram, L.; Funch-Jensen, P.; Rosenberg, J. Assessment of technical surgical skills. Eur. J. Surg. 2002, 168, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.A.; Regehr, G.; Reznick, R.; Macrae, H.; Murnaghan, J.; Hutchison, C.; Brown, M. Objective structured assessment of technical skill (OSATS) for surgical residents. Br. J. Surg. 1997, 84, 273–278. [Google Scholar] [CrossRef]
- Vassiliou, M.C.; Feldman, L.S.; Andrew, C.G.; Bergman, S.; Leffondré, K.; Stanbridge, D.; Fried, G.M. A global assessment tool for evaluation of intraoperative laparoscopic skills. Am. J. Surg. 2005, 190, 107–113. [Google Scholar] [CrossRef]
- Goh, A.C.; Goldfarb, D.W.; Sander, J.C.; Miles, B.J.; Dunkin, B.J. Global evaluative assessment of robotic skills: Validation of a clinical assessment tool to measure robotic surgical skills. J. Urol. 2012, 187, 247–252. [Google Scholar] [CrossRef]
- Nisky, I.; Okamura, A.M.; Hsieh, M.H. Effects of robotic manipulators on movements of novices and surgeons. Surg. Endosc. 2014, 28, 2145–2158. [Google Scholar] [CrossRef] [PubMed]
- Ershad, M.; Rege, R.; Majewicz Fey, A. Automatic and near real-time stylistic behavior assessment in robotic surgery. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 635–643. [Google Scholar] [CrossRef]
- Oropesa, I.; Sánchez-González, P.; Chmarra, M.K.; Lamata, P.; Fernández, Á.; Sánchez-Margallo, J.A.; Jansen, F.W.; Dankelman, J.; Sánchez-Margallo, F.M.; Gómez, E.J. EVA: Laparoscopic instrument tracking based on endoscopic video analysis for psychomotor skills assessment. Surg. Endosc. 2013, 27, 1029–1039. [Google Scholar] [CrossRef] [Green Version]
- Kitaguchi, D.; Takeshita, N.; Matsuzaki, H.; Oda, T.; Watanabe, M.; Mori, K.; Kobayashi, E.; Ito, M. Automated laparoscopic colorectal surgery workflow recognition using artificial intelligence: Experimental research. Int. J. Surg. 2020, 79, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Azari, D.P.; Miller, B.L.; Le, B.V.; Greenberg, C.C.; Radwin, R.G. Quantifying surgeon maneuevers across experience levels through marker-less hand motion kinematics of simulated surgical tasks. Appl. Ergon. 2020, 87, 103136. [Google Scholar] [CrossRef] [PubMed]
- Zhenzhu, L.; Lu, L.; Zhenzhi, L.; Xuzhi, L.; Yizhi, L.; Gangxian, F.; Henglu, W.; Jinke, D.; Qingbo, W.; Pengfei, L.; et al. Feasibility study of the low-cost motion tracking system for assessing endoscope holding skills. World Neurosurg. 2020, 140, 312–319. [Google Scholar] [CrossRef]
- Hogan, N.; Sternad, D. Sensitivity of smoothness measures to movement duration, amplitude, and arrests. J. Mot. Behav. 2009, 41, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Zia, A.; Essa, I. Automated surgical skill assessment in RMIS training. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 731–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chmarra, M.K.; Kolkman, W.; Jansen, F.W.; Grimbergen, C.A.; Dankelman, J. The influence of experience and camera holding on laparoscopic instrument movements measured with the TrEndo tracking system. Surg. Endosc. 2007, 21, 2069–2075. [Google Scholar] [CrossRef] [Green Version]
- Slack, P.S.; Coulson, C.J.; Ma, X.; Pracy, P.; Parmar, S.; Webster, K. The effect of operating time on surgeon’s hand tremor. Eur. Arch. Oto-Rhino-Laryngol. 2009, 266, 137–141. [Google Scholar] [CrossRef]
- Tatinati, S.; Nazarpour, K.; Ang, W.T.; Veluvolu, K.C. Multidimensional modeling of physiological tremor for active compensation in handheld surgical robotics. IEEE Trans. Ind. Electron. 2016, 64, 1645–1655. [Google Scholar] [CrossRef] [Green Version]
- Roizenblatt, M.; Grupenmacher, A.T.; Junior, R.B.; Maia, M.; Gehlbach, P.L. Robot-assisted tremor control for performance enhancement of retinal microsurgeons. Br. J. Ophthalmol. 2019, 103, 1195–1200. [Google Scholar] [CrossRef]
- Davids, J.; Makariou, S.G.; Ashrafian, H.; Darzi, A.; Marcus, H.J.; Giannarou, S. Automated Vision-Based Microsurgical Skill Analysis in Neurosurgery Using Deep Learning: Development and Preclinical Validation. World Neurosurg. 2021, 149, 669–686. [Google Scholar] [CrossRef]
- Maithel, S.K.; Villegas, L.; Stylopoulos, N.; Dawson, S.; Jones, D.B. Simulated laparoscopy using a head-mounted display vs traditional video monitor: An assessment of performance and muscle fatigue. Surg. Endosc. 2005, 19, 406–411. [Google Scholar] [CrossRef]
- Sánchez-Margallo, J.A.; Sánchez-Margallo, F.M.; Carrasco, J.B.P.; García, I.O.; Aguilera, E.J.G.; del Pozo, J.M. Usefulness of an optical tracking system in laparoscopic surgery for motor skills assessment. Cirugía Española 2014, 92, 421–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansoor, S.M.; Våpenstad, C.; Mårvik, R.; Glomsaker, T.; Bliksøen, M. Construct validity of eoSim–a low-cost and portable laparoscopic simulator. Minim. Invasive Ther. Allied Technol. 2020, 29, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Ghasemloonia, A.; Maddahi, Y.; Zareinia, K.; Lama, S.; Dort, J.C.; Sutherland, G.R. Surgical Skill Assessment Using Motion Quality and Smoothness. J. Surg. Educ. 2017, 74, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Vassiliou, M.C.; Dunkin, B.J.; Marks, J.M.; Fried, G.M. FLS and FES: Comprehensive models of training and assessment. Surg. Clin. N. Am. 2010, 90, 535–558. [Google Scholar] [CrossRef]
- Anderson, F.; Birch, D.W.; Boulanger, P.; Bischof, W.F. Sensor fusion for laparoscopic surgery skill acquisition. Comput. Aided Surg. 2012, 17, 269–283. [Google Scholar] [CrossRef]
- Schmidt, M.W.; Kowalewski, K.F.; Schmidt, M.L.; Wennberg, E.; Garrow, C.R.; Paik, S.; Benner, L.; Schijven, M.P.; Müller-Stich, B.P.; Nickel, F. The Heidelberg VR Score: Development and validation of a composite score for laparoscopic virtual reality training. Surg. Endosc. 2019, 33, 2093–2103. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Motion Smoothness Metric | Formula |
|---|---|
| Mean tooltip motion jerk | |
| Logarithmic dimensionless tooltip motion jerk | |
| 95% tooltip motion frequency | The frequency below which contains 95% of the total power of the tooltip position signal. |
| Metric | Task | The Instrument Held in the Dominant Hand | The Instrument Held in the Non-Dominant Hand | ||||||
|---|---|---|---|---|---|---|---|---|---|
| All | N-E | N-I | I-E | All | N-E | N-I | I-E | ||
| Mean tooltip motion jerk (J) | Peg transfer | 0.580 | 0.825 | 0.438 | 0.413 | 0.043 * | 0.003 * | 0.438 | 0.556 |
| Bimanual peg transfer | 0.736 | 0.825 | 0.518 | 0.730 | 0.970 | 0.940 | 0.797 | 1.000 | |
| Rubber band translocation | 0.698 | 0.604 | 0.518 | 0.730 | 0.114 | 0.050 | 0.438 | 0.286 | |
| Logarithmic dimensionless tooltip motion jerk (DJ) | Peg transfer | 0.002 * | 0.003 * | 0.019 * | 0.016 * | 0.002 * | 0.003 * | 0.019 * | 0.016 * |
| Bimanual peg transfer | 0.001 * | 0.003 * | 0.001 * | 0.016 * | 0.001 * | 0.003 * | 0.001 * | 0.032 * | |
| Rubber band translocation | 0.006 * | 0.003 * | 0.060 | 0.063 | 0.011 * | 0.003 * | 0.147 | 0.111 | |
| 95% tooltip motion frequency (f95%) | Peg transfer | 0.020 * | 0.020 * | 0.029 * | 0.905 | 0.004 * | 0.003 * | 0.007 * | 0.730 |
| Bimanual peg transfer | 0.023 * | 0.011 * | 0.083 | 0.413 | 0.024 * | 0.020 * | 0.083 | 0.190 | |
| Rubber band translocation | 0.024 * | 0.011 * | 0.060 | 0.905 | 0.004 * | 0.003 * | 0.007 * | 0.730 | |
| Tooltip path length (PL) | Peg transfer | 0.003 * | <0.001 * | 0.240 | 0.008 * | 0.005* | 0.002 * | 0.083 | 0.056 |
| Bimanual peg transfer | 0.002 * | <0.001 * | 0.012 * | 0.095 | <0.001* | <0.001 * | <0.001 * | 0.095 | |
| Rubber band translocation | 0.007 * | <0.001 * | 0.112 | 0.222 | 0.004* | <0.001 * | 0.042 * | 0.222 | |
| Task duration (T) | Peg transfer | All: 0.001 * | N-E: 0.001 * | N-I: 0.007 * | I-E: 0.016 * | ||||
| Bimanual peg transfer | All: 0.001 * | N-E: 0.001 * | N-I: 0.001 * | I-E: 0.016 * | |||||
| Rubber band translocation | All: 0.004 * | N-E: 0.001 * | N-I: 0.112 | I-E: 0.056 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aghazadeh, F.; Zheng, B.; Tavakoli, M.; Rouhani, H. Motion Smoothness-Based Assessment of Surgical Expertise: The Importance of Selecting Proper Metrics. Sensors 2023, 23, 3146. https://doi.org/10.3390/s23063146
Aghazadeh F, Zheng B, Tavakoli M, Rouhani H. Motion Smoothness-Based Assessment of Surgical Expertise: The Importance of Selecting Proper Metrics. Sensors. 2023; 23(6):3146. https://doi.org/10.3390/s23063146
Chicago/Turabian StyleAghazadeh, Farzad, Bin Zheng, Mahdi Tavakoli, and Hossein Rouhani. 2023. "Motion Smoothness-Based Assessment of Surgical Expertise: The Importance of Selecting Proper Metrics" Sensors 23, no. 6: 3146. https://doi.org/10.3390/s23063146