
Using Digital Human Modelling to Evaluate the Risk of Musculoskeletal Injury for Workers in the Healthcare Industry

Abstract
:1. Introduction
2. Methods
2.1. System Setup and Participants
2.2. Operational Tasks
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
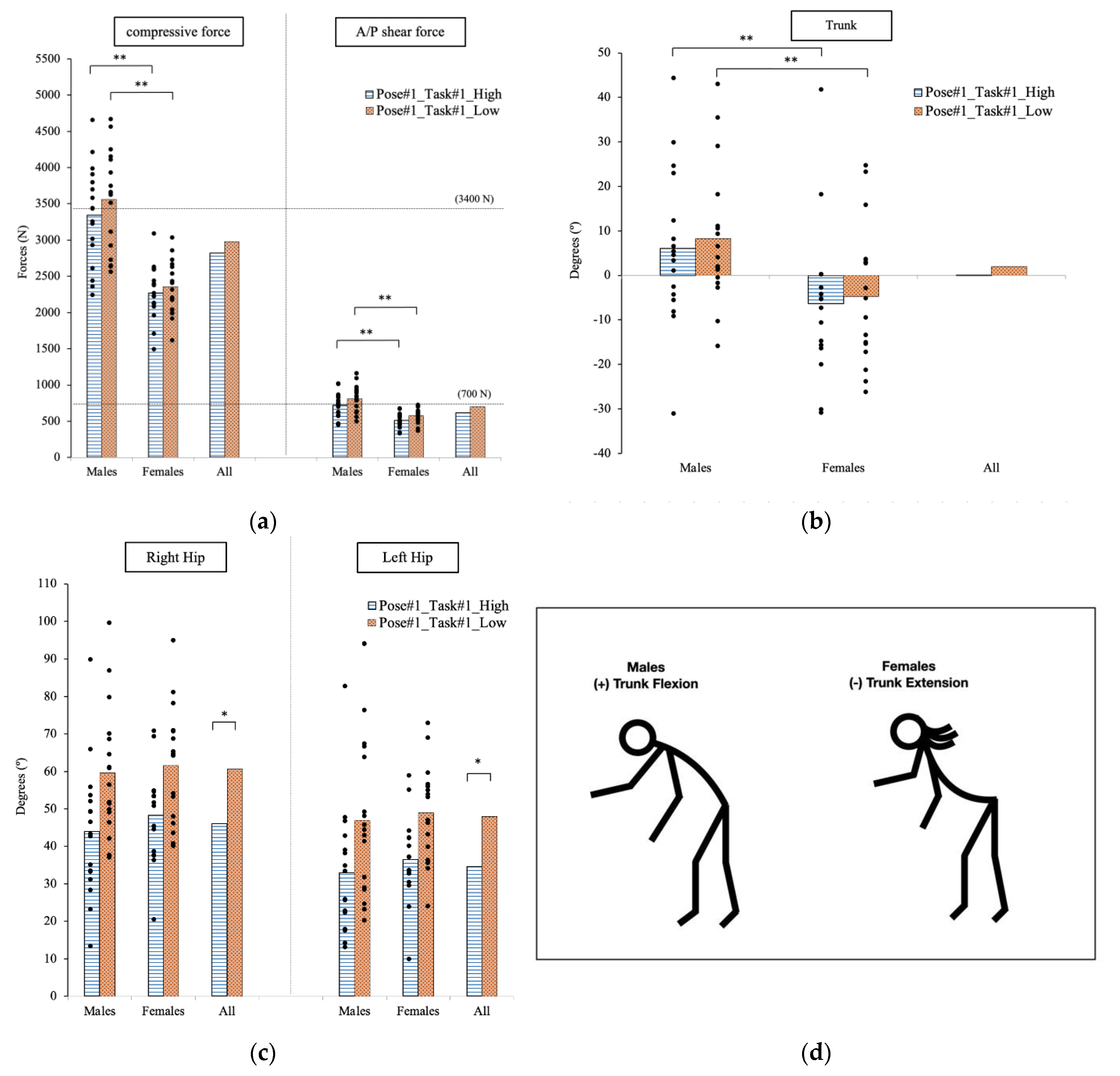
3.1. Pose#1 in Task#1: Assisting Patient Manikin from Lying to Sitting in the Hospital Bed
3.1.1. Force Analysis
3.1.2. Joint Angle
3.1.3. Cross-Correlation
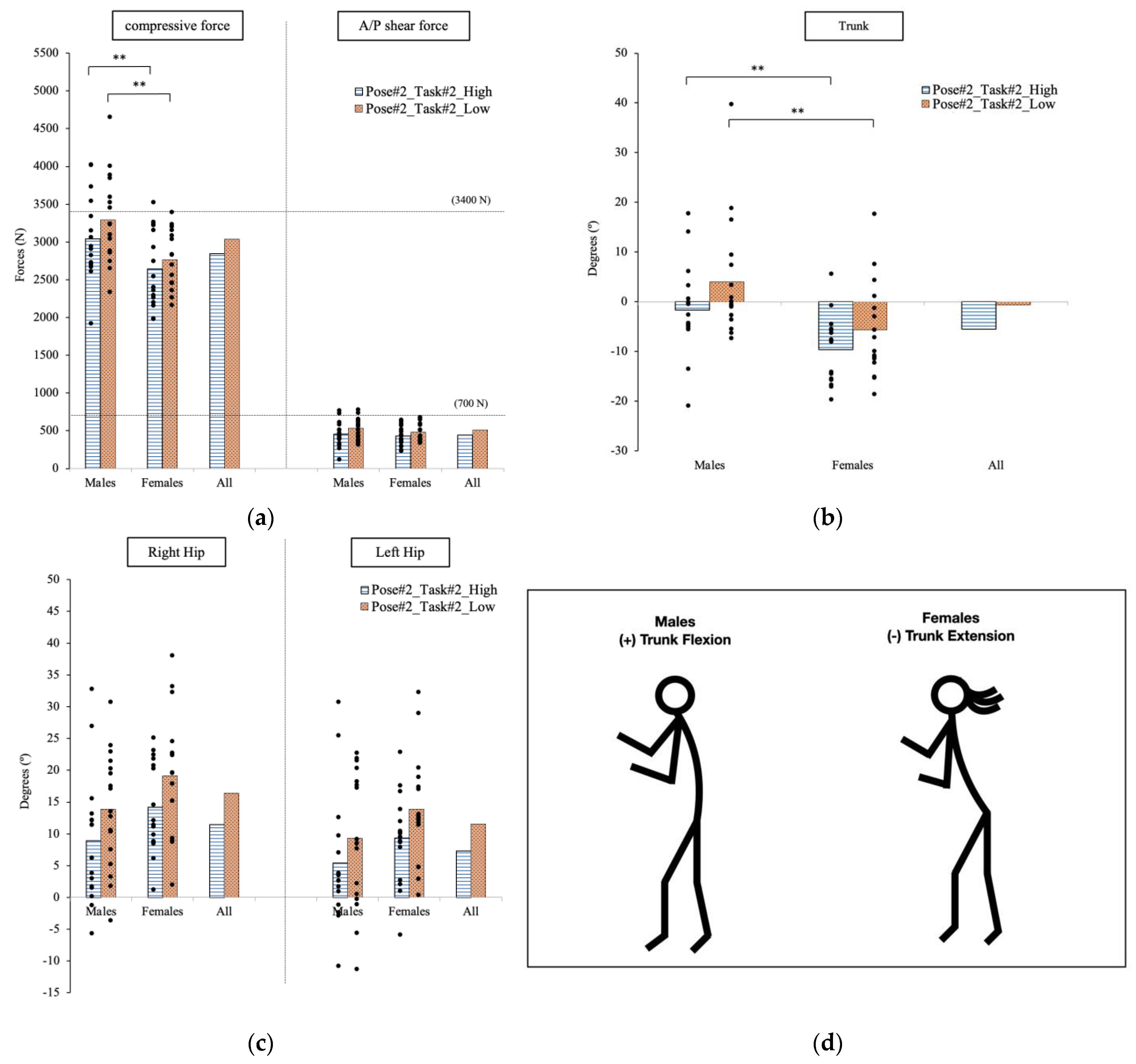
3.2. Pose#2 in Task#2: Moving the Manikin from the Bed to the Wheelchair
3.2.1. Force Analysis
3.2.2. Joint Angle
3.2.3. Cross-Correlation
3.3. Pose#3 in Task#2: Positioning the Patient Manikin in Wheelchair
3.3.1. Force Analysis
3.3.2. Joint Angle
3.3.3. Cross-Correlation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tavakkol, R.; Kavi, E.; Hassanipour, S.; Rabiei, H.; Malakoutikhah, M. The global prevalence of musculoskeletal disorders among operating room personnel: A systematic review and meta-analysis. Clin. Epidemiol. Glob. Health 2020, 8, 1053–1061. [Google Scholar] [CrossRef] [Green Version]
- Davis, K.G.; Freeman, A.M.; Ying, J.; Huth, J.R. Workers’ compensation costs for healthcare caregivers: Home healthcare, long-term care, and hospital nurses and nursing aides. Am. J. Ind. Med. 2021, 64, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, K.S.; Raju, G.; Shawkataly, O. Prevalence of work-related musculoskeletal disorders: Psychological and physical risk factors. Int. J. Environ. Res. Public Health 2021, 18, 9361. [Google Scholar] [CrossRef] [PubMed]
- U.S. Bureau of Labor Statistics. Occupational Injuries and Illnesses Resulting in Musculoskeletal Disorders (MSDs). Available online: https://www.bls.gov/iif/factsheets/msds.htm (accessed on 5 May 2022).
- LM. Workplace Safety Index: Healthcare and Social Assistance. Available online: https://business.libertymutualgroup.com/business-insurance/Documents/Services/RC2030.pdf (accessed on 6 March 2022).
- Iridiastadi, H.; Anggawisnu, B.; Didin, F.S.; Yamin, P.A.R. The Prevalence of Musculoskeletal Complaints among Hospital Nurses and Nursing Home Caregivers in Indonesia. Prevalence 2019, 10, 854. [Google Scholar] [CrossRef] [Green Version]
- U.S. Bureau of Labor Statistics. Injuries, Illnesses, and Fatalities. Available online: https://www.bls.gov/iif/oshwc/case/msds.htm (accessed on 5 May 2022).
- Ji, X.; Piovesan, D.; Conley, K. The Effect of Pulling Effort on Lumbar Spine via Applying Digital Human Modeling Technology. In Proceedings of the Institute of Industrial and Systems Engineers (IISE) Annual Conference, Seattle, WA, USA, 21–24 May 2022; pp. 21–24. [Google Scholar]
- Choi, S.D.; Brings, K. Work-related musculoskeletal risks associated with nurses and nursing assistants handling overweight and obese patients: A literature review. Work 2016, 53, 439–448. [Google Scholar] [CrossRef] [Green Version]
- Gilchrist, A.; Pokorná, A. Prevalence of musculoskeletal low back pain among registered nurses: Results of an online survey. J. Clin. Nurs. 2021, 30, 1675–1683. [Google Scholar] [CrossRef]
- Nourollahi, M.; Afshari, D.; Dianat, I. Awkward trunk postures and their relationship with low back pain in hospital nurses. Work 2018, 59, 317–323. [Google Scholar] [CrossRef] [Green Version]
- Van Hoof, W.; O’Sullivan, K.; O’Keeffe, M.; Verschueren, S.; O’Sullivan, P.; Dankaerts, W. The efficacy of interventions for low back pain in nurses: A systematic review. Int. J. Nurs. Stud. 2018, 77, 222–231. [Google Scholar] [CrossRef] [Green Version]
- OSHA. Occupational Safety and Health Administration. Safe Patient Handling. Available online: https://www.osha.gov/healthcare/safe-patient-handling (accessed on 22 July 2022).
- UNC EHS. Lifting and Material Handling. Available online: https://ehs.unc.edu/workplace-%20safety/ergonomics/lifting/ (accessed on 3 November 2022).
- Estrada, J.E.; Vea, L.A. Modelling and Simulation of Spine in Sitting Posture in a Computer-Related Workplace. Int. J. Comput. Sci. Mob. Comput. 2018, 7, 121–135. [Google Scholar]
- Rusu, C.-A.; Constantinescu, C.; Marinescu, S.-C. A generic hybrid Human/Exoskeleton Digital Model towards Digital Transformation of Exoskeletons-integrated workplaces. Procedia CIRP 2021, 104, 1787–1790. [Google Scholar] [CrossRef]
- Maurya, C.M.; Karmakar, S.; Das, A.K. Digital human modeling (DHM) for improving work environment for specially-abled and elderly. SN Appl. Sci. 2019, 1, 1326. [Google Scholar] [CrossRef] [Green Version]
- Quintero-Duran, M.; Paul, G. Ergonomic assessment of a physical task using two different digital human modelling systems: A case study. Int. J. Hum. Factors Model. Simul. 2018, 6, 298–313. [Google Scholar] [CrossRef]
- Cao, W.; Jiang, M.; Han, Y.; Khasawneh, M.T. Ergonomic assessment of patient barrow lifting technique using digital human modeling. In Proceedings of the International Conference on Digital Human Modeling and Applications in Health, Safety, Ergonomics and Risk Management, Las Vegas, NV, USA, 21–26 July 2013; pp. 20–29. [Google Scholar]
- Samson, A. Digital Human Modeling for Ergonomic Assessment of Patient Lifting by Paramedics; State University of New York at Binghamton: Binghamton, NY, USA, 2009. [Google Scholar]
- Irshaidat, F. Digital Human Modeling for Ergonomic Assessment of Patient Lifting with and without Assistive Devices in Operating Rooms; State University of New York at Binghamton: Binghamton, NY, USA, 2012. [Google Scholar]
- Ji, X.; Piovesan, D.; Arenas, M.; Liu, H. Analysis of Healthcare Push and Pull Task via JACK: Predicted Joint Accuracy during Full-Body Simulation. Appl. Sci. 2022, 12, 6450. [Google Scholar] [CrossRef]
- Lad, U. Comparing the Kinematic and Kinetic Outputs from Digital Human Modeling Tools to a Lab-Based Rigid-Link Model for the Investigation of Musculoskeletal Disorder Hazards during Patient Handling; University of Waterloo: Waterloo, ON, Canada, 2018. [Google Scholar]
- Constantinescu, C.; Todorovic, O.; Ippolito, D. Comprehensive modelling and simulation towards the identification of critical parameters for evaluation of exoskeleton-centred workplaces. Procedia CIRP 2019, 79, 176–179. [Google Scholar] [CrossRef]
- Zhou, H.; Hu, H. Human motion tracking for rehabilitation—A survey. Biomed. Signal Process. Control 2008, 3, 1–18. [Google Scholar] [CrossRef]
- Roetenberg, D.; Luinge, H.; Slycke, P. Xsens MVN: Full 6DOF human motion tracking using miniature inertial sensors. Xsens Motion Technol. BV Tech. Rep. 2009, 1, 1–7. [Google Scholar]
- Yu, D.; Dural, C.; Morrow, M.; Yang, L.; Collins, J.W.; Hallbeck, S.; Kjellman, M.; Forsman, M. Intraoperative workload in robotic surgery assessed by wearable motion tracking sensors and questionnaires. Surg. Endosc. 2017, 31, 877–886. [Google Scholar] [CrossRef]
- Willy, R.W. Innovations and pitfalls in the use of wearable devices in the prevention and rehabilitation of running related injuries. Phys. Ther. Sport 2018, 29, 26–33. [Google Scholar] [CrossRef]
- Tao, W.; Lai, Z.-H.; Leu, M.C.; Yin, Z. Worker activity recognition in smart manufacturing using IMU and sEMG signals with convolutional neural networks. Procedia Manuf. 2018, 26, 1159–1166. [Google Scholar] [CrossRef]
- Puthenveetil, S.C.; Daphalapurkar, C.P.; Zhu, W.; Leu, M.C.; Liu, X.F.; Gilpin-Mcminn, J.K.; Snodgrass, S.D. Computer-automated ergonomic analysis based on motion capture and assembly simulation. Virtual Real. 2015, 19, 119–128. [Google Scholar] [CrossRef]
- Raschke, U.; Cort, C. Siemens jack. In DHM and Posturography; Elsevier: Amsterdam, The Netherlands, 2019; pp. 35–48. [Google Scholar]
- Chaffin, D.B. Improving digital human modelling for proactive ergonomics in design. Ergonomics 2005, 48, 478–491. [Google Scholar] [CrossRef] [PubMed]
- Cutler, B.; Merritt, T.; Eger, T.; Godwin, A. Using Peak Vicon data to drive Classic JACK animation for the comparison of low back loads experienced during para-rowing. Int. J. Hum. Factors Model. Simul. 2015, 5, 99–112. [Google Scholar] [CrossRef]
- Qi, Z.; Chen, Y. Investigation of Ergonomics in Photocuring 3D Printing Post-Processing Using Jack. In Proceedings of the 2020 IEEE 7th International Conference on Industrial Engineering and Applications (ICIEA), Bangkok, Thailand, 16–18 April 2020; pp. 326–329. [Google Scholar]
- Waters, T.R.; Putz-Anderson, V.; Garg, A.; Fine, L.J. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics 1993, 36, 749–776. [Google Scholar] [CrossRef]
- LibreTexts Statistics. Testing the Significance of the Correlation Coefficient. Available online: https://courses.lumenlearning.com/introstats1/chapter/testing-the-significance-of-the-correlation-coefficient/ (accessed on 17 December 2022).
- Gallagher, S.; Marras, W.S. Tolerance of the lumbar spine to shear: A review and recommended exposure limits. Clin. Biomech. 2012, 27, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Hlavenka, T.M.; Christner, V.F.; Gregory, D.E. Neck posture during lifting and its effect on trunk muscle activation and lumbar spine posture. Appl. Ergon. 2017, 62, 28–33. [Google Scholar] [CrossRef]
- Ji, X.; Tiari, S. Posture evaluation for the full-body dynamic simulation in JACK Siemens PLM. Int. J. Hum. Factors Ergon. 2022, 9, 261–281. [Google Scholar] [CrossRef]
- Patel, P.; Parmar, L. Comparison Between Genders for Trunk Mobility in Normal Adults: A Cross Sectional Study. Int. J. Health Sci. 2022, 6, 1564–1573. [Google Scholar] [CrossRef]
- Clinic, M. Proper Lifting Techniques. Available online: https://www.mayoclinic.org/healthy-lifestyle/adult-health/multimedia/back-pain/sls-20076866?s=5 (accessed on 3 November 2022).
- Chen, G.; Liu, L.; Yu, J. A comparative study on strength between American college male and female students in Caucasian and Asian populations. Sport Sci. Rev. 2012, 21, 153. [Google Scholar] [CrossRef]
- Akhavanfar, M.; Kazemi, H.; Eskandari, A.; Arjmand, N. Obesity and spinal loads; a combined MR imaging and subject-specific modeling investigation. J. Biomech. 2018, 70, 102–112. [Google Scholar] [CrossRef]
- Dolan, P.; Mannion, A.; Adams, M. Passive tissues help the back muscles to generate extensor moments during lifting. J. Biomech. 1994, 27, 1077–1085. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Operational Height | Force Magnitude | Application Point | Force Direction | |
|---|---|---|---|---|
| P#1_T#1 | high | 70 N | right hand | vertical |
| low | 70 N | right hand | vertical | |
| P#2_T#2 | high | 125 N | both hands | vertical |
| low | 125 N | both hands | vertical | |
| P#3_T#2 | -- | 125 N | both hands | vertical |
| Operational Height | Average Comp Force_Male | Average Comp Force_Female | Average A/P Force_Male | Average A/P Force_Female | |
|---|---|---|---|---|---|
| P#1_T#1 | high | 3342.6 N (682.4 N) | 2266.7 N (382.2) | 720.4 N (173.8 N) | 510.9 N (100.2 N) |
| low | 3559.8 N (686.7 N) | 2360.3 N (375.5 N) | 812.2 N (185.3 N) | 574.1 N (103.0 N) | |
| P#2_T#2 | high | 3038.1 N (549.0 N) | 2644.1 N (511.4 N) | 455.6 N (161.7 N) | 432.5 N (133.0 N) |
| low | 3293.2 N (584.4 N) | 2766.2 N (388.1 N) | 534.2 N (140.1 N) | 483.9 N (118.0 N) | |
| P#3_T#2 | -- | 5201.0 N (781.0 N) | 4003.3 N (521.5 N) | 1116.6 N (221.0 N) | 854.7 N (168.9 N) |
| Operational Height | Average Trunk Angle | Average Right Hip | Average Left Hip | ||||
|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | ||
| P#1_T#1 | high | 6.1° (17.5°) | −6.4° (17.6°) | 44.0° (17.8°) | 48.3° (12.6°) | 32.9° (16.9°) | 36.5° (11.5°) |
| low | 8.3° (15.6°) | −4.8° (16.0°) | 59.7° (17.3°) | 61.6° (15.9°) | 47.0° (20.8°) | 49.0° (13.1°) | |
| P#2_T#2 | high | −1.7° (9.0°) | −9.6° (6.9°) | 8.9° (9.9°) | 14.2° (7.2°) | 5.4° (10.1°) | 9.3° (7.0°) |
| low | 4.0° (11.8°) | −5.6° (9.7°) | 13.9° (9.1°) | 19.2° (10.0°) | 9.3° (10.6°) | 13.9° (8.7°) | |
| P#3_T#2 | -- | 3.5° (15.0°) | −6.2° (11.6°) | 43.2° (19.3°) | 37.8° (14.1°) | 25.1° (13.2°) | 29.1° (15.7°) |
| Variable vs. Force | Body Height | Body Weight | Hip | Trunk | |
|---|---|---|---|---|---|
| P#1_T#1 high | Comp | 0.93 | 0.78 | 0.01 | 0.51 |
| A/P | 0.86 | 0.72 | 0.27 | 0.34 | |
| P#1_T#1 low | Comp | 0.94 | 0.79 | 0.09 | 0.43 |
| A/P | 0.91 | 0.80 | 0.22 | 0.30 | |
| P#2_T#2 high | Comp | 0.49 | 0.41 | 0.47 | 0.32 |
| A/P | 0.26 | 0.22 | 0.68 | 0.18 | |
| P#2_T#2 low | Comp | 0.68 | 0.48 | 0.21 | 0.34 |
| A/P | 0.43 | 0.29 | 0.60 | 0.04 | |
| P#3_T#2 | Comp | 0.81 | 0.65 | 0.43 | 0.37 |
| A/P | 0.71 | 0.59 | 0.66 | 0.15 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ji, X.; Hettiarachchige, R.O.; Littman, A.L.E.; Piovesan, D. Using Digital Human Modelling to Evaluate the Risk of Musculoskeletal Injury for Workers in the Healthcare Industry. Sensors 2023, 23, 2781. https://doi.org/10.3390/s23052781
Ji X, Hettiarachchige RO, Littman ALE, Piovesan D. Using Digital Human Modelling to Evaluate the Risk of Musculoskeletal Injury for Workers in the Healthcare Industry. Sensors. 2023; 23(5):2781. https://doi.org/10.3390/s23052781
Chicago/Turabian StyleJi, Xiaoxu, Ranuki O. Hettiarachchige, Alexa L. E. Littman, and Davide Piovesan. 2023. "Using Digital Human Modelling to Evaluate the Risk of Musculoskeletal Injury for Workers in the Healthcare Industry" Sensors 23, no. 5: 2781. https://doi.org/10.3390/s23052781