
Accelerations Recorded by Simple Inertial Measurement Units with Low Sampling Frequency Can Differentiate between Individuals with and without Knee Osteoarthritis: Implications for Remote Health Care

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
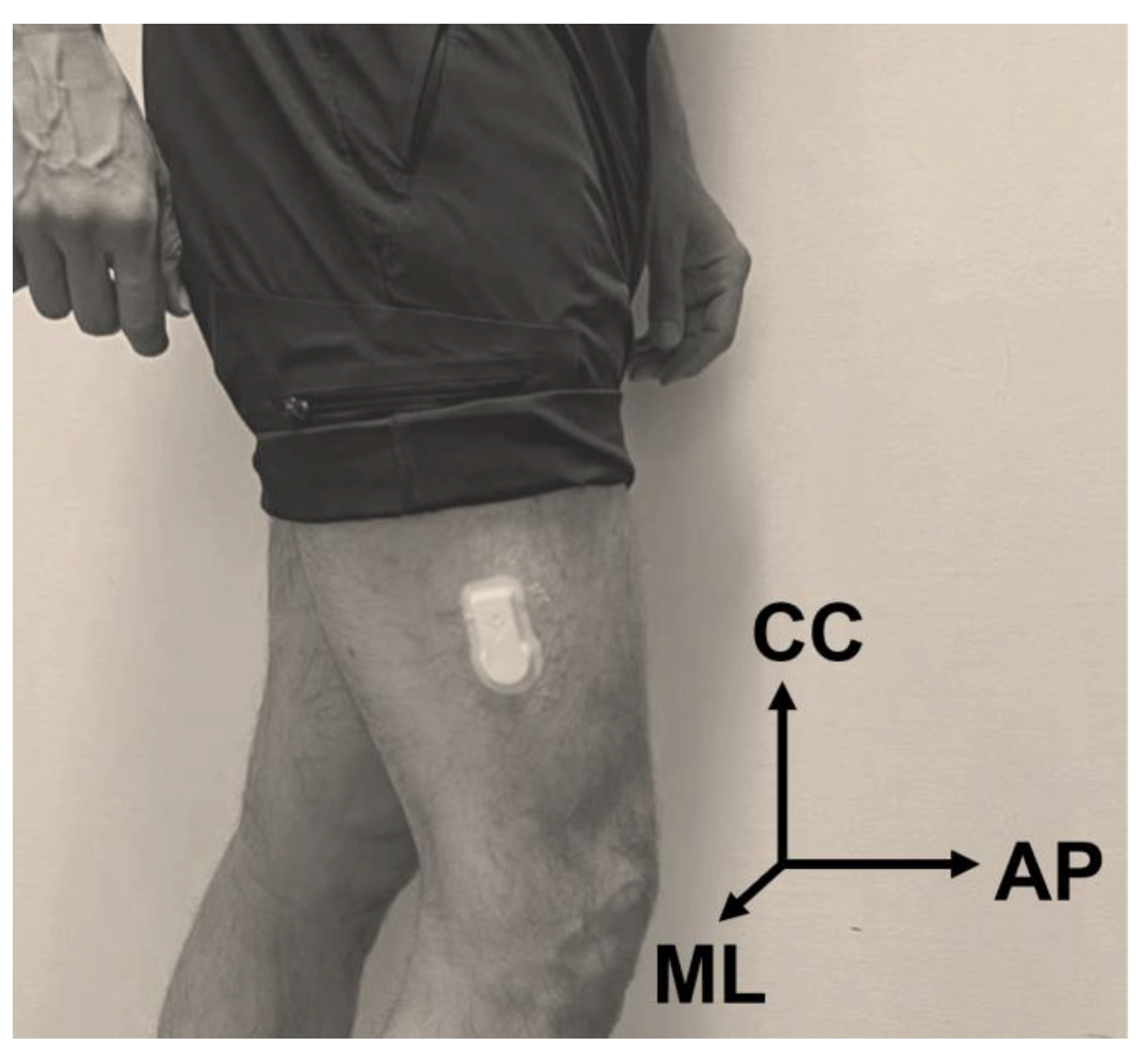
2.2. Data Collection
2.3. Acceleration Signal Processing
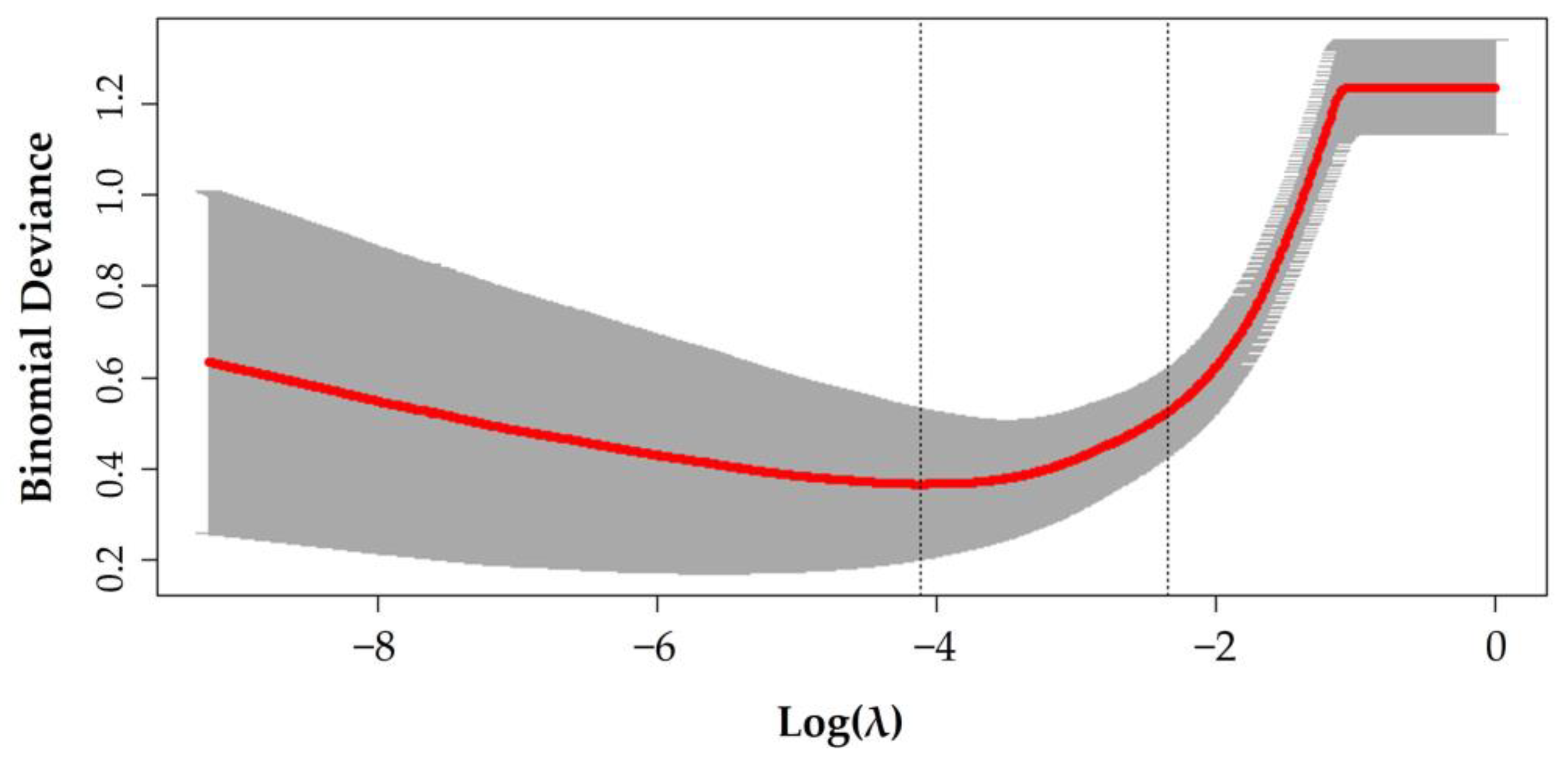
2.4. Logistic LASSO Regression
2.5. Comparing the Severity of Knee OA
2.6. Statistical Analysis
3. Results
3.1. Participants
3.2. Frequency Content Comparison
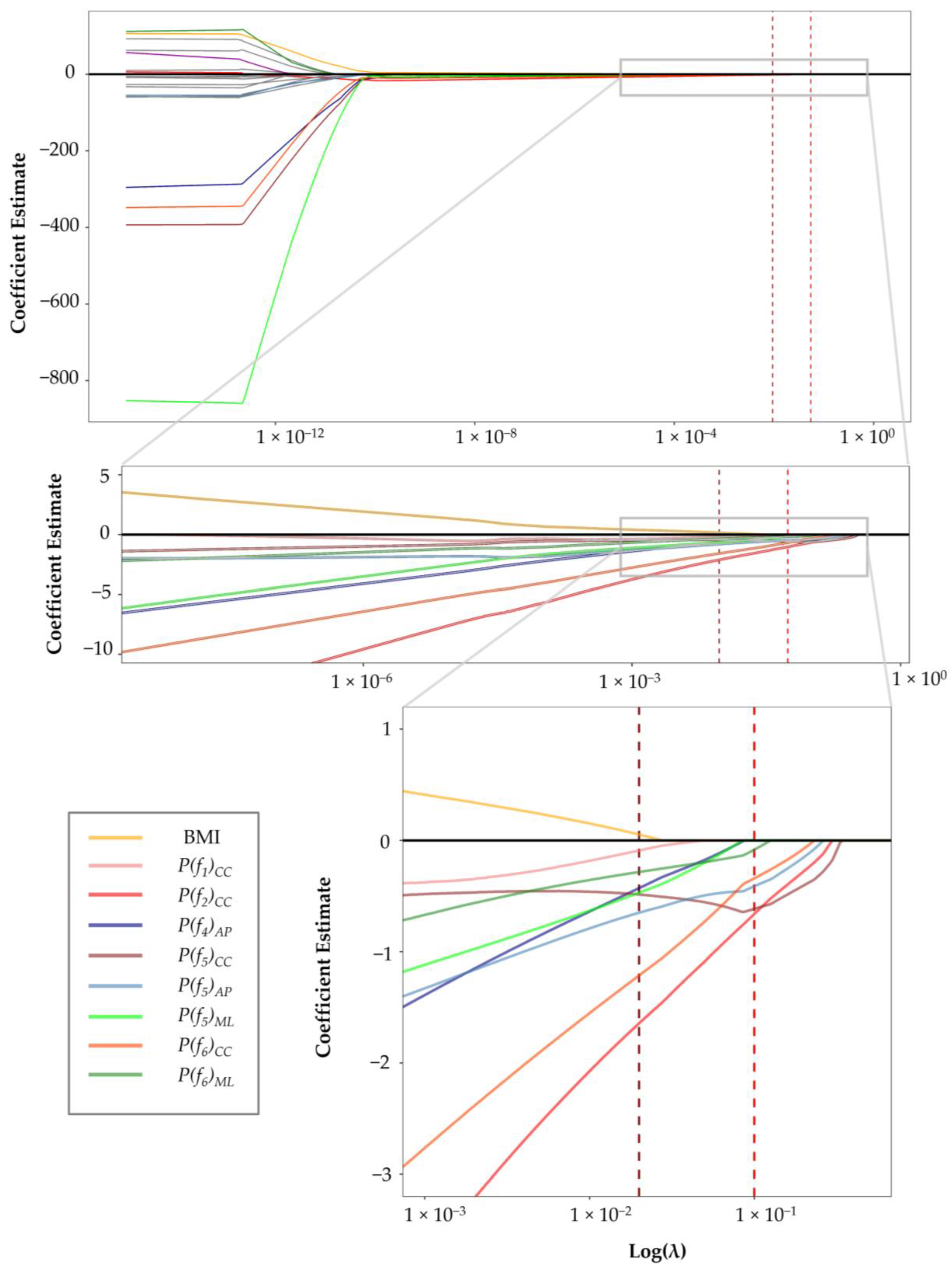
3.3. Frequency Content Feature Selection
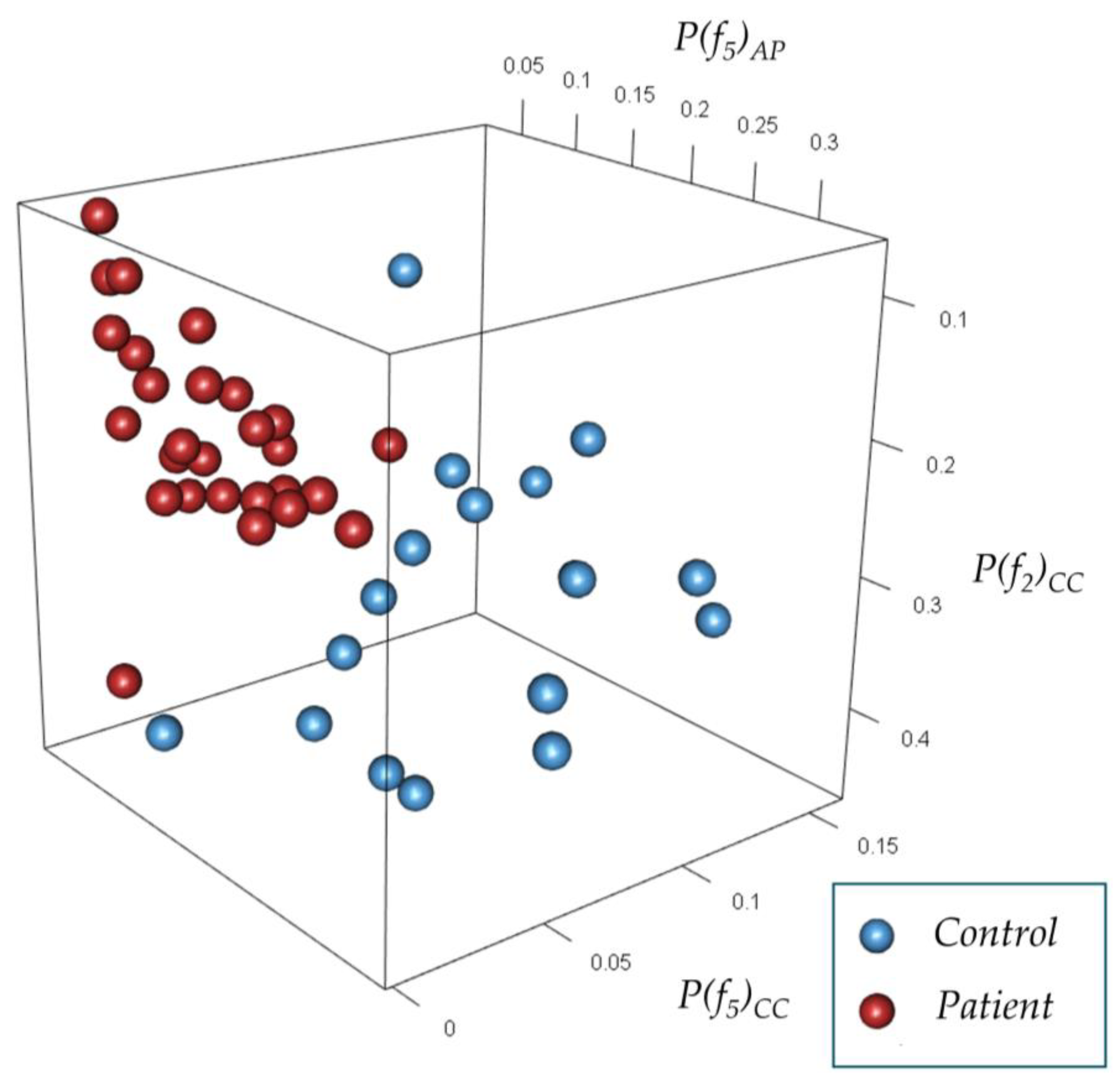
3.4. Classification of Gait Accelerations
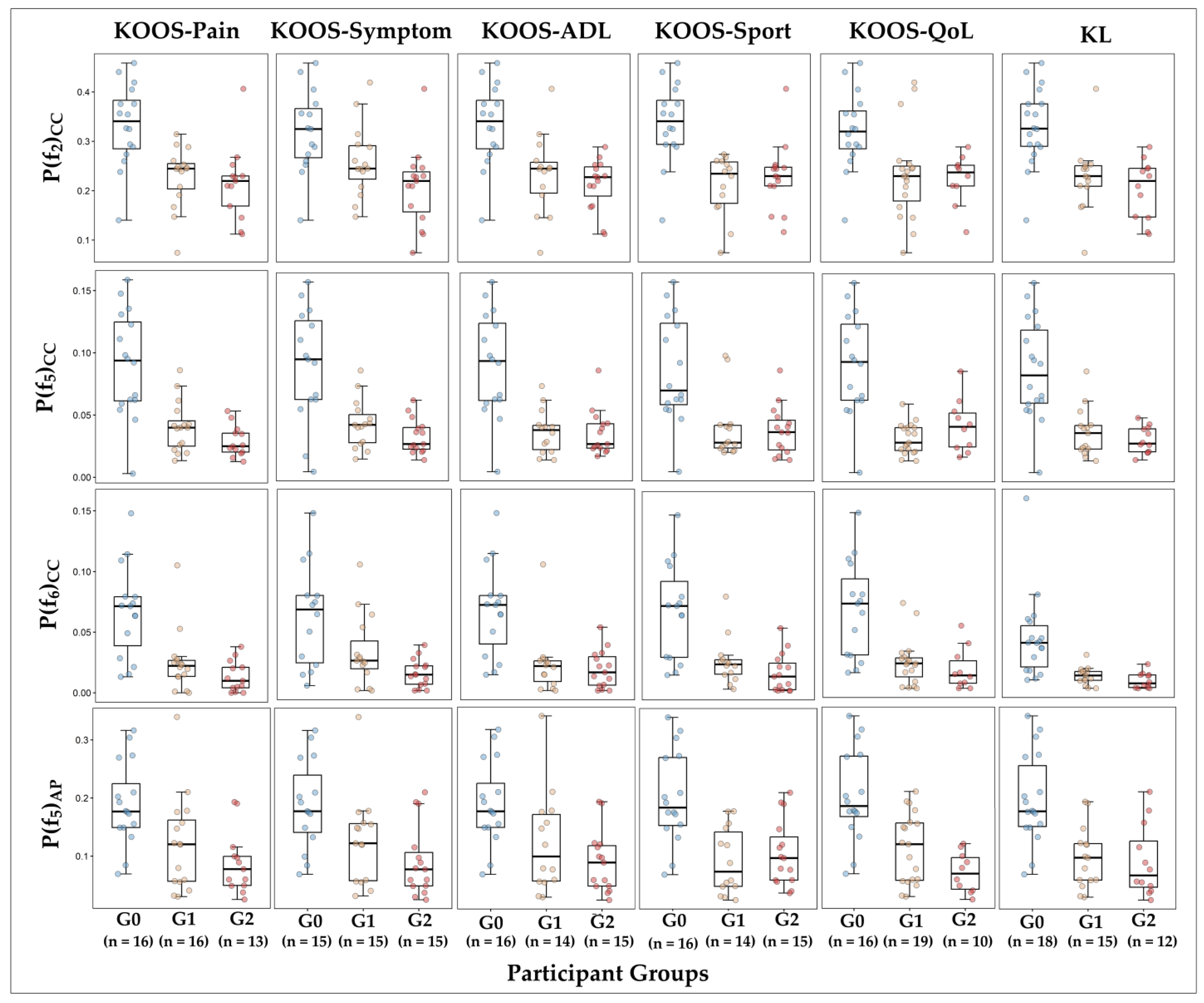
3.5. Selected Features vs. Severity of Knee OA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mills, K.; Hunt, M.A.; Ferber, R. Biomechanical deviations during level walking associated with knee osteoarthritis: A systematic review and meta-analysis. Arthritis Care Res. 2013, 65, 1643–1665. [Google Scholar] [CrossRef] [Green Version]
- Renggli, D.; Graf, C.; Tachatos, N.; Singh, N.; Meboldt, M.; Taylor, W.R.; Stieglitz, L.; Daners, M.S. Wearable Inertial Measurement Units for Assessing Gait in Real-World Environments. Front. Physiol. 2020, 11, 90. [Google Scholar] [CrossRef]
- Rose, M.J.; Costello, K.E.; Eigenbrot, S.; Torabian, K.; Kumar, D. Inertial Measurement Units and Application for Remote Health Care in Hip and Knee Osteoarthritis: Narrative Review. JMIR Rehabil. Assist. Technol. 2022, 9, e33521. [Google Scholar] [CrossRef]
- Ismailidis, P.; Egloff, C.; Hegglin, L.; Pagenstert, G.; Kernen, R.; Eckardt, A.; Ilchmann, T.; Mündermann, A.; Nüesch, C. Kinematic changes in patients with severe knee osteoarthritis are a result of reduced walking speed rather than disease severity. Gait Posture 2020, 79, 256–261. [Google Scholar] [CrossRef]
- Odonkor, C.; Kuwabara, A.; Tomkins-Lane, C.; Zhang, W.; Muaremi, A.; Leutheuser, H.; Sun, R.; Smuck, M. Gait features for discriminating between mobility-limiting musculoskeletal disorders: Lumbar spinal stenosis and knee osteoarthritis. Gait Posture 2020, 80, 96–100. [Google Scholar] [CrossRef]
- Tadano, S.; Takeda, R.; Sasaki, K.; Fujisawa, T.; Tohyama, H. Gait characterization for osteoarthritis patients using wearable gait sensors (H-Gait systems). J. Biomech. 2016, 49, 684–690. [Google Scholar] [CrossRef]
- Van Der Straaten, R.; Wesseling, M.; Jonkers, I.; Vanwanseele, B.; Bruijnes, A.; Malcorps, J.; Bellemans, J.; Truijen, J.; De Baets, L.; Timmermans, A. Functional movement assessment by means of inertial sensor technology to discriminate between movement behaviour of healthy controls and persons with knee osteoarthritis. J. Neuroeng. Rehabil. 2020, 17, 65. [Google Scholar] [CrossRef]
- Tanimoto, K.; Takahashi, M.; Tokuda, K.; Sawada, T.; Anan, M.; Shinkoda, K. Lower limb kinematics during the swing phase in patients with knee osteoarthritis measured using an inertial sensor. Gait Posture 2017, 57, 236–240. [Google Scholar] [CrossRef] [Green Version]
- Barrois, R.; Gregory, T.; Oudre, L.; Moreau, T.; Truong, C.; Pulini, A.A.; Vienne, A.; Labourdette, C.; Vayatis, N.; Buffat, S.; et al. An automated recording method in clinical consultation to rate the limp in lower limb osteoarthritis. PLoS ONE 2016, 11, e0164975. [Google Scholar] [CrossRef]
- Na, A.; Buchanan, T.S. Validating Wearable Sensors Using Self-Reported Instability among Patients with Knee Osteoarthritis. PM R 2021, 13, 119–127. [Google Scholar] [CrossRef]
- Honert, E.C.; Pataky, T.C. Timing of gait events affects whole trajectory analyses: A statistical parametric mapping sensitivity analysis of lower limb biomechanics. J. Biomech. 2021, 119, 110329. [Google Scholar] [CrossRef]
- Pataky, T.C. Generalized n-dimensional biomechanical field analysis using statistical parametric mapping. J. Biomech. 2010, 43, 1976–1982. [Google Scholar] [CrossRef]
- Deluzio, K.J.; Astephen, J.L. Biomechanical features of gait waveform data associated with knee osteoarthritis. An application of principal component analysis. Gait Posture 2007, 25, 86–93. [Google Scholar] [CrossRef]
- Begg, R.; Kamruzzaman, J. A machine learning approach for automated recognition of movement patterns using basic, kinetic and kinematic gait data. J. Biomech. 2005, 38, 401–408. [Google Scholar] [CrossRef]
- Agostini, V.; Nascimbeni, A.; Gaffuri, A.; Imazio, P.; Benedetti, M.G.; Knaflitz, M. Normative EMG activation patterns of school-age children during gait. Gait Posture 2010, 32, 285–289. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.A.; Simon, S.; Olshen, R.A. Statistical analysis of gait patterns of persons with cerebral palsy. Stat. Med. 1983, 2, 345–354. [Google Scholar] [CrossRef] [Green Version]
- Long, J.T.; Klein, J.P.; Sirota, N.M.; Wertsch, J.J.; Janisse, D.; Harris, G.F. Biomechanics of the Double Rocker Sole Shoe: Gait Kinematics and Kinetics. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2004, 7, 5107–5110. [Google Scholar] [CrossRef] [Green Version]
- Giakas, G.; Baltzopoulos, V. Time and frequency domain analysis of ground reaction forces during walking: An investigation of variability and symmetry. Gait Posture 1997, 5, 189–197. [Google Scholar] [CrossRef]
- Schneider, E.; Chao, E.Y. Fourier analysis of ground reaction forces in normals and patients with knee joint disease. J. Biomech. 1983, 16, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Chao, E. Gait analysis: A survey. In Biomechanics: Basic and Applied Research, Selected Proceedings of the Fifth Meeting, European Society of Biomechanics, Berlin, Germany, 8–10 September 1986; Bergmann, G., Kölbel, R., Rohlmann, A., Eds.; Springer: Berlin, Germany, 1987; pp. 33–50. [Google Scholar]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)--development of a self-administered outcome measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886. [Google Scholar] [CrossRef] [Green Version]
- Ghaffari, A.; Rahbek, O.; Lauritsen, R.E.K.; Kappel, A.; Kold, S.; Rasmussen, J. Criterion Validity of Linear Accelerations Measured with Low-Sampling-Frequency Accelerometers during Overground Walking in Elderly Patients with Knee Osteoarthritis. Sensors 2022, 22, 5289. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.S.; Kristensen, M.T.; Josefsen, C.O.; Lykkegaard, K.L.; Jønsson, L.R.; Pedersen, M.M. Validation of Two Activity Monitors in Slow and Fast Walking Hospitalized Patients. Rehabil. Res. Pract. 2022, 2022, 9230081. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. Biomechanics and Motor Control of Human Movement, 4th ed.; Wiley: New York, NY, USA, 2009. [Google Scholar] [CrossRef]
- Derrick, T.R. Signal Processing. In Research Methods in Biomechanics; Robertson, D.G.E., Caldwell, G.E., Hamil, J., Kamen, G., Whittlesey, S.N., Eds.; Human Kinetics: Champaign, IL, USA, 2013; pp. 279–290. [Google Scholar]
- Van Rossum, G.; Drake, F.L. Python 3 Reference Manual; CreateSpace: Scotts Valley, CA, USA, 2009. [Google Scholar]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 5 December 2022).
- Friedman, J.H.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhn, M. Building Predictive Models in R Using the caret Package. J. Stat. Softw. 2008, 28, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Simon, N.; Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Cox’s Proportional Hazards Model via Coordinate Descent. J. Stat. Softw. 2011, 39, 1–13. [Google Scholar] [CrossRef]
- Taylor, J.; Tibshirani, R. Post-selection inference for L1-penalized likelihood models. Can. J. Stat. 2016, 46, 41–61. [Google Scholar] [CrossRef]
- Hung, S.W.; Shih, Y.F.; Chiang, W.H.; Chen, W.Y. Vertical and mediolateral knee acceleration during level walking in individuals with medialcompartment knee osteoarthritis and a lateral thrust gait. Physiotherapy 2015, 101, e615–e616. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhou, X.; Pijnappels, M.; Bruijn, S.M. Differences in Gait Stability and Acceleration Characteristics between Healthy Young and Older Females. Front. Rehabil. Sci. 2021, 2, 763309. [Google Scholar] [CrossRef]
- Levinger, P.; Lai, D.T.H.; Begg, R.; Menz, H.; Feller, J.; Webster, K. Fourier analysis of tibia acceleration in subjects with knee oste-oarthritis: Preliminary results. In Proceedings of the ISSNIP 2008—2008 International Conference on Intelligent Sensors, Sensor Networks and Information Processing, Sydney, NSW, Australia, 15–18 December 2008; pp. 315–320. [Google Scholar] [CrossRef]
- Bedson, J.; Croft, P.R. The discordance between clinical and radiographic knee osteoarthritis: A systematic search and summary of the literature. BMC Musculoskelet. Disord. 2008, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). International Classification of Functioning, Disability, and Health; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Khera, P.; Kumar, N. Role of machine learning in gait analysis: A review. J. Med. Eng. Technol. 2020, 44, 441–467. [Google Scholar] [CrossRef] [PubMed]
- Pourhoseingholi, M.A.; Baghestani, A.R.; Vahedi, M. How to control confounding effects by statistical analysis. Gastroenterol. Hepatol. Bed Bench. 2012, 5, 79. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017459/ (accessed on 7 January 2023). [PubMed]
- Kobsar, D.; Barden, J.M.; Clermont, C.; Wilson, J.L.A.; Ferber, R. Sex differences in the regularity and symmetry of gait in older adults with and without knee osteoarthritis. Gait Posture 2022, 95, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Judge, J.O.; Ounpuu, S.; Davis, R.B. Effects of Age on the Biomechanics and Physiology of Gait. Clin. Geriatr. Med. 1996, 12, 659–678. [Google Scholar] [CrossRef]
- Rosso, V.; Agostini, V.; Takeda, R.; Tadano, S.; Gastaldi, L. Influence of BMI on Gait Characteristics of Young Adults: 3D Evalu-ation Using Inertial Sensors. Sensors 2019, 19, 4221. [Google Scholar] [CrossRef] [Green Version]
- Kobsar, D.; Charlton, J.M.; Hunt, M.A. Individuals with knee osteoarthritis present increased gait pattern deviations as measured by a knee-specific gait deviation index. Gait Posture 2019, 72, 82–88. [Google Scholar] [CrossRef]
- Astephen Wilson, J.L. Challenges in dealing with walking speed in knee osteoarthritis gait analyses. Clin. Biomech. 2012, 27, 210–212. [Google Scholar] [CrossRef]
- Oishi, K.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Sasaki, E.; Chiba, D.; Takahashi, I.; Nakaji, S.; Ishibashi, Y. The Knee injury and Osteoarthritis Outcome Score reflects the severity of knee osteoarthritis better than the revised Knee Society Score in a general Japanese population. Knee 2016, 23, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Doherty, M.; Peat, G.; Bierma-Zeinstra, M.A.; Arden, N.K.; Bresnihan, B.; Herrero-Beaumont, G.; Kirschner, S.; Leeb, B.F.; Lohmander, S.; et al. EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis. Ann. Rheum. Dis. 2010, 69, 483–489. [Google Scholar] [CrossRef] [Green Version]
- Nyquist, H.; Nyquist, H. Certain Topics in Telegraph Transmission Theory. Trans. Am. Inst. Electr. Eng. 1928, 47, 617–624. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Type | Description | |
|---|---|---|---|
| Explanatory variables | Age | Continuous | Age in years |
| Sex | Binomial | Male/female | |
| BMI | Continuous | Body mass index as kg/m2 | |
| ω | Continuous | The fundamental angular stride frequency of gait acceleration signals | |
| Power | Continuous | 18 variables regarding the power of the signal at the first six frequencies of the CC 1, AP 2, and ML 3 axes | |
| Outcome variable | Knee OA | Binomial | Yes/no |
| Variable | Control (n = 18) | Patients (n = 27) | 95% CI 1 (Differences of Means) | p-Value | |
|---|---|---|---|---|---|
| Female sex (n (%)) | 11 (61) | 15 (56) | - | 0.9 | |
| Age (years) | 60.8 ± 5.4 | 67.2 ± 9.4 | (−10.9, −2.0) | 0.006 | |
| BMI (kg/m2) | 23.7 ± 3.0 | 27.7 ± 3.8 | (−6.1 −2.0) | 0.0003 | |
| Pain score 2 | Ipsilateral knee | - | 4.3 ± 2.2 | - | - |
| Contralateral knee | - | 0.3 ± 0.7 | - | - | |
| KOOS 3 | Pain | 99.7 ± 0.9 | 53.6 ± 17.2 | (36.1, 52.8) | <0.0001 |
| Symptom | 96.8 ± 5.3 | 58.3 ± 23.2 | (28.6, 46.4) | <0.0001 | |
| ADL 4 | 99.3 ± 1.0 | 60.4 ± 16.4 | (30.9, 48.5) | <0.0001 | |
| Sport | 96.7 ± 5.4 | 26.0 ± 20.5 | (65.0, 80.0) | <0.0001 | |
| QoL 5 | 97.2 ± 4.4 | 38.2 ± 15.3 | (56.2, 62.5) | <0.0001 | |
| Knee OA severity 6,7 | 0 (n (%)) | - | 0 | - | - |
| 1 (n (%)) | - | 7 (26) | - | - | |
| 2 (n (%)) | - | 8 (30) | - | - | |
| 3 (n (%)) | - | 9 (33) | - | - | |
| 4 (n (%)) | - | 3 (11) | - | - | |
| Painful knee | Right (n (%)) | - | 14 (52) | - | - |
| Left (n (%)) | - | 13 (48) | - | - | |
| Cadence (Steps/minute) | 118 [112, 128] | 109 [83, 134] | (5, 16) | 0.001 | |
| Variable | Control (n = 18) | Patient (n = 27) | Differences of Means (95% CI) | p-Value | |
|---|---|---|---|---|---|
| ω 1 | 6.16 [5.90, 6.68] | 5.7 [4.34, 6.92] | (0.18, 0.64) | 0.001 | |
| CC axis | P(f1)CC | 0.15 [0.06, 0.25] | 0.10 [0.02, 0.16] | (0.03, 0.07) | <0.0001 |
| P(f2)CC | 0.33 [0.14, 0.46] | 0.21 [0.07, 0.29] | (0.07, 0.16) | <0.0001 | |
| P(f3)CC | 0.20 [0.10, 0.30] | 0.11 [0.01, 0.18] | (0.05, 0.12) | <0.0001 | |
| P(f4)CC | 0.11 [0.02, 0.46] | 0.05 [0.01, 0.40] | (0.03, 0.07) | <0.0001 | |
| P(f5)CC | 0.08 [0.00, 0.14] | 0.04 [0.01, 0.09] | (0.03, 0.06) | <0.0001 | |
| P(f6)CC | 0.08 [0.02, 0.30] | 0.02 [0.00, 0.18] | (0.03, 0.07) | <0.0001 | |
| AP axis | P(f1)AP | 0.16 [0.07, 0.35] | 0.09 [0.02, 0.29] | (0.05, 0.10) | <0.0001 |
| P(f2)AP | 0.42 [0.14, 0.58] | 0.29 [0.05, 0.44] | (0.06, 0.18) | 0.0002 | |
| P(f3)AP | 0.26 [0.07, 0.44] | 0.19 [0.02, 0.33] | (0.01, 0.12) | 0.02 | |
| P(f4)AP | 0.26 [0.11, 0.57] | 0.12 [0.02, 0.44] | (0.06, 0.18) | 0.0001 | |
| P(f5)AP | 0.20 [0.07, 0.34] | 0.09 [0.01, 0.21] | (0.08, 0.15) | <0.0001 | |
| P(f6)AP | 0.10 [0.01, 0.36] | 0.04 [0.00, 0.22] | (0.01, 0.09) | 0.003 | |
| ML axis | P(f1)ML | 0.08 [0.01, 0.15] | 0.06 [0.00, 0.13] | (−0.01, 0.04) | 0.2 |
| P(f2)ML | 0.12 [0.02, 0.26] | 0.07 [0.02, 0.17] | (0.03, 0.08) | 0.003 | |
| P(f3)ML | 0.09 [0.03, 0.15] | 0.04 [0.00, 0.09] | (0.03, 0.07) | 0.0002 | |
| P(f4)ML | 0.07 [0.00, 0.20] | 0.05 [0.00, 0.17] | (−0.01, 0.04) | 0.3 | |
| P(f5)ML | 0.06 [0.02, 0.22] | 0.02 [0.00, 0.07] | (0.01, 0.05) | 0.005 | |
| P(f6)ML | 0.08 [0.00, 0.28] | 0.03 [0.00, 0.15] | (0.03, 0.06) | 0.0001 | |
| Variable | Coefficient [95% CI] | p-Value | |
|---|---|---|---|
| Sex | - | - | |
| Age | - | - | |
| BMI | - | - | |
| ω | - | - | |
| CC axis | P(f1)CC | - | - |
| P(f2)CC | −0.66 [−0.81, −0.50] | <0.0001 | |
| P(f3)CC | - | - | |
| P(f4)CC | - | - | |
| P(f5)CC | −0.62 [−0.96, −0.39] | <0.0001 | |
| P(f6)CC | −0.34 [−0.46, −0.21] | <0.0001 | |
| AP axis | P(f1)AP | - | - |
| P(f2)AP | - | - | |
| P(f3)AP | - | - | |
| P(f4)AP | - | - | |
| P(f5)AP | −0.41 [−0.62, −0.22] | <0.0001 | |
| P(f6)AP | - | - | |
| ML axis | P(f1)ML | - | - |
| P(f2)ML | - | - | |
| P(f3)ML | - | - | |
| P(f4)ML | - | - | |
| P(f5)ML | - | - | |
| P(f6)ML | −0.08 [−0.13, 0.07] | 0.1 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghaffari, A.; Rasmussen, J.; Kold, S.; Lauritsen, R.E.K.; Kappel, A.; Rahbek, O. Accelerations Recorded by Simple Inertial Measurement Units with Low Sampling Frequency Can Differentiate between Individuals with and without Knee Osteoarthritis: Implications for Remote Health Care. Sensors 2023, 23, 2734. https://doi.org/10.3390/s23052734
Ghaffari A, Rasmussen J, Kold S, Lauritsen REK, Kappel A, Rahbek O. Accelerations Recorded by Simple Inertial Measurement Units with Low Sampling Frequency Can Differentiate between Individuals with and without Knee Osteoarthritis: Implications for Remote Health Care. Sensors. 2023; 23(5):2734. https://doi.org/10.3390/s23052734
Chicago/Turabian StyleGhaffari, Arash, John Rasmussen, Søren Kold, Rikke Emilie Kildahl Lauritsen, Andreas Kappel, and Ole Rahbek. 2023. "Accelerations Recorded by Simple Inertial Measurement Units with Low Sampling Frequency Can Differentiate between Individuals with and without Knee Osteoarthritis: Implications for Remote Health Care" Sensors 23, no. 5: 2734. https://doi.org/10.3390/s23052734