
Association of Heart Rate Variability with Pulmonary Function Impairment and Symptomatology Post-COVID-19 Hospitalization
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Heart Rate Variability
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Study Population
3.2. Baseline Characteristics
3.3. Pulmonary Function Tests
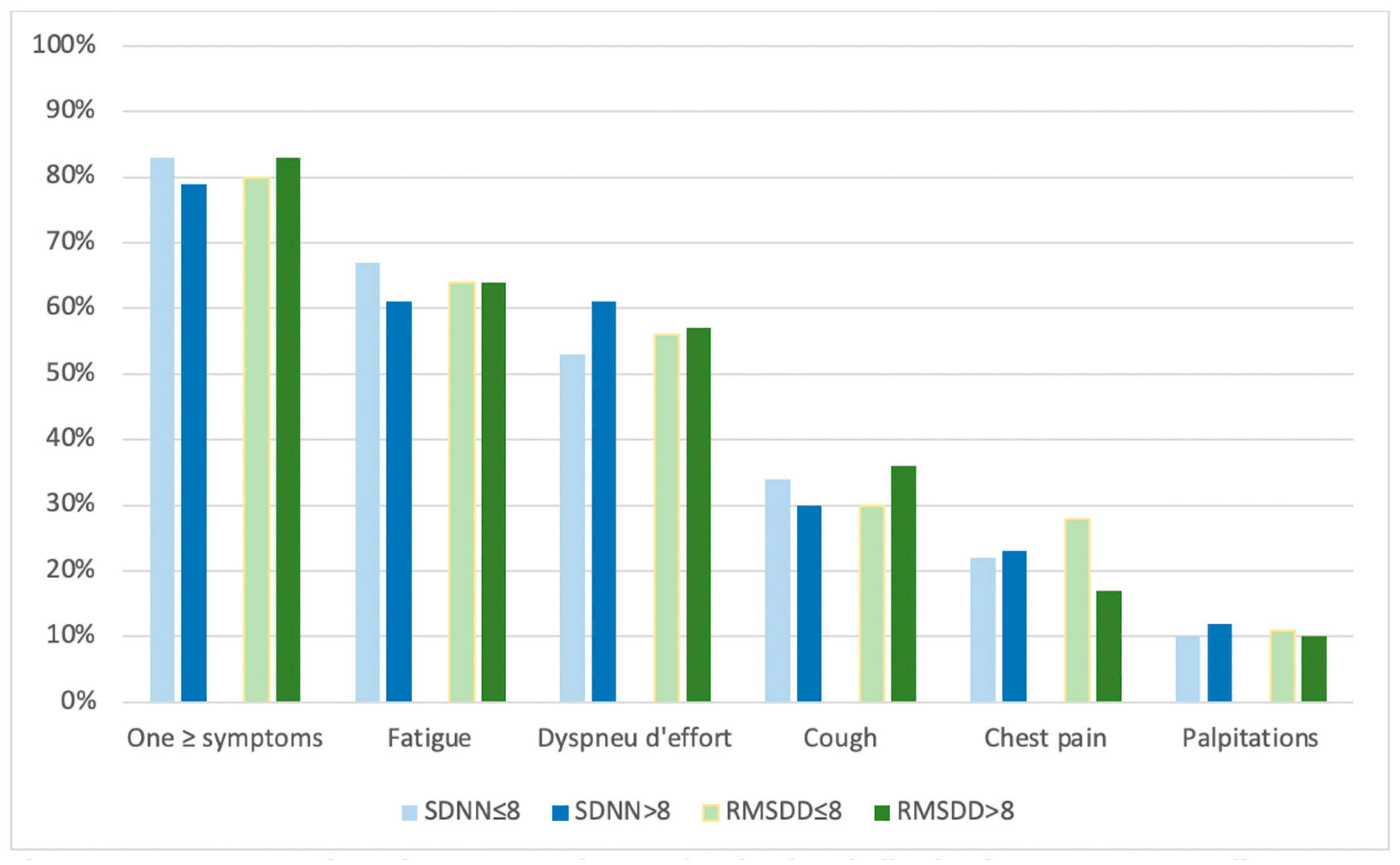
3.4. Number of Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 1 June 2022).
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. Eclinicalmedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.W.; Shah, A.S.; Johnston, J.C.; Carlsten, C.; Ryerson, C.J. Patient-reported outcome measures after COVID-19: A prospective cohort study. Eur. Respir. J. 2020, 56, 2003276. [Google Scholar] [CrossRef] [PubMed]
- Todt, B.C.; Szlejf, C.; Duim, E.; Linhares, A.O.; Kogiso, D.; Varela, G.; Campos, B.A.; Fonseca, C.M.B.; Polesso, L.E.; Bordon, I.N.; et al. Clinical outcomes and quality of life of COVID-19 survivors: A follow-up of 3 months post hospital discharge. Respir. Med. 2021, 184, 106453. [Google Scholar] [CrossRef]
- Malik, P.; Patel, K.; Pinto, C.; Jaiswal, R.; Tirupathi, R.; Pillai, S.; Patel, U. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)—A systematic review and meta-analysis. J. Med. Virol. 2022, 94, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.A.; McAuley, H.; Harrison, E.M.; Shikotra, A.; Singapuri, A.; Sereno, M.; Elneima, O.; Docherty, A.B.; Lone, N.I.; Leavy, O.C.; et al. Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): A UK multicentre, prospective cohort study. Lancet Respir. Med. 2021, 9, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.J.; Williams, D.M.; Walker, A.J.; Mitchell, R.E.; Niedzwiedz, C.L.; Yang, T.C.; Huggins, C.F.; Kwong, A.S.F.; Silverwood, R.J.; Gessa, G.D.; et al. Risk Factors for Long COVID: Analyses of 10 Longitudinal Studies and Electronic Health Records in the UK. medRxiv 2021, 2021, 21259277. [Google Scholar]
- Whitaker, M.; Elliott, J.; Chadeau-Hyam, M.; Riley, S.; Darzi, A.; Cooke, G.; Ward, H.; Elliott, P. Persistent symptoms following SARS-CoV-2 in-fection in a random community sample of 508,707 people. medRxiv 2021, 2021, 21259452. [Google Scholar]
- Peghin, M.; Palese, A.; Venturini, M.; De Martino, M.; Gerussi, V.; Graziano, E.; Bontempo, G.; Marrella, F.; Tommasini, A.; Fabris, M.; et al. Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin. Microbiol. Infect. 2021, 27, 1507–1513. [Google Scholar] [CrossRef]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic dysfunction in ‘long COVID’: Rationale, physiology and management strategies. Clin. Med. 2021, 21, e63–e67. [Google Scholar] [CrossRef]
- Bonaz, B.; Sinniger, V.; Pellissier, S. Anti-inflammatory properties of the vagus nerve: Potential therapeutic implications of vagus nerve stimulation. J. Physiol. 2016, 594, 5781–5790. [Google Scholar] [CrossRef] [Green Version]
- Rosas-Ballina, M.; Olofsson, P.S.; Ochani, M.; Valdés-Ferrer, S.I.; Levine, Y.A.; Reardon, C.; Tusche, M.W.; Pavlov, V.A.; Andersson, U.; Chavan, S.; et al. Acetylcholine-Synthesizing T Cells Relay Neural Signals in a Vagus Nerve Circuit. Science 2011, 334, 98–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olofsson, P.S.; Rosas-Ballina, M.; Levine, Y.A.; Tracey, K.J. Rethinking inflammation: Neural circuits in the regulation of immunity. Immunol. Rev. 2012, 248, 188–204. [Google Scholar] [CrossRef] [Green Version]
- Ohira, H.; Matsunaga, M.; Osumi, T.; Fukuyama, S.; Shinoda, J.; Yamada, J.; Gidron, Y. Vagal nerve activity as a moderator of brain–immune relationships. J. Neuroimmunol. 2013, 260, 28–36. [Google Scholar] [CrossRef]
- Qin, W.; Chen, S.; Zhang, Y.; Dong, F.; Zhang, Z.; Hu, B.; Zhu, Z.; Li, F.; Wang, X.; Wang, Y.; et al. Diffusion Capacity Abnormalities for Carbon Monoxide in Patients with COVID-19 At Three-Month Follow-up. Eur. Respir. J. 2021, 58, 2003677. [Google Scholar] [CrossRef]
- Rangon, C.-M.; Krantic, S.; Moyse, E.; Fougère, B. The Vagal Autonomic Pathway of COVID-19 at the Crossroad of Alzheimer’s Disease and Aging: A Review of Knowledge. J. Alzheimer’s Dis. Rep. 2020, 4, 537–551. [Google Scholar] [CrossRef]
- Becker, R.C. Autonomic dysfunction in SARS-CoV-2 infection acute and long-term implications COVID-19 editor’s page series. J. Thromb. Thrombolysis 2021, 52, 692–707. [Google Scholar] [CrossRef] [PubMed]
- Acanfora, D.; Nolano, M.; Acanfora, C.; Colella, C.; Provitera, V.; Caporaso, G.; Rodolico, G.R.; Bortone, A.S.; Galasso, G.; Casucci, G. Impaired Vagal Activity in Long-COVID-19 Patients. Viruses 2022, 14, 1035. [Google Scholar] [CrossRef] [PubMed]
- EurekAlert! Pilot Study Suggests Long COVID Could Be Linked to The Effects of SARS-CoV-2 on The Vagus Nerve. Available online: http://www.eurekalert.org/news-releases/943102 (accessed on 1 June 2022).
- Dryden, M.; Mudara, C.; Vika, C.; Blumberg, L.; Mayet, N.; Cohen, C.; Tempia, S.; Parker, A.; Nel, J.; Perumal, R.; et al. Post-COVID-19 condition 3 months after hospitalisation with SARS-CoV-2 in South Africa: A prospective cohort study. Lancet Glob. Health 2022, 10, e1247–e1256. [Google Scholar] [CrossRef]
- WHO. Global COVID-19 Clinical Platform: Rapid Core Case Report Form (CRF). Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Clinical_CRF-2020.4 (accessed on 1 June 2022).
- Stanojevic, S.; Kaminsky, D.A.; Miller, M.R.; Thompson, B.; Aliverti, A.; Barjaktarevic, I.; Cooper, B.G.; Culver, B.; Derom, E.; Hall, G.L.; et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur. Respir. J. 2021, 60, 2101499. [Google Scholar] [CrossRef]
- Mccraty, R.; Shaffer, F. Heart Rate Variability: New Perspectives on Physiological Mechanisms, Assessment of Self-regulatory Capacity, and Health Risk. Glob. Adv. Health Med. 2015, 4, 46–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vollmer, M. Robust, Simple and Reliable Measure of Heart Rate Variability using Relative RR Intervals. In Proceedings of the Computing in Cardiology Conference, Nice, France, 6–9 September 2015; pp. 609–612. [Google Scholar] [CrossRef]
- Nussinovitch, U.; Elishkevitz, K.P.; Katz, K.; Nussinovitch, M.; Segev, S.; Volovitz, B.; Nussinovitch, N. Reliability of Ultra-Short ECG Indices for Heart Rate Variability. Ann. Noninvasive Electrocardiol. 2011, 16, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Mol, M.B.A.; Strous, M.T.A.; van Osch, F.H.M.; Vogelaar, F.J.; Barten, D.G.; Farchi, M.; Foudraine, N.A.; Gidron, Y. Heart-rate-variability (HRV), predicts outcomes in COVID-19. PLoS ONE 2021, 16, e0258841. [Google Scholar] [CrossRef] [PubMed]
- Munoz, M.L.; van Roon, A.; Riese, H.; Thio, C.; Oostenbroek, E.; Westrik, I.; de Geus, E.J.C.; Gansevoort, R.; Lefrandt, J.; Nolte, I.M.; et al. Validity of (Ultra-)Short Recordings for Heart Rate Variability Measurements. PLoS ONE 2015, 10, e0138921. [Google Scholar] [CrossRef] [Green Version]
- Guénard, H.; Rouatbi, S. Physiological aspects of the decline of pulmonary function with age. Rev. des Mal. Respir. 2004, 21, 8S13–24. [Google Scholar]
- LoMauro, A.; Aliverti, A. Sex differences in respiratory function. Breathe 2018, 14, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Bellemare, F.; Jeanneret, A.; Couture, J. Sex Differences in Thoracic Dimensions and Configuration. Am. J. Respir. Crit. Care Med. 2003, 168, 305–312. [Google Scholar] [CrossRef]
- Koenig, J.; Thayer, J.F. Sex differences in healthy human heart rate variability: A meta-analysis. Neurosci. Biobehav. Rev. 2016, 64, 288–310. [Google Scholar] [CrossRef]
- Zhao, Y.-M.; Shang, Y.-M.; Song, W.-B.; Li, Q.-Q.; Xie, H.; Xu, Q.-F.; Jia, J.-L.; Li, L.-M.; Mao, H.-L.; Zhou, X.-M.; et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. Eclinicalmedicine 2020, 25, 100463. [Google Scholar] [CrossRef]
- Wu, X.; Liu, X.; Zhou, Y.; Yu, H.; Li, R.; Zhan, Q.; Ni, F.; Fang, S.; Lu, Y.; Ding, X.; et al. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalisation: A prospective study. Lancet Respir. Med. 2021, 9, 747–754. [Google Scholar] [CrossRef]
- Sonnweber, T.; Sahanic, S.; Pizzini, A.; Luger, A.; Schwabl, C.; Sonnweber, B.; Kurz, K.; Koppelstätter, S.; Haschka, D.; Petzer, V.; et al. Cardiopulmonary recovery after COVID-19: An observational prospective multicentre trial. Eur. Respir. J. 2021, 57, 2003481. [Google Scholar] [CrossRef] [PubMed]
- Sibila, O.; Albacar, N.; Perea, L.; Faner, R.; Torralba, Y.; Hernandez-Gonzalez, F.; Moisés, J.; Sanchez-Ruano, N.; Sequeira-Aymar, E.; Badia, J.R.; et al. Lung Function sequelae in COVID-19 Patients 3 Months After Hospital Discharge. Arch. Bronconeumol. 2021, 57, 59–61. [Google Scholar] [CrossRef] [PubMed]
- Lerum, T.V.; Aaløkken, T.M.; Brønstad, E.; Aarli, B.; Ikdahl, E.; Lund, K.M.A.; Durheim, M.T.; Rodriguez, J.R.; Meltzer, C.; Tonby, K.; et al. Dyspnoea, lung function and CT findings 3 months after hospital admission for COVID-19. Eur. Respir. J. 2021, 57, 2003448. [Google Scholar] [CrossRef] [PubMed]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.M.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Adler, T.E.; Norcliffe-Kaufmann, L.; Condos, R.; Fishman, G.; Kwak, D.; Talmor, N.; Reynolds, H. Heart rate variability is reduced 3- AND 6-months after hospitalization for COVID-19 infection. J. Am. Coll. Cardiol. 2021, 77, 3062. [Google Scholar] [CrossRef]
- Bai, T.; Zhou, D.; Yushanjiang, F.; Wang, D.; Zhang, D.; Liu, X.; Song, J.; Zhang, J.; Hou, X.; Ma, Y. Alternation of the Autonomic Nervous System Is Associated With Pulmonary Sequelae in Patients With COVID-19 After Six Months of Discharge. Front. Physiol. 2021, 12. [Google Scholar] [CrossRef]
- Janszky, I.; Ericson, M.; Mittleman, M.; Wamala, S.; Al-Khalili, F.; Schenck-Gustafsson, K.; Orth-Gomer, K. Heart rate variability in long-term risk assessment in middle-aged women with coronary heart disease: The Stockholm Female Coronary Risk Study. J. Intern. Med. 2004, 255, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Shah, B.; Kunal, S.; Bansal, A.; Jain, J.; Poundrik, S.; Shetty, M.K.; Batra, V.; Chaturvedi, V.; Yusuf, J.; Mukhopadhyay, S.; et al. Heart rate variability as a marker of cardiovascular dysautonomia in post-COVID-19 syndrome using artificial intelligence. Indian Pacing Electrophysiol. J. 2022, 22, 70–76. [Google Scholar] [CrossRef]
- Marques, K.C.; Silva, C.C.; Trindade, S.D.S.; Santos, M.C.D.S.; Rocha, R.S.B.; Vasconcelos, P.F.D.C.; Quaresma, J.A.S.; Falcão, L.F.M. Reduction of Cardiac Autonomic Modulation and Increased Sympathetic Activity by Heart Rate Variability in Patients With Long COVID. Front. Cardiovasc. Med. 2022, 9, 862001. [Google Scholar] [CrossRef]
- Xhyheri, B.; Manfrini, O.; Mazzolini, M.; Pizzi, C.; Bugiardini, R. Heart Rate Variability Today. Prog. Cardiovasc. Dis. 2012, 55, 321–331. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total | SDNN ≤ 8 | SDNN > 8 | p-Value | RMSSD ≤ 8 | RMSDD > 8 | p-Value |
|---|---|---|---|---|---|---|---|
| N | 171 | 99 (58) | 72 (42) | 90 (53) | 81 (47) | ||
| Age in years, mean ± SD | 67 ± 11 | 65 ± 11 | 69 ± 11 | 0.031 | 65 ± 11 | 69 ± 11 | 0.031 |
| Sex, n (%) | 0.802 | 0.389 | |||||
| Male | 105 (61) | 60 (61) | 45 (63) | 58 (64) | 47 (58) | ||
| Female | 66 (39) | 39 (39) | 27 (38) | 32 (36) | 34 (42) | ||
| Comorbidities, n (%) | |||||||
| Chronic obstructive pulmonary disease | 37 (22) [7] | 18 (19) | 19 (28) | 0.194 | 17 (19) | 20 (26) | 0.285 |
| Chronic heart disease | 37 (23) [8] | 23 (24) | 14 (21) | 0.586 | 16 (18) | 21 (28) | 0.160 |
| Hypertension | 72 (42) | 41 (41) | 31 (43) | 0.830 | 36 (40) | 36 (44) | 0.557 |
| Obesity (BMI ≥ 30) | 59 (35) [2] | 35 (36) | 24 (33) | 0.711 | 29 (33) | 30 (37) | 0.578 |
| Diabetes | 42 (25) [2] | 26 (26) | 16 (22) | 0.545 | 28 (31) | 14 (17) | 0.036 |
| Hospital stay | |||||||
| Oxygen therapy, n (%) | 149 (87) | 91 (91) | 58 (81) | 0.028 | 80 (89) | 69 (85) | 0.470 |
| Days from admission to discharge | 6 {3–9} | 6 {3–10} | 6 {3–9} | 0.528 | 6 {3–10} | 6 {3–9} | 0.507 |
| Days from discharge to follow-up assessment | 119 {101–141} | 120 {101–144} | 118 {102–141} | 0.857 | 121 {102–144} | 117 {101–141} | 0.909 |
| Days from discharge to lung function assessment | 113 {98–134} | 113 {97–137} | 113 {98–134} | 0.939 | 112 {97–138} | 113 {98–133} | 0.949 |
| FEV1 | FEV1/FVC * | FVC | TLC | DLCO | PI | PE | ||
|---|---|---|---|---|---|---|---|---|
| <80% pred | n, (%) | 40 (23) | 14 (8) (1) | 26 (15) | 19 (12) [6] | 66 (41) [8] | 50 (31) (1) | 60 (37) (1) |
| SDNN > 8 | Unadjusted | 1.18 (0.57–2.38) | 1.02 (0.34–3.10) | 0.69 (0.29–1.65) | 0.31 (0.10–0.99) | 1.24 (0.66–2.33) | 0.93 (0.47–1.83) | 1.01 (0.53–1.92) |
| Model 1 | 1.07 (0.51–2.22) | 0.94 (0.31–2.90) | 0.69 (0.29–1.65) | 0.32 (0.10–1.02) | 1.08 (0.56–2.11) | 0.82 (0.40–1.66) | 0.89 (0.44–1.81) | |
| p | 0.865 | 0.920 | 0.400 | 0.055 | 0.813 | 0.580 | 0.755 | |
| RMSDD > 8 | Unadjusted | 1.15 (0.57–2.33) | 1.56 (0.52–4.70) | 0.94 (0.41–2.18) | 0.27 (0.08–0.84) | 0.91 (0.51–1.80) | 0.98 (0.50–1.92) | 1.02 (0.54–1.94) |
| Model 1 | 1.03 (0.50–2.15) | 1.41 (0.46–4.31) | 0.94 (0.41–2.19) | 0.28 (0.09–0.90) | 0.88 (0.46–1.70) | 0.92 (0.46–1.85) | 1.00 (0.50–2.00) | |
| p | 0.933 | 0.552 | 0.891 | 0.033 | 0.705 | 0.811 | 0.994 |
| Number of Symptoms | None | One | Two | Three to Five | |
|---|---|---|---|---|---|
| 32 (20) | 36 (23) | 40 (25) | 51 (32) | ||
| SDNN > 8 | Unadjusted | Reference category | 2.29 (0.84–6.28) | 0.72 (0.28–1.84) | 1.26 (0.52–3.07) |
| Model 1 | 2.37 (0.86–6.53) | 0.72 (0.28–1.84) | 1.23 (0.50–3.00) | ||
| p | 0.095 | 0.493 | 0.657 | ||
| RMSDD > 8 | Unadjusted | 1.09 (0.42–2.85) | 1.03 (0.42–2.50) | 1.03 (0.42–2.50) | |
| Model 1 | 1.10 (0.42–2.91) | 0.99 (0.40–2.43) | 0.99 (0.40–2.43) | ||
| p | 0.848 | 0.978 | 0.978 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adang, E.A.M.C.; Strous, M.T.A.; van den Bergh, J.P.; Gach, D.; van Kampen, V.E.M.; van Zeeland, R.E.P.; Barten, D.G.; van Osch, F.H.M. Association of Heart Rate Variability with Pulmonary Function Impairment and Symptomatology Post-COVID-19 Hospitalization. Sensors 2023, 23, 2473. https://doi.org/10.3390/s23052473
Adang EAMC, Strous MTA, van den Bergh JP, Gach D, van Kampen VEM, van Zeeland REP, Barten DG, van Osch FHM. Association of Heart Rate Variability with Pulmonary Function Impairment and Symptomatology Post-COVID-19 Hospitalization. Sensors. 2023; 23(5):2473. https://doi.org/10.3390/s23052473
Chicago/Turabian StyleAdang, Estelle A. M. C., Maud T. A. Strous, Joop P. van den Bergh, Debbie Gach, Vivian E. M. van Kampen, Roel E. P. van Zeeland, Dennis G. Barten, and Frits H. M. van Osch. 2023. "Association of Heart Rate Variability with Pulmonary Function Impairment and Symptomatology Post-COVID-19 Hospitalization" Sensors 23, no. 5: 2473. https://doi.org/10.3390/s23052473