
A Fiber-Optic Non-Invasive Swallowing Assessment Device Based on a Wearable Pressure Sensor

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
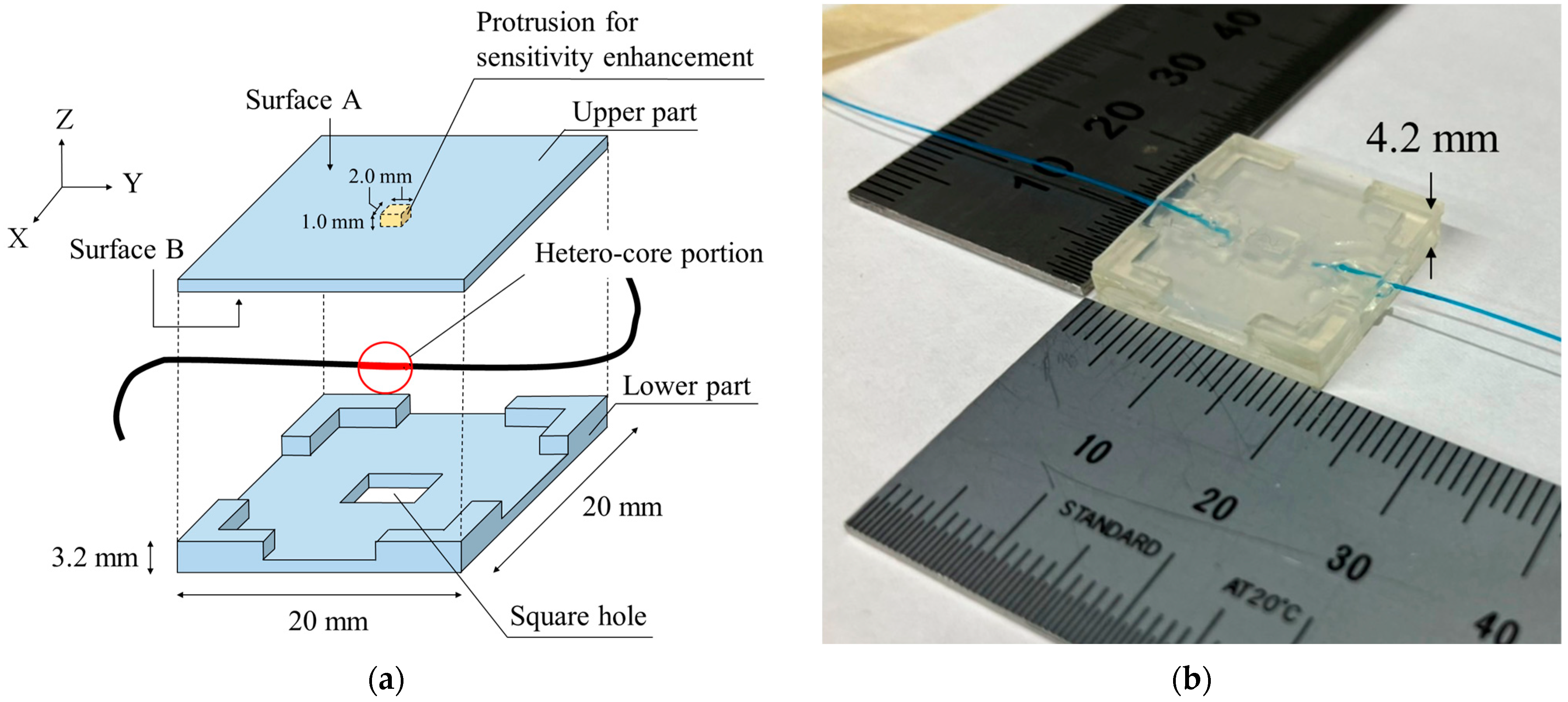
2.1. A Hetero-Core Fiber-Optic Pressure Sensor
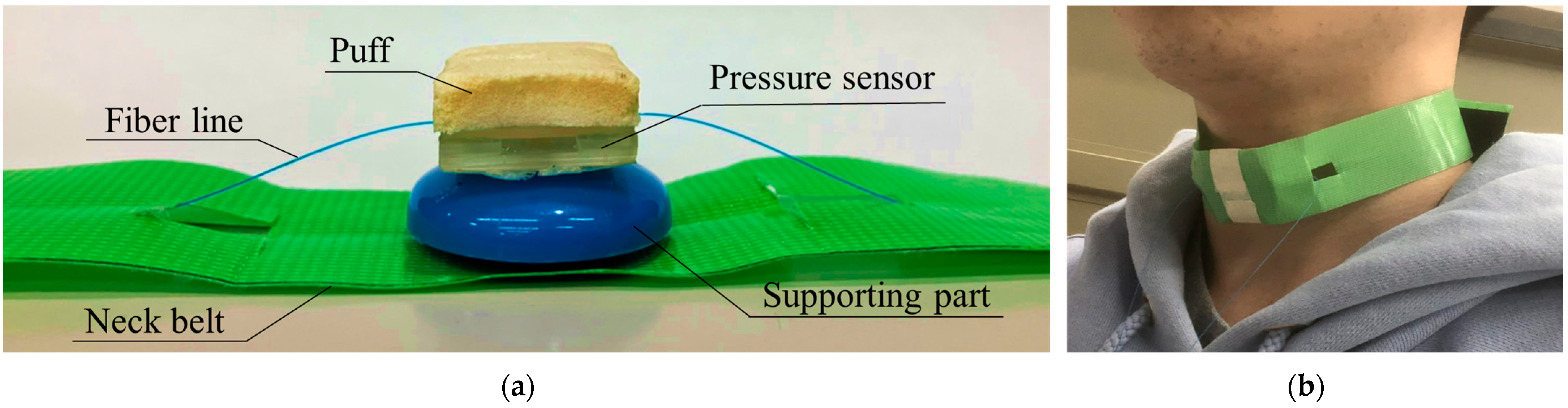
2.2. Wearable Swallowing Assessment Device Using the Hetero-Core Fiber-Optic Pressure Sensor
2.3. Experimental Setup
3. Results
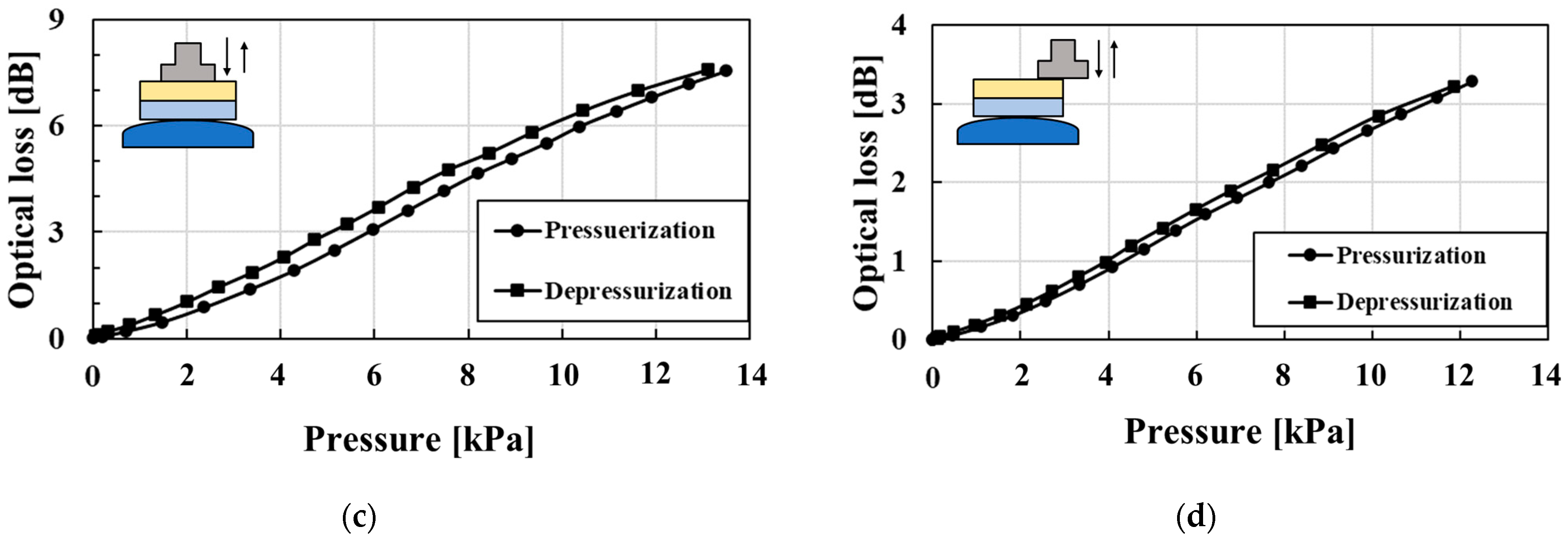
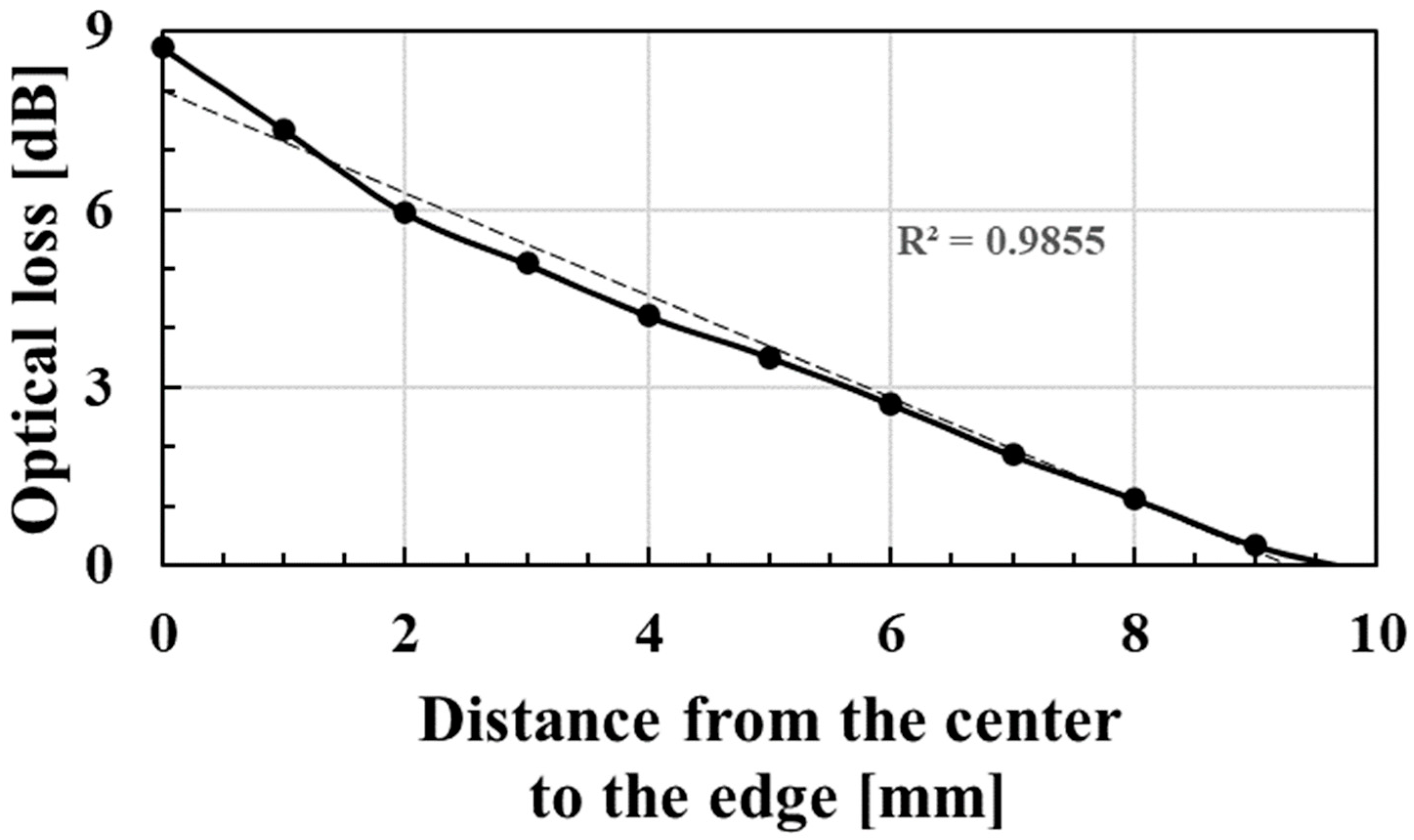
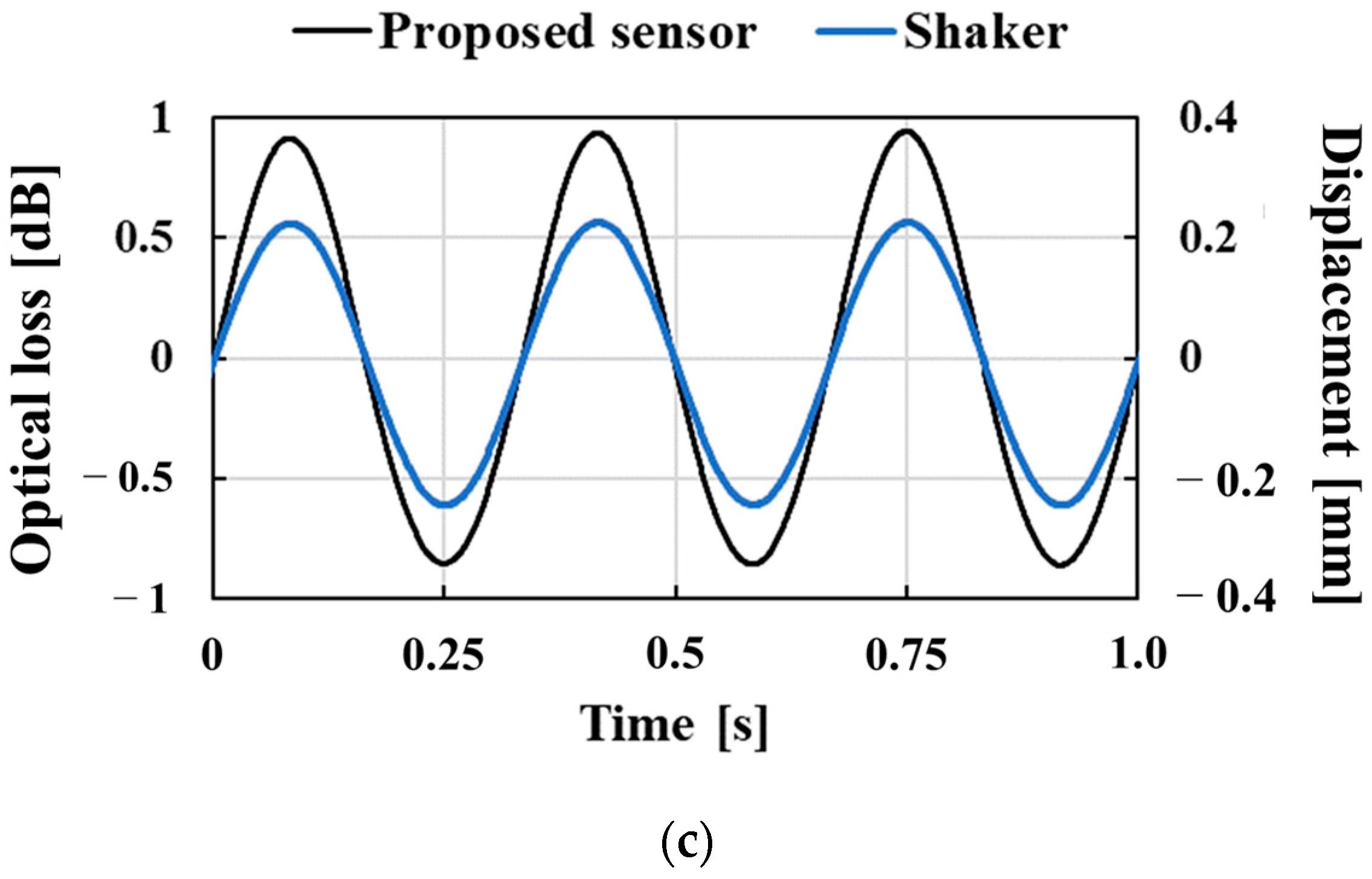
3.1. Characteristics of the Hetero-Core Fiber-Optic Pressure Sensor
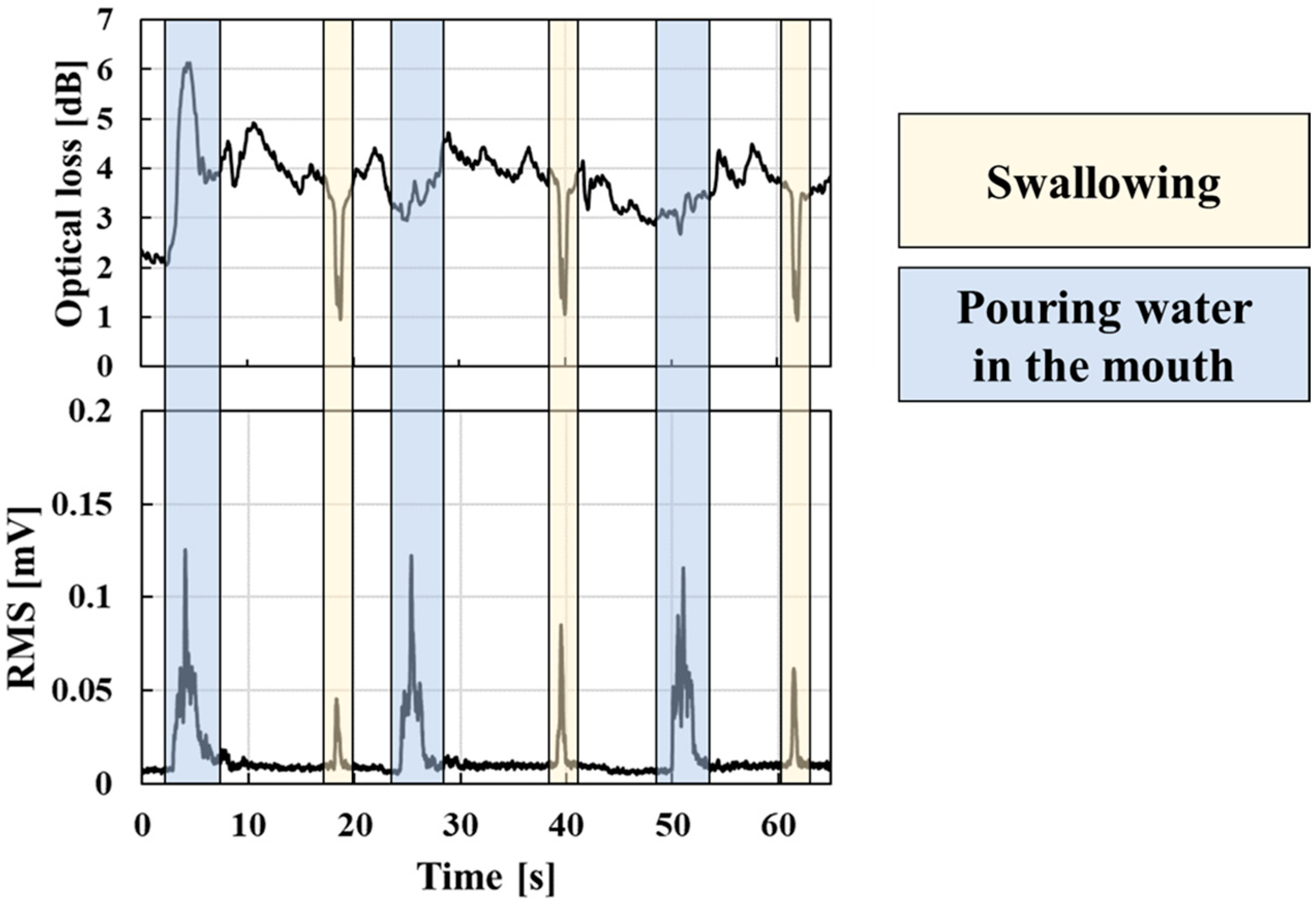
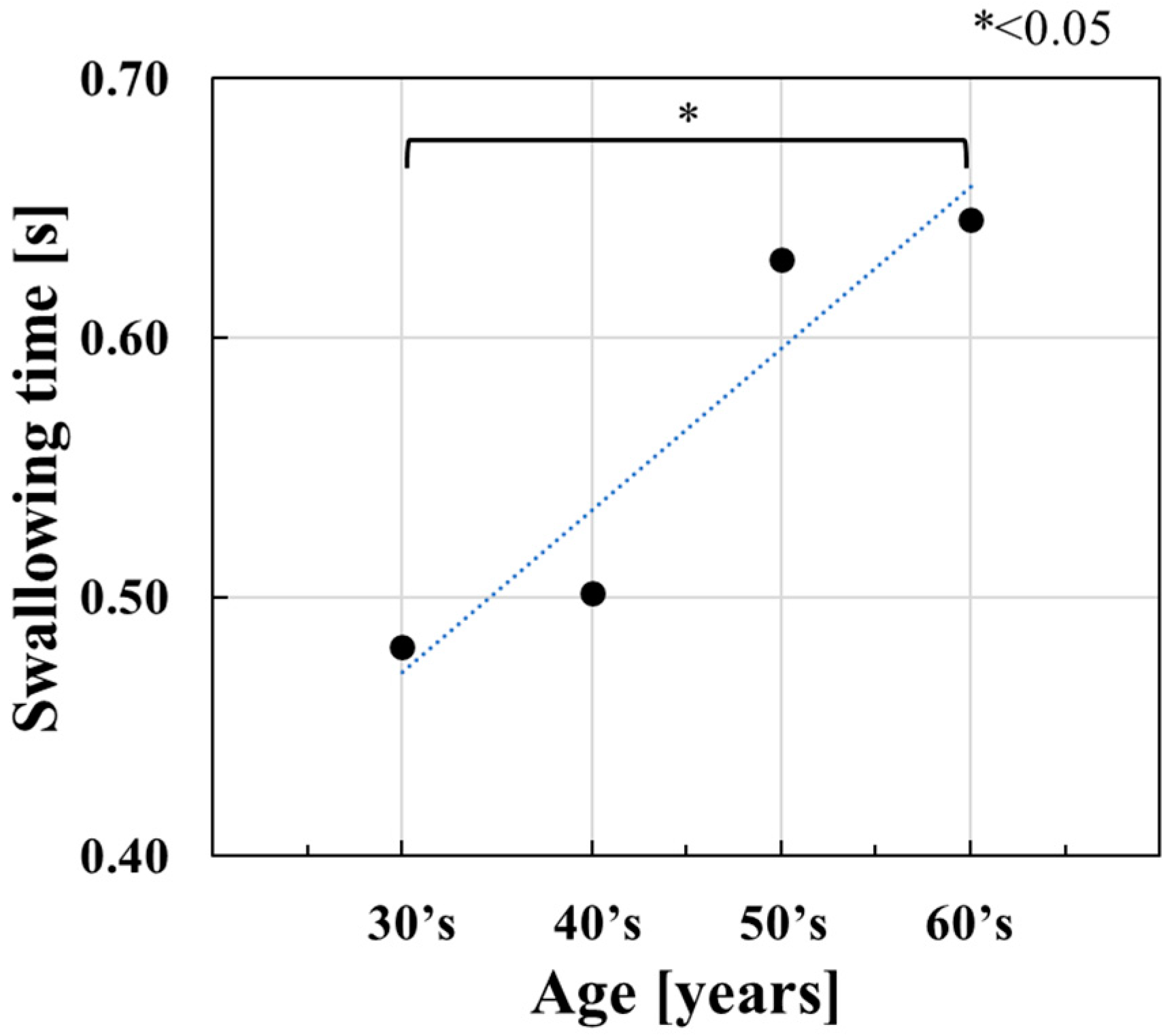
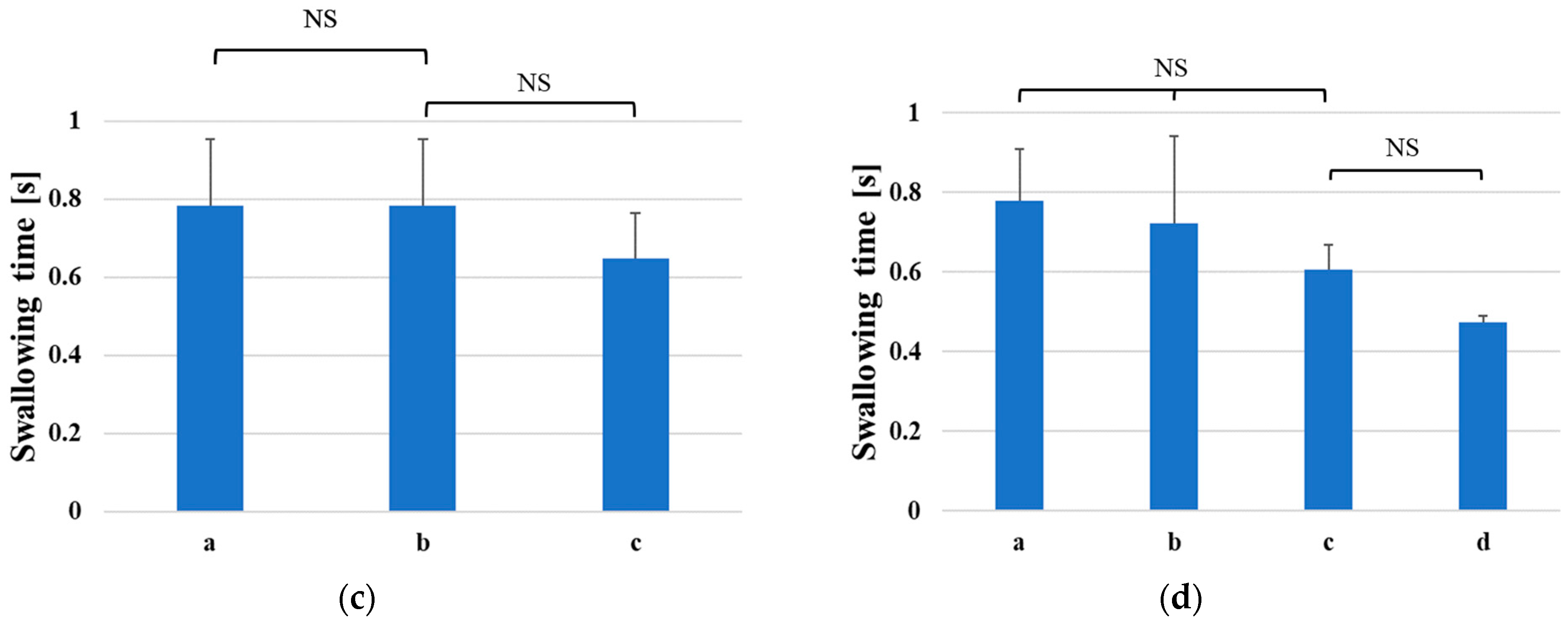
3.2. Evaluation of the Neck-Wearable Swallowing Device
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. The World Population Prospects 2019: Highlights; United Nations: New York, NY, USA, 2019. Available online: https://population.un.org/wpp/Publications/Files/WPP2019_Highlights.pdf (accessed on 30 November 2022).
- Gu, D.; Andreev, K.; Dupre, M.E. Major Trends in Population Growth Around the World. China CDC Wkly. 2021, 3, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Bloom, D.E.; Canning, D.; Fink, G. Implications of population ageing for economic growth. Oxf. Rev. Econ. Policy 2010, 26, 583–612. [Google Scholar] [CrossRef] [Green Version]
- Vesey, S. Dysphagia and quality of life. Br. J. Community Nurs. 2013, 18, S14–S19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smithard, D.; Hansjee, D.; Henry, D.; Mitchell, L.; Sabaharwal, A.; Salkeld, J.; Yeung, E.; Younus, O.; Swaine, I. Inter-Relationships between Frailty, Sarcopenia, Undernutrition and Dysphagia in Older People Who Are Admitted to Acute Frailty and Medical Wards: Is There an Older Adult Quartet? Geriatrics 2020, 5, 41. [Google Scholar] [CrossRef]
- Palacios-Ceña, D.; Hernández-Barrera, V.; López-de-Andrés, A.; Fernández-de-Las-Peñas, C.; Palacios-Ceña, M.; de Miguel-Díez, J.; Carrasco-Garrido, P.; Jiménez-García, R. Time trends in incidence and outcomes of hospitalizations for aspiration pneumonia among elderly people in Spain (2003–2013). Eur. J. Intern. Med. 2017, 38, 61–67. [Google Scholar] [CrossRef]
- Baijens, L.W.; Clavé, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders—European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, K. Cineradiographic analysis of laryngeal movement during deglutition. J. Otolaryngol. Jpn. 1984, 87, 169–181. (In Japanese) [Google Scholar]
- Chen, M.Y.; Lin, L.C. Nonimaging Clinical Assessment of Impaired Swallowing in Community-Dwelling Older Adults in Taiwan. J. Nurs. Res. 2012, 20, 272–280. [Google Scholar] [CrossRef] [Green Version]
- McCullough, G.H.; Kim, Y. Effects of the Mendelsohn Maneuver on Extent of Hyoid Movement and UES Opening Post-Stroke. Dysphagia 2013, 28, 511–519. [Google Scholar] [CrossRef]
- Martin-Harris, B.; Jones, B. The Videofluorographic Swallowing Study. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 769–785. [Google Scholar] [CrossRef] [Green Version]
- Bastian, R.W. Contemporary Diagnosis of the Dysphagic Patient. Otolaryngol. Clin. N. Am. 1998, 31, 489–506. [Google Scholar] [CrossRef] [PubMed]
- Bastian, R.W. The videoendoscopic swallowing study: An alternative and partner to the videofluoroscopic swallowing study. Dysphagia 1993, 8, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Santoso, L.F.; Baqai, F.; Gwozdz, M.; Lange, J.; Rosenberger, M.G.; Sulzer, J.; Paydarfar, D. Applying Machine Learning Algorithms for Automatic Detection of Swallowing from Sound. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 2584–2588. [Google Scholar]
- Honda, T.; Baba, T.; Fujimoto, K.; Goto, T.; Nagao, K.; Harada, M.; Honda, E.; Ichikawa, T. Characterization of Swallowing Sound: Preliminary Investigation of Normal Subjects. PLoS ONE 2016, 11, 12. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Hori, K.; Minagi, Y.; Ono, T.; Chen, Y.; Kondo, J.; Fujiwara, S.; Tamine, K.; Hayashi, H.; Inoue, M.; et al. Development of a System to Monitor Laryngeal Movement during Swallowing Using a Bend Sensor. PLoS ONE 2013, 8, 8. [Google Scholar] [CrossRef]
- Shieh, W.Y.; Wang, C.M.; Chang, C.S. Development of a Portable Non-Invasive Swallowing and Respiration Assessment Device. Sensors 2015, 15, 12428–12453. [Google Scholar] [CrossRef] [Green Version]
- Ono, T.; Hori, K.; Masuda, Y.; Hayashi, T. Recent Advances in Sensing Oropharyngeal Swallowing Function in Japan. Sensors 2010, 10, 176–202. [Google Scholar] [CrossRef] [Green Version]
- Nishiyama, M.; Miyamoto, M.; Watanabe, K. Respiration and body movement analysis during sleep in bed using hetero-core fiber optic pressure sensors without constraint to human activity. J. Biomed. Opt. 2011, 16, 017002. [Google Scholar] [CrossRef] [Green Version]
- Otsuka, Y.; Koyama, Y.; Watanabe, K. Monitoring of Plantar Pressure in Gait Based on Hetero-Core Optical Fiber Sensor. Procedia Eng. 2014, 87, 1465–1468. [Google Scholar] [CrossRef] [Green Version]
- Nishiyama, M.; Sonobe, M.; Watanabe, K. Unconstrained pulse pressure monitoring for health management using hetero-core fiber optic sensor. Biomed. Opt. Express 2016, 7, 3675–3685. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, H.; Kubota, Y.; Watanabe, K. A Hetero-Core Splice Fiber Optic Displacement Sensor and the Accuracy Evaluation. Trans. Soc. Instrum. Control. Eng. 2004, 40, 981–987. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Savović, S.; Djordjevich, A.; Savović, I. Theoretical investigation of bending loss in step-index plastic optical fibers. Opt. Commun. 2020, 475, 126200. [Google Scholar] [CrossRef]
- Interlink Electronics, Inc. FSR 402 Data Sheet. Available online: https://www.interlinkelectronics.com/ (accessed on 6 February 2023).


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Without the Puff and the Supporting Part | With the Puff | With the Puff and the Supporting Part | |||
|---|---|---|---|---|---|
| Pressurized position | Center | Edge | |||
| Pressurization | Sensitivity [dB/kPa] | 1.83 | 0.530 | 0.592 | 0.274 |
| R-square value | 0.962 | 0.996 | 0.995 | 0.996 | |
| Depressurization | Sensitivity [dB/kPa] | 1.90 | 0.557 | 0.606 | 0.280 |
| R-square value | 0.979 | 0.998 | 0.997 | 0.997 | |
| Age Group | Average [years] | Number of Participants | Average of Swallowing Time [s] |
| 30’s | 34.4 | 5 | 0.48 |
| 40’s | 48.0 | 4 | 0.50 |
| 50’s | 55.7 | 3 | 0.63 |
| 60’s | 63.3 | 4 | 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maeda, M.; Kadokura, M.; Aoki, R.; Komatsu, N.; Kawakami, M.; Koyama, Y.; Watanabe, K.; Nishiyama, M. A Fiber-Optic Non-Invasive Swallowing Assessment Device Based on a Wearable Pressure Sensor. Sensors 2023, 23, 2355. https://doi.org/10.3390/s23042355
Maeda M, Kadokura M, Aoki R, Komatsu N, Kawakami M, Koyama Y, Watanabe K, Nishiyama M. A Fiber-Optic Non-Invasive Swallowing Assessment Device Based on a Wearable Pressure Sensor. Sensors. 2023; 23(4):2355. https://doi.org/10.3390/s23042355
Chicago/Turabian StyleMaeda, Masanori, Miyuki Kadokura, Ryoko Aoki, Noriko Komatsu, Masaru Kawakami, Yuya Koyama, Kazuhiro Watanabe, and Michiko Nishiyama. 2023. "A Fiber-Optic Non-Invasive Swallowing Assessment Device Based on a Wearable Pressure Sensor" Sensors 23, no. 4: 2355. https://doi.org/10.3390/s23042355