1. Introduction
Life expectancy has increased rapidly, due to improvements in sanitation, nutrition, and medicine. The highest life expectancy in the nineteenth century was lower than that today in all countries of the world, thanks to the sociosanitary advances during the past decades [
1]. Hospitals have led these improvements as the main health providers in national health systems (NHS). They are highly complex institutions, offering a wide variety of medical and surgical interventions. However, along with this demographic change, the cost of care continues to increase. In a situation of global economic unpredictability, many health systems are looking for long-term solutions that contribute to the sustainability, accessibility, and appropriateness of health services [
1]. In this sense, hospitals, as the main drivers of health care delivery, are required to consider how to optimize patient care.
One of the most extensive practices for increasing admission efficacy, moderating costs, and reducing the demand for beds is hospitalization at home (HaH) interventions. This type of intervention is already common in European hospitals [
2,
3,
4], and they have shown maturity and the generation of health value. HaH could meet the increased demand for healthcare services, while reducing the inconveniences of traditional hospitalization, such as nosocomial infections, pressure sores, lack of privacy, family burden, and the associated cost of hospital beds [
5]. Current HaH protocols are made up of a set of well-standardized actions that are tailored according to the patients’ health conditions and socio-economic profile and are provided around daily nurse home visits. These nurses have special training to decide on complementary treatment actions. In addition, physician home visits are scheduled during the admission period, to control the clinical evolution of the patient.
Although technology is increasingly present in all hospitals, due to the growing use, among others, of IoT devices [
6], HaH remains highly dependent on the availability of human resources for its effective adoption. In fact, the need for daily physical visits from highly qualified personnel to monitor, follow-up, and administer treatment to each patient limits the growth of HaH units. Smart technologies can provide pathways and associated services that could guarantee continuous care and safety for more patients with the same human resources [
7]. Although telemedicine and remote monitoring solutions based on sensors and other IoT devices are mature enough to be applied in real settings [
8], the acceptance of this technology in supporting the daily management of HaH units remains very low [
9]. On the contrary, effective technological adoption has allowed chronic disease management to benefit from outpatient procedures in one of the hospital services with the most extensive hospitalization events: remote monitoring technology and digital care solutions allowed these patients to receive regular health checks, health coaching, and general disease monitoring, and, in the long term, prevented acute care episodes [
10], reducing associated costs, supporting patient participation, and improving health outcomes [
11].
In addition, digital care solutions can complement the care of patients with HaH [
12]: remote automatic monitoring solutions could provide new data, and continuous monitoring could enable virtual visits while optimizing physical visits, as well as adding professional, technical, and medical support for family members and informal careers. All of this could contribute to reducing the heavy dependence on human resources in HaH units, provide additional operational resources, and potentially favor their expansion. However, there is still a need for evidence of the effective integration of digital technologies into the clinical workflow of HaH, which can support the sustainable and scalable adoption of this technology. Addressing the need for patients and clinicians to use smart technology during admission to HaH can bridge the current gap between participation in technology and clinical procedures. The challenge lies in the need to create trust and systems that ethically and effectively use new digital tools, and maintain the quality of service and patient satisfaction. Unlike with chronic diseases, patients are admitted for 3 to 10 days and require medical and technological expertise for a very short period of time in highly personalized, customized, and specific care routines, while care professionals need to have real-time access to specific monitoring data and alerts, which can prevent any possible risk to the patient. To this end, the transparent usage offered by IoT devices facilitates the skill acquisition of the patients. This study aimed to support the effective definition of new models and approaches that adapt the current ones through the use of available smart digital solutions, which can bring together various expectations and a willingness to ensure the satisfaction of the current and future needs of HaH units.
The study is part of a project called Better@Home [
11], which evaluates the acceptability of adopting a HaH monitoring and follow-up system supported by IoT devices. The objective of this study was to provide evidence on the acceptability and effectiveness of integrating wearable and IoT technologies to support the remote monitoring and follow-up of patients admitted to HaH units, as well as the acceptability of these solutions in care processes for healthcare professionals and patients. Finally, the study aimed to demonstrate the usefulness of IoT technologies in overcoming current HaH barriers resulting from a lack of human resources. The paper is structured as follows:
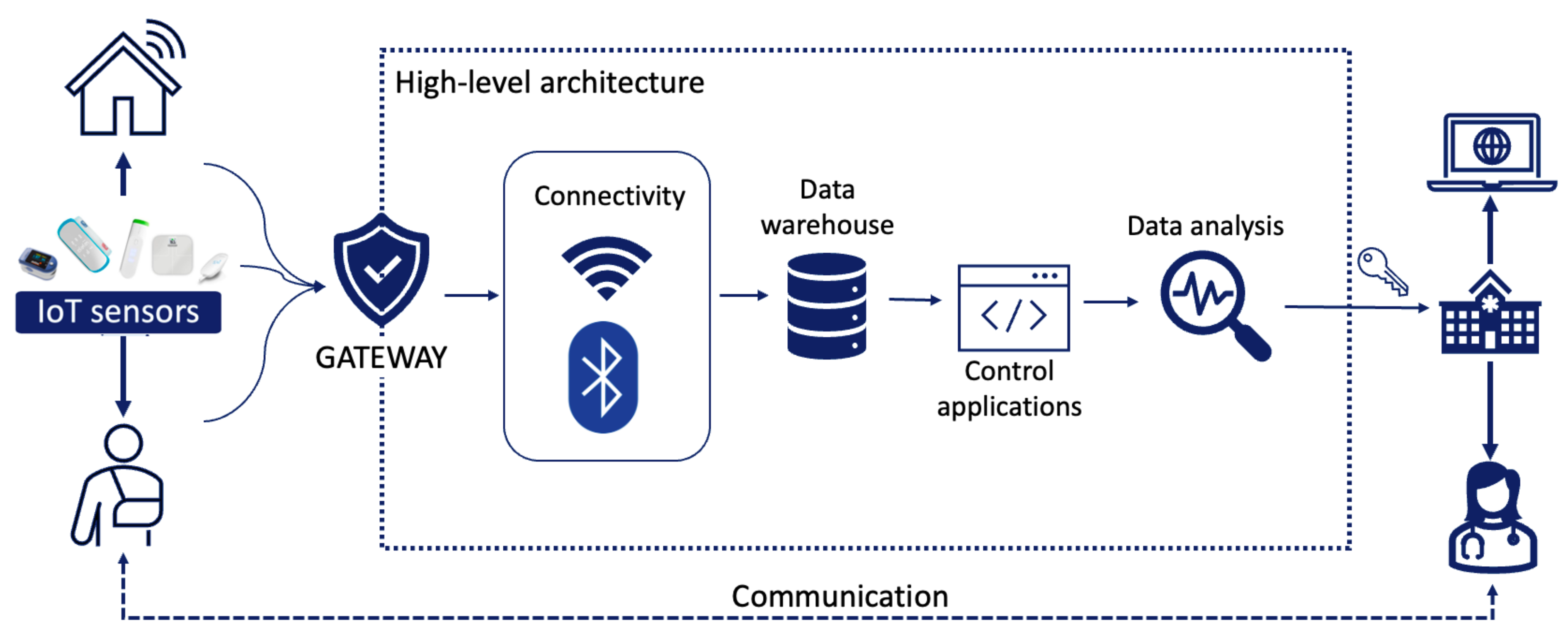
Section 2 describes the proposed technological system and its components, and the methods used to evaluate its feasibility, usability, and other relevant aspects for patient care and professional and patients’ acceptance.
Section 3 describes the evaluation results, while in
Section 4 and
Section 5, the obtained outcomes and their contribution to the objective of the study and conclusions are reported.
3. Results
From February 2021 to December 2021, a total of 208 patients participated in the study. The sociodemographic characteristics of each of the current samples in the group are shown in
Table 5 (patients) and
Table 6 (professionals). Most of the patients evaluated the HaH with infections (both urinary and tissues) and in the case of lung diseases, COVID-19 was one of the most frequent causes of admission (n = 57, 87.30%).
3.1. KPIs Results
The KPI outcomes obtained after evaluating the results in each patient showed a significant improvement in the hospitalization service compared to the traditional service. It is especially relevant in reducing face-to-face intervention, which has the potential to increase the number of beds without increasing the number of medical personnel. The reduction in readmissions was not so high, but this was significant because of the implications for the disease had for self-management, which reduces the number of exacerbations in short- and medium-term, see
Table 7.
3.2. Main Outcomes for Patients
Of the patients admitted to the emergency room as eligible for an HaH intervention, 90.4% accepted to participate in the program (approximately 60% of the total of patients admitted to the emergency room during the period with the same type of disease and admission cause). Of these, 75.96% completed the evaluation. In general, the HaH intervention was rated as positive in the four evaluated domains, with an agreement rate of more than 6, ranging from 5 to 7 per domain (
Table 8). The domain with the highest rating was the acquisition of health literacy from patients, and the lowest rated was the empowerment of patients.
In addition to these data, the mode of admission days changed from 11 days in traditional HaH to 6 days, implying a 54% reduction, while the mode of required professional visits changed from 3 to 1. During the study period, no adverse events were documented, and 18 patients (9.23%) required emergency assistance. No statistically significant differences were found between the responses to the questionnaire and the sex, age, or disease (p > 0.05) of the patients.
Finally, 98% of the patients considered that if they had to be readmitted, they would like to use digital HaH again, because they could integrate telemedicine and IoT devices into their lives without problems and felt confident, obtaining a high satisfaction rate from over 95% of the patients.
Thematic analysis of free-text comments led to the identification of the process and impact as the two main themes: identified barriers and improvement suggestions and the willingness to use this mode of hospitalization in the future. Most of the respondents reported very positive experiences, while few patients provided information on difficulties due to not being physically attended by a healthcare professional or barriers when using the digital solutions. The feedback was most encouraging about the benefits of being able to stay at home and being proactive with their daily care plans.
The percentage of patients who used each type of IoT device available is shown in
Table 9.
3.3. Main Results for Professionals
The results of the baseline and final evaluation of the professional intervention program performed are shown in
Table 10 for the MBI-HSS and CREAC questionnaires.
The analysis of professional comments suggested that the main barriers identified were related to the need to educate and inform all users. The technical strategies adopted with the inclusion of monitoring technologies were considered very positive and were not considered a barrier, rather a facilitator to improving their effectiveness.
4. Discussion
The presented study provides prerequisites for the adoption of a digital solution to support HaH units, offering the opportunity to evaluate how remote monitoring systems and telemedicine can influence the quality of life of patients admitted to a HaH service, but also their health empowerment and satisfaction at discharge, as well as providing initial evidence of their feasibility of implementation and integration into national health systems from a technical point of view. Furthermore, the study aimed to provide evidence on the impact of introducing these remote monitoring and support tools into a HaH unit workflow, which is key to the implementation of the final service [
24]. By using already mature technologies with proven effectiveness in reducing service costs and maintaining service quality [
25], there is the opportunity to extend the benefits of HaH, increasing the number of beds available in current units. Recent studies have shown the benefits of HaH, but also its barriers and future challenges [
12,
26]. Therefore, they are many points in common with other experiences and the remote collection of health records already evaluated using different methods and tools, and in different research areas.
The intervention involved more than 90.4% of hospital patients admitted to the emergency department. The number of adverse events was lower than the hospital average; only 9% of the patients needed urgent intervention, even considering that part of the study was carried out under the adverse conditions of the COVID-19 pandemic, with a great reduction of emergency services in the same period [
23,
24,
25]. This also highlights the feasibility and adaptability of the solution from a technical point of view, since it allowed for fast integration and management of the monitored patients in such a complicated situation. Four disease protocols, with up to 16 different pathways, were successfully implemented with the selected set of IoT devices, which demonstrate the computational efficiency of the proposed solution.
Although there were difficult conditions when deploying the system, the average number of hospitalization days was six, while in traditional HaH this was 11; the number of required visits was reduced from three to one on average [
27]. This is also good evidence of the usefulness of the proposed real-time transmission of data and alert management, generating a situation of trust and reliability regarding the proposed solution and the associated devices.
The influence of the pandemic on the results of professionals was also observed. They were also very positive, in general, but with signs of overwork and burnout due to stressful situations. This was also highlighted in other research studies aimed at assessing anxiety and burnout levels in emergency medical workers during the COVID-19 pandemic; however, our findings showed better results at the end of the evaluation, with lower burnout rates in the three domains [
28,
29]. However, some positive effects were observed at this point in the study. The proposed solution helped to create a secure environment, where professionals do not feel overwhelmed by the new processes and tools, even during the problematic situation they were facing, according to the improvements in the CREAC and MBI-HSS results [
30]. These results show professionals feel confident in the solution, which helps build trust with patients.
Both groups of participants were positive about the usefulness and effectiveness of the intervention. Taking into account the heterogeneity of the medical, social, educational, educational, and demographic conditions of the patients, the system demonstrated personalization, adaptability, and feasibility.
In the case of patients, the worst rated dimension was patient empowerment. Taking into account that this was the first time they were hospitalized at home with this technical support, we consider that the lower rates of self-perceived empowerment may have been due to the subjective need of depending on healthcare professionals [
31]. Further analysis should focus on analyzing the empowerment of patients who were previously hospitalized at home.
Our findings demonstrate that the integration of different methodological approaches from various research fields opens an opportunity to bridge the existing lack of evidence on the applicability of digital technologies. Interventions have been previously developed to promote digital education in home care and specifically in HaH [
32,
33]. Most of them did not target a wide spectrum of ages and socio-economic profiles, nor address the challenge of building the educational capacity of patients and professionals [
34,
35]. When the target group is homogeneous, the educational content is more specific and well-defined. Conversely, addressing different target groups entails difficulties in delivering and adapting the educational content and information [
31,
32,
34]. One of the challenges of developing this intervention was in allowing professionals and patients to learn how to use multiple devices and services in a few hours, without compromising patient safety and avoiding any type of risk. Based on studies published previously [
36,
37,
38], we obtained the background necessary to describe the problem, define the intervention, and plan data collection.
The evaluation results demonstrated high levels of satisfaction, both in patients and professionals. This is highly relevant in the case of patients, since their perceived service quality was reinforced by their trust in the solution, the easy communication with the professionals, and the comfort of being admitted in a familiar environment, as it was their own home.
There are some limitations to our study. A larger sample size would be necessary to improve the statistical power of the outcomes. Some of the results of the questions did not reach significance as a result of the sample size. In addition, some of the questionnaires used for the evaluation were related to subjective feelings and could result users to multiple interpretations, turning them into a source of bias. This risk is currently being reduced, as the questionnaire is in the validation process. Furthermore, this study focused on aspects of human–human interaction acceptance; more studies will be conducted in the future, in more hospital settings, on the reliability and stability of the proposed system. Future evaluations will help identify whether the intervention effectively contributes to improving patient-reported outcomes and reduces the workload and costs associated with health professionals, as well as supporting patients to improve their health outcomes and contributing to the efficient and effective adoption of digital HaH programs.

 ,
, 




{kind=link}
{kind=link}