
Dual-Task Interference Effects on Lower-Extremity Muscle Activities during Gait Initiation and Steady-State Gait among Healthy Young Individuals, Measured Using Wireless Electromyography Sensors

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
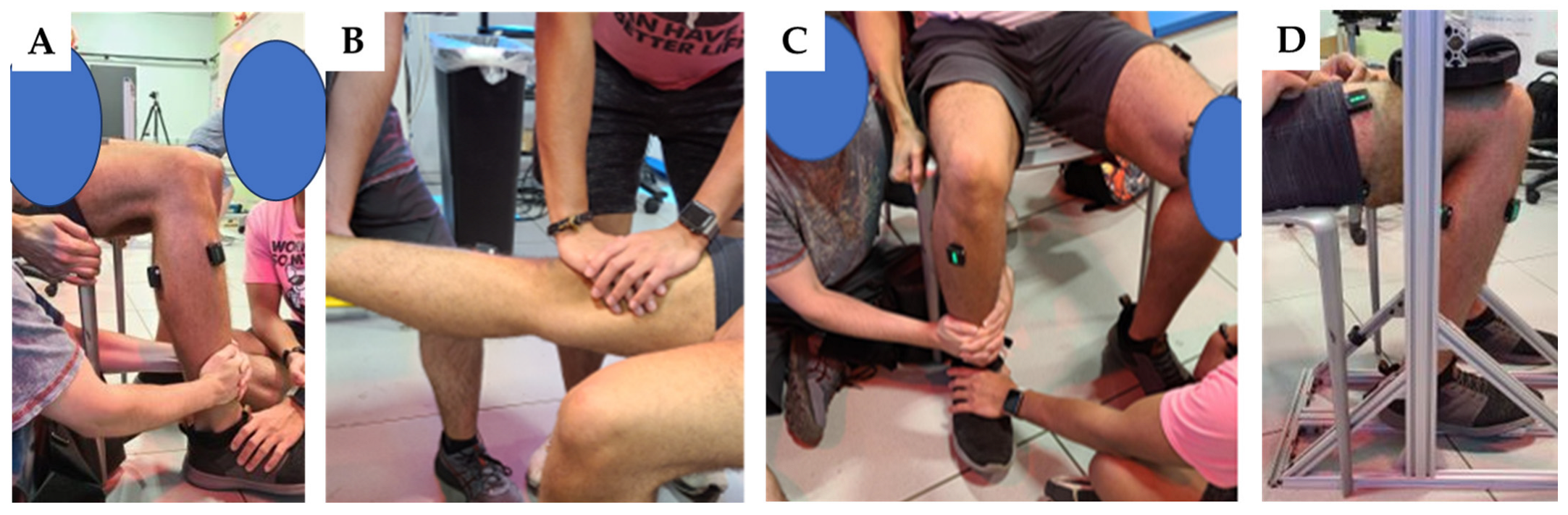
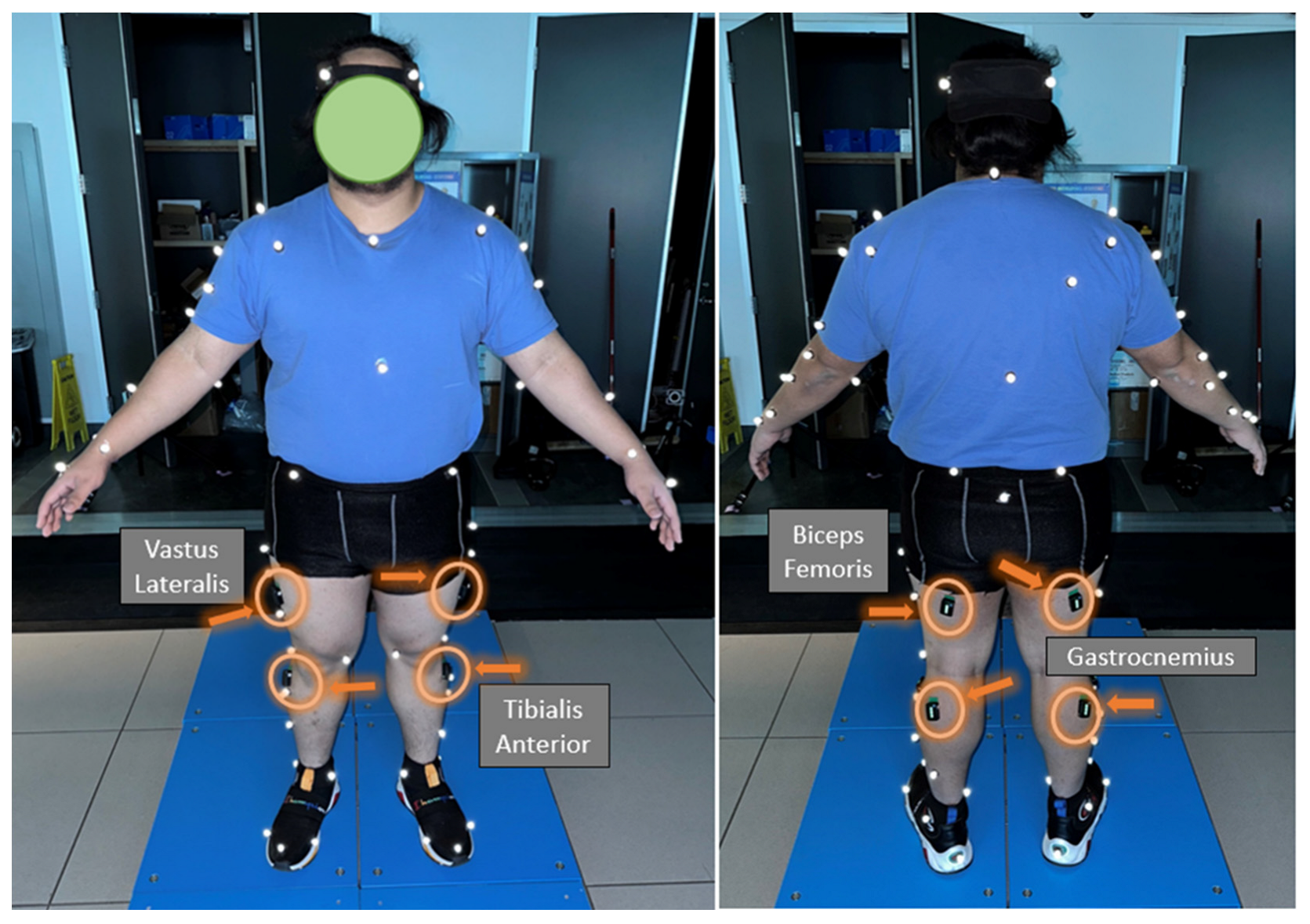
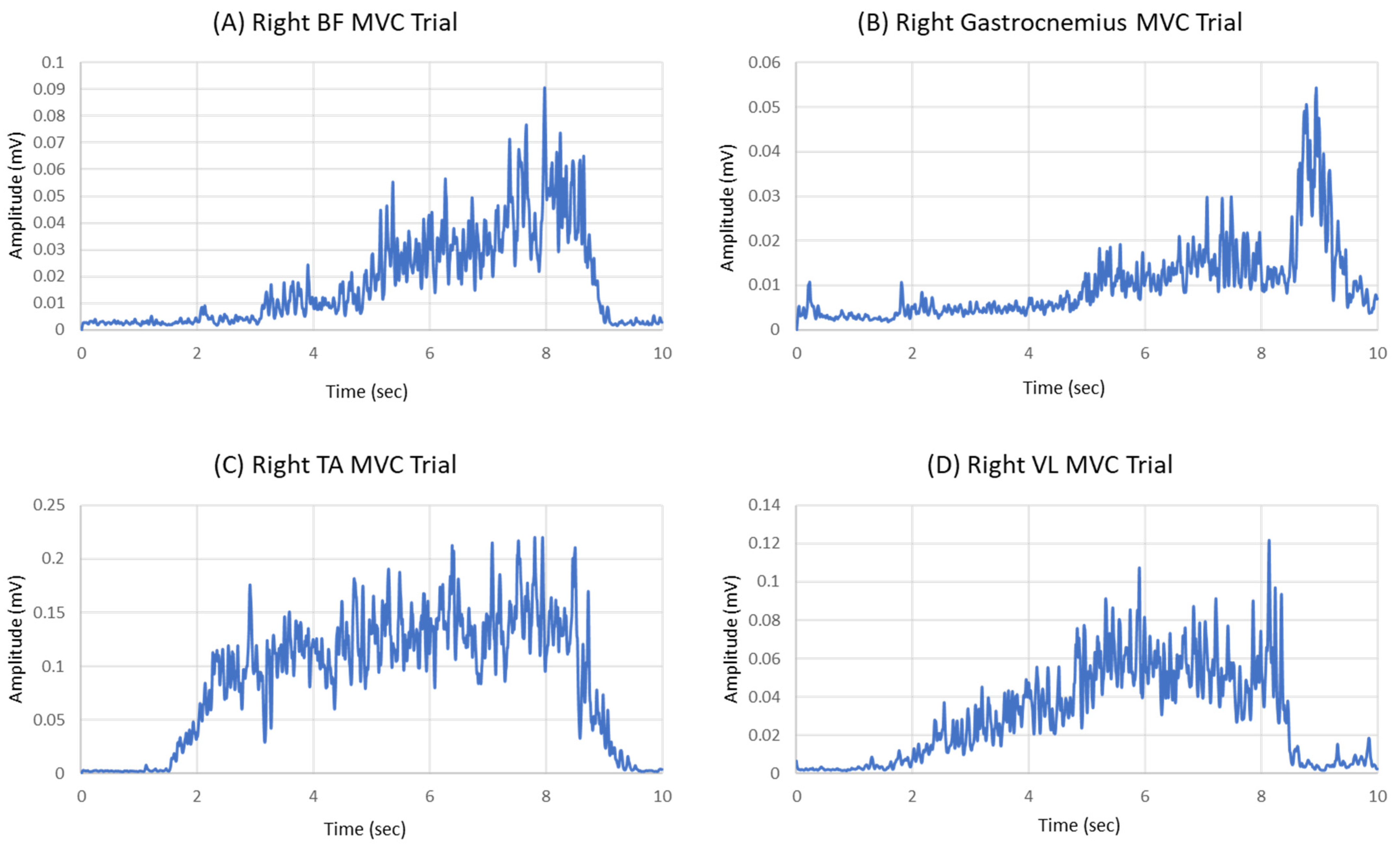
2.2. Experimental Protocol
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Participants
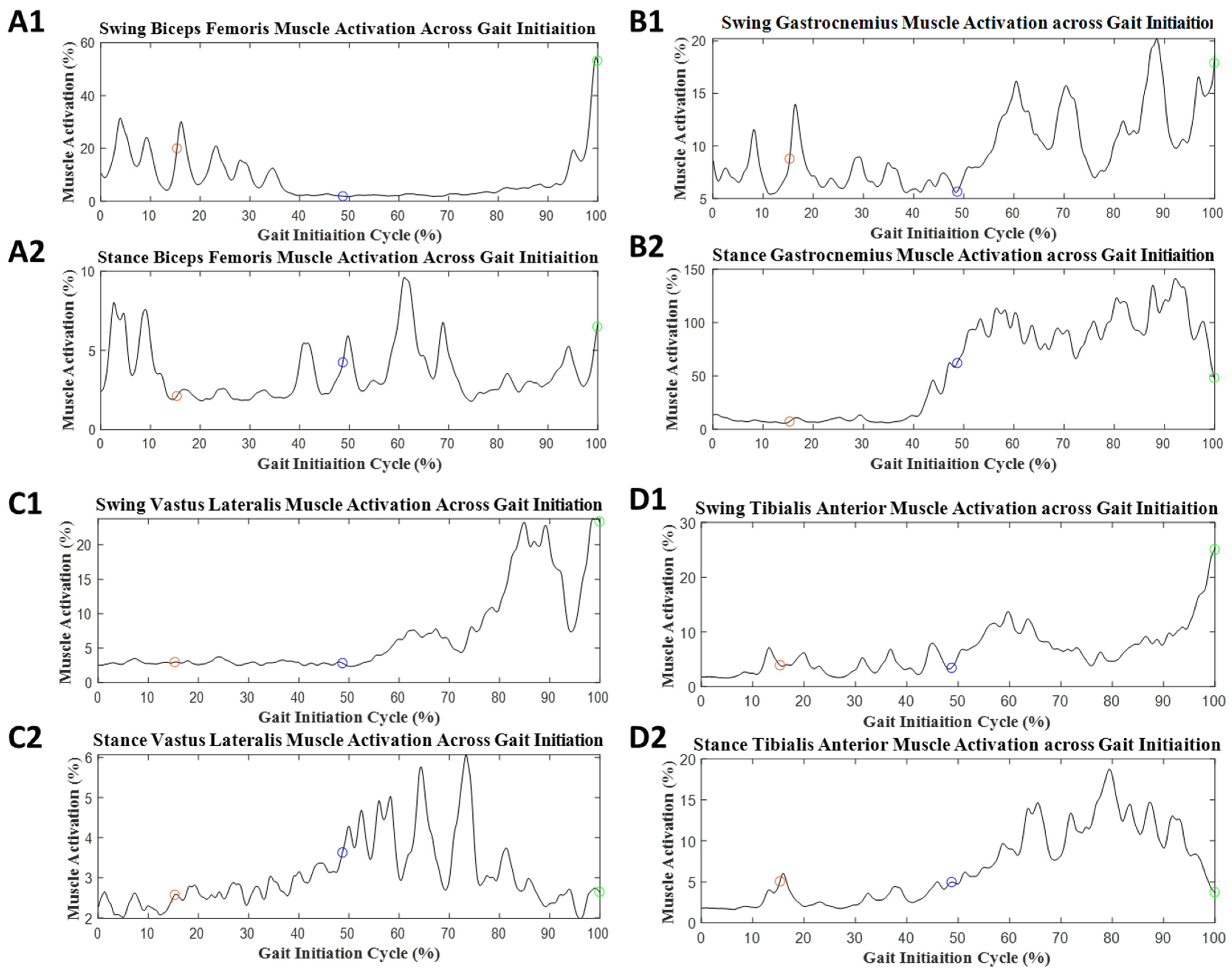
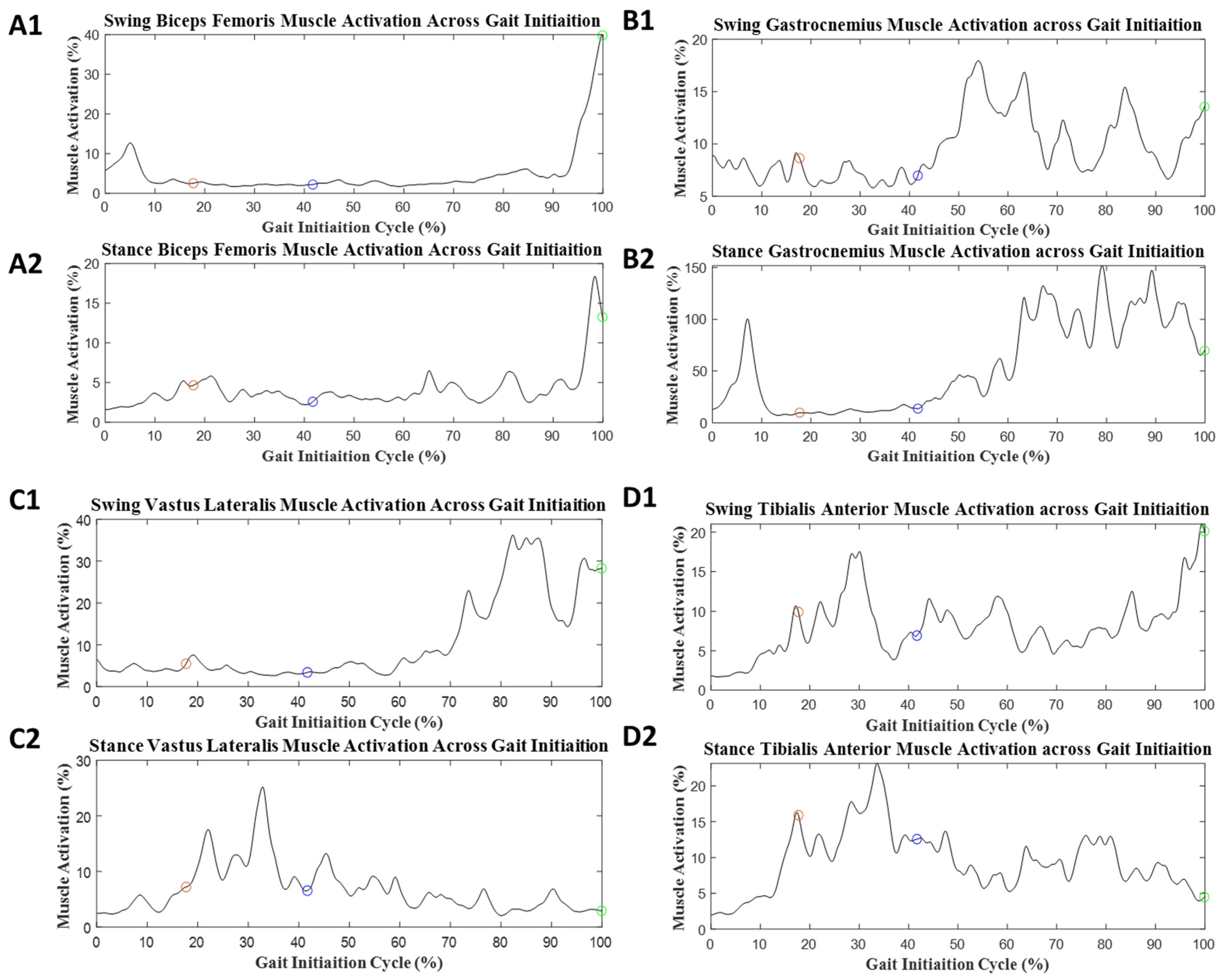
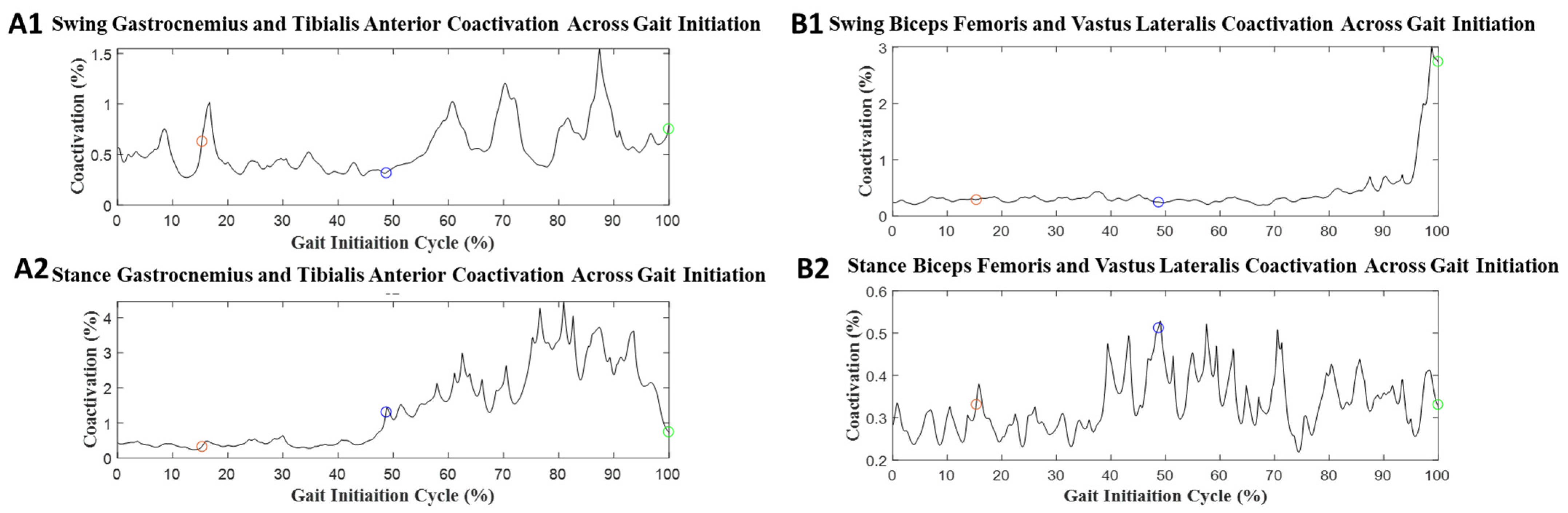
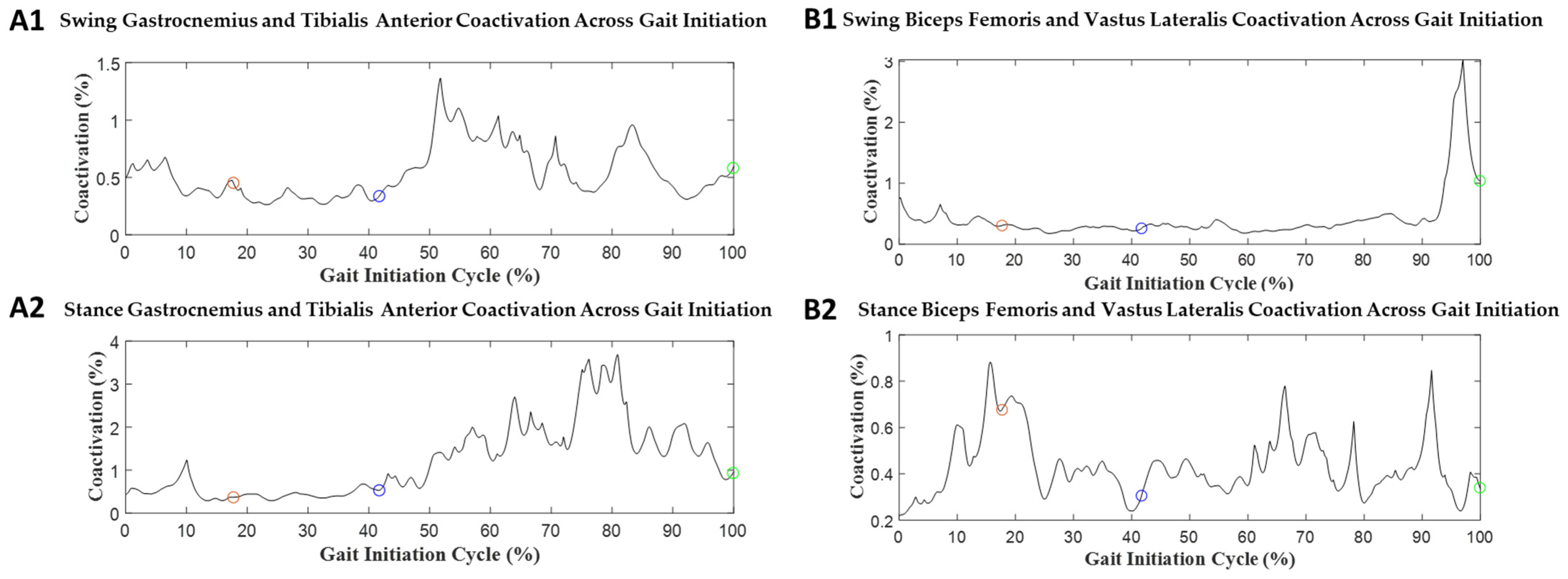
3.2. Gait Initiation
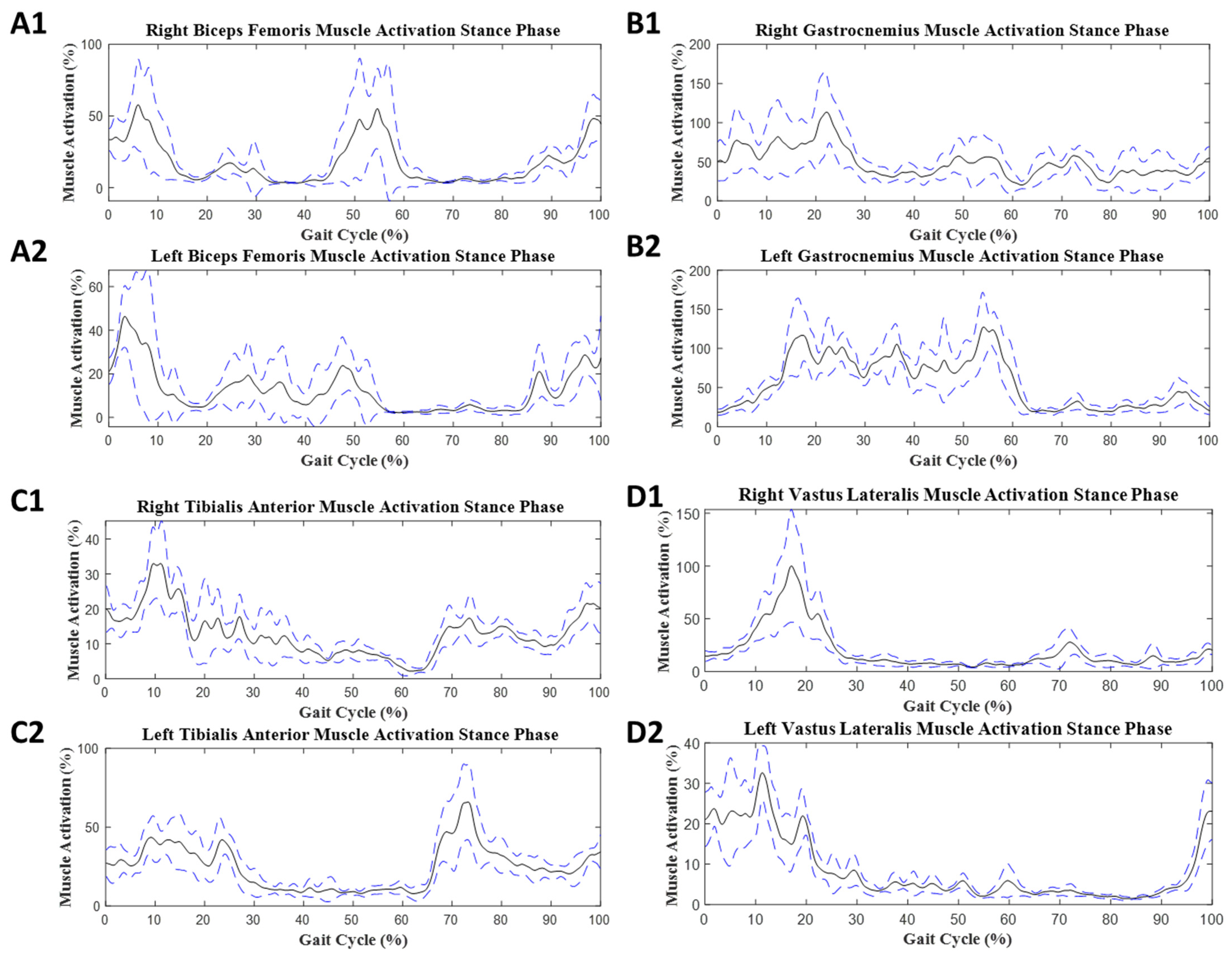
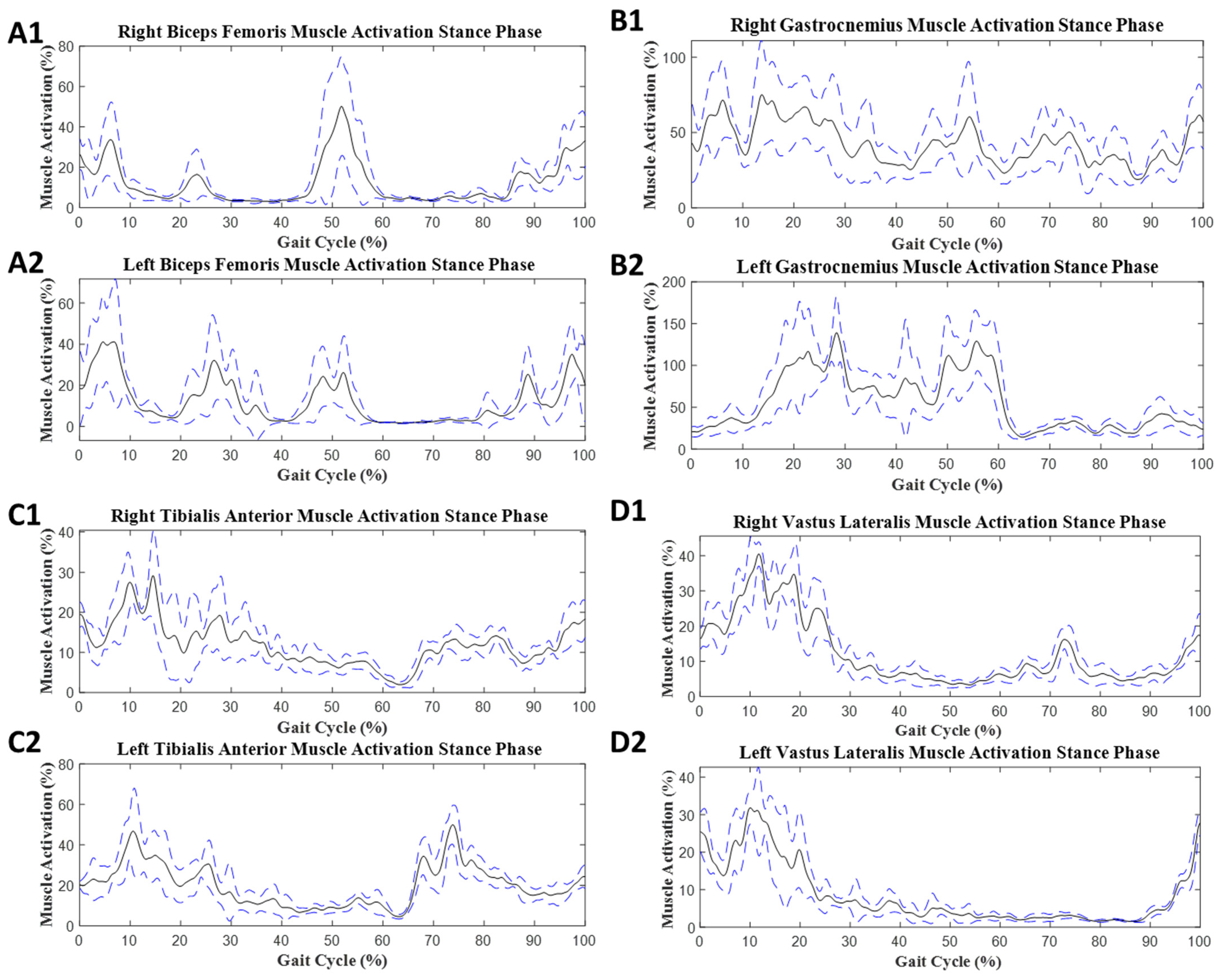
3.3. Steady-State Gait
4. Discussion
4.1. Gait Initiation Phases
4.2. Steady-State Gait
4.3. Potential Benefits and Implications
4.4. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. Off. J. Mov. Disord. Soc. 2008, 23, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Mc Ardle, R.; Del Din, S.; Donaghy, P.; Galna, B.; Thomas, A.J.; Rochester, L. The impact of environment on gait assessment: Considerations from real-world gait analysis in dementia subtypes. Sensors 2021, 21, 813. [Google Scholar] [CrossRef] [PubMed]
- Pitts, J.; Singhal, K.; Apte, Y.; Patel, P.; Kannan, L.; Bhatt, T. The Effect of Cognitive Task, Gait Speed, and Age on Cognitive–Motor Interference during Walking. Sensors 2023, 23, 7368. [Google Scholar] [CrossRef] [PubMed]
- Camp, N.; Vagnetti, R.; Bisele, M.; Felton, P.; Hunter, K.; Magistro, D. The Effect of Cognitive Task Complexity on Healthy Gait in the Walking Corsi Test. Brain Sci. 2023, 13, 1019. [Google Scholar] [CrossRef] [PubMed]
- Bayot, M.; Dujardin, K.; Tard, C.; Defebvre, L.; Bonnet, C.T.; Allart, E.; Delval, A. The interaction between cognition and motor control: A theoretical framework for dual-task interference effects on posture, gait initiation, gait and turning. Neurophysiol. Clin. 2018, 48, 361–375. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.E.; Zhou, H.; Varghese, V.; Najafi, B. Characteristics of the gait initiation phase in older adults with diabetic peripheral neuropathy compared to control older adults. Clin. Biomech. 2020, 72, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.E.; Yang, J.; Najafi, B. Does the presence of cognitive impairment exacerbate the risk of falls in people with peripheral neuropathy? An application of body-worn inertial sensors to measure gait variability. Sensors 2020, 20, 1328. [Google Scholar] [CrossRef] [PubMed]
- Muir-Hunter, S.; Wittwer, J. Dual-task testing to predict falls in community-dwelling older adults: A systematic review. Physiotherapy 2016, 102, 29–40. [Google Scholar] [CrossRef]
- Woollacott, M.; Shumway-Cook, A. Attention and the control of posture and gait: A review of an emerging area of research. Gait Posture 2002, 16, 1–14. [Google Scholar] [CrossRef]
- Parati, M.; Gallotta, M.; Muletti, M.; Pirola, A.; Bellafà, A.; De Maria, B.; Ferrante, S. Validation of pressure-sensing insoles in patients with Parkinson’s disease during overground walking in single and cognitive dual-task conditions. Sensors 2022, 22, 6392. [Google Scholar] [CrossRef]
- Prell, T.; Uhlig, M.; Derlien, S.; Maetzler, W.; Zipprich, H.M. Fear of falling does not influence dual-task gait costs in people with parkinson’s disease: A cross-sectional study. Sensors 2022, 22, 2029. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.; Cusack, T.; Blake, C. The effect of a dual task on gait speed in community dwelling older adults: A systematic review and meta-analysis. Gait Posture 2016, 44, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Plummer, P.; Apple, S.; Dowd, C.; Keith, E. Texting and walking: Effect of environmental setting and task prioritization on dual-task interference in healthy young adults. Gait Posture 2015, 41, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Kelly, V.E.; Eusterbrock, A.J.; Shumway-Cook, A. A review of dual-task walking deficits in people with Parkinson’s disease: Motor and cognitive contributions, mechanisms, and clinical implications. Park. Dis. 2012, 2012, 918719. [Google Scholar] [CrossRef]
- Piche, E.; Gerus, P.; Chorin, F.; Jaafar, A.; Guerin, O.; Zory, R. The effect of different dual tasks conditions on gait kinematics and spatio-temporal walking parameters in older adults. Gait Posture 2022, 95, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.-U.; Jerome, G.J.; Simonsick, E.M.; Studenski, S.; Hausdorff, J.M.; Ferrucci, L. Differential associations between dual-task walking abilities and usual gait patterns in healthy older adults—Results from the Baltimore Longitudinal Study of Aging. Gait Posture 2018, 63, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Hallal, C.Z.; Marques, N.R.; Spinoso, D.H.; Vieira, E.R.; Gonçalves, M. Electromyographic patterns of lower limb muscles during apprehensive gait in younger and older female adults. J. Electromyogr. Kinesiol. 2013, 23, 1145–1149. [Google Scholar] [CrossRef]
- Saraiva, M.; Castro, M.A.; Vilas-Boas, J.P. Influence of cognitive and motor tasks using smartphone during gait: EMG and gait performance analysis–Dual-task study. Hum. Mov. Sci. 2023, 89, 103097. [Google Scholar] [CrossRef]
- Yiou, E.; Caderby, T.; Delafontaine, A.; Fourcade, P.; Honeine, J.-L. Balance control during gait initiation: State-of-the-art and research perspectives. World J. Orthop. 2017, 8, 815. [Google Scholar] [CrossRef]
- Kang, G.E.; Gross, M.M. Emotional influences on sit-to-walk in healthy young adults. Hum. Mov. Sci. 2015, 40, 341–351. [Google Scholar] [CrossRef]
- Kang, G.E.; Gross, M.M. The effect of emotion on movement smoothness during gait in healthy young adults. J. Biomech. 2016, 49, 4022–4027. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.E.; Mickey, B.J.; Krembs, B.S.; McInnis, M.G.; Gross, M.M. The effect of mood phases on balance control in bipolar disorder. J. Biomech. 2019, 82, 266–270. [Google Scholar] [CrossRef]
- Albarqi, G.; Tavakoli, P. The effects of proficiency level and dual-task condition on L2 self-monitoring behavior. Stud. Second Lang. Acquis. 2023, 45, 212–233. [Google Scholar] [CrossRef]
- Kahya, M.; Liao, K.; Gustafson, K.M.; Akinwuntan, A.E.; Manor, B.; Devos, H. Cortical Correlates of Increased Postural Task Difficulty in Young Adults: A Combined Pupillometry and EEG Study. Sensors 2022, 22, 5594. [Google Scholar] [CrossRef] [PubMed]
- Monfrini, R.; Rossetto, G.; Scalona, E.; Galli, M.; Cimolin, V.; Lopomo, N.F. Technological Solutions for Human Movement Analysis in Obese Subjects: A Systematic Review. Sensors 2023, 23, 3175. [Google Scholar] [CrossRef] [PubMed]
- Cimolin, V.; Gobbi, M.; Buratto, C.; Ferraro, S.; Fumagalli, A.; Galli, M.; Capodaglio, P. A Comparative Analysis of Shoes Designed for Subjects with Obesity Using a Single Inertial Sensor: Preliminary Results. Sensors 2022, 22, 782. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Heintz, S.; Gutierrez-Farewik, E.M. Static optimization of muscle forces during gait in comparison to EMG-to-force processing approach. Gait Posture 2007, 26, 279–288. [Google Scholar] [CrossRef]
- Kang, G.E.; Mickey, B.J.; McInnis, M.G.; Krembs, B.S.; Gross, M.M. Motor behavior characteristics in various phases of bipolar disorder revealed through biomechanical analysis: Quantitative measures of activity and energy variables during gait and sit-to-walk. Psychiatry Res. 2018, 269, 93–101. [Google Scholar] [CrossRef]
- Tweel, E.; Stromberg, A.J.; Gera, G. Use of Wearable Sensors to Assess the Effects of Performing a Cognitive Task on Sensory Integration of Balance in Healthy Individuals. Sensors 2022, 22, 2776. [Google Scholar] [CrossRef] [PubMed]
- Carneros-Prado, D.; Dobrescu, C.C.; González, I.; Fontecha, J.; Johnson, E.; Hervás, R. Analysis of Dual-Tasking Effect on Gait Variability While Interacting with Mobile Devices. Mathematics 2022, 11, 202. [Google Scholar] [CrossRef]
- Kang, G.E.; Stout, A.; Waldon, K.V.; Kang, S.; Killeen, A.L.; Crisologo, P.A.; Siah, M.; Jupiter, D.; Najafi, B.; Vaziri, A.; et al. Digital Biomarkers of Gait and Balance in Diabetic Foot, Measurable by Wearable Inertial Measurement Units: A Mini Review. Sensors 2022, 22, 9278. [Google Scholar] [CrossRef] [PubMed]
- Pitts, J.; Kannan, L.; Bhatt, T. Cognitive Task Domain Influences Cognitive-Motor Interference during Large-Magnitude Treadmill Stance Perturbations. Sensors 2023, 23, 7746. [Google Scholar] [CrossRef] [PubMed]
- Zeni, J., Jr.; Richards, J.; Higginson, J. Two simple methods for determining gait events during treadmill and overground walking using kinematic data. Gait Posture 2008, 27, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Acuña, S.A.; Francis, C.A.; Franz, J.R.; Thelen, D.G. The effects of cognitive load and optical flow on antagonist leg muscle coactivation during walking for young and older adults. J. Electromyogr. Kinesiol. 2019, 44, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Di Nardo, F.; Morano, M.; Strazza, A.; Fioretti, S. Muscle Co-Contraction Detection in the Time–Frequency Domain. Sensors 2022, 22, 4886. [Google Scholar] [CrossRef] [PubMed]
- Bandini, V.; Carpinella, I.; Marzegan, A.; Jonsdottir, J.; Frigo, C.A.; Avanzino, L.; Pelosin, E.; Ferrarin, M.; Lencioni, T. Surface-Electromyography-Based Co-Contraction Index for Monitoring Upper Limb Improvements in Post-Stroke Rehabilitation: A Pilot Randomized Controlled Trial Secondary Analysis. Sensors 2023, 23, 7320. [Google Scholar] [CrossRef]
- Khanmohammadi, R.; Talebian, S.; Hadian, M.R.; Olyaei, G.; Bagheri, H. Characteristic muscle activity patterns during gait initiation in the healthy younger and older adults. Gait Posture 2016, 43, 148–153. [Google Scholar] [CrossRef]
- Souissi, H.; Zory, R.; Bredin, J.; Gerus, P. Comparison of methodologies to assess muscle co-contraction during gait. J. Biomech. 2017, 57, 141–145. [Google Scholar] [CrossRef]
- Kang, G.E.; Najafi, B. Sensor-based daily physical activity: Towards prediction of the level of concern about falling in peripheral neuropathy. Sensors 2020, 20, 505. [Google Scholar] [CrossRef]
- Mickelborough, J.; Van Der Linden, M.; Tallis, R.; Ennos, A. Muscle activity during gait initiation in normal elderly people. Gait Posture 2004, 19, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Hass, C.J.; Gregor, R.J.; Waddell, D.E.; Oliver, A.; Smith, D.W.; Fleming, R.P.; Wolf, S.L. The influence of Tai Chi training on the center of pressure trajectory during gait initiation in older adults. Arch. Phys. Med. Rehabil. 2004, 85, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
- Polcyn, A.F.; Lipsitz, L.A.; Kerrigan, D.C.; Collins, J.J. Age-related changes in the initiation of gait: Degradation of central mechanisms for momentum generation. Arch. Phys. Med. Rehabil. 1998, 79, 1582–1589. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, M.; Castro, M.A.; Vilas-Boas, J.P. Muscular and Prefrontal Cortex Activity during Dual-Task Performing in Young Adults. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Horata, E.T.; Kundakci, Y.E. Comparison of gait parameters under single-and dual-task conditions between children with specific learning disorder and typically developing children. Gait Posture 2022, 98, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Abbud, G.d.A.; Li, K.; DeMont, R. Attentional requirements of walking according to the gait phase and onset of auditory stimuli. Gait Posture 2009, 30, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Campanini, I.; Merlo, A.; Disselhorst-Klug, C.; Mesin, L.; Muceli, S.; Merletti, R. Fundamental concepts of bipolar and high-Density surface EMG understanding and teaching for clinical, occupational, and sport applications: Origin, detection, and main errors. Sensors 2022, 22, 4150. [Google Scholar] [CrossRef]
- Qassim, H.M.; Hasan, W.Z.W.; Ramli, H.R.; Harith, H.H.; Mat, L.N.I.; Ismail, L.I. Proposed fatigue index for the objective detection of muscle fatigue using surface electromyography and a double-step binary classifier. Sensors 2022, 22, 1900. [Google Scholar] [CrossRef]
- Ye-Lin, Y.; Prats-Boluda, G.; Galiano-Botella, M.; Roldan-Vasco, S.; Orozco-Duque, A.; Garcia-Casado, J. Directed functional coordination analysis of swallowing muscles in healthy and dysphagic subjects by surface electromyography. Sensors 2022, 22, 4513. [Google Scholar] [CrossRef]
- Park, J.-W.; Baek, S.-H.; Sung, J.H.; Kim, B.-J. Predictors of Step Length from Surface Electromyography and Body Impedance Analysis Parameters. Sensors 2022, 22, 5686. [Google Scholar] [CrossRef]
- Henriksson, M.; Hirschfeld, H. Physically active older adults display alterations in gait initiation. Gait Posture 2005, 21, 289–296. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurements | mean ± standard deviation |
| Subjects (n) | 21 |
| Males (n) | 14 |
| Age (years) | 21.9 ± 3.3 |
| Height (m) | 1.69 ± 0.06 |
| Weight (kg) | 71.26 ± 9.01 |
| BMI (kg/m²) | 24.4 ± 2.38 |
| MOCA (out of 30) | 28.09 ± 1.54 |
| Phase | Muscle | ST GI | DT GI | p-Value | Group Effect (d) |
|---|---|---|---|---|---|
| Onset | Swing BF | 5.87 ± 4.05 | 5.13 ± 2.23 | 0.795 | 0.07 |
| Stance BF | 5.66 ± 3.93 | 4.33 ± 2.53 | 0.071 | 0.50 | |
| Swing gastrocnemius | 7.05 ± 5.84 | 6.56 ± 4.26 | 0.983 | 0.01 | |
| Stance gastrocnemius | 11.80 ± 14.94 | 8.67 ± 8.63 | 0.345 | 0.26 | |
| Swing TA | 6.31 ± 6.60 | 5.23 ± 4.04 | 0.908 | 0.03 | |
| Stance TA | 5.03 ± 4.06 | 4.26 ± 2.41 | 0.566 | 0.15 | |
| Swing VL | 5.49 ± 4.38 | 6.98 ± 5.93 | 0.266 | 0.30 | |
| Stance VL | 7.27 ± 7.67 | 6.59 ± 4.62 | 0.877 | 0.04 | |
| Weight Transition | Swing BF | 6.04 ± 3.89 | 5.35 ± 2.76 | 0.362 | 0.24 |
| Stance BF | 5.83 ± 3.77 | 6.15 ± 3.54 | 0.364 | 0.24 | |
| Swing gastrocnemius | 7.92 ± 6.70 | 8.11 ± 6.76 | 0.813 | 0.06 | |
| Stance gastrocnemius | 20.98 ± 33.15 | 11.81 ± 11.48 | 0.088 | 0.49 | |
| Swing TA | 7.46 ± 5.83 | 6.99 ± 5.37 | 0.854 | 0.05 | |
| Stance TA | 13.17 ± 16.10 | 8.25 ± 5.00 | 0.173 | 0.37 | |
| Swing VL | 4.84 ± 3.05 | 6.86 ± 5.46 | 0.123 | 0.42 | |
| Stance VL | 10.98 ± 8.83 | 11.04 ± 8.40 | 0.874 | 0.04 | |
| Offset | Swing BF | 7.89 ± 5.10 | 6.70 ± 3.88 | 0.220 | 0.33 |
| Stance BF | 11.61 ± 13.32 | 10.32 ± 14.06 | 0.038 * | 0.59 | |
| Swing gastrocnemius | 12.51 ± 15.40 | 12.48 ± 15.44 | 0.885 | 0.04 | |
| Stance gastrocnemius | 47.55 ± 40.89 | 36.92 ± 29.90 | 0.074 | 0.52 | |
| Swing TA | 14.27 ± 6.93 | 14.12 ± 6.55 | 0.957 | 0.01 | |
| Stance TA | 23.94 ± 19.65 | 17.33 ± 17.33 | <0.001 * | 1.1 | |
| Swing VL | 7.86 ± 5.00 | 8.22 ± 5.76 | 0.792 | 0.07 | |
| Stance VL | 8.84 ± 6.81 | 8.35 ± 6.10 | 0.584 | 0.15 | |
| Full GI | Swing BF | 6.87 ± 3.90 | 6.01 ± 3.00 | 0.201 | 0.35 |
| Stance BF | 8.35 ± 6.35 | 7.77 ± 7.41 | 0.162 | 0.38 | |
| Swing gastrocnemius | 9.88 ± 9.25 | 7.28 ± 4.89 | 0.445 | 0.20 | |
| Stance gastrocnemius | 36.40 ± 46.47 | 27.21 ± 25.03 | 0.216 | 0.35 | |
| Swing TA | 10.48 ± 5.41 | 9.85 ± 4.16 | 0.809 | 0.06 | |
| Stance TA | 16.45 ± 13.47 | 12.73 ± 11.02 | 0.003 * | 0.91 | |
| Swing VL | 4.20 ± 1.30 | 5.36 ± 2.87 | 0.101 | 0.45 | |
| Stance VL | 6.34 ± 4.01 | 5.58 ± 3.49 | 0.163 | 0.38 |
| Phase | Muscle | ST GI | DT | p-Value | Group Effect (d) |
|---|---|---|---|---|---|
| Onset | Swing BF/VL | 0.33 ± 0.08 | 0.36 ± 0.14 | 0.852 | 0.22 |
| Stance BF/VL | 0.35 ± 0.10 | 0.34 ± 0.09 | 0.852 | 0.043 | |
| Swing gastrocnemius/TA | 0.44 ± 0.14 | 0.42 ± 0.11 | 0.625 | 0.13 | |
| Stance gastrocnemius/TA | 0.44 ± 0.16 | 0.38 ± 0.11 | 0.093 | 0.47 | |
| Weight Transition | Swing BF/VL | 0.34 ± 0.10 | 0.47 ± 0.15 | 0.140 | 0.73 |
| Stance BF/VL | 0.45 ± 0.18 | 0.33 ± 0.09 | 0.004 * | 0.88 | |
| Swing gastrocnemius/TA | 0.45 ± 0.14 | 0.45 ± 0.11 | 0.878 | 0.042 | |
| Stance gastrocnemius/TA | 0.62 ± 0.22 | 0.48 ± 0.14 | 0.043 * | 0.60 | |
| Offset | Swing BF/VL | 0.48 ± 0.15 | 0.44 ± 0.12 | 0.220 | 0.33 |
| Stance BF/VL | 0.46 ± 0.19 | 0.46 ± 0.18 | 0.852 | 0.049 | |
| Swing gastrocnemius/TA | 0.50 ± 0.15 | 0.59 ± 0.31 | 0.512 | 0.17 | |
| Stance gastrocnemius/TA | 1.78 ± 0.46 | 1.25 ± 0.47 | <0.001 * | 1.1 | |
| Full GI | Swing BF/VL | 0.41 ± 0.10 | 0.39 ± 0.10 | 0.645 | 0.12 |
| Stance BF/VL | 0.43 ± 0.14 | 0.44 ± 0.14 | 0.999 | 0.00 | |
| Swing gastrocnemius/TA | 0.47 ± 0.11 | 0.48 ± 0.15 | 0.963 | 0.01 | |
| Stance gastrocnemius/TA | 1.11 ± 0.27 | 0.90 ± 0.28 | 0.006 * | 0.84 |
| Muscle | ST Gait | DT Gait | p-Value | Group Effect (d) |
|---|---|---|---|---|
| Right BF | 17.21 ± 11.64 | 12.43 ± 7.79 | 0.003 * | 0.16 |
| Left BF | 13.94 ± 11.72 | 10.71 ± 9.83 | <0.001 * | 0.1 |
| Right gastrocnemius | 31.77 ± 17.99 | 28.91 ± 17.77 | 0.7 | 0.1 |
| Left gastrocnemius | 49.2 ± 58.79 | 45.31 ± 47.39 | 0.45 | 0.21 |
| Right TA | 44.43 ± 69.01 | 34.26 ± 50.81 | <0.001 * | 0.11 |
| Left TA | 30.06 ± 23.52 | 24.94 ± 18.72 | <0.001 * | 0.91 |
| Right VL | 15.34 ± 12.92 | 11.23 ± 9.66 | <0.001 * | 0.11 |
| Left VL | 12.87 ± 9.07 | 9.93 ± 6.59 | 0.001 * | 0.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waldon, K.T.; Stout, A.; Manning, K.; Gray, L.; Wilson, D.G.; Kang, G.E. Dual-Task Interference Effects on Lower-Extremity Muscle Activities during Gait Initiation and Steady-State Gait among Healthy Young Individuals, Measured Using Wireless Electromyography Sensors. Sensors 2023, 23, 8842. https://doi.org/10.3390/s23218842
Waldon KT, Stout A, Manning K, Gray L, Wilson DG, Kang GE. Dual-Task Interference Effects on Lower-Extremity Muscle Activities during Gait Initiation and Steady-State Gait among Healthy Young Individuals, Measured Using Wireless Electromyography Sensors. Sensors. 2023; 23(21):8842. https://doi.org/10.3390/s23218842
Chicago/Turabian StyleWaldon, Ke’Vaughn Tarrel, Angeloh Stout, Kaitlin Manning, Leslie Gray, David George Wilson, and Gu Eon Kang. 2023. "Dual-Task Interference Effects on Lower-Extremity Muscle Activities during Gait Initiation and Steady-State Gait among Healthy Young Individuals, Measured Using Wireless Electromyography Sensors" Sensors 23, no. 21: 8842. https://doi.org/10.3390/s23218842