

Automatic Detection of Cognitive Impairment with Virtual Reality

Abstract
:1. Introduction
2. Related Work
2.1. Pen and Paper Methods
2.2. VR Cognitive Assessments
2.3. Cognitive State Features
3. VR Study
3.1. VStore
3.2. Clinical Study
3.3. Procedure
4. Proposed Methodology
4.1. Feature Extraction
- VStore accounts for slow walkers as it is a VR simulation, one command to a controller is equivalent to one human stride. Hence pace of movement through this environment is better constrained to decision making as opposed to physical ability. This is one of the key advantages of VR cognitive assessments, they also enable large-scale spatial navigation to be assessed.
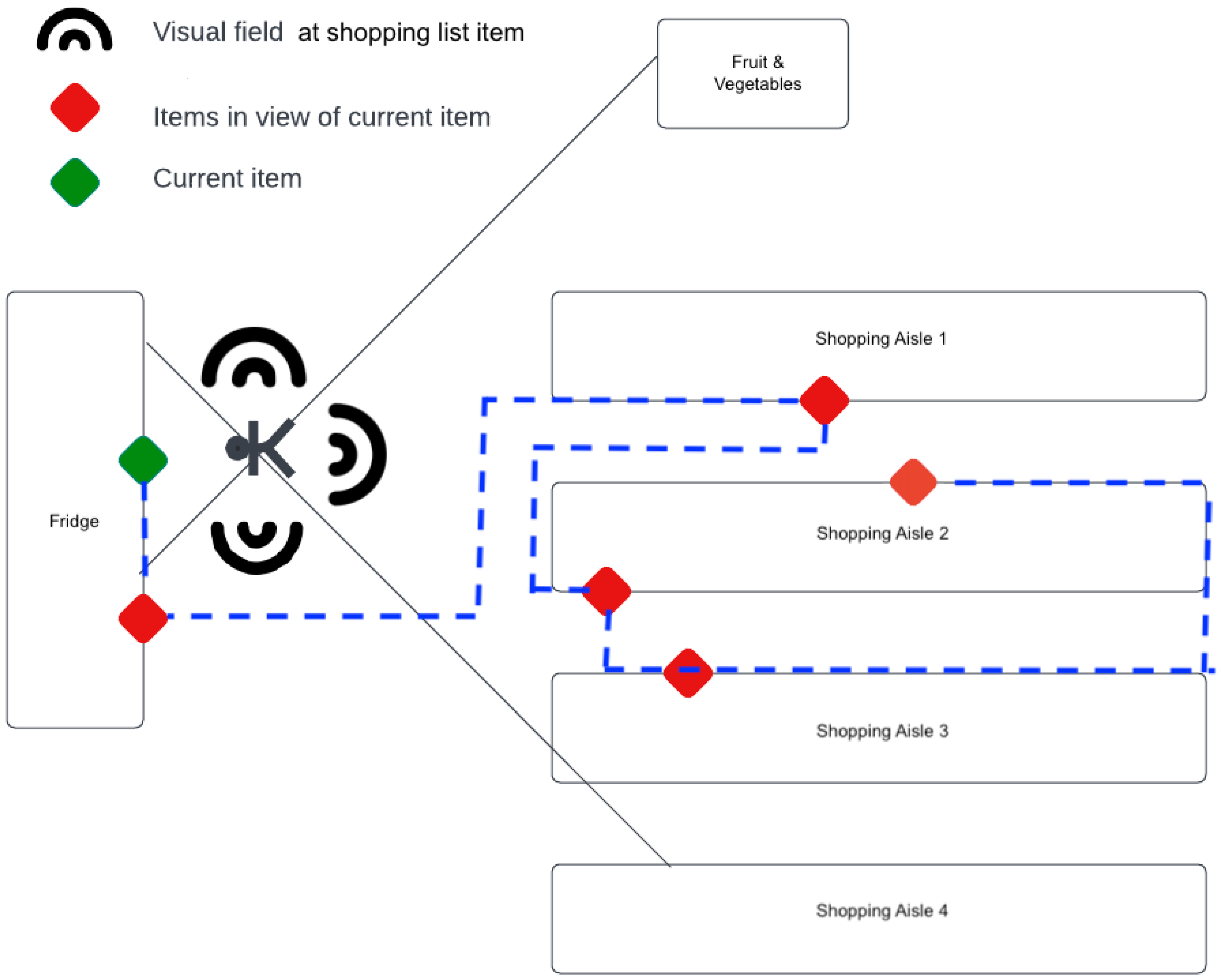
- The virtual supermarket shop floor consists of four shopping aisles with further shelving spanning the perimeter of the store. In some positions of the VR environment, participants can see what is on many other shelves of the aisles without having to walk down an aisle to find them. This is particularly significant at the fridges where participants can see six items on the list at once. This stage of the VR environment can be modelled on Traveling Salesman Problem (TSP). Any VR based cognitive assessment that requires decision making between simultaneously visible landmarks can also be modelled on TSP. The participant paths taken may provide insight on executive function, specifically, goal-directed motor function.
- Aisles are also labelled with the category of items they contain whether a participant can see the item or not, introducing bias to the aisles a participant explores. This is not simply an explore-exploit feedback system but one that invites strategic and optimal route planning, and cognition permitting. This observation can be translated to sophisticated VR cognitive assessments that compound behaviours in decisions made.
4.1.1. Spatial Features
Route Optimality Score
Proportional Distance Score
4.1.2. Execution Error Score
4.1.3. Hesitation Score
5. Cognitive Score Prediction
6. Experimental Results
6.1. Cognitive Scores
6.2. Participant Path
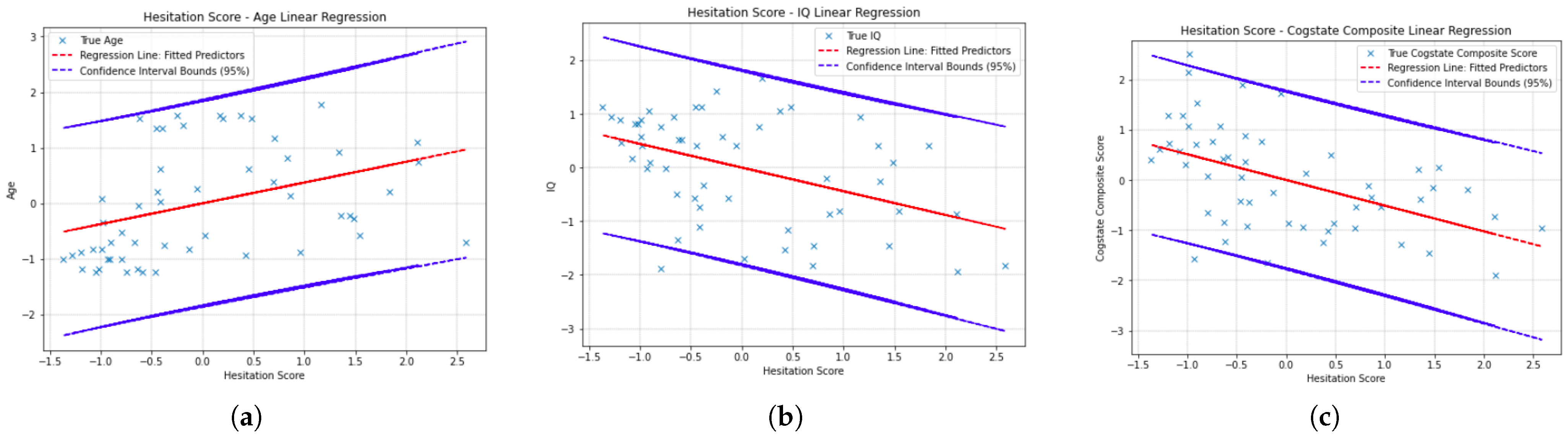
6.3. Hesitation Score Residual Plot
6.4. Data Tables
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Millan, M.; Agid, Y.; Brüne, M.; Bullmore, E.; Carter, C.; Clayto, N.; Connor, R.; Davis, S.; Deakin, B.; DeRubeis, R.; et al. Cognitive dysfunction in psychiatric disorders: Characteristics, causes and the quest for improved therapy. Nat. Rev. Drug Discov. 2012, 11, 141–168. [Google Scholar] [CrossRef] [PubMed]
- Vita, A.; Wolfgang, G.; Mucci, A.; Sachs, G.; Barlati, S.; Giordano, G.; Nibbio, G.; Nordentoft, M.; Wykes, T.; Galderisi, S. European Psychiatric Association guidance on treatment of cognitive impairment in schizophrenia. Eur. Psychiatry 2022, 65, e57. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Benito, J.; Guilera, G.; Pino, Ó.; Rojo, E.; Tabarés-Seisdedos, R.; Safont, G.; Martínez-Arán, A.; Franco, M.; Cuesta, M.J.; Crespo-Facorro, B.; et al. The screen for cognitive impairment in psychiatry: Diagnostic-specific standardization in psychiatric ill patients. BMC Psychiatry 2013, 13, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurford, I.; Marder, S.; Keefe, R.; Reise, S.; Bilder, R. A brief cognitive assessment tool for schizophrenia: Construction of a tool for clinicians. Schizophr. Bull. 2011, 37, 538–545. [Google Scholar] [CrossRef] [Green Version]
- Green, M.; Nuechterlein, K. The MATRICS initiative: Developing a consensus cognitive battery for clinical trials. Schizophr. Res. 2004, 72, 1–3. [Google Scholar] [CrossRef]
- Randolph, C.; Tierney, M.; Mohr, E.; Chase, T. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary clinical validity. J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef]
- Miskowiak, K.; Jespersen, A.; Kessing, L.; Aggestrup, A.; Glenthøj, L.; Nordentoft, M.; Ott, C.; Lumbye, A. Cognition Assessment in Virtual Reality: Validity and feasibility of a novel virtual reality test for real-life cognitive functions in mood disorders and psychosis spectrum disorders. J. Psychiatr. Res. 2022, 145, 182–189. [Google Scholar] [CrossRef]
- Ouellet, E.; Boller, B.; Corriveau-Lecavalier, N.; Cloutier, S.; Belleville, S. The Virtual Shop: A new immersive virtual reality environment and scenario for the assessment of everyday memory. J. Neurosci. Methods 2018, 303, 126–135. [Google Scholar] [CrossRef]
- Howett, D.; Castegnaro, A.; Krzywicka, K.; Hagman, J.; Marchment, D.; Henson, R.; Rio, M.; King, J.; Burgess, N.; Chan, D. Differentiation of mild cognitive impairment using an entorhinal cortex-based test of virtual reality navigation. Brain 2019, 142, 1751–1766. [Google Scholar] [CrossRef] [Green Version]
- Porffy, L.; Mehta, M.; Patchitt, J.; Boussebaa, C.; Brett, J.; D’Oliveira, T.; Mouchlianitis, E.; Shergill, S. A Novel Virtual Reality Assessment of Functional Cognition: Validation Study. J. Med. Internet Res. 2022, 24, e27641. [Google Scholar] [CrossRef]
- Maj, M.; Os, J.; Hert, M.D.; Gaebel, W.; Galderisi, S.; Green, M.; Guloksu, S.; Harvey, P.; Jones, P.; Malaspina, D.; et al. The clinical characterization of the patient with primary psychosis aimed at personalization of management. World Psychiatry 2021, 20, 4–33. [Google Scholar] [CrossRef] [PubMed]
- Education, O.M. Mini-Mental-State Examination. 2013. Available online: https://oxfordmedicaleducation.com/geriatrics/mini-mental-state-examination-mmse/ (accessed on 23 November 2022).
- Crum, R.; Anthony, J.; Bassett, S.; Folstein, M. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA 1993, 269, 2386–2391. [Google Scholar] [CrossRef]
- Cortes, C.; Vapnik, V. Support-vector networks. Mach. Learn. 1995, 20, 917–925. [Google Scholar] [CrossRef]
- Freitas, S.; Simões, M.; Alves, L.; Santana, I. MoCA: Normative study for the Portuguese population. J. Exp. Clin. Neuropsychol. 2011, 33, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Schulman, K. Clock Drawing Test. 1986. Available online: https://www.cgakit.com/m-1-clock-test (accessed on 23 November 2022).
- Freund, B.; Gravenstein, S.; Ferris, R.; Burke, B.; Shaheen, E. Drawing Clocks and Driving Cars. J. Gen. Intern. Med. 2005, 20, 240–244. [Google Scholar] [CrossRef] [Green Version]
- Baek, M.; Kim, H.; Ryu, H.; Lee, S.; Han, S.; Na, H.; Chang, Y.; Chey, J.; Kim, S. The usefulness of the story recall test in patients with mild cognitive impairment and AD. Aging Neuropsychol. Cogn. 2011, 18, 214–229. [Google Scholar] [CrossRef]
- Tuena, C.; Mancuso, V.; Stramba-Badiale, C.; Pedroli, E.; Stramba-Badiale, M.; Riva, G.; Repetto, C. Egocentric and Allocentric Spatial Memory in Mild Cognitive Impairment withReal-World and Virtual Navigation Tasks: A Systematic Review. J. Alzheimer’s Dis. 2021, 79, 95–116. [Google Scholar] [CrossRef]
- Plancher, G.; Tirard, A.; Gyselinck, V.; Nicolas, S.; Piolino, P. Using virtual reality to characterize episodic memory profiles in amnestic mild cognitive impairment and Alzheimer’s disease: Influence of active and passive encoding. Neuropsychologia 2012, 50, 592–602. [Google Scholar] [CrossRef]
- Alzheimer’s-Association. Alzheimer’s Disease facts and figures. Alzheimer’s Dement 2019, 15, 321–387. [Google Scholar]
- Horan, B.; Heckenberg, R.; Maruff, P.; Wright, B. Development of a new virtual reality test of cognition: assessing the test-retest reliability, convergent and ecological validity of CONVIRT. BMC Psychol. 2020, 8, 61. [Google Scholar] [CrossRef]
- Santos, N.; Costa, P.; Cunha, P.; Cotter, J.; Sampaio, A.; Zihl, J.; Almeida, O.; Cerqueira, J.; Palha, J.; Sousa, N. Mood is a key determinant of cognitive performance in community-dwelling older adults: a cross-sectional analysis. Off. J. Am. Aging Assoc. 2013, 35, 1983–1993. [Google Scholar] [CrossRef] [PubMed]
- Bolandzadeh, N.; Kordin, K.; Salowitz, N.; Davis, J.; Hsu, L.; Chan, A.; Sharma, D.; Blohm, G.; Liu-Ambrose, T. Predicting Cognitive Function from Clinical Measures of Physical Function and Health Status in Older Adults. PLoS ONE 2015, 10, e0119075. [Google Scholar] [CrossRef] [PubMed]
- Dansson, H.; Stempfle, L.; Egilsdóttir, H.; Schliep, A.; Portelius, E.; Blennow, K.; Zetterberg, H.; Johansson, F. Predicting progression and cognitive decline in amyloid-positive patients with Alzheimer’s disease. Alzheimer’s Res. Ther. 2021, 13, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Vitae VR Homepage. Vitae VR. Available online: https://www.vitaevr.com (accessed on 23 November 2022).
- Porffy, L.; Mehta, M.; Mouchlianitis, E.; Shergill, S. VStore: Feasibility and acceptability of a novel virtual reality functional cognition task. Frontiers 2022, 3, 875197. [Google Scholar] [CrossRef]
- Gates, T.; Kamminga, J.; Jayewardene, A.; Vincent, T.; Quan, D.; Brew, B.; Bloch, M.; Cysique, L. An examination of reliable change methods for measuring cognitive change with the Cogstate Computerized Battery: Research and clinical implications. Arch. Clin. Neuropsychol. 2021, 36, 597–612. [Google Scholar] [CrossRef]
- Guo, J.; Wei, A. NP-Completeness. 2022. Available online: https://math.mit.edu/research/highschool/primes/circle/documents/2022/Jessica%20&%20Audrey.pdf (accessed on 23 November 2022).
- Bouman, P.; Agatz, N.; Schmidt, M. Dynamic programming approaches for the traveling salesman problem with drone. Networks 2018, 72, 528–542. [Google Scholar] [CrossRef] [Green Version]
- Badal, V.; Depp, C.; Hitchcock, P.; Penn, D.; Harvey, P.; Pinkham, A. Computational methods for integrative evaluation of confidence, accuracy, and reaction time in facial affect recognition in schizophrenia. Schizophr. Res. Cogn. 2021, 25, 100196. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | F-stat | p (F-stat) | |
|---|---|---|---|
| Age | 0.380 | 14.270 | |
| IQ | 0.057 | 1.399 | 0.240 |
| Cog Comp | 0.224 | 6.713 | |
| DET | 0.071 | 1.775 | 0.140 |
| OCL | 0.044 | 1.075 | 0.374 |
| ONB | 0.070 | 1.752 | 0.145 |
| IDN | 0.050 | 1.256 | 0.293 |
| Feature | F-stat | p (F-stat) | |
|---|---|---|---|
| Age | 0.173 | 2.561 | 0.05 |
| IQ | 0.252 | 4.1118 | 0.00591 |
| Cog Comp | 0.328 | 5.986 | 0.000528 |
| DET | 0.369 | 7.158 | 0.000128 |
| OCL | 0.364 | 6.997 | 0.000154 |
| ONB | 0.359 | 6.872 | 0.000179 |
| IDN | 0.364 | 7.009 | 0.000152 |
| Cognitive Score | Feature | Coef | Std Error | t | |||
|---|---|---|---|---|---|---|---|
| Age | |||||||
| Cst. | 0.0055 | 0.082 | 0.067 | 0.947 | −0.210 | 0.221 | |
| PD | −0.2079 | 0.097 | −2.154 | 0.034 | −0.462 | 0.046 | |
| RO | −0.0758 | 0.086 | −0.882 | 0.38 | −0.302 | 0.150 | |
| ExErr | 0.2283 | 0.093 | 2.456 | 0.016 | −0.016 | 0.473 | |
| Hes | 0.6878 | 0.095 | 7.260 | 0.000 | 0.439 | 0.937 | |
| IQ | |||||||
| Cst. | 0.0178 | 0.100 | 0.179 | 0.858 | −0.244 | 0.280 | |
| PD | 0.0182 | 0.117 | 0.155 | 0.877 | −0.290 | 0.326 | |
| RO | 0.0326 | 0.104 | 0.312 | 0.756 | −0.242 | 0.307 | |
| ExErr | −0.0489 | 0.113 | −0.433 | 0.666 | −0.346 | 0.248 | |
| Hes | 0.2175 | 0.115 | 1.891 | 0.062 | −0.085 | 0.520 | |
| Cog Comp | |||||||
| Cst. | −0.0087 | 0.092 | −0.095 | 0.925 | −0.250 | 0.233 | |
| PD | 0.1214 | 0.108 | 1.125 | 0.264 | −0.163 | 0.405 | |
| RO | 0.1457 | 0.096 | 1.515 | 0.133 | −0.107 | 0.339 | |
| ExErr | −0.1960 | 0.104 | −1.884 | 0.063 | −0.470 | 0.078 | |
| Hes | −0.4994 | 0.106 | −4.710 | 0.000 | −0.778 | −0.221 | |
| DET | |||||||
| Cst. | −0.0051 | 0.100 | −0.051 | 0.959 | −0.269 | 0.259 | |
| PD | 0.1101 | 0.118 | 0.933 | 0.353 | −0.200 | −0.421 | |
| RO | 0.0717 | 0.105 | 0.682 | 0.497 | −0.205 | 0.348 | |
| ExErr | 0.0028 | 0.114 | 0.024 | 0.981 | −0.296 | 0.302 | |
| Hes | −0.2828 | 0.116 | −2.439 | 0.017 | −0.588 | −0.022 | |
| OCL | |||||||
| Cst. | −0.0053 | 0.102 | −0.052 | 0.958 | −0.273 | 0.262 | |
| PD | −0.0158 | 0.120 | −0.132 | 0.895 | −0.331 | 0.299 | |
| RO | 0.0815 | 0.107 | 0.765 | 0.446 | −0.199 | 0.362 | |
| ExErr | 0.0616 | 0.115 | 0.534 | 0.595 | −0.242 | 0.365 | |
| Hes | −0.1599 | 0.118 | −1.361 | 0.177 | −0.469 | 0.149 | |
| ONB | |||||||
| Cst. | 0.0002 | 0.101 | 0.002 | 0.998 | −0.264 | 0.265 | |
| PD | −0.0694 | 0.118 | −0.587 | 0.558 | −0.380 | 0.241 | |
| RO | 0.0877 | 0.105 | 0.833 | 0.407 | −0.189 | 0.364 | |
| ExErr | −0.0229 | 0.114 | −0.201 | 0.841 | −0.322 | 0.277 | |
| Hes | −0.2101 | 0.116 | −1.811 | 0.073 | −0.515 | 0.095 | |
| IDN | |||||||
| Cst. | 0.0043 | 0.102 | 0.042 | 0.966 | −0.263 | 0.271 | |
| PD | −0.2123 | 0.119 | −1.778 | 0.079 | −0.526 | 0.102 | |
| RO | −0.0981 | 0.106 | −0.922 | 0.359 | −0.378 | 0.182 | |
| ExErr | 0.1759 | 0.115 | 1.529 | 0.130 | −0.127 | 0.478 | |
| Hes | 0.0441 | 0.117 | 0.376 | 0.708 | −0.264 | 0.352 |
| Cognitive Score | Feature | Coef | Std Error | t | |||
|---|---|---|---|---|---|---|---|
| Age | |||||||
| Cst. | −0.0302 | 0.128 | −0.237 | 0.814 | −0.372 | 0.312 | |
| PD | 0.0975 | 0.134 | 0.727 | 0.471 | −0.262 | 0.457 | |
| RO | −0.1477 | 0.133 | −1.111 | 0.272 | −0.504 | 0.209 | |
| ExErr | −0.0108 | 0.130 | −0.083 | 0.934 | −0.358 | 0.337 | |
| Hes | 0.3869 | 0.129 | 3.000 | 0.004 | 0.041 | 0.733 | |
| IQ | |||||||
| Cst. | −0.0249 | 0.123 | −0.203 | 0.840 | −0.354 | 0.304 | |
| PD | 0.0553 | 0.129 | 0.428 | 0.670 | −0.291 | 0.304 | |
| RO | −0.1328 | 0.128 | −1.038 | 0.304 | −0.476 | 0.210 | |
| ExErr | −0.1719 | 0.125 | −1.377 | 0.175 | −0.506 | 0.163 | |
| Hes | −0.4051 | 0.124 | −3.263 | 0.002 | −0.738 | −0.072 | |
| Cog Comp | |||||||
| Cst. | −0.0011 | 0.118 | −0.009 | 0.993 | −0.318 | 0.316 | |
| PD | −0.1767 | 0.124 | −1.423 | 0.161 | −0.509 | 0.156 | |
| RO | 0.1673 | 0.123 | −1.359 | 0.180 | −0.163 | 0.497 | |
| ExErr | −0.1785 | 0.120 | −1.487 | 0.144 | −0.500 | 0.143 | |
| Hes | −0.4937 | 0.119 | −4.135 | 0.000 | −0.814 | −0.174 | |
| DET | |||||||
| Cst. | −0.0130 | 0.114 | −0.114 | 0.910 | −0.318 | 0.292 | |
| PD | 0.1073 | 0.120 | 0.896 | 0.375 | −0.214 | −0.428 | |
| RO | −0.1295 | 0.119 | −1.092 | 0.280 | −0.448 | 0.188 | |
| ExErr | −0.1019 | 0.116 | −0.880 | 0.383 | −0.412 | 0.208 | |
| Hes | −0.5543 | 0.115 | −4.815 | 0.000 | −0.863 | −0.246 | |
| OCL | |||||||
| Cst. | −0.0159 | 0.114 | −0.139 | 0.890 | −0.322 | 0.290 | |
| PD | 0.1104 | 0.120 | 0.921 | 0.362 | −0.211 | 0.432 | |
| RO | −0.1513 | 0.119 | −1.273 | 0.209 | −0.470 | 0.167 | |
| ExErr | −0.1219 | 0.116 | −1.051 | 0.298 | −0.433 | 0.189 | |
| Hes | −0.5335 | 0.115 | −4.626 | 0.000 | −0.843 | −0.224 | |
| ONB | |||||||
| Cst. | −0.0142 | 0.115 | −0.124 | 0.902 | −0.321 | 0.293 | |
| PD | 0.1389 | 0.120 | 1.153 | 0.254 | −0.184 | 0.426 | |
| RO | −0.1284 | 0.119 | −1.075 | 0.287 | −0.448 | 0.192 | |
| ExErr | −0.1131 | 0.116 | −0.971 | 0.336 | −0.424 | 0.199 | |
| Hes | −0.5399 | 0.116 | −4.662 | 0.000 | −0.850 | −0.230 | |
| IDN | |||||||
| Cst. | −0.0137 | 0.114 | −0.120 | 0.905 | −0.320 | 0.292 | |
| PD | 0.1235 | 0.120 | 1.028 | 0.309 | −0.198 | 0.445 | |
| RO | −0.1351 | 0.119 | −1.135 | 0.262 | −0.454 | 0.184 | |
| ExErr | −0.1088 | 0.116 | −0.937 | 0.353 | −0.420 | 0.202 | |
| Hes | −0.5447 | 0.115 | −4.718 | 0.000 | −0.854 | −0.235 |
| Feature | F-stat | p (F-stat) | |
|---|---|---|---|
| Age | 0.128 | 9.035 | 0.00407 |
| IQ | 0.201 | 13.09 | 0.000673 |
| Cog Comp | 0.262 | 18.47 | |
| DET | 0.335 | 26.24 | |
| OCL | 0.319 | 24.39 | |
| ONB | 0.318 | 24.22 | |
| IDN | 0.325 | 25.04 |
| Cognitive Score | Feature | Coef | Std Error | t | |||
|---|---|---|---|---|---|---|---|
| Age | |||||||
| Cst. | −0.0327 | 0.126 | −0.260 | 0.796 | −0.369 | 0.303 | |
| Hes | 0.3743 | 0.125 | 3.006 | 0.004 | 0.041 | 0.707 | |
| IQ | |||||||
| Cst. | −0.0229 | 0.123 | −0.186 | 0.853 | −0.352 | 0.306 | |
| Hes | −0.4414 | 0.122 | −3.618 | 0.001 | −0.768 | −0.115 | |
| Cog Comp | |||||||
| Cst. | 0.0074 | 0.120 | −0.061 | 0.951 | −0.314 | 0.329 | |
| Hes | −0.5116 | 0.119 | −4.298 | 0.000 | −0.830 | −0.193 | |
| DET | |||||||
| Cst. | −0.0137 | 0.113 | −0.121 | 0.904 | −0.317 | 0.289 | |
| Hes | −0.5756 | 0.112 | −5.122 | 0.000 | −0.876 | −0.275 | |
| OCL | |||||||
| Cst. | −0.0163 | 0.114 | −0.142 | 0.887 | −0.322 | 0.290 | |
| Hes | −0.5603 | 0.113 | −4.938 | 0.000 | −0.864 | −0.257 | |
| ONB | |||||||
| Const. | −0.0155 | 0.115 | −0.135 | 0.893 | −0.322 | 0.291 | |
| Hes | −0.5594 | 0.114 | −4.921 | 0.000 | −0.863 | −0.255 | |
| IDN | |||||||
| Cst. | −0.0147 | 0.114 | −0.129 | 0.898 | −0.320 | 0.291 | |
| Hes | −0.5661 | 0.113 | −5.004 | 0.000 | −0.869 | −0.264 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mannan, F.A.; Porffy, L.A.; Joyce, D.W.; Shergill, S.S.; Celiktutan, O. Automatic Detection of Cognitive Impairment with Virtual Reality. Sensors 2023, 23, 1026. https://doi.org/10.3390/s23021026
Mannan FA, Porffy LA, Joyce DW, Shergill SS, Celiktutan O. Automatic Detection of Cognitive Impairment with Virtual Reality. Sensors. 2023; 23(2):1026. https://doi.org/10.3390/s23021026
Chicago/Turabian StyleMannan, Farzana A., Lilla A. Porffy, Dan W. Joyce, Sukhwinder S. Shergill, and Oya Celiktutan. 2023. "Automatic Detection of Cognitive Impairment with Virtual Reality" Sensors 23, no. 2: 1026. https://doi.org/10.3390/s23021026