

Acute Recovery after a Fatigue Protocol Using a Recovery Sports Legging: An Experimental Study
 , , ,
, , ,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
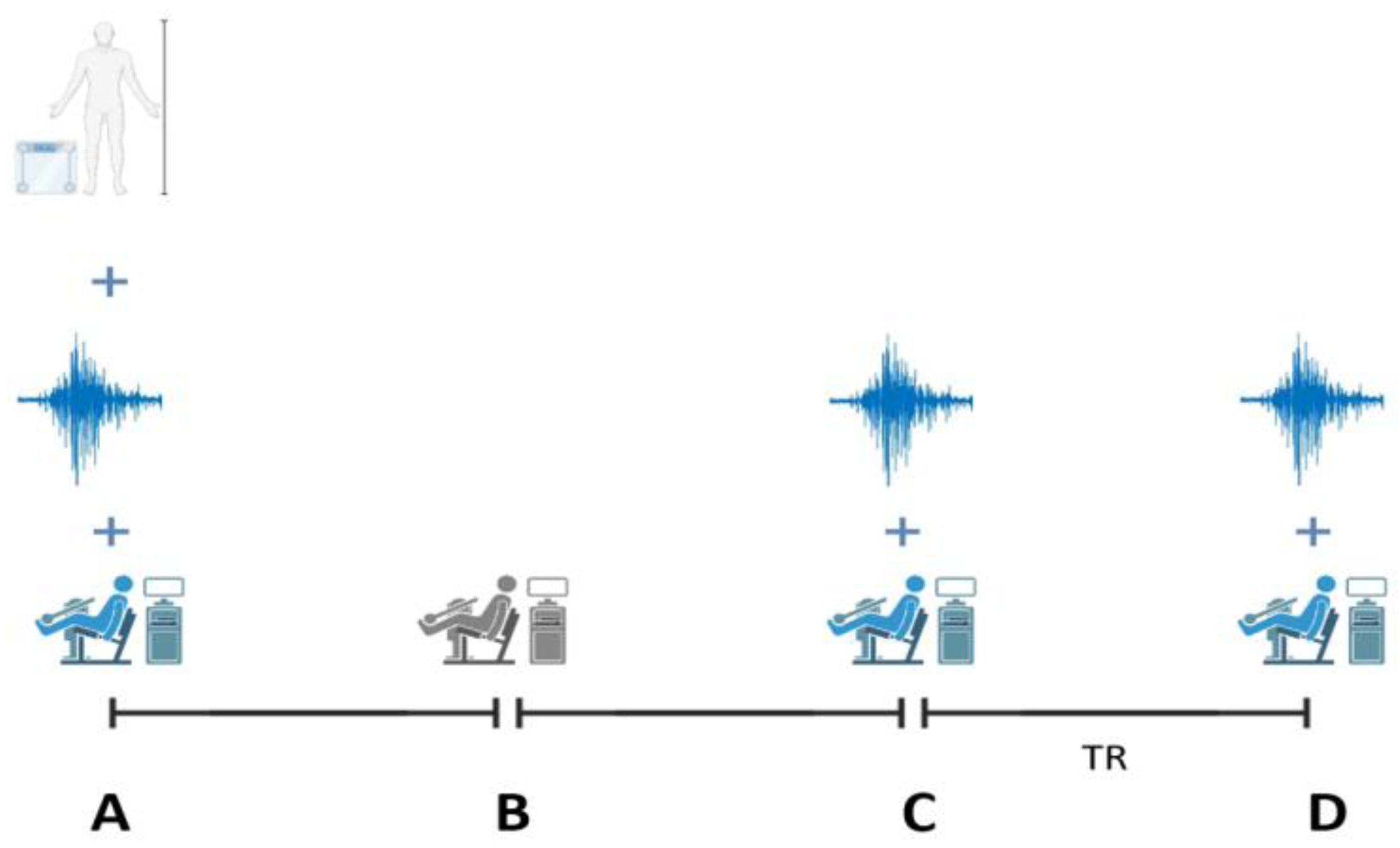
2.2. Experimental Design
2.3. Intervention
2.3.1. Localised Heating
2.3.2. Compression
2.3.3. Electrostimulation
2.3.4. Control Group
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nédélec, M.; McCall, A.; Carling, C.; Legall, F.; Berthoin, S.; Dupont, G. Recovery in soccer: Part I—Post-match fatigue and time course of recovery. Sports Med. 2012, 42, 997–1015. [Google Scholar] [PubMed]
- Halson, S.L. Monitoring Training Load to Understand Fatigue in Athletes. Sports Med. 2014, 44, 139–147. [Google Scholar] [CrossRef]
- Halson, S.L. Sleep in elite athletes and nutritional interventions to enhance sleep. Sports Med. 2014, 44 (Suppl. 1), S13–S23. [Google Scholar] [CrossRef] [PubMed]
- Versey, N.G.; Halson, S.L.; Dawson, B.T. Water immersion recovery for athletes: Effect on exercise performance and practical recommendations. Sports Med. 2013, 43, 1101–1130. [Google Scholar] [CrossRef]
- Duarte, J.P.; Silva, G.; Sousa, F.; Machado, L.; Fernandes, R.J.; Vilas-Boas, J.P. The Post-Exercise Lower Limbs Recovery Process: A Questionnaire Applied to Physiotherapists. Open Sports Sci. J. 2023, 16, e1875399X2301300. [Google Scholar]
- Duarte, J.P.; Fernandes, R.J.; Silva, G.; Sousa, F.; Machado, L.; Pereira, J.R.; Vilas-Boas, J.P. Lower Limbs Wearable Sports Garments for Muscle Recovery: An Umbrella Review. Healthcare 2022, 10, 1552. [Google Scholar] [CrossRef] [PubMed]
- Babault, N.; Cometti, C.; Maffiuletti, N.A.; Deley, G. Does electrical stimulation enhance post-exercise performance recovery? Eur. J. Appl. Physiol. 2011, 111, 2501–2507. [Google Scholar] [CrossRef] [PubMed]
- Maffiuletti, N.A. Physiological and methodological considerations for the use of neuromuscular electrical stimulation. Eur. J. Appl. Physiol. 2010, 110, 223–234. [Google Scholar] [CrossRef]
- Lattier, G.; Millet, G.Y.; Martin, A.; Martin, V. Fatigue and recovery after high-intensity exercise. Part II: Recovery interventions. Int. J. Sports Med. 2004, 25, 509–515. [Google Scholar] [CrossRef]
- Day, J.T.; Newman, J. The effect of neuromuscular electrical stimulation on function outcome measures following muscle fatigue: A systematic review. Curr. Orthop. Pract. 2020, 31, 394–399. [Google Scholar]
- Thorpe, R.T. Post-exercise Recovery: Cooling and Heating, a Periodized Approach. Front. Sports Act. Living 2021, 3, 707503. [Google Scholar] [CrossRef] [PubMed]
- Ihsan, M.; Deldicque, L.; Molphy, J.; Britto, F.; Cherif, A.; Racinais, S. Skeletal Muscle Signaling Following Whole-Body and Localized Heat Exposure in Humans. Front. Physiol. 2020, 11, 839. [Google Scholar] [CrossRef]
- Kim, K.; Kuang, S.; Song, Q.; Gavin, T.P.; Roseguini, B.T. Impact of heat therapy on recovery after eccentric exercise in humans. J. Appl. Physiol. 2019, 126, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Sabapathy, M.; Tan, F.; Al Hussein, S.; Jaafar, H.; Brocherie, F.; Racinais, S.; Ihsan, M. Effect of heat pre-conditioning on recovery following exercise-induced muscle damage. Curr. Res. Physiol. 2021, 4, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Monroe, J.C.; Gavin, T.P.; Roseguini, B.T. Local Heat Therapy to Accelerate Recovery After Exercise-Induced Muscle Damage. Exerc. Sport Sci. Rev. 2020, 48, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Brunt, V.E.; Howard, M.J.; Francisco, M.A.; Ely, B.R.; Minson, C.T. Passive heat therapy improves endothelial function, arterial stiffness and blood pressure in sedentary humans. J. Physiol. 2016, 594, 5329–5342. [Google Scholar] [CrossRef]
- Sobajima, M.; Nozawa, T.; Fukui, Y.; Ihori, H.; Ohori, T.; Fujii, N.; Inoue, H. Waon therapy improves quality of life as well as cardiac function and exercise capacity in patients with chronic heart failure. Int. Heart J. 2015, 56, 203–208. [Google Scholar] [CrossRef]
- Liu, R.; Lao, T.T.; Kwok, Y.L.; Li, Y.; Ying, M.T. Effects of graduated compression stockings with different pressure profiles on lower-limb venous structures and haemodynamics. Adv. Ther. 2008, 25, 465–478. [Google Scholar] [CrossRef]
- Da Silva, C.A.; Helal, L.; da Silva, R.P.; Belli, K.C.; Umpierre, D.; Stein, R. Association of Lower Limb Compression Garments During High-Intensity Exercise with Performance and Physiological Responses: A Systematic Review and Meta-analysis. Sports Med. 2018, 48, 1859–1873. [Google Scholar] [CrossRef]
- Davies, V.; Thompson, K.G.; Cooper, S.M. The effects of compression garments on recovery. J. Strength Cond. Res. 2009, 23, 1786–1794. [Google Scholar] [CrossRef]
- Jakeman, J.R.; Byrne, C.; Eston, R.G. Efficacy of lower limb compression and combined treatment of manual massage and lower limb compression on symptoms of exercise-induced muscle damage in women. J. Strength Cond. Res. 2010, 24, 3157–3165. [Google Scholar] [CrossRef] [PubMed]
- Carling, J.; Francis, K.; Lorish, C. The effects of continuous external compression on delayed-onset muscle soreness (DOMS). Int. J. Rehabil. Health 1995, 1, 223–235. [Google Scholar] [CrossRef]
- Pérez-Soriano, P.; García-Roig, Á.; Sanchis-Sanchis, R.; Aparicio, I. Influence of compression sportswear on recovery and performance: A systematic review. J. Ind. Text. 2018, 48, 1505–1524. [Google Scholar] [CrossRef]
- Weakley, J.; Broatch, J.; O’Riordan, S.; Morrison, M.; Maniar, N.; Halson, S.L. Putting the Squeeze on Compression Garments: Current Evidence and Recommendations for Future Research: A Systematic Scoping Review. Sports Med. 2022, 52, 1141–1160. [Google Scholar] [CrossRef]
- McGorm, H.; Roberts, L.A.; Coombes, J.S.; Peake, J.M. Turning Up the Heat: An Evaluation of the Evidence for Heating to Promote Exercise Recovery, Muscle Rehabilitation and Adaptation. Sports Med. 2018, 48, 1311–1328. [Google Scholar] [CrossRef] [PubMed]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining Training and Performance Caliber: A Participant Classification Frameworknt. J. Sports Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. SENIAM: European Recommendations for Surface Electromyography: Results of the SENIAM Project; Roessingh Research and Development: Enschede, The Netherlands, 1999; Volume 8, pp. 13–54. [Google Scholar]
- Priego-Quesada, J.I.; Goethel, M.F.; Becker, K.M.; Fernandes, R.J.; Vilas-Boas, J.P. How to Work with Electromyography Decomposition in Practical Classes of Exercise Physiology and Biomechanics. Life 2022, 12, 483. [Google Scholar] [CrossRef]
- Sumida, K.D.; Greenberg, M.B.; Hill, J.M. Hot Gel Packs and Reduction of Delayed-Onset Muscle Soreness 30 Minutes After Treatment. J. Sport Rehabil. 2003, 12, 221–228. [Google Scholar] [CrossRef]
- Otsuka, K.; Ren, X. Recent developments in the research of shape memory alloys. Intermetallics 1999, 7, 511–528. [Google Scholar] [CrossRef]
- Argus, C.K.; Driller, M.W.; Ebert, T.R.; Martin, D.T.; Halson, S.L. The effects of 4 different recovery strategies on repeat sprint-cycling performance. Int. J. Sports Physiol. Perform. 2013, 8, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Taylor, T.; West, D.J.; Howatson, G.; Jones, C.; Bracken, R.M.; Love, T.D.; Cook, C.J.; Swift, E.; Baker, J.S.; Kilduff, L.P. The impact of neuromuscular electrical stimulation on recovery after intensive, muscle damaging, maximal speed training in professional team sports players. J. Sci. Med. Sport 2015, 18, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Bieuzen, F.; Pournot, H.; Roulland, R.; Hausswirth, C. Recovery After High-Intensity Intermittent Exercise in Elite Soccer Players Using VEINOPLUS Sport Technology for Blood-Flow Stimulation. J. Athl. Train. 2012, 47, 498–506. [Google Scholar] [CrossRef]
- Martínez-Gómez, R.; Valenzuela, P.L.; Lucia, A.; Barranco-Gil, D. Comparison of Different Recovery Strategies After High-Intensity Functional Training: A Crossover Randomized Controlled Trial. Front. Physiol. 2022, 13, 819588. [Google Scholar] [CrossRef]
- Byrne, C.; Twist, C.; Eston, R. Neuromuscular Function After Exercise-Induced Muscle Damage. Sports Med. 2004, 34, 49–69. [Google Scholar] [CrossRef]
- Wang, Y.; Li, S.; Zhang, Y.; Chen, Y.; Yan, F.; Han, L.; Ma, Y. Heat and cold therapy reduce pain in patients with delayed onset muscle soreness: A systematic review and meta-analysis of 32 randomized controlled trials. Phys. Ther. Sport 2021, 48, 177–187. [Google Scholar] [CrossRef]
- Hill, J.; Howatson, G.; van Someren, K.; Leeder, J.; Pedlar, C. Compression garments and recovery from exercise-induced muscle damage: A meta-analysis. Br. J. Sports Med. 2014, 48, 1340–1346. [Google Scholar] [CrossRef]
- Négyesi, J.; Hortobágyi, T.; Hill, J.; Granacher, U.; Nagatomi, R. Can Compression Garments Reduce the Deleterious Effects of Physical Exercise on Muscle Strength? A Systematic Review and Meta-Analyses. Sports Med. 2022, 52, 2159–2175. [Google Scholar] [CrossRef] [PubMed]
- Négyesi, J.; Zhang, L.Y.; Jin, R.N.; Hortobágyi, T.; Nagatomi, R. A below-knee compression garment reduces fatigue-induced strength loss but not knee joint position sense errors. Eur. J. Appl. Physiol. 2021, 121, 219–229. [Google Scholar] [CrossRef]
- Ibegbuna, V.; Delis, K.T.; Nicolaides, A.N.; Aina, O. Effect of elastic compression stockings on venous hemodynamics during walking. J. Vasc. Surg. 2003, 37, 420–425. [Google Scholar] [CrossRef]
- Maton, B.; Thiney, G.; Dang, S.; Tra, S.; Bassez, S.; Wicart, P.; Ouchene, A. Human muscle fatigue and elastic compressive stockings. Eur. J. Appl. Physiol. 2006, 97, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A.M.; Stout, J.R.; Jajtner, A.R.; Townsend, J.R.; Wells, A.J.; Beyer, K.S.; Boone, C.H.; Pruna, G.J.; Mangine, G.T.; Scanlon, T.M.; et al. Effects of β-hydroxy-β-methylbutyrate free acid and cold water immersion on post-exercise markers of muscle damage. Amino Acids 2014, 46, 1501–1511. [Google Scholar] [CrossRef] [PubMed]
- Markus, I.; Constantini, K.; Hoffman, J.R.; Bartolomei, S.; Gepner, Y. Exercise-induced muscle damage: Mechanism, assessment and nutritional factors to accelerate recovery. Eur. J. Appl. Physiol. 2021, 121, 969–992. [Google Scholar] [CrossRef] [PubMed]
- Peake, J.M.; Neubauer, O.; Della Gatta, P.A.; Nosaka, K. Muscle damage and inflammation during recovery from exercise. J. Appl. Physiol. 2016, 122, 559–570. [Google Scholar] [CrossRef]
- Baumert, P.; Lake, M.J.; Stewart, C.E.; Drust, B.; Erskine, R.M. Genetic variation and exercise-induced muscle damage: Implications for athletic performance, injury and ageing. Eur. J. Appl. Physiol. 2016, 116, 1595–1625. [Google Scholar] [CrossRef]
- Hayashi, K.; Leary, M.E.; Roy, S.J.; Laosiripisan, J.; Pasha, E.P.; Tanaka, H. Recovery from Strenuous Downhill Running in Young and Older Physically Active Adults. Int. J. Sports. Med. 2019, 40, 696–703. [Google Scholar] [CrossRef]
- De Carvalho, G.; Girasol, C.E.; Gonçalves, L.G.C.; Guirro, E.C.O.; Guirro, R.R.d.J. Correlation between skin temperature in the lower limbs and biochemical marker, performance data, and clinical recovery scales. PLoS ONE 2021, 16, e0248653. [Google Scholar] [CrossRef]
- Machado, A.F.; Micheletti, J.K.; Lopes, J.S.S.; Vanderlei, F.M.; Leal-Junior, E.C.P.; Netto Junior, J.; Pastre, C.M. Phototherapy on Management of Creatine Kinase Activity in General Versus Localized Exercise: A Systematic Review and Meta-Analysis. Clin. J. Sport Med. 2020, 30, 267–274. [Google Scholar] [CrossRef]
- Felici, F.; Del Vecchio, A. Surface Electromyography: What Limits Its Use in Exercise and Sport Physiology? Front. Neurol. 2020, 11, 578504. [Google Scholar] [CrossRef]
- Del Vecchio, A.; Holobar, A.; Falla, D.; Felici, F.; Enoka, R.M.; Farina, D. Tutorial: Analysis of motor unit discharge characteristics from high-density surface EMG signals. J. Electromyogr. Kinesiol. 2020, 53, 102426. [Google Scholar] [CrossRef]
- Bigland-Ritchie, B.; Johansson, R.; Lippold, O.C.; Smith, S.; Woods, J.J. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J. Physiol. 1983, 340, 335–346. [Google Scholar] [CrossRef] [PubMed]
- De Luca, C.J.; Foley, P.J.; Erim, Z. Motor unit control properties in constant-force isometric contractions. J. Neurophysiol. 1996, 76, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Adam, A.; De Luca, C.J. Firing rates of motor units in human vastus lateralis muscle during fatiguing isometric contractions. J. Appl. Physiol. 2005, 99, 268–280. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Participant ID | Legging | Digitimer DS8R |
|---|---|---|
| 01 | 20 mA | 8.5 mA |
| 02 | 20 mA | 9.5 mA |
| 03 | 15 mA | 5.0 mA |
| 04 | 10 mA | 5.0 mA |
| 05 | 30 mA | 8.0 mA |
| 06 | 15 mA | 4.5mA |
| 07 | 15 mA | 10.0 mA |
| 08 | 20 mA | 4.5 mA |
| Measure | Method | Instant | Instant | Mean Differences | p Value | d Value | Power |
|---|---|---|---|---|---|---|---|
| Peak torque | Localised heating | Pre-fatigue | Post-fatigue | 15.456 | 0.001 | 5.53 | 1 |
| Pre-fatigue | Post-recovery | 8.247 | 0.229 | 1.7 | 0.93 | ||
| Post-fatigue | Post-recovery | −7.209 | 0.382 | 2.6 | 0.99 | ||
| Compression | Pre-fatigue | Post-fatigue | 16.208 | 0.001 | 0.69 | 0.37 | |
| Pre-fatigue | Post-recovery | 8.294 | 0.181 | 1.49 | 0.89 | ||
| Post-fatigue | Post-recovery | 9.902 | 0.119 | 1.55 | 0.90 | ||
| Electrostimulation | Pre-fatigue | Post-fatigue | 8.924 | 0.091 | 1.99 | 1 | |
| Pre-fatigue | Post-recovery | 13.623 | 0.014 | 2.24 | 0.94 | ||
| Post-fatigue | Post-recovery | 4.700 | 0.943 | 0.73 | 0.85 | ||
| Control | Pre-fatigue | Post-fatigue | 14.354 | 0.001 | 7.03 | 0.99 | |
| Pre-fatigue | Post-recovery | 4.602 | 0.926 | 1.61 | 0.99 | ||
| Post-fatigue | Post-recovery | −4.199 | 1.000 | 1.42 | 0.40 | ||
| Peak torque EMG | Localised heating | Pre-fatigue | Post-fatigue | 3.639 | 1.000 | 0.47 | 0.14 |
| Pre-fatigue | Post-recovery | −8.955 | 1.000 | 0.65 | 0.23 | ||
| Post-fatigue | Post-recovery | −12.595 | 1.000 | 0.29 | 0.08 | ||
| Compression | Pre-fatigue | Post-fatigue | −18.604 | 0.527 | 1.66 | 0.87 | |
| Pre-fatigue | Post-recovery | −29.689 | 0.188 | 2.1 | 0.97 | ||
| Post-fatigue | Post-recovery | −11.085 | 1.000 | 0.73 | 0.27 | ||
| Electrostimulation | Pre-fatigue | Post-fatigue | 3.090 | 1.000 | 0.5 | 0.15 | |
| Pre-fatigue | Post-recovery | 1.566 | 1.000 | 0.5 | 0.15 | ||
| Post-fatigue | Post-recovery | −1.524 | 1.000 | 0.71 | 0.26 | ||
| Control | Pre-fatigue | Post-fatigue | −17.651 | 0.594 | 5.73 | 1 | |
| Pre-fatigue | Post-recovery | −21.039 | 0.542 | 3.61 | 0.99 | ||
| Post-fatigue | Post-recovery | −3.388 | 1.000 | 5.74 | 1 | ||
| Impulse | Localised heating | Pre-fatigue | Post-fatigue | 18.226 | 0.014 | 3.33 | 0.99 |
| Pre-fatigue | Post-recovery | 11.595 | 0.604 | 2.61 | 0.99 | ||
| Post-fatigue | Post-recovery | −6.631 | 1.000 | 0.95 | 0.42 | ||
| Compression | Pre-fatigue | Post-fatigue | −3.365 | 1.000 | 0.81 | 0.33 | |
| Pre-fatigue | Post-recovery | 9.611 | 0.957 | 1.35 | 0.71 | ||
| Post-fatigue | Post-recovery | 12.976 | 0.447 | 1.59 | 0.84 | ||
| Electrostimulation | Pre-fatigue | Post-fatigue | 7.639 | 0.625 | 1.71 | 0.89 | |
| Pre-fatigue | Post-recovery | 17.653 | 0.169 | 1.91 | 0.94 | ||
| Post-fatigue | Post-recovery | 10.014 | 0.693 | 0.98 | 0.45 | ||
| Control | Pre-fatigue | Post-fatigue | 15.356 | 0.046 | 5.71 | 1 | |
| Pre-fatigue | Post-recovery | 3.259 | 1.000 | 1 | 0.46 | ||
| Post-fatigue | Post-recovery | −12.098 | 0.451 | 2.95 | 0.99 | ||
| Peak EMG | Localised heating | Pre-fatigue | Post-fatigue | 0.743 | 1.000 | 0.9 | 0.39 |
| Pre-fatigue | Post-recovery | 8.004 | 1.000 | 1.05 | 0.5 | ||
| Post-fatigue | Post-recovery | 7.260 | 1.000 | 0.67 | 0.24 | ||
| Compression | Pre-fatigue | Post-fatigue | −9.637 | 1.000 | 1.24 | 0.64 | |
| Pre-fatigue | Post-recovery | −30.328 | 0.083 | 2.14 | 0.98 | ||
| Post-fatigue | Post-recovery | −20.691 | 0.386 | 1.28 | 0.66 | ||
| Electrostimulation | Pre-fatigue | Post-fatigue | 2.204 | 1.000 | 0.86 | 0.36 | |
| Pre-fatigue | Post-recovery | 9.447 | 1.000 | 4.55 | 1 | ||
| Post-fatigue | Post-recovery | 7.243 | 1.000 | 2.31 | 0.99 | ||
| Control | Pre-fatigue | Post-fatigue | −19.930 | 0.198 | 2.02 | 0.96 | |
| Pre-fatigue | Post-recovery | −7.187 | 1.000 | 0.82 | 0.33 | ||
| Post-fatigue | Post-recovery | 12.743 | 0.933 | 0.97 | 0.44 | ||
| Integral EMG | Localised heating | Pre-fatigue | Post-fatigue | 4.263 | 1.000 | 0.56 | 0.18 |
| Pre-fatigue | Post-recovery | 10.879 | 0.966 | 1.26 | 0.65 | ||
| Post-fatigue | Post-recovery | 6.616 | 1.000 | 0.57 | 0.18 | ||
| Compression | Pre-fatigue | Post-fatigue | −0.901 | 1.000 | 0.07 | 0.05 | |
| Pre-fatigue | Post-recovery | −4.459 | 1.000 | 0.63 | 0.21 | ||
| Post-fatigue | Post-recovery | −3.558 | 1.000 | 0.25 | 0.08 | ||
| Electrostimulation | Pre-fatigue | Post-fatigue | 5.707 | 1.000 | 0.94 | 0.41 | |
| Pre-fatigue | Post-recovery | 5.631 | 1.000 | 0.71 | 0.26 | ||
| Post-fatigue | Post-recovery | −0.076 | 1.000 | 0.007 | 0.05 | ||
| Control | Pre-fatigue | Post-fatigue | −6.836 | 1.000 | 0.79 | 0.31 | |
| Pre-fatigue | Post-recovery | −19.979 | 0.224 | 2.79 | 0.99 | ||
| Post-fatigue | Post-recovery | −13.143 | 0.698 | 1.18 | 0.59 | ||
| Neuromechanical efficiency | Localised heating | Pre-fatigue | Post-fatigue | 11.139 | 1.000 | 2.32 | 0.99 |
| Pre-fatigue | Post-recovery | −13.387 | 0.855 | 0.93 | 0.41 | ||
| Post-fatigue | Post-recovery | −24.527 | 0.201 | 1.62 | 0.85 | ||
| Compression | Pre-fatigue | Post-fatigue | −20.990 | 0.290 | 1.39 | 0.73 | |
| Pre-fatigue | Post-recovery | 8.276 | 1.000 | 0.93 | 0.41 | ||
| Post-fatigue | Post-recovery | 29.266 | 0.127 | 1.67 | 0.87 | ||
| Electrostimulation | Pre-fatigue | Post-fatigue | −0.303 | 1.000 | 0.86 | 0.36 | |
| Pre-fatigue | Post-recovery | 13.828 | 0.810 | 3.18 | 0.99 | ||
| Post-fatigue | Post-recovery | 14.130 | 0.843 | 2.35 | 0.99 | ||
| Control | Pre-fatigue | Post-fatigue | 14.714 | 0.624 | 0.7 | 0.05 | |
| Pre-fatigue | Post-recovery | 17.474 | 0.498 | 6.86 | 1 | ||
| Post-fatigue | Post-recovery | 2.760 | 1.000 | 2.63 | 0.99 |
| Measure | Instant | Mean Differences | p Value | d | Power |
|---|---|---|---|---|---|
| Peak torque | Pre-fatigue | - | - | - | - |
| Post-fatigue | 2.299 | 1.000 | 0.29 | 0.08 | |
| Post-recovery | −6.085 | 1.000 | 0.76 | 0.29 | |
| Peak torque EMG | Pre-fatigue | - | - | - | - |
| Post-fatigue | −21.597 | 1.000 | 2.17 | 0.98 | |
| Post-recovery | −15.895 | 1.000 | 1.97 | 0.96 | |
| Impulse | Pre-fatigue | - | - | - | - |
| Post-fatigue | 7.718 | 1.000 | 0.97 | 0.44 | |
| Post-recovery | −14.393 | 1.000 | 1.8 | 0.92 | |
| Peak EMG | Pre-fatigue | - | - | - | - |
| Post-fatigue | −22.134 | 0.863 | 2.77 | 0.99 | |
| Post-recovery | −16.634 | 1.000 | 2.08 | 0.97 | |
| Integral EMG | Pre-fatigue | - | - | - | - |
| Post-fatigue | −12.543 | 1.000 | 1.57 | 0.83 | |
| Post-recovery | −25.610 | 0.627 | 3.2 | 0.99 | |
| Neuromechanical efficiency | Pre-fatigue | - | - | - | - |
| Post-fatigue | 15.017 | 1.000 | 1.87 | 0.93 | |
| Post-recovery | 3.647 | 1.000 | 0.46 | 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, G.; Goethel, M.; Machado, L.; Sousa, F.; Costa, M.J.; Magalhães, P.; Silva, C.; Midão, M.; Leite, A.; Couto, S.; et al. Acute Recovery after a Fatigue Protocol Using a Recovery Sports Legging: An Experimental Study. Sensors 2023, 23, 7634. https://doi.org/10.3390/s23177634
Silva G, Goethel M, Machado L, Sousa F, Costa MJ, Magalhães P, Silva C, Midão M, Leite A, Couto S, et al. Acute Recovery after a Fatigue Protocol Using a Recovery Sports Legging: An Experimental Study. Sensors. 2023; 23(17):7634. https://doi.org/10.3390/s23177634
Chicago/Turabian StyleSilva, Gonçalo, Márcio Goethel, Leandro Machado, Filipa Sousa, Mário Jorge Costa, Pedro Magalhães, Carlos Silva, Marta Midão, André Leite, Suse Couto, and et al. 2023. "Acute Recovery after a Fatigue Protocol Using a Recovery Sports Legging: An Experimental Study" Sensors 23, no. 17: 7634. https://doi.org/10.3390/s23177634