
Automatic Detection of Focal Cortical Dysplasia Using MRI: A Systematic Review
 , , , , , and
, , , , , and
Abstract
:1. Introduction
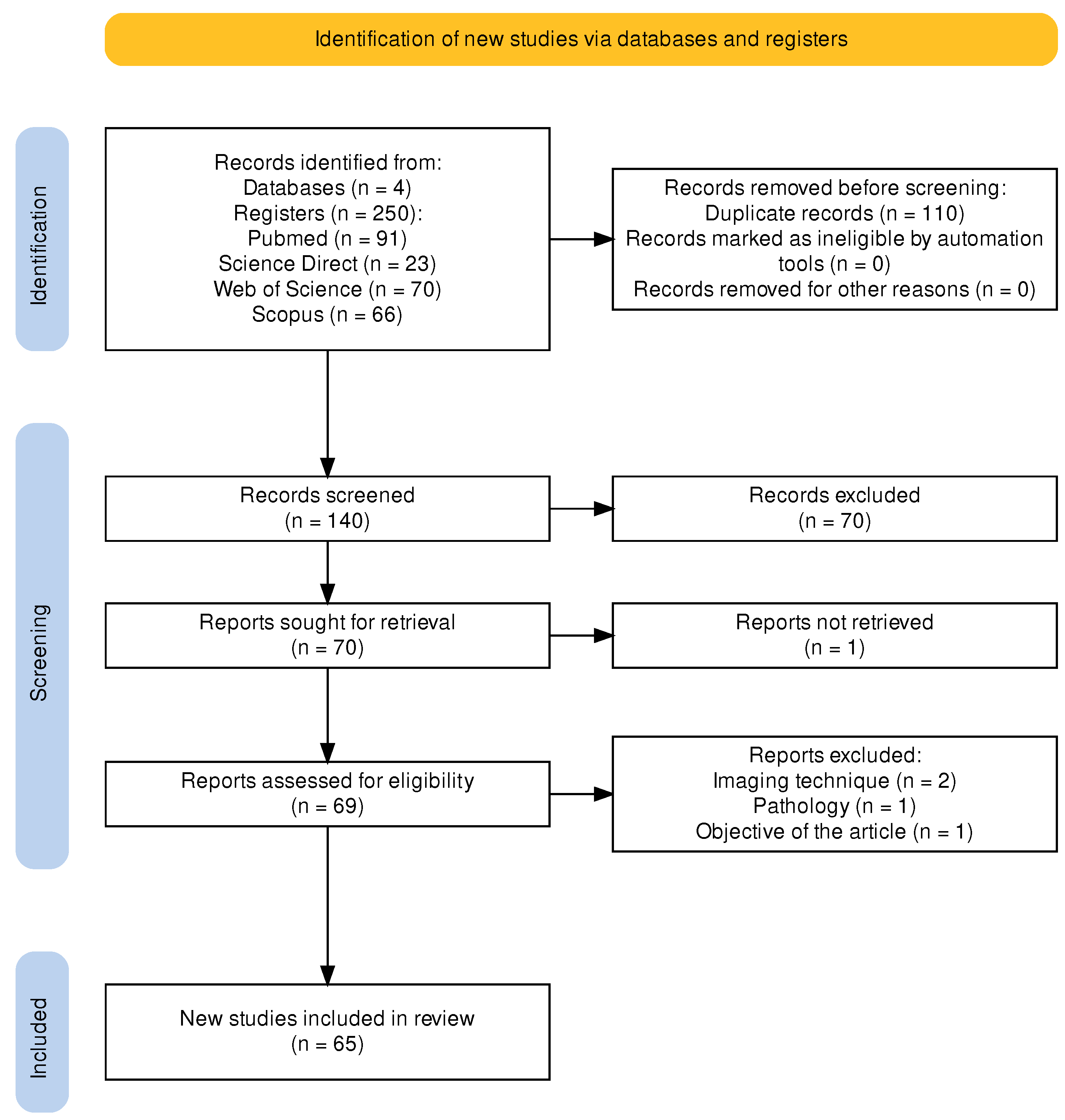
2. Materials and Methods
(((FCD) OR (Focal Cortical Dysplasia)) AND ((Automatic) OR (Automated)) AND ((MRI) OR (Magnetic Resonance Images)))
2.1. FCD Datasets
2.2. General Framework
2.3. Visual Methods
2.4. Semi-Automatic Methods
2.5. Automatic Methods
2.5.1. Mathematical Methods
2.5.2. Automatic Methods Based on Volumetric Morphometry
Voxel-Based Morphometry (VBM)
Statistical Parametric Mapping (SPM)
2.5.3. Automatic Methods Based on Machine Learning
Bayes Classifier
Support Vector Machines (SVMs)
Decision Trees
Other Machine Learning Methods
2.5.4. Automatic Methods Based on Deep Learning Algorithms
Artificial Neural Networks (ANNs)
Convolutional Neural Networks (CNNs)
3. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kabat, J.; Król, P. Focal cortical dysplasia–review. POlish J. Radiol. 2012, 77, 35. [Google Scholar] [CrossRef] [PubMed]
- Widdess-Walsh, P.; Kellinghaus, C.; Jeha, L.; Kotagal, P.; Prayson, R.; Bingaman, W.; Najm, I.M. Electro-clinical and imaging characteristics of focal cortical dysplasia: Correlation with pathological subtypes. Epilepsy Res. 2005, 67, 25–33. [Google Scholar] [CrossRef]
- Zvi, I.B.; Enright, N.; D’arco, F.; Tahir, M.Z.; Chari, A.; Cross, J.H.; Eltze, C.; Tisdall, M.M. Children with seizures and radiological diagnosis of focal cortical dysplasia: Can drug-resistant epilepsy be predicted earlier? Epileptic Disord. 2022, 24, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Veersema, T. Cognitive functioning after epilepsy surgery in children with mild malformation of cortical development and focal cortical dysplasia. Epilepsy Behav. 2019, 94, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyseni, F. The importance of magnetic resonance in detection of cortical dysplasia. Curr. Health Sci. J. 2021, 47, 585. [Google Scholar]
- Huppertz, H.-J.; Grimm, C.; Fauser, S.; Kassubek, J.; Mader, I.; Hochmuth, A.; Spreer, J.; Schulze-Bonhage, A. Enhanced visualization of blurred gray–white matter junctions in focal cortical dysplasia by voxel-based 3D MRI analysis. Epilepsy Res. 2005, 67, 35–50. [Google Scholar] [CrossRef]
- Bernasconi, A.; Antel, S.B.; Collins, D.L.; Bernasconi, N.; Olivier, A.; Dubeau, F.; Pike, G.B.; Andermann, F.; Arnold, D.L. Texture analysis and morphological processing of magnetic resonance imaging assist detection of focal cortical dysplasia in extra-temporal partial epilepsy. Ann. Neurol. 2001, 49, 770–775. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, Y.; Wang, H.; Cui, J.; Nguchu, B.A.; Zhang, X.; Qiu, B.; Wang, X.; Zhu, M. Voxel-based automated detection of focal cortical dysplasia lesions using diffusion tensor imaging and T2-weighted MRI data. Epilepsy Behav. 2018, 84, 127–134. [Google Scholar] [CrossRef]
- Ahmed, B.; Brodley, C.E.; Blackmon, K.E.; Kuzniecky, R.; Barash, G.; Carlson, C.; Quinn, B.T.; Doyle, W.; French, J.; Devinsky, O.; et al. Cortical feature analysis and machine learning improves detection of “MRI-negative” focal cortical dysplasia. Epilepsy Behav. 2015, 48, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Wang, I.; Alexopoulos, A. MRI postprocessing in presurgical evaluation. Curr. Opin. Neurol. 2016, 29, 168–174. [Google Scholar] [CrossRef] [Green Version]
- Ganji, Z.; Hakak, M.A.; Zamanpour, S.A.; Zare, H. Automatic Detection of Focal Cortical Dysplasia Type II in MRI: Is the Application of Surface-Based Morphometry and Machine Learning Promising? Front. Hum. Neurosci. 2021, 15, 2. [Google Scholar] [CrossRef]
- Feng, C.; Zhao, H.; Zhang, J.; Cheng, Z.; Wen, J. Automated localization of Epileptic Focus Using Convolutional Neural Network. Int. Conf. Big Data Eng. Technol. 2020, 72–75. [Google Scholar] [CrossRef] [Green Version]
- Baffa, M.D.F.O.; Pereira, J.; Simozo, F.H.; Murta, L.O.; Felipe, J.C., Jr. Focal cortical dysplasia classification for refractory epilepsy detection using artificial neural network. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2022, 11, 326–330. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar] [CrossRef]
- Lampinen, B.; Zampeli, A.; Björkman-Burtscher, I.M.; Szczepankiewicz, F.; Källén, K.; Strandberg, M.C.; Nilsson, M. Tensor-valued diffusion mri differentiates cortex and white matter in malformations of cortical development associated with epilepsy. Epilepsia 2020, 61, 1701–1713. [Google Scholar] [CrossRef] [PubMed]
- Antel, S.B.; Bernasconi, A.; Bernasconi, N.; Collins, D.L.; Kearney, R.E.; Shinghal, R.; Arnold, D.L. Computational Models of MRI Characteristics of Focal Cortical Dysplasia Improve Lesion Detection. NeuroImage 2002, 17, 1755–1760. [Google Scholar] [CrossRef]
- Roca, P.; Mellerio, C.; Chassoux, F.; Rivière, D.; Cachia, A.; Charron, S.; Lion, S.; Mangin, J.-F.; Devaux, B.; Meder, J.-F. Sulcus-Based MR Analysis of Focal Cortical Dysplasia Located in the Central Region. PLoS ONE 2015, 10, e0122252. [Google Scholar] [CrossRef]
- Sepúlveda, M.M.; Rojas, G.M.; Faure, E.; Pardo, C.R.; las Heras, F.; Okuma, C.; Cordovez, J.; Iglesia-Vayá, M.D.; Molina-Mateo, J.; Gálvez, M. Visual analysis of automated segmentation in the diagnosis of focal cortical dysplasias with magnetic resonance imaging. Epilepsy Behav. 2020, 102, 106684. [Google Scholar] [CrossRef] [PubMed]
- Lorio, S.; Adler, S.; Gunny, R.; D’Arco, F.; Kaden, E.; Wagstyl, K.; Jacques, T.S.; Clark, C.A.; Cross, J.H.; Baldeweg, T.; et al. MRI profiling of focal cortical dysplasia using multi-compartment diffusion models. Epilepsia 2020, 61, 433–444. [Google Scholar] [CrossRef]
- Colliot, O.; Mansi, T.; Bernasconi, N.; Naessens, V.; Klironomos, D.; Bernasconi, A. Segmentation of Focal Cortical Dysplasia Lesions Using a Feature-Based Level Set. Lect. Notes Comput. Sci. 2005, 3749, 375–382. [Google Scholar] [CrossRef] [Green Version]
- Colliot, O.; Mansi, T.; Bernasconi, N.; Naessens, V.; Klironomos, D.; Bernasconi, A. Segmentation of focal cortical dysplasia lesions on MRI using level set evolution. NeuroImage 2006, 32, 1621–1630. [Google Scholar] [CrossRef] [Green Version]
- Despotovic, I.; Segers, I.; Platisa, L.; Vansteenkiste, E.; Pizurica, A.; Deblaere, K.; Philips, W. Automatic 3D graph cuts for brain cortex segmentation in patients with focal cortical dysplasia. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011. [Google Scholar]
- Snyder, K.; Whitehead, E.P.; Theodore, W.H.; Zaghloul, K.A.; Inati, S.J.; Inati, S.K. Distinguishing type II focal cortical dysplasias from normal cortex: A novel normative modeling approach. NeuroImage Clin. 2021, 30, 102565. [Google Scholar] [CrossRef] [PubMed]
- Lotan, E.; Tomer, O.; Tavor, I.; Blatt, I.; Goldberg-Stern, H.; Hoffmann, C.; Tsarfaty, G.; Tanne, D.; Assaf, Y. Widespread cortical dyslamination in epilepsy patients with malformations of cortical development. Neuroradiology 2020, 63, 225–234. [Google Scholar] [CrossRef]
- Kassubek, J.; Huppertz, H.-J.; Spreer, J.; Schulze-Bonhage, A. Detection and Localization of Focal Cortical Dysplasia by Voxel-based 3-D MR Analysis. Epilepsia 2002, 43, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Qu, X.; Platisa, L.; Despotovic, I.; Kumcu, A.; Bai, T.; Deblaere, K.; Philips, W. Estimating blur at the brain gray-white matter boundary for FCD detection in MRI. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014. [Google Scholar]
- House, P.M.; Lanz, M.; Holst, B.; Martens, T.; Stodieck, S.; Huppertz, H.-J. Comparison of morphometric analysis based on T1- and T2-weighted MRI data for visualization of focal cortical dysplasia. Epilepsy Res. 2013, 106, 403–409. [Google Scholar] [CrossRef]
- Qu, X.; Yang, J.; Ai, D.; Song, H.; Zhang, L.; Wang, Y.; Bai, T.; Philips, W. Local Directional Probability Optimization for Quantification of Blurred Gray/White Matter Junction in Magnetic Resonance Image. Front. Comput. Neurosci. 2017, 11, 83. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Qian, T.; Maréchal, B.; Zhang, G.; Yu, T.; Ren, Z.; Ni, D.; Liu, C.; Fu, Y.; Chen, N. Quantitative volume-based morphometry in focal cortical dysplasia: A pilot study for lesion localization at the individual level. Eur. J. Radiol. 2018, 105, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Qu, X.; Deblaere, K.; Philips, W.; Yang, J.; Platis, L.; Kumcu, A.; Ai, D.; Goossens, B.; Bai, T.; Wang, Y. Multiple Classifier Fusion and Optimization for Automatic Focal Cortical Dysplasia Detection on Magnetic Resonance Images. IEEE Access 2018, 6, 73786–73801. [Google Scholar] [CrossRef]
- Feng, C.; Zhao, H.; Tian, M.; Lu, M.; Wen, J. Detecting focal cortical dysplasia lesions from FLAIR-negative images based on cortical thickness. Biomed. Eng. Online 2020, 19, 13. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, S.; Maes, F.; Vandermeulen, D.; Paesschen, W.V.; Dupont, P.; Suetens, P. Feature-based statistical analysis of structural MR data for automatic detection of focal cortical dysplastic lesions. NeuroImage 2005, 27, 253–266. [Google Scholar] [CrossRef]
- Focke, N.K.; Symms, M.R.; Burdett, J.L.; Duncan, J.S. Voxel-based analysis of whole brain FLAIR at 3T detects focal cortical dysplasia. Epilepsia 2008, 49, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Focke, N.K.; Bonelli, S.B.; Yogarajah, M.; Scott, C.; Symms, M.R.; Duncan, J.S. Automated normalized FLAIR imaging in MRI-negative patients with refractory focal epilepsy. Epilepsia 2009, 50, 1484–1490. [Google Scholar] [CrossRef] [PubMed]
- Wong-Kisiel, L.C.; Quiroga, D.F.T.; Kenney-Jung, D.L.; Witte, R.J.; Santana-Almansa, A.; Worrell, G.A.; Britton, J.; Brinkmann, B.H. Morphometric analysis on T1-weighted MRI complements visual MRI review in focal cortical dysplasia. Epilepsy Res. 2018, 140, 184–191. [Google Scholar] [CrossRef]
- Lin, Y.; Fang, Y.-H.D.; Wu, G.; Jones, S.E.; Prayson, R.A.; Moosa, A.N.V.; Overmyer, M.; Bena, J.; Larvie, M.; Bingaman, W.; et al. Quantitative positron emission tomography-guided magnetic resonance imaging postprocessing in magnetic resonance imaging-negative epilepsies. Epilepsia 2018, 59, 1583–1594. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Lin, Y.; Wang, S.; Jones, S.; Prayson, R.; Moosa, A.N.V.; McBride, A.; Gonzalez-Martinez, J.; Bingaman, W.; Najm, I. Voxel-based morphometric magnetic resonance imaging postprocessing in non-lesional pediatric epilepsy patients using pediatric normal databases. Eur. J. Neurol. 2019, 26, 969-e71. [Google Scholar] [CrossRef] [PubMed]
- Antel, S.B.; Collins, D.L.; Bernasconi, N.; Andermann, F.; Shinghal, R.; Kearney, R.E.; Arnold, D.L.; Bernasconi, A. Automated detection of focal cortical dysplasia lesions using computational models of their MRI characteristics and texture analysis. NeuroImage 2003, 19, 1748–1759. [Google Scholar] [CrossRef]
- Yang, C.-A.; Kaveh, M.; Erickson, B.J. Automated detection of Focal Cortical Dysplasia lesions on T1-weighted MRI using volume-based distributional features. In Proceedings of the 2011 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Chicago, IL, USA, 30 March–2 April 2011. [Google Scholar]
- Yang, C.-A.; Kaveh, M.; Erickson, B. Cluster-based differential features to improve detection accuracy of focal cortical dysplasia. SPIE Proc. 2012, 8315, 433–438. [Google Scholar] [CrossRef]
- Strumia, M.; Ramantani, G.; Mader, I.; Henning, J.; Bai, L.; Hadjidemetriou, S. Analysis of Structural MRI Data for the Localisation of Focal Cortical Dysplasia in Epilepsy. Clin.-Image Based Proced. Plan. Interv. 2013, 7761, 25–32. [Google Scholar] [CrossRef]
- Kulaseharan, S.; Aminpour, A.; Ebrahimi, M.; Widjaja, E. Identifying lesions in paediatric epilepsy using morphometric and textural analysis of magnetic resonance images. NeuroImage Clin. 2019, 21, 101663. [Google Scholar] [CrossRef]
- Feng, C.; Zhao, H.; Li, Y.; Cheng, Z.; Wen, J. Improved detection of focal cortical dysplasia in normal-appearing FLAIR images using a Bayesian classifier. Med. Phys. 2020, 48, 912–925. [Google Scholar] [CrossRef]
- Hong, S.-J.; Bernhardt, B.C.; Schrader, D.S.; Bernasconi, N.; Bernasconi, A. Whole-brain MRI phenotyping in dysplasia-related frontal lobe epilepsy. Neurology 2016, 86, 643–650. [Google Scholar] [CrossRef] [Green Version]
- Azami, M.E.; Hammers, A.; Jung, J.; Costes, N.; Bouet, R.; Lartizien, C. Detection of Lesions Underlying Intractable Epilepsy on T1-Weighted MRI as an Outlier Detection Problem. PLoS ONE 2016, 11, e0161498. [Google Scholar] [CrossRef] [Green Version]
- Tan, Y.-L.; Kim, H.; Lee, S.; Tihan, T.; Hoef, L.V.; Mueller, S.G.; Barkovich, A.J.; Xu, D.; Knowlton, R. Quantitative surface analysis of combined MRI and PET enhances detection of focal cortical dysplasias. NeuroImage 2018, 166, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Gill, R.S.; Hong, S.-J.; Fadaie, F.; Caldairou, B.; Bernhardt, B.; Bernasconi, N.; Bernasconi, A. Automated Detection of Epileptogenic Cortical Malformations Using Multimodal MRI. Deep. Learn. Med. Image Anal. Multimodal Learn. Clin. Decis. Support 2017, 10553, 349–356. [Google Scholar] [CrossRef]
- Lin, Y.; Mo, J.; Jin, H.; Cao, X.; Zhao, Y.; Wu, C.; Zhang, K.; Hu, W.; Lin, Z. Automatic analysis of integrated magnetic resonance and positron emission tomography images improves the accuracy of detection of focal cortical dysplasia type IIb lesions. Eur. J. Neurosci. 2021, 53, 3231–3241. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-J.; Kim, H.; Schrader, D.; Bernasconi, N.; Bernhardt, B.C.; Bernasconi, A. Automated detection of cortical dysplasia type II in MRI-negative epilepsy. Neurology 2014, 83, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Qu, X.; Yang, J.; Ma, S.; Zhao, Y.; Bai, T. An unanimous voting of the multiple classifiers method for detecting focal cortical dysplasia on brain magnetic resonance image. In Proceedings of the 2015 IET International Conference on Biomedical Image and Signal Processing (ICBISP 2015), Beijing, China, 19 November 2015. [Google Scholar]
- Qu, X.; Yang, J.; Ma, S.; Bai, T.; Philips, W. Positive Unanimous Voting Algorithm for Focal Cortical Dysplasia Detection on Magnetic Resonance Image. Front. Comput. Neurosci. 2016, 10, 25. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.M.; Gill, R.S.; Fadaie, F.; Cho, K.H.; Guiot, M.C.; Hong, S.-J.; Bernasconi, N.; Bernasconi, A. Unsupervised machine learning reveals lesional variability in focal cortical dysplasia at mesoscopic scale. NeuroImage Clin. 2020, 28, 102438. [Google Scholar] [CrossRef] [PubMed]
- Jin, B.; Krishnan, B.; Adler, S.; Wagstyl, K.; Hu, W.; Jones, S.; Najm, I.; Alexopoulos, A.; Zhang, K.; Zhang, J. Automated detection of focal cortical dysplasia type II with surface-based magnetic resonance imaging postprocessing and machine learning. Epilepsia 2018, 59, 982–992. [Google Scholar] [CrossRef] [Green Version]
- Besson, P.; Andermann, F.; Dubeau, F.; Bernasconi, A. Small focal cortical dysplasia lesions are located at the bottom of a deep sulcus. Brain 2008, 131, 3246–3255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besson, P.; Colliot, O.; Evans, A.; Bernasconi, A. Automatic detection of subtle focal cortical dysplasia using surface-based features on MRI. In Proceedings of the 2008 5th IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Paris, France, 14–17 May 2008. [Google Scholar]
- Besson, P.; Bernasconi, N.; Colliot, O.; Evans, A.; Bernasconi, A. Surface-Based Texture and Morphological Analysis Detects Subtle Cortical Dysplasia. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention—MICCAI 2008, New York, NY, USA, 6–10 September 2008; pp. 645–652. [Google Scholar]
- Adler, S.; Wagstyl, K.; Gunny, R.; Ronan, L.; Carmichael, D.; Cross, J.H.; Fletcher, P.C.; Baldeweg, T. Novel surface features for automated detection of focal cortical dysplasias in paediatric epilepsy. NeuroImage Clin. 2017, 14, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Mo, J.-J.; Zhang, J.-G.; Li, W.-L.; Chen, C.; Zhou, N.-J.; Hu, W.-H.; Zhang, C.; Wang, Y.; Wang, X.; Liu, C.; et al. Clinical Value of Machine Learning in the Automated Detection of Focal Cortical Dysplasia Using Quantitative Multimodal Surface-Based Features. Front. Neurosci. 2019, 12, 1008. [Google Scholar] [CrossRef] [Green Version]
- Wagstyl, K.; Adler, S.; Pimpel, B.; Chari, A.; Seunarine, K.; Lorio, S.; Thornton, R.; Baldeweg, T.; Tisdall, M. Planning stereoelectroencephalography using automated lesion detection: Retrospective feasibility study. Epilepsia 2020, 61, 1406–1416. [Google Scholar] [CrossRef]
- David, B.; Kröll-Seger, J.; Schuch, F.; Wagner, J.; Wellmer, J.; Woermann, F.; Oehl, B.; Paesschen, W.V.; Breyer, T.; Becker, A.; et al. External validation of automated focal cortical dysplasia detection using morphometric analysis. Epilepsia 2021, 62, 1005–1021. [Google Scholar] [CrossRef]
- Gill, R.S.; Hong, S.-J.; Fadaie, F.; Caldairou, B.; Bernhardt, B.C.; Barba, C.; Brandt, A.; Coelho, V.C.; d’Incerti, L.; Lenge, M.; et al. Deep Convolutional Networks for Automated Detection of Epileptogenic Brain Malformations. In Proceedings of the Medical Image Computing and Computer Assisted Intervention—MICCAI 2018, Granada, Spain, 16–20 September 2018; pp. 490–497. [Google Scholar]
- Dev, K.B.; Jogi, P.S.; Niyas, S.; Vinayagamani, S.; Kesavadas, C.; Rajan, J. Automatic detection and localization of focal cortical dysplasia lesions in MRI using fully convolutional neural network. Biomed. Signal Process. Control 2019, 52, 218–225. [Google Scholar]
- Wang, H.; Ahmed, S.N.; Mandal, M. Automated detection of focal cortical dysplasia using a deep convolutional neural network. Comput. Med. Imaging Graph. 2020, 79, 101662. [Google Scholar] [CrossRef] [PubMed]
- Feng, C.; Zhao, H.; Li, Y.; Wen, J. Automatic localization and segmentation of focal cortical dysplasia in FLAIR-negative patients using a convolutional neural network. J. Appl. Clin. Med. Phys. 2020, 21, 215–226. [Google Scholar] [CrossRef]
- Aliev, R.; Kondrateva, E.; Sharaev, M.; Bronov, O.; Marinets, A.; Subbotin, S.; Bernstein, A.; Burnaev, E. Convolutional Neural Networks for Automatic Detection of Focal Cortical Dysplasia. Adv. Intell. Syst. Comput. 2020, 1358, 582–588. [Google Scholar] [CrossRef]
- Thomas, E.; Pawan, S.J.; Kumar, S.; Horo, A.; Niyas, S.; Vinayagamani, S.; Kesavadas, C.; Rajan, J. Multi-Res-Attention UNet: A CNN Model for the Segmentation of Focal Cortical Dysplasia Lesions from Magnetic Resonance Images. IEEE J. Biomed. Health Inform. 2021, 25, 1724–1734. [Google Scholar] [CrossRef] [PubMed]
- Gill, R.S.; Lee, H.S.; Caldairou, B.; Choi, H.G.; Barba, C.; Deleo, F.; D’Incerti, L.; Coelho, V.F.N.; Lenge, M.; Semmelroch, M.; et al. Multicenter Validation of a Deep Learning Detection Algorithm for Focal Cortical Dysplasia. Neurology 2021, 97, e1571–e1582. [Google Scholar] [CrossRef]
- House, P.M.; Kopelyan, M.; Braniewska, N.; Silski, B.; Chudzinska, A.; Holst, B.; Sauvigny, T.; Martens, T.; Stodieck, S.; Pelzl, S. Automated detection and segmentation of focal cortical dysplasias (FCDs) with artificial intelligence: Presentation of a novel convolutional neural network and its prospective clinical validation. Epilepsy Res. 2021, 172, 106594. [Google Scholar] [CrossRef] [PubMed]
- Aminpour, A.; Ebrahimi, M.; Widjaja, E. Lesion Segmentation in Paediatric Epilepsy Utilizing Deep Learning Approaches. Adv. Artif. Intell. Mach. Learn. 2022, 2, 422–440. [Google Scholar] [CrossRef]
- Saini, J.; Singh, A.; Kesavadas, C.; Thomas, B.; Rathore, C.; Bahuleyan, B.; Radhakrishnan, A.; Radhakrishnan, K. Role of three-dimensional fluid-attenuated inversion recovery (3D FLAIR) and proton density magnetic resonance imaging for the detection and evaluation of lesion extent of focal cortical dysplasia in patients with refractory epilepsy. Acta Radiol. 2010, 51, 218–225. [Google Scholar] [CrossRef]
- Schmitter, D.; Roche, A.; Maréchal, B.; Ribes, D.; Abdulkadir, A.; Bach-Cuadra, M.; Daducci, A.; Granziera, C.; Klöppel, S.; Maeder, P.; et al. An evaluation of volume-based morphometry for prediction of mild cognitive impairment and Alzheimer’s disease. NeuroImage Clin. 2015, 7, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Friston, K.J.; Holmes, A.P.; Worsley, K.J.; Poline, J.-P.; Frith, C.D.; Frackowiak, R.S.J. Statistical parametric maps in functional imaging: A general linear approach. Hum. Brain Mapp. 1994, 2, 189–210. [Google Scholar] [CrossRef]
- Yousaf, T.; Dervenoulas, G.; Politis, M. Advances in MRI Methodology. Int. Rev. Neurobiol. 2018, 141, 31–76. [Google Scholar] [CrossRef]
- Ibtehaz, N.; Rahman, M.M. MultiResUNet: Rethinking the U-Net architecture for multimodal biomedical image segmentation. Neural Netw. 2020, 121, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Schlemper, J.; Oktay, O.; Schaap, M.; Heinrich, M.P.; Kainz, B.; Glocker, B.; Rueckert, D. Attention gated networks: Learning to leverage salient regions in medical images. Med. Image Anal. 2019, 53, 197–207. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Patients | Age Range | Sequence | Magnetic Field | Availability of the Dataset |
|---|---|---|---|---|---|
| [8] | 12 | 15 ± 8 | T1, T2, FLAIR | 1.5 T | — |
| [9] | 31 | range from 14 to 51 | T1 | 3 T | — |
| [11] | 30 | range from 1 to 46 | T1, FLAIR | 1.5 T | available upon request |
| [12] | 10 | range from 5 to 28 | — | — | — |
| [13] | 15 | — | T1, T2, FLAIR | — | — |
| [15] | 4 | 32 ± 13 | dMRI | 7 T | available upon request |
| [16] | 14 | — | T1 | 1.5 T | — |
| [17] | 29 | median 20 (IQR 13–29) | T1 | 1.5 T–3 T | — |
| [18] | 20 | range from 3 to 43 | T1 | 1.5 T | — |
| [19] | 33 | 10 ± 4 | T1, FLAIR | 3 T | — |
| [20,21] | 24 | 24 ± 8 | T1 | 1.5 T | — |
| [22] | 8 | — | T1 | 3 T | — |
| [23] | 15 | range from 15 to 53 | T1, T2, FLAIR | 3 T | — |
| [24] | 9 | range from 18 to 36 | T1 | 3 T | available upon request |
| [25] | 7 | range from 14 to 51 | T1 | 1.5 T | — |
| [26] | 8 | — | T1 | 3 T | — |
| [27] | 20 | range from 17 to 59 | T1, T2 | 3 T | — |
| [28] | 10 | — | T1 | 3 T | — |
| [29] | 16 | 26.4 ± 6.2 | T1 | 3 T | — |
| [30] | 10 | 36 ± 11 | T1 | 3 T | — |
| [31] | 6 | 32 ± 13 | FLAIR | 3 T | |
| [32] | 17 | range from 17 to 53 | T1 | 1.5 T–3 T | — |
| [33] | 25 | range from 17 to 59 | T1, T2 | 3 T | — |
| [34] | 70 | range from 18 to 60 | T1, T2 | 3 T | — |
| [35] | 39 | pediatric median 13 (IQR 13–14), adults median 37 (IQR 32–42) | T1 | 3 T | — |
| [36] | 104 | 32.3 ± 14.2 | T1, QPET | 1.5 T–3 T | — |
| [37] | 78 | 14.2 ± 4.5 | T1 | 1.5 T–3 T | — |
| [38] | 18 | 34 ± 2.5 | T1 | 1.5 T | — |
| [39,40] | 21 | — | T1 | — | — |
| [41] | 11 | range from 5 to 38 | T1, FLAIR | 3 T | — |
| [42] | 54 | range from 6.45 to 17.11 | T1 | 3 T | — |
| [43] | 7 | 33 ± 12 | FLAIR | 3 T | — |
| [44] | 41 | — | T1 | 1.5 T | — |
| [45] | 11 | — | T1 | 1.5 T | — |
| [46] | 28 | 26.5 ± 14.1 | T1 | 3 T | — |
| [47] | 41 | 27 ± 9 | T1, T2, FLAIR | 3 T | — |
| [48] | 22 | 14.68 ± 9.12 | T1 | 3 T | available upon request |
| [49] | 19 | 29 ± 8 | T1, T2 | 1.5 T–3 T | — |
| [50,51] | 10 | — | T1 | 3 T | — |
| [52] | 46 | 27.1 ± 8.6 | T1, FLAIR | 3 T | — |
| [53] | 62 | — | T1 | 3 T | — |
| [54] | 43 | 24 ± 10 | T1 | 1.5 T | — |
| [55,56] | 41 | 24.9 ± 10.9 | T1 | 1.5 T | — |
| [57] | 22 | 12.1 ± 3.9 | T1, FLAIR | 1.5 T | — |
| [58] | 40 | — | T1, FLAIR, PET | 3 T | — |
| [59] | 34 | range from 3.6 to 18.5 | T1, FLAIR | 3 T | — |
| [60] | 113 | 29.5 ± 13.6 | T1 | 1.5 T–3 T | available upon request |
| [61] | 107 | 27 ± 9 | T1, FLAIR | 1.5 T–3 T | — |
| [62] | 43 | — | FLAIR | 1.5 T–3 T | — |
| [63] | 10 | — | T1 | 1.5 T | — |
| [64] | 19 | 24 ± 10 | FLAIR | 1.5 T–3 T | — |
| [65] | 30 | — | — | 3 T | — |
| [66] | 26 | — | FLAIR | 3 T | — |
| [67] | 171 | range from 2 to 55 | T1, FLAIR | 1.5 T–3 T | available upon request |
| [68] | 201 | range from 8 to 68 | T1, FLAIR | 1.5 T–3 T | — |
| [69] | 80 | 11.5 ± 3.22 | T1, T2, FLAIR | 3 T | — |
| Study | Technique | Sensitivity % | Sequence | Patients | Controls | Age Group |
|---|---|---|---|---|---|---|
| [32] | SPM | 53 | T1 | 17 | 64 | Adult patients |
| [33] | SPM-5 | 88 | T2-FLAIR | 25 | 25 | Adult patients |
| [35] | SPM-12 | 92 | T1 | 39 | 105 | Adult patients/Pediatric patients |
| [36] | SPM-12 | 74 | T1 | 104 | N/A | Adult patients |
| [37] | SPM-12 | 56 | T1 | 78 | 370 | Pediatric patients |
| Study | Technique | Sensitivity % | Patients | Age Group |
|---|---|---|---|---|
| [38] | Two-stage Bayes | 85 | 18 | Adult patients |
| [39] | Naïve Bayes | 62.49 | 21 | Adult patients |
| [40] | Naïve Bayes + SVM | 88 | 21 | Adult patients |
| [41] | Naïve Bayes | 51 | 11 | Pediatric patients/Adult patients |
| [42] | Two-stage Bayes | 70 | 54 | Pediatric patients |
| [43] | Three-stage Bayes | 87.5 | 7 | Adult patients |
| Study | Technique | Sensitivity % | Sequence | Patients | Age Group |
|---|---|---|---|---|---|
| [40] | Naïve Bayes + SVM | 88 | T1 | 21 | Adult patients |
| [44] | SVM | 98 | T1 | 41 | Adult patients |
| [45] | OC-SVM | 77 | T1 | 11 (13 lesions) | Adult patients |
| [46] | SVM-Mat | 93 | T1, PET | 28 | Adult patients |
| Study | Technique | Sensitivity % | Sequence | Patients |
|---|---|---|---|---|
| [47] | Two-stage RUSBoost | 92 | T1, T2, FLAIR | 41 |
| [48] | XGBoost | 93 | T1, FLAIR, PET | 22 |
| Study | Detection Rate | Sensitivity % | Sequence | Patients | Controls | Age Group | ||
|---|---|---|---|---|---|---|---|---|
| Training | Testing | Training | Testing | |||||
| [61] | 35/40 | 61/67 | 87 | 91 | T1, FLAIR | 107 | 101 | Pediatric patients/Adult patients |
| [63] | - | 0.9 | - | 0.9 | T1 | 10 | 20 | — |
| [62] | 33/40 | - | 82.5 | - | FLAIR | 43 | - | — |
| [12] | - | - | 100 | 92.45 | T1 | 10 | 95 | Pediatric patients/Adult patients |
| [64] | - | 15/18 | - | 83.33 | FLAIR | 19 | - | Pediatric patients/Adult patients |
| [65] | - | 11/15 | - | 73.3 | - | 30 | 17 | — |
| [66] | - | - | - | 92 | FLAIR | 26 | - | — |
| [67] | 137/148 | 19/23 | 93 | 83 | T1, FLAIR | 171 | 131 | Pediatric patients/Adult patients |
| [68] | - | - | 70.1 | 77.8 | T1, FLAIR | 201 | 150 | Pediatric patients/Adult patients |
| [13] | - | - | - | 96.47 | - | 15 | - | — |
| [69] | 77/80 | 4/6 | 96 | 67 | T1, T2, FLAIR | 80 | 15 | Pediatric patients |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Murillo, D.; Castro-Ospina, A.E.; Duque-Muñoz, L.; Martínez-Vargas, J.D.; Suárez-Revelo, J.X.; Vélez-Arango, J.M.; de la Iglesia-Vayá, M. Automatic Detection of Focal Cortical Dysplasia Using MRI: A Systematic Review. Sensors 2023, 23, 7072. https://doi.org/10.3390/s23167072
Jiménez-Murillo D, Castro-Ospina AE, Duque-Muñoz L, Martínez-Vargas JD, Suárez-Revelo JX, Vélez-Arango JM, de la Iglesia-Vayá M. Automatic Detection of Focal Cortical Dysplasia Using MRI: A Systematic Review. Sensors. 2023; 23(16):7072. https://doi.org/10.3390/s23167072
Chicago/Turabian StyleJiménez-Murillo, David, Andrés Eduardo Castro-Ospina, Leonardo Duque-Muñoz, Juan David Martínez-Vargas, Jazmín Ximena Suárez-Revelo, Jorge Mario Vélez-Arango, and Maria de la Iglesia-Vayá. 2023. "Automatic Detection of Focal Cortical Dysplasia Using MRI: A Systematic Review" Sensors 23, no. 16: 7072. https://doi.org/10.3390/s23167072