
Monitoring of Cardiorespiratory Parameters during Sleep Using a Special Holder for the Accelerometer Sensor

 ,
,  , , , ,
, , , ,  ,
,  and
and 
Abstract
:1. Introduction
- How can we use mechanical oscillations from the subject in cardiorespiratory measurements?
2. Materials and Methods
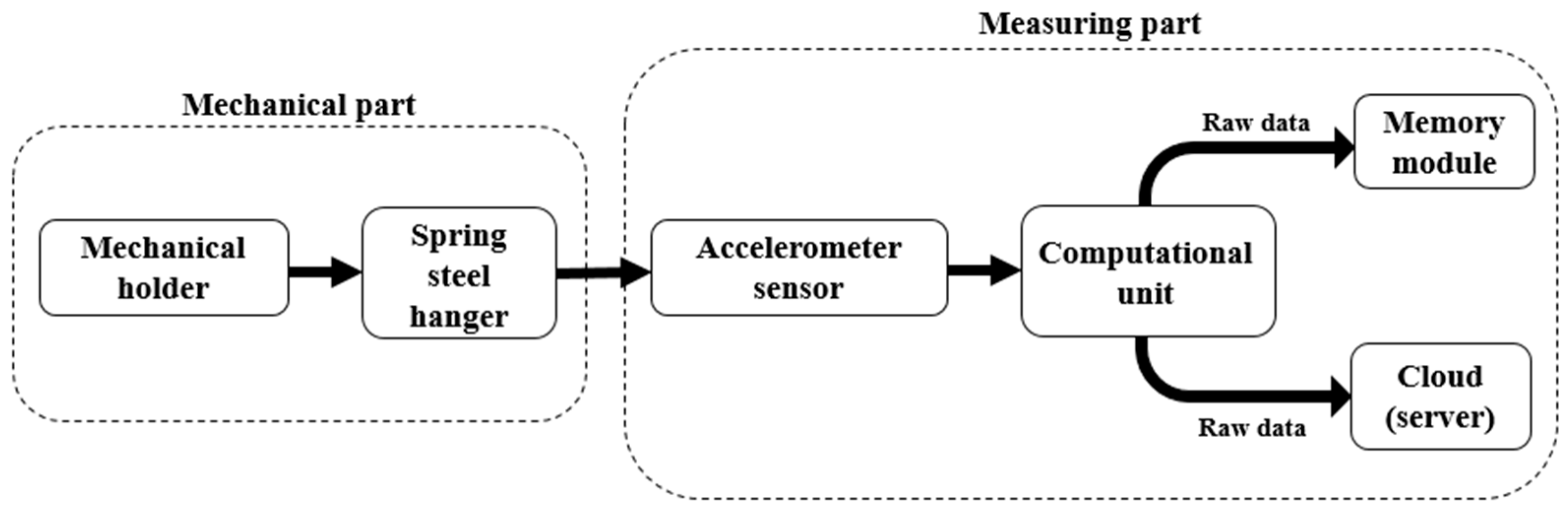
2.1. Mechanical Holder
2.2. Data Acquisition
2.3. Signal Processing and Analysis
2.3.1. HR Estimation Algorithm
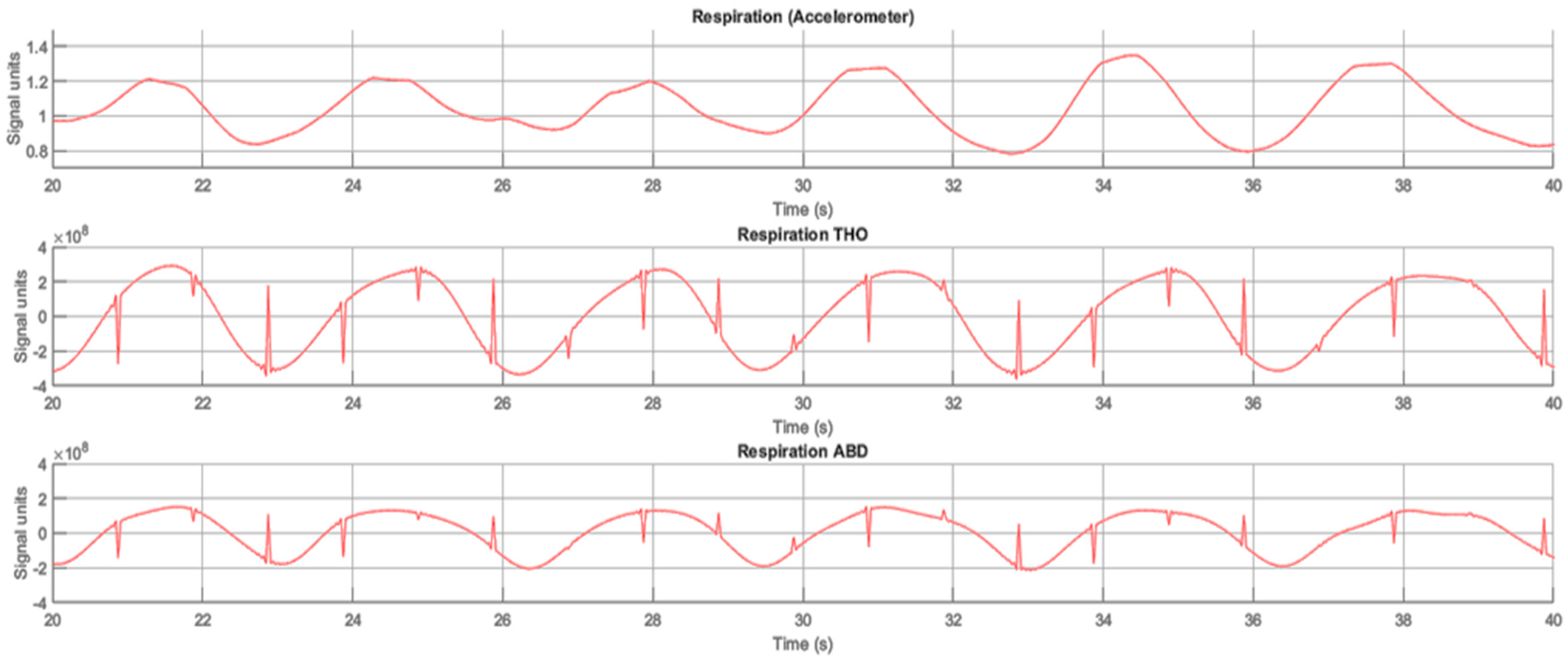
2.3.2. RR Estimation Algorithm
2.4. Experiment Design
3. Results
3.1. Subjects’ Statistical Data
3.2. Heart Rate Monitoring
3.3. Respiratory Rate Monitoring
4. Discussion
4.1. Remaining Challenges
4.2. Enhancements, Applications and Features
- Keeping the environment isolated from sound pollutants (a possible reason for different oscillations);
- Air conditions such as temperature, humidity and pressure by continuously measuring and monitoring these parameters;
- Conducting experiments at fixed times of the day with some tolerance;
- Leaving the bed unoccupied for some time (duration is up to 10–15 min) to restore the potential drift of the sensors to the initial states from previous experiments (influenced by the weight, force and surface of objects).
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Worley, S.L. The Extraordinary Importance of Sleep: The Detrimental Effects of Inadequate Sleep on Health and Public Safety Drive an Explosion of Sleep Research. PT Peer-Rev. J. Formul. Manag. 2018, 43, 758–763. [Google Scholar]
- Grandner, M.A. Sleep, Health, and Society. Sleep Med. Clin. 2017, 12, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Wu, W.; Li, S. Design and Implementation of an IoT-Based Indoor Air Quality Detector with Multiple Communication Interfaces. IEEE Internet Things J. 2019, 6, 9621–9632. [Google Scholar] [CrossRef]
- Inan, O.T.; Migeotte, P.-F.; Park, K.-S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.; Tank, J.; Funtova, I.; Prisk, G.K.; et al. Ballistocardiography and Seismocardiography: A Review of Recent Advances. IEEE J. Biomed. Health Inform. 2015, 19, 1414–1427. [Google Scholar] [CrossRef] [Green Version]
- Stamatakis, E.; Rezende LFM de Rey-López, J.P. Sedentary Behaviour and Cardiovascular Disease. In Sedentary Behaviour Epidemiology; Leitzmann, M.F., Jochem, C., Schmid, D., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 215–243. [Google Scholar] [CrossRef]
- Caples, S.M.; Anderson, W.M.; Calero, K.; Howell, M.; Hashmi, S.D. Use of Polysomnography and Home Sleep Apnea Tests for the Longitudinal Management of Obstructive Sleep Apnea in Adults: An American Academy of Sleep Medicine Clinical Guidance Statement. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2021, 17, 1287–1293. [Google Scholar] [CrossRef]
- Berry, R.B.; Albertario, C.L.; Harding, S.M.; Lloyd, R.M.; Plante, D.T.; Quan, S.F.; Troester, M.T.; Vaughn, B.V. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; American Academy of Sleep Medicine: Darien, IL, USA, 2018. [Google Scholar]
- Asadov, A.; Seepold, R.; Martínez Madrid, N.; Ortega, J.A. Non-invasive Cardiorespiration Monitoring Using Force Resistive Sensor. In Hardware and Software Supporting Physiological Measurement (HSPM-2022); Hochschule Reutlingen: Reutlingen, Germany, 2022; pp. 20–22. [Google Scholar] [CrossRef]
- Moridian, P.; Shoeibi, A.; Khodatars, M.; Jafari, M.; Pachori, R.B.; Khadem, A.; Alizadehsani, R.; Ling, S.H. Automatic Diagnosis of Sleep Apnea from Biomedical Signals Using Artificial Intelligence Techniques: Methods, Challenges, and Future Works. WIREs Data Min. Knowl. Discov. 2022, 12, e1478. [Google Scholar] [CrossRef]
- Hussain, Z.; Sheng, Q.Z.; Zhang, W.E.; Ortiz, J.; Pouriyeh, S. Non-Invasive Techniques for Monitoring Different Aspects of Sleep: A Comprehensive Review. ACM Trans. Comput. Healthc. 2022, 3, 1–26. [Google Scholar] [CrossRef]
- Jakkaew, P.; Onoye, T. Non-Contact Respiration Monitoring and Body Movements Detection for Sleep Using Thermal Imaging. Sensors 2020, 20, 6307. [Google Scholar] [CrossRef] [PubMed]
- Fino, E.; Plazzi, G.; Filardi, M.; Marzocchi, M.; Pizza, F.; Vandi, S.; Mazzetti, M. (Not so) Smart Sleep Tracking through the Phone: Findings from a Polysomnography Study Testing the Reliability of Four Sleep Applications. J. Sleep Res. 2020, 29, e12935. [Google Scholar] [CrossRef]
- Shkilniuk, Y.; Gaiduk, M.; Seepold, R. Unobtrusive Accelerometer-Based Heart Rate Detection. In Applications in Electronics Pervading Industry, Environment and Society; Saponara, S., de Gloria, A., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 49–54. [Google Scholar] [CrossRef]
- Bruser, C.; Stadlthanner, K.; de Waele, S.; Leonhardt, S. Adaptive Beat-to-Beat Heart Rate Estimation in Ballistocardiograms. IEEE Trans. Inf. Technol. Biomed. 2011, 15, 778–786. [Google Scholar] [CrossRef] [Green Version]
- Albukhari, A.; Lima, F.; Mescheder, U. Bed-Embedded Heart and Respiration Rates Detection by Longitudinal Ballistocardiography and Pattern Recognition. Sensors 2019, 19, 1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadek, I.; Biswas, J. Nonintrusive Heart Rate Measurement Using Ballistocardiogram Signals: A Comparative Study. Signal Image Video Process. 2019, 13, 475–482. [Google Scholar] [CrossRef]
- Jiao, C.; Su, B.-Y.; Lyons, P.; Zare, A.; Ho, K.C.; Skubic, M. Multiple Instance Dictionary Learning for Beat-to-Beat Heart Rate Monitoring From Ballistocardiograms. IEEE Trans. Biomed. Eng. 2018, 65, 2634–2648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, A.R.; Boger, J. Zero-Effort Ambient Heart Rate Monitoring Using Ballistocardiography Detected Through a Seat Cushion: Prototype Development and Preliminary Study. JMIR Rehabil. Assist. Technol. 2021, 8, e25996. [Google Scholar] [CrossRef]
- Xu, W.; Yu, C.; Dong, B.; Wang, Y.; Zhao, W. Thin Piezoelectric Sheet Assisted PGC Demodulation of Fiber-Optic Integrated MZI and its Application in Under Mattress Vital Signs Monitoring. IEEE Sens. J. 2022, 22, 2151–2159. [Google Scholar] [CrossRef]
- Gomez-Clapers, J.; Serra-Rocamora, A.; Casanella, R.; Pallas-Areny, R. Towards the Standardization of Ballistocardiography Systems for J-peak Timing Measurement. Measurement 2014, 58, 310–316. [Google Scholar] [CrossRef] [Green Version]
- Gaiduk, M.; Seepold, R.; Martínez Madrid, N.; Orcioni, S.; Conti, M. Recognizing Breathing Rate and Movement While Sleeping in Home Environment. In Applications in Electronics Pervading Industry, Environment and Society; Saponara, S., de Gloria, A., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 333–339. [Google Scholar] [CrossRef]
- D’Mello, Y.; Skoric, J.; Xu, S.; Roche, P.J.R.; Lortie, M.; Gagnon, S.; Plant, D.V. Real-Time Cardiac Beat Detection and Heart Rate Monitoring from Combined Seismocardiography and Gyrocardiography. Sensors 2019, 19, 3472. [Google Scholar] [CrossRef] [Green Version]
- Romano, C.; Schena, E.; Formica, D.; Massaroni, C. Comparison between Chest-Worn Accelerometer and Gyroscope Performance for Heart Rate and Respiratory Rate Monitoring. Biosensors 2022, 12, 834. [Google Scholar] [CrossRef]
- Hersek, S.; Semiz, B.; Shandhi, M.M.H.; Orlandic, L.; Inan, O.T. A Globalized Model for Mapping Wearable Seismocardiogram Signals to Whole-Body Ballistocardiogram Signals Based on Deep Learning. IEEE J. Biomed. Health Inform. 2020, 24, 1296–1309. [Google Scholar] [CrossRef]
- Skoric, J.; D’Mello, Y.; Aboulezz, E.; Hakim, S.; Clairmonte, N.; Lortie, M.A.; Plant, D.V. Respiratory Modulation of Sternal Motion in the Context of Seismocardiography. IEEE Sens. J. 2022, 22, 13055–13066. [Google Scholar] [CrossRef]
- Boiko, A.; Scherz, W.D.; Gaiduk, M.; Gentili, A.; Conti, M.; Orcioni, S.; Seepold, R.; Martínez Madrid, N. Sleep Respiration Rate Detection Using an Accelerometer Sensor with Special Holder Setup. In Proceedings of the 2022 E-Health and Bioengineering Conference (EHB), Iasi, Romania, 17–18 November 2022; pp. 1–4. [Google Scholar] [CrossRef]
- Boiko, A.; Martínez Madrid, N.; Seepold, R. Determination of Accelerometer Sensor Position for Respiration Rate Detection: Initial Research. In Hardware and Software Supporting Physiological Measurement (HSPM-2022); Hochschule Reutlingen: Reutlingen, Germany, 2022; pp. 16–19. [Google Scholar] [CrossRef]
- Gaiduk, M.; Wehrle, D.; Seepold, R.; Ortega, J.A. Non-obtrusive System for Overnight Respiration and Heartbeat Tracking. Procedia Comput. Sci. 2020, 176, 2746–2755. [Google Scholar] [CrossRef]
- Haghi, M.; Asadov, A.; Boiko, A.; Ortega, J.A.; Martínez Madrid, N.; Seepold, R. Validating Force Sensitive Resistor Strip Sensors for Cardiorespiratory Measurement during Sleep: A Preliminary Study. Sensors 2023, 23, 3973. [Google Scholar] [CrossRef] [PubMed]
- Conti, M.; Aironi, C.; Orcioni, S.; Seepold, R.; Gaiduk, M.; Martínez Madrid, N. Heart Rate Detection with Accelerometric Sensors under the Mattress. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 4063–4066. [Google Scholar] [CrossRef]
- Mora, N.; Cocconcelli, F.; Matrella, G.; Ciampolini, P. Accurate Heartbeat Detection on Ballistocardiogram Accelerometric Traces. IEEE Trans. Instrum. Meas. 2020, 69, 9000–9009. [Google Scholar] [CrossRef]
- Ashouri, H.; Hersek, S.; Inan, O.T. Universal Pre-Ejection Period Estimation Using Seismocardiography: Quantifying the Effects of Sensor Placement and Regression Algorithms. IEEE Sens. J. 2018, 18, 1665–1674. [Google Scholar] [CrossRef] [PubMed]
- Floris, C.; Solbiati, S.; Landreani, F.; Damato, G.; Lenzi, B.; Megale, V.; Caiani, E.G. Feasibility of Heart Rate and Respiratory Rate Estimation by Inertial Sensors Embedded in a Virtual Reality Headset. Sensors 2020, 20, 7168. [Google Scholar] [CrossRef]
- Higashino, M.; Miyata, K.; Kudo, K. Coordination Dynamics of Thoracic and Abdominal Movements during Voluntary Breathing. Sci. Rep. 2022, 12, 13266. [Google Scholar] [CrossRef]
- Ullal, A.; Su, B.Y.; Enayati, M.; Skubic, M.; Despins, L.; Popescu, M.; Keller, J. Non-invasive Monitoring of Vital Signs for Older Adults using Recliner Chairs. Health Technol. 2021, 11, 169–184. [Google Scholar] [CrossRef]
- Watanabe, S.; Murozaki, Y.; Sugiura, H.; Sato, Y.; Honbe, K.; Arai, F. Non-invasive Biosignals Detection for Continuous Monitoring of a Neonate using Quartz Crystal Resonator. Sens. Actuators A Phys. 2021, 317, 112475. [Google Scholar] [CrossRef]
- Lokavee, S.; Tantrakul, V.; Pengjiam, J.; Kerdcharoen, T. A Sleep Monitoring System Using Force Sensor and an Accelerometer Sensor for Screening Sleep Apnea. In Proceedings of the 2021 13th International Conference on Knowledge and Smart Technology (KST), Bangsaen, Chonburi, Thailand, 21–24 January 2021; pp. 208–213. [Google Scholar] [CrossRef]
- Fekedulegn, D.; Andrew, M.E.; Shi, M.; Violanti, J.M.; Knox, S.; Innes, K.E. Actigraphy-Based Assessment of Sleep Parameters. Ann. Work Expo. Health 2020, 64, 350–367. [Google Scholar] [CrossRef] [Green Version]
- Da Estrela, C.; McGrath, J.; Booij, L.; Gouin, J.-P. Heart Rate Variability, Sleep Quality, and Depression in the Context of Chronic Stress. Ann. Behav. Med. 2020, 55, 155–164. [Google Scholar] [CrossRef]
- Scott, H.; Lack, L.; Lovato, N. A Systematic Review of the Accuracy of Sleep Wearable Devices for Estimating Sleep Onset. Sleep Med. Rev. 2020, 49, 101227. [Google Scholar] [CrossRef] [PubMed]
- Gaiduk, M.; Perea Rodríguez, J.J.; Seepold, R.; Martínez Madrid, N.; Penzel, T.; Glos, M.; Ortega, J.A. Estimation of Sleep Stages Analyzing Respiratory and Movement Signals. IEEE J. Biomed. Health Inform. 2022, 26, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Andreozzi, E.; Fratini, A.; Esposito, D.; Naik, G.; Polley, C.; Gargiulo, G.D.; Bifulco, P. Forcecardiography: A Novel Technique to Measure Heart Mechanical Vibrations onto the Chest Wall. Sensors 2020, 20, 3885. [Google Scholar] [CrossRef] [PubMed]
- Andreozzi, E.; Centracchio, J.; Punzo, V.; Esposito, D.; Polley, C.; Gargiulo, G.D.; Bifulco, P. Respiration Monitoring via Forcecardiography Sensors. Sensors 2021, 21, 3996. [Google Scholar] [CrossRef] [PubMed]
- Pan, Q.; Brulin, D.; Campo, E. Current Status and Future Challenges of Sleep Monitoring Systems: Systematic Review. JMIR Biomed. Eng. 2020, 5, e20921. [Google Scholar] [CrossRef]
- Chen, Q.; Jiang, X.; Liu, X.; Lu, C.; Wang, L.; Chen, W. Non-Contact Heart Rate Monitoring in Neonatal Intensive Care Unit using RGB Camera. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 5822–5825. [Google Scholar] [CrossRef]
- Villarroel, M.; Jorge, J.; Meredith, D.; Sutherland, S.; Pugh, C.; Tarassenko, L. Non-contact Vital-sign Monitoring of Patients Undergoing Haemodialysis Treatment. Sci. Rep. 2020, 10, 18529. [Google Scholar] [CrossRef]
- Han, P.; Li, L.; Zhang, H.; Guan, L.; Marques, C.; Savović, S.; Ortega, B.; Min, R.; Li, X. Low-cost Plastic Optical Fiber Sensor Embedded in Mattress for Sleep Performance Monitoring. Opt. Fiber Technol. 2021, 64, 102541. [Google Scholar] [CrossRef]
- Sadek, I.; Heng, T.T.S.; Seet, E.; Abdulrazak, B. A New Approach for Detecting Sleep Apnea Using a Contactless Bed Sensor: Comparison Study. J. Med. Internet Res. 2020, 22, e18297. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Gender | Age (Years) | Height (cm) | Weight (kg) |
|---|---|---|---|---|
| 1 | Male | 26 | 179 | 72 |
| 2 | Male | 25 | 181 | 74 |
| 3 | Male | 40 | 170 | 65 |
| 4 | Female | 25 | 168 | 67 |
| 5 | Female | 37 | 160 | 52 |
| 6 | Male | 36 | 171 | 80 |
| 7 | Female | 33 | 167 | 73 |
| 8 | Male | 31 | 177 | 70 |
| 9 | Female | 24 | 155 | 50 |
| 10 | Female | 43 | 178 | 78 |
| 11 | Male | 23 | 179 | 65 |
| 12 | Male | 34 | 184 | 75 |
| 13 | Male | 34 | 180 | 67 |
| 14 | Male | 28 | 179 | 88 |
| 15 | Female | 23 | 175 | 62 |
| 16 | Male | 53 | 176 | 82 |
| 17 | Female | 24 | 171 | 87 |
| 18 | Female | 19 | 169 | 69 |
| 19 | Female | 27 | 150 | 60 |
| 20 | Male | 54 | 188 | 85 |
| 21 | Female | 25 | 166 | 60 |
| 22 | Male | 32 | 179 | 130 |
| 23 | Male | 27 | 178 | 72 |
| Subject Position | Sensor Position | |||
|---|---|---|---|---|
| S1 | S2 | S3 | S4 | |
| Prone (P1) | 2.15 | 2.34 | 2.75 | 2.51 |
| Right lateral (P2) | 2.13 | 2.37 | 3.12 | 3.37 |
| Supine (P3) | 2.29 | 2.92 | 2.80 | 3.40 |
| Left lateral (P4) | 2.40 | 2.58 | 3.00 | 3.21 |
| Average | 2.24 | 2.53 | 2.92 | 3.12 |
| Subject Position | Sensor Position | |||||||
|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S4 | |||||
| Males | Females | Males | Females | Males | Females | Males | Females | |
| Prone (P1) | 2.14 | 2.18 | 2.29 | 2.39 | 2.33 | 3.29 | 2.49 | 2.53 |
| Right lateral (P2) | 2.20 | 2.04 | 2.28 | 2.49 | 2.77 | 3.61 | 3.14 | 3.65 |
| Supine (P3) | 2.33 | 2.24 | 2.92 | 2.65 | 3.05 | 2.49 | 3.20 | 3.67 |
| Left lateral (P4) | 2.47 | 2.31 | 2.43 | 2.78 | 2.77 | 3.27 | 3.35 | 3.04 |
| Average | 2.28 | 2.19 | 2.50 | 2.57 | 2.70 | 3.19 | 3.06 | 3.21 |
| Subject Position | Sensor Position | |||||||
|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S4 | |||||
| THO | ABD | THO | ABD | THO | ABD | THO | ABD | |
| Prone (P1) | 1.19 | 1.04 | 1.48 | 1.36 | 1.49 | 1.30 | 2.18 | 1.91 |
| Right lateral (P2) | 1.68 | 1.41 | 1.61 | 1.33 | 1.72 | 1.48 | 1.79 | 1.62 |
| Supine (P3) | 1.62 | 1.37 | 1.65 | 1.48 | 1.88 | 1.63 | 1.92 | 1.84 |
| Left lateral (P4) | 1.57 | 1.42 | 1.95 | 1.72 | 1.66 | 1.61 | 1.99 | 1.69 |
| Average | 1.51 | 1.31 | 1.67 | 1.47 | 1.69 | 1.50 | 1.97 | 1.77 |
| Subject Position | Sensor Position | |||||||
|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S4 | |||||
| Males | Females | Males | Females | Males | Females | Males | Females | |
| Prone (P1) | 1.05 | 1.02 | 1.29 | 1.18 | 1.44 | 1.31 | 1.91 | 1.95 |
| Right lateral (P2) | 1.16 | 1.37 | 1.06 | 1.27 | 1.43 | 1.50 | 1.44 | 1.26 |
| Supine (P3) | 1.26 | 1.32 | 1.40 | 1.42 | 1.62 | 1.79 | 1.70 | 1.81 |
| Left lateral (P4) | 1.36 | 1.51 | 1.55 | 1.77 | 1.67 | 1.55 | 1.42 | 1.50 |
| Average | 1.21 | 1.30 | 1.32 | 1.41 | 1.54 | 1.54 | 1.62 | 1.63 |
| Subject Position | Sensor Position | |||||||
|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S4 | |||||
| Males | Females | Males | Females | Males | Females | Males | Females | |
| Prone (P1) | 1.03 | 1.05 | 1.41 | 1.45 | 1.20 | 1.35 | 1.91 | 2.10 |
| Right lateral (P2) | 1.61 | 1.65 | 1.54 | 1.60 | 1.52 | 1.63 | 1.77 | 1.94 |
| Supine (P3) | 1.46 | 1.59 | 1.54 | 1.57 | 1.63 | 1.67 | 1.94 | 1.74 |
| Left lateral (P4) | 1.46 | 1.36 | 1.85 | 1.82 | 1.57 | 1.48 | 1.90 | 2.09 |
| Average | 1.39 | 1.41 | 1.59 | 1.61 | 1.48 | 1.53 | 1.88 | 1.97 |
| Number of Subjects | Sensor Type | Reliability | Unobtrusiveness | ||||
|---|---|---|---|---|---|---|---|
| HR MAE, bpm | RR MAE, rpm | HR MAPE, % | RR MAPE, % | Yes or No | |||
| [45] | 5 | Camera | 7.40 | - | 12.46 | - | No |
| [46] | 40 | Camera | 2.80 | 2.10 | - | - | No |
| [47] | 10 | Fiber optic | 2.00 | 1.00 | - | - | Yes |
| [48] | 10 | Fiber optic | - | - | 5.41 | 11.60 | Yes |
| [29] | 20 | FSR | 3.24 | 2.32 | - | - | Yes |
| [35] | 45 | ACC | 10.10 | 1.76 | 3.60 | 6.25 | Yes |
| This work | 23 | ACC | 2.24 | 1.52 | - | - | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boiko, A.; Gaiduk, M.; Scherz, W.D.; Gentili, A.; Conti, M.; Orcioni, S.; Martínez Madrid, N.; Seepold, R. Monitoring of Cardiorespiratory Parameters during Sleep Using a Special Holder for the Accelerometer Sensor. Sensors 2023, 23, 5351. https://doi.org/10.3390/s23115351
Boiko A, Gaiduk M, Scherz WD, Gentili A, Conti M, Orcioni S, Martínez Madrid N, Seepold R. Monitoring of Cardiorespiratory Parameters during Sleep Using a Special Holder for the Accelerometer Sensor. Sensors. 2023; 23(11):5351. https://doi.org/10.3390/s23115351
Chicago/Turabian StyleBoiko, Andrei, Maksym Gaiduk, Wilhelm Daniel Scherz, Andrea Gentili, Massimo Conti, Simone Orcioni, Natividad Martínez Madrid, and Ralf Seepold. 2023. "Monitoring of Cardiorespiratory Parameters during Sleep Using a Special Holder for the Accelerometer Sensor" Sensors 23, no. 11: 5351. https://doi.org/10.3390/s23115351