
RBEF: Ransomware Efficient Public Blockchain Framework for Digital Healthcare Application


Abstract
:1. Introduction
Motivation and Methodology
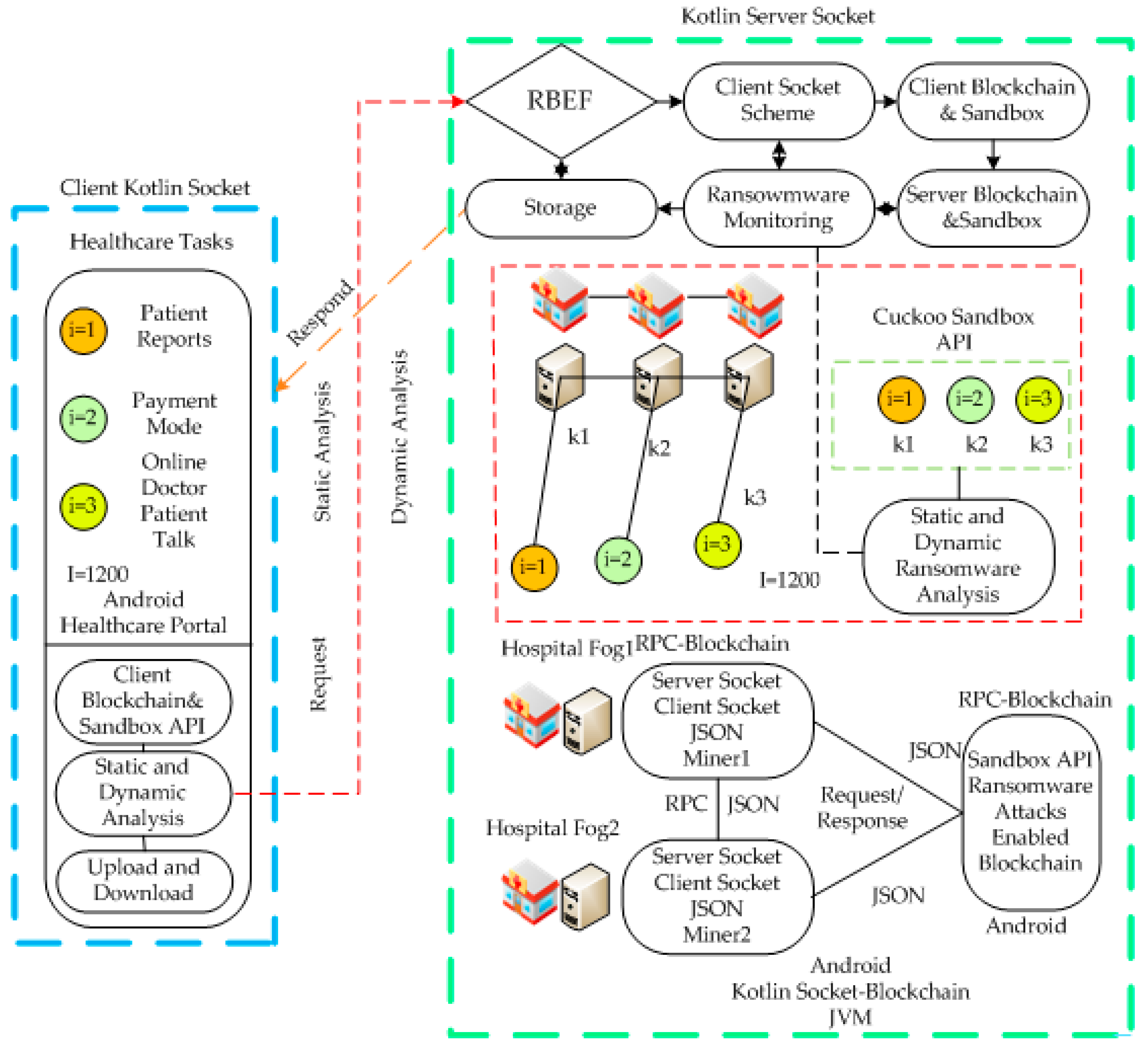
- This paper introduces the RBEF blockchain simulator, which was developed using Android and Kotlin languages, with the aim of incorporating hospitals, wireless, and other healthcare services into the framework for execution;
- The RBEF simulator consists of static, dynamic and blockchain validation schemes. All nodes (e.g., mobile, wireless network, fog and cloud computing) perform blockchain hashing, and smart-contract rules validate all transactions against ransomware attacks and their encryption within the framework;
- A mathematical model is presented for the problem under consideration, based on different constraints such as delay, security, and resources required for processing blockchain validation against malware in healthcare applications;
- We implemented the cuckoo sandbox static and dynamic data sampling schemes to validate the blockchain transaction among nodes. We handle both static and dynamic ransomware attacks based on the pattern of transactions among nodes.
2. Related Work
3. Proposed Architecture
Problem Formulation
4. Proposed Algorithm Methodology
| Algorithm 1: RBEF |
| Input: M, I, K, B, BC, Ransomware-Trained [List] Output: Minimized T,Cost. For (I = 1 to I) For (k = 1 to K) Call Algorithm 2 to process the local healthcare tasks based on blockchain sandbox scheme Call Algorithm 3 to process the fog cloud healthcare tasks based on blockchain sandbox scheme End Main Assignment End Main Loop |
| Algorithm 2: Client Blockchain Sandbox Scheme |
| Input: M, I, B, BC, Ransomware-Trained [List] Output: Minimized T. Sandbox Sampling Trained [List] For (I = 1 to I) Determined assignment the local execution delay based on Equations (1)–(3) and (8) Determined the local blockchain at mobile wallet blockchain validation based on Equation (4) Apply the Static Analysis If (m~i~bc1~Ransomware-Trained [List]! = success) { Apply the blockchain hashing AES-256 to workload i based on Equations (5)–(7) All transactions must have blockchain pattern (Random hashing and time) } If (b1~i~bc2~m1~Ransomware-Trained [List] = success) { Call Dynamic Analysis Determined the pattern~b1~i~bc1~Ransomware-Trained [List] Repeat Until ~Ransomware-Trained [List]! = success Matched the pervious hash b1~i~bc1~Ransomware-Trained [List] = success Apply the blockchain hashing AES-256 to workload i All transactions must have blockchain pattern } End Main Assignment End Main Loop |
| Algorithm 3: Server Blockchain Sandbox Scheme |
| Input: M, K, B, BC, Ransomware-Trained [List] Output: Minimized T. Sandbox Sampling Trained [List] For (k = 1 to K) Determined assignment the fog cloud execution delay based on Equation (10) Apply the Static Analysis If (m~i~bc1~Ransomware-Trained [List]! = success) { Apply the blockchain hashing AES-256 to workload i All transactions must have blockchain pattern (Random hashing and time) } If (k1~i~bc2~k2~Ransomware-Trained [List]! = success) { Matched the pervious hash k1~i~k2~Ransomware-Trained [List]! = success Apply the blockchain hashing AES-256 to workload i All transactions must have blockchain pattern Determine the cost based on Equations (12) and (13) } If (k2~i~bc2~k3~Ransomware-Trained [List] = success) { Call Dynamic Analysis Determined the pattern~k2~i~k3~Ransomware-Trained [List] Repeat Until ~Ransomware-Trained [List]! = success Matched the pervious hash k2~i~k3~Ransomware-Trained [List] = success Apply the blockchain hashing AES-256 to workload i All transactions must have blockchain pattern } End Main Assignment End Main Loop |
5. Performance Evaluation and Implementation
RBEF Implemented Simulator
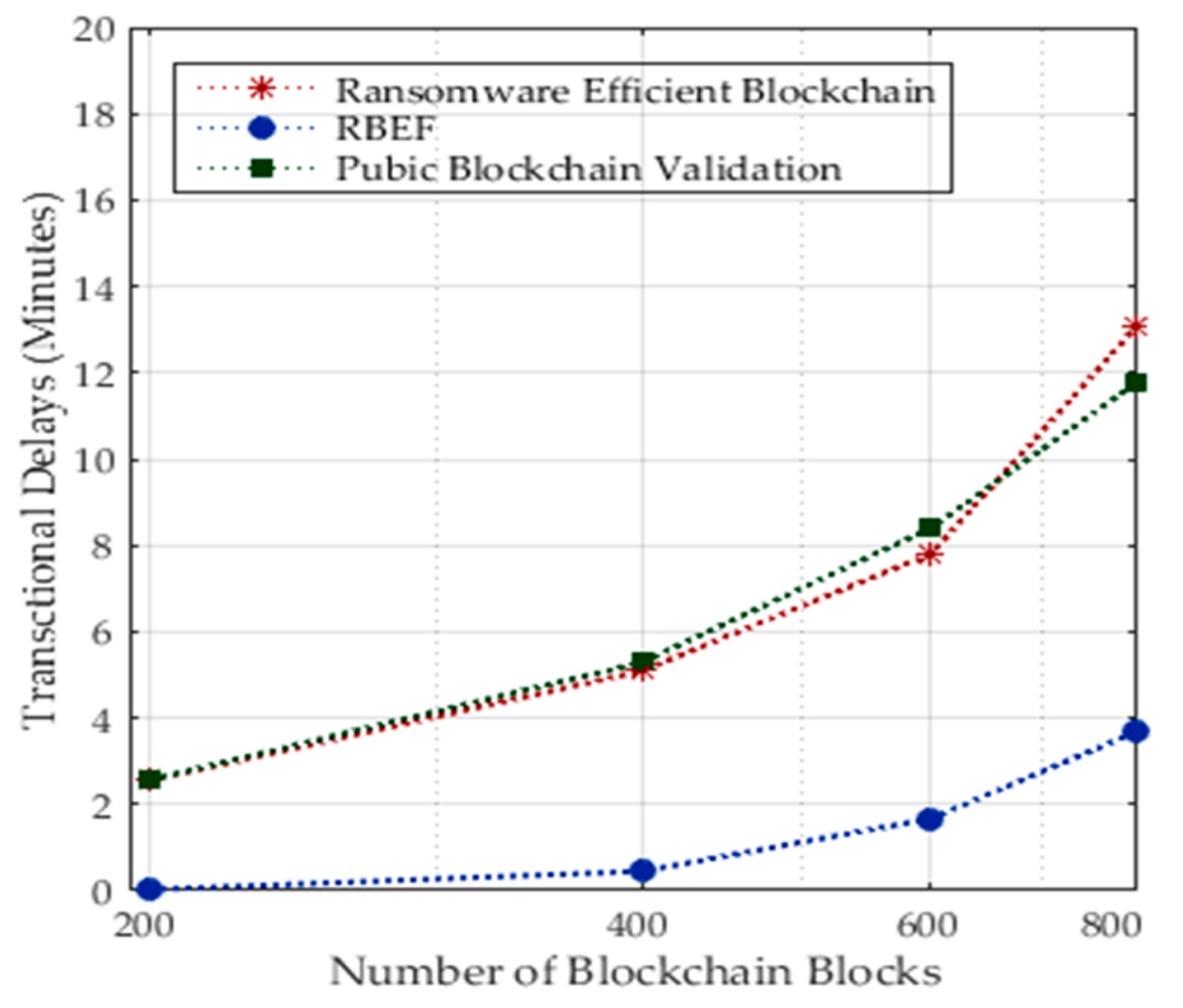
6. Results and Discussion
6.1. Results and Discussion of Performance on Dynamic Analysis of Ransomware Attacks
6.2. Results and Discussion of Performance on Dynamic Analysis of Ransomware Attacks
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antwi, M.; Adnane, A.; Ahmad, F.; Hussain, R.; ur Rehman, M.H.; Kerrache, C.A. The case of HyperLedger Fabric as a blockchain solution for healthcare applications. Blockchain Res. Appl. 2021, 2, 100012. [Google Scholar] [CrossRef]
- Wazid, M.; Das, A.K.; Shetty, S. BSFR-SH: Blockchain-Enabled Security Framework Against Ransomware Attacks for Smart Healthcare. IEEE Trans. Consum. Electron. 2022, 69, 18–28. [Google Scholar] [CrossRef]
- Kumar, S.; Bharti, A.K.; Amin, R. Decentralized secure storage of medical records using Blockchain and IPFS: A comparative analysis with future directions. Secur. Priv. 2021, 4, e162. [Google Scholar] [CrossRef]
- Shaen, C.; Goodell, J.W. The reputational contagion effects of ransomware attacks. Financ. Res. Lett. 2022, 47, 102715. [Google Scholar]
- Almashhadani, A.O.; Kaiiali, M.; Sezer, S.; O’Kane, P. A Multi-Classifier Network-Based Crypto Ransomware Detection System: A Case Study of Locky Ransomware. IEEE Access 2019, 7, 47053–47067. [Google Scholar] [CrossRef]
- Kumar, A.; Singh, A.K.; Ahmad, I.; Singh, P.K.; Anushree; Verma, P.K.; Alissa, K.A.; Bajaj, M.; Rehman, A.U.; Tag-Eldin, E. A Novel Decentralized Blockchain Architecture for the Preservation of Privacy and Data Security against Cyberattacks in Healthcare. Sensors 2022, 22, 5921. [Google Scholar] [CrossRef]
- Ramzan, S.; Aqdus, A.; Ravi, V.; Koundal, D.; Amin, R.; Al Ghamdi, M.A. Healthcare Applications Using Blockchain Technology: Motivations and Challenges. IEEE Trans. Eng. Manag. 2022, 1–17. [Google Scholar] [CrossRef]
- Gohar, A.N.; Abdelmawgoud, S.A.; Farhan, M.S. A Patient-Centric Healthcare Framework Reference Architecture for Better Semantic Interoperability Based on Blockchain, Cloud, and IoT. IEEE Access 2022, 10, 92137–92157. [Google Scholar] [CrossRef]
- Govindan, K.; Nasr, A.K.; Heidary, M.S.; Nosrati-Abarghooee, S.; Mina, H. Prioritizing adoption barriers of platforms based on blockchain technology from balanced scorecard perspectives in healthcare industry: A structural approach. Int. J. Prod. Res. 2022, 61, 3512–3526. [Google Scholar] [CrossRef]
- Ch, R.; Srivastava, G.; Nagasree, Y.L.V.; Ponugumati, A.; Ramachandran, S. Robust Cyber-Physical System Enabled Smart Healthcare Unit Using Blockchain Technology. Electronics 2022, 11, 3070. [Google Scholar] [CrossRef]
- Sangal, S.; Nigam, A.; Bhutani, C. Conceptualizing the role of blockchain in omnichannel healthcare: A Delphi study. Aslib J. Inf. Manag. 2022, 74, 782–800. [Google Scholar] [CrossRef]
- Zhang, G.; Yang, Z.; Liu, W. Blockchain-based privacy preserving e-health system for healthcare data in cloud. Comput. Netw. 2022, 203, 108586. [Google Scholar] [CrossRef]
- Zulkifl, Z.; Khan, F.; Tahir, S.; Afzal, M.; Iqbal, W.; Rehman, A.; Saeed, S.; Almuhaideb, A.M. FBASHI: Fuzzy and Blockchain-Based Adaptive Security for Healthcare IoTs. IEEE Access 2022, 10, 15644–15656. [Google Scholar] [CrossRef]
- Azbeg, K.; Ouchetto, O.; Andaloussi, S.J. BlockMedCare: A healthcare system based on IoT, Blockchain and IPFS for data management security. Egypt. Inform. J. 2022, 23, 329–343. [Google Scholar] [CrossRef]
- Pelekoudas-Oikonomou, F.; Zachos, G.; Papaioannou, M.; de Ree, M.; Ribeiro, J.C.; Mantas, G.; Rodriguez, J. Blockchain-Based Security Mechanisms for IoMT Edge Networks in IoMT-Based Healthcare Monitoring Systems. Sensors 2022, 22, 2449. [Google Scholar] [CrossRef]
- Alabdulatif, A.; Khalil, I.; Saidur Rahman, M. Security of Blockchain and AI-Empowered Smart Healthcare: Application-Based Analysis. Appl. Sci. 2022, 12, 11039. [Google Scholar] [CrossRef]
- Hegde, M.; Rao, R.R.; Nikhil, B.M. DDMIA: Distributed Dynamic Mutual Identity Authentication for Referrals in Blockchain-Based Health Care Networks. IEEE Access 2022, 10, 78557–78575. [Google Scholar] [CrossRef]
- Xu, B.; Xu, L.D.; Wang, Y.; Cai, H. A distributed dynamic authorization method for Internet+ medical & healthcare data access based on consortium blockchain. Enterp. Inf. Syst. 2022, 16, 1922757. [Google Scholar]
- Ajayi, O.; Abouali, M.; Saadawi, T. Blockchain architecture for secured inter-healthcare electronic health records exchange. In Advances in Intelligent Networking and Collaborative Systems, Proceedings of the 12th International Conference on Intelligent Networking and Collaborative Systems (INCoS-2020), Victoria, BC, Canada, 31 August–2 September 2020; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; pp. 161–172. [Google Scholar]
- Taloba, A.I.; Elhadad, A.; Rayan, A.; Abd El-Aziz, R.M.; Salem, M.; Alzahrani, A.A.; Alharithi, F.S.; Park, C. A blockchain-based hybrid platform for multimedia data processing in IoT-Healthcare. Alex. Eng. J. 2023, 65, 263–274. [Google Scholar] [CrossRef]
- Tortorella, G.L.; Fogliatto, F.S.; Saurin, T.A.; Tonetto, L.M.; McFarlane, D. Contributions of Healthcare 4.0 digital applications to the resilience of healthcare organizations during the COVID-19 outbreak. Technovation 2022, 111, 102379. [Google Scholar] [CrossRef]
- Jayabalan, J.; Jeyanthi, N. Scalable blockchain model using off-chain IPFS storage for healthcare data security and privacy. J. Parallel Distrib. Comput. 2022, 164, 152–167. [Google Scholar] [CrossRef]
- Denham, B.; Thompson, D.R. Ransomware and malware sandboxing. In Proceedings of the 2022 IEEE 13th Annual Ubiquitous Computing, Electronics & Mobile Communication Conference (UEMCON), New York, NY, USA, 26–29 October 2022; pp. 0173–0179. [Google Scholar]
- Lakhan, A.; Morten Groenli, T.; Majumdar, A.; Khuwuthyakorn, P.; Hussain Khoso, F.; Thinnukool, O. Potent Blockchain-Enabled Socket RPC Internet of Healthcare Things (IoHT) Framework for Medical Enterprises. Sensors 2022, 22, 4346. [Google Scholar] [CrossRef] [PubMed]
- Nwosu, A.U.; Goyal, S.B.; Bedi, P. Blockchain transforming cyber-attacks: Healthcare industry. In Innovations in Bio-Inspired Computing and Applications, Proceedings of the 11th International Conference on Innovations in Bio-Inspired Computing and Applications (IBICA 2020), 16–18 December 2020; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; pp. 258–266. [Google Scholar]
- Faghihi, F.; Zulkernine, M. RansomCare: Data-centric detection and mitigation against smartphone crypto-ransomware. Comput. Netw. 2021, 191, 108011. [Google Scholar] [CrossRef]
- Akter, S.; Michael, K.; Uddin, M.R.; McCarthy, G.; Rahman, M. Transforming business using digital innovations: The application of AI, blockchain, cloud and data analytics. Ann. Oper. Res. 2022, 308, 7–39. [Google Scholar] [CrossRef]
- Dootio, M.A.; Lakhan, A.; Sodhro, A.H.; Groenli, T.M.; Bawany, N.Z.; Kumar, S. Secure and failure hybrid delay enabled a lightweight RPC and SHDS schemes in Industry 4.0 aware IIoHT enabled fog computing. Math. Biosci.Eng. 2022, 19, 513–536. [Google Scholar] [CrossRef]
- Alzahrani, S.; Xiao, Y.; Sun, W. An Analysis of Conti Ransomware Leaked Source Codes. IEEE Access 2022, 10, 100178–100193. [Google Scholar] [CrossRef]
- Ravi, V.; Pham, T.D.; Alazab, M. Attention-based multidimensional deep learning approach for cross-architecture IoMT malware detection and classification in healthcare cyber-physical systems. IEEE Trans. Comput. Soc. Syst. 2022. [Google Scholar] [CrossRef]
- Ravi, V.; Alazab, M.; Selvaganapathy, S.; Chaganti, R. A Multi-View attention-based deep learning framework for malware detection in smart healthcare systems. Comput. Commun. 2022, 195, 73–81. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Security Scheme | Protocol | Attacks | Applications | Research Gap |
|---|---|---|---|---|---|
| [1] | Blockchain PoW | HTTP, FTP | Ransomware and data attacks | Healthcare | Higher delays |
| [2] | Blockchain PoW | TCP/IP, UDP | Static Ransomware Attacks | Healthcare | Higher delays |
| [3,4,5] | Blockchain PoC | TCP/IP, UDP | Static Ransomware attacks | Healthcare | Higher delays |
| [6,7,8] | Blockchain Semantic | TCP/IP, UDP | Anonymous attacks | Healthcare | Higher delays |
| [9,10,11,12,13,14,15] | Blockchain-enabled security | TCP/IP, UDP | Invalid transaction, failure node | Healthcare | Higher delays |
| [16,17,18,19,20,21,22] | Network Security | TCP/IP | Malware | Healthcare | Higher delays |
| [23,24,25] | Static Analysis | REST API | Known Ransomware | Healthcare | Higher delays |
| [26,27,28,29,30,31] | Dynamic Analysis | REST API | Unknown Ransomware | Healthcare | Higher delays |
| proposed | RBEF | RPC | Ransomware attacks | Healthcare | delays, cost |
| Symbol | Description |
|---|---|
| Number of Healthcare Tasks | |
| Particular task of healthcare | |
| Number of workloads | |
| Workload of task | |
| Deadline of workload | |
| Fog, Cloud, and Mobile Devices | |
| Particular fog cloud and mobile | |
| Speed of computing node | |
| Speed of mobile devices | |
| B | Number of base stations |
| Base station in network | |
| 0, 1, 2 | Assignment of workload to the base station and cloud computing |
| Number of blockchain blocks | |
| Blockchain block | |
| Hashing attributes of blockchain | |
| Public key of the blockchain | |
| Private key of the blockchain | |
| Local execution Delay | |
| Downloading time | |
| Offloading time | |
| Total Delay | |
| Total Transactional cost | |
| Fog and Cloud Delay | |
| Processing Cost |
| Parameter | Value |
|---|---|
| Workload | https://physionet.org/ (accessed on 21 September 2022) |
| Platform | Android JAVA, KOTLIN |
| Runtime Environment | Android X86 |
| k1, k2, k3 | 500 GB, 64 RAM, Core i7 |
| m1 | Android Appo-15, RAM 6G, Processing core |
| Blockchain Attributes | Public, AES-256, |
| Ransomware | Trained 500 Samples: https://github.com/ABDULLAH-RAZA/Heartbeat-Malware\_Detection-Dataset (accessed on 24 May 2021) |
| Upload and Download Bandwidth | Wifi: 20–56 mbps, heterogeneous |
| Date Time | Attack | Layer | Industry | Longitude | Latitude | Effected Data | Transaction Delays (min) |
|---|---|---|---|---|---|---|---|
| 1 January 2023 11.00 a.m. | Ryuk | Request RPC | Healthcare | 51.4 | −87 | i = 1 | 5 |
| 5 January 2023 10.00 a.m. | Ryuk | Request RPC | Healthcare | 45.4 | −65 | i = 1 | 3 |
| 5 January 2023 06.00 a.m. | unknown | Request RPC | Healthcare | 33.9 | −67 | i = 1 | 7 |
| 9 January 2023 09.00 a.m. | Conti | Respond RPC | Healthcare | 40.9 | −78 | i = 1 | 6 |
| 9 January 2023 10.00 a.m. | SamSam | Respond RPC | Healthcare | 45.8 | −89 | i = 1 | 4 |
| 11 January 2023 10.00 a.m. | Unknown | Respond RPC | Healthcare | 42 | −83 | i = 1 | 5 |
| 12 January 2023 10.00 a.m. | Ryuk | Respond RPC | Healthcare | 40 | −81 | i = 2 | 10 |
| Blockchain | Attack | Workloads | Nodes | Deadline (min) | Effected Data | Transaction Delays (min) | |
|---|---|---|---|---|---|---|---|
| BSFR-SH [2] | Ryuk | i = 1, i = 2, i = 3 | 50, 100, 500 | 18, 20, 25 | 30, 30, 40 | i = 1, i = 2, i = 3 | 12, 10, 15 |
| IPFS [3] | Ryuk | i = 1, i = 2, i = 3 | 55, 100 | 16, 20, 25 | 25, 30, 36 | i = 1, i = 3 | 9, 10, 11 |
| Ransomware Blockchain [4] | unknown | i = 1, i = 2, i = 3 | 100, 250 | 19, 23, 21 | 27, 33, 31 | i = 1, i = 3 | 8, 10, 10 |
| Ransomware Blockchain [5] | Conti | i = 1, i = 2, i = 3 | 250, 300 | 15, 16, 19 | 35, 32, 38 | i = 1, i = 3 | 20, 16, 19 |
| FBASHI [13] | SamSam | i = 1, i = 2, i = 3 | 300, 500 | 13, 15, 17 | 31, 30, 34 | i = 1, i = 2 | 18, 15, 17 |
| Block MedCare [14] | Uknown | i = 1, i = 2, i = 3 | 500, 1000 | 15, 16, 18 | 33, 32, 36 | i = 1, i = 3 | 18, 16, 18 |
| Blockchain-IoMT [15] | Ryuk | i = 1, i = 2, i = 3 | 1000 | 14, 20, 25 | 27, 40, 50 | i = 2, i = 3 | 13, 20, 25 |
| Proposed RBEF | Ryuk, Conti | i = 1, i = 2, i = 3 | 1000 | 14, 20, 25 | 15, 19, 24 | i = 1, i = 2, i = 3 | 10, 10, 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lakhan, A.; Thinnukool, O.; Groenli, T.M.; Khuwuthyakorn, P. RBEF: Ransomware Efficient Public Blockchain Framework for Digital Healthcare Application. Sensors 2023, 23, 5256. https://doi.org/10.3390/s23115256
Lakhan A, Thinnukool O, Groenli TM, Khuwuthyakorn P. RBEF: Ransomware Efficient Public Blockchain Framework for Digital Healthcare Application. Sensors. 2023; 23(11):5256. https://doi.org/10.3390/s23115256
Chicago/Turabian StyleLakhan, Abdullah, Orawit Thinnukool, Tor Morten Groenli, and Pattaraporn Khuwuthyakorn. 2023. "RBEF: Ransomware Efficient Public Blockchain Framework for Digital Healthcare Application" Sensors 23, no. 11: 5256. https://doi.org/10.3390/s23115256