



Inertial Sensors for Hip Arthroplasty Rehabilitation: A Scoping Review

 , , ,
, , , 
Abstract
:1. Introduction
2. Background and Motivation
3. Materials and Methods
3.1. Definition of the Research Questions to Determine the Scope
3.2. Search Strategy to Extract the Documents
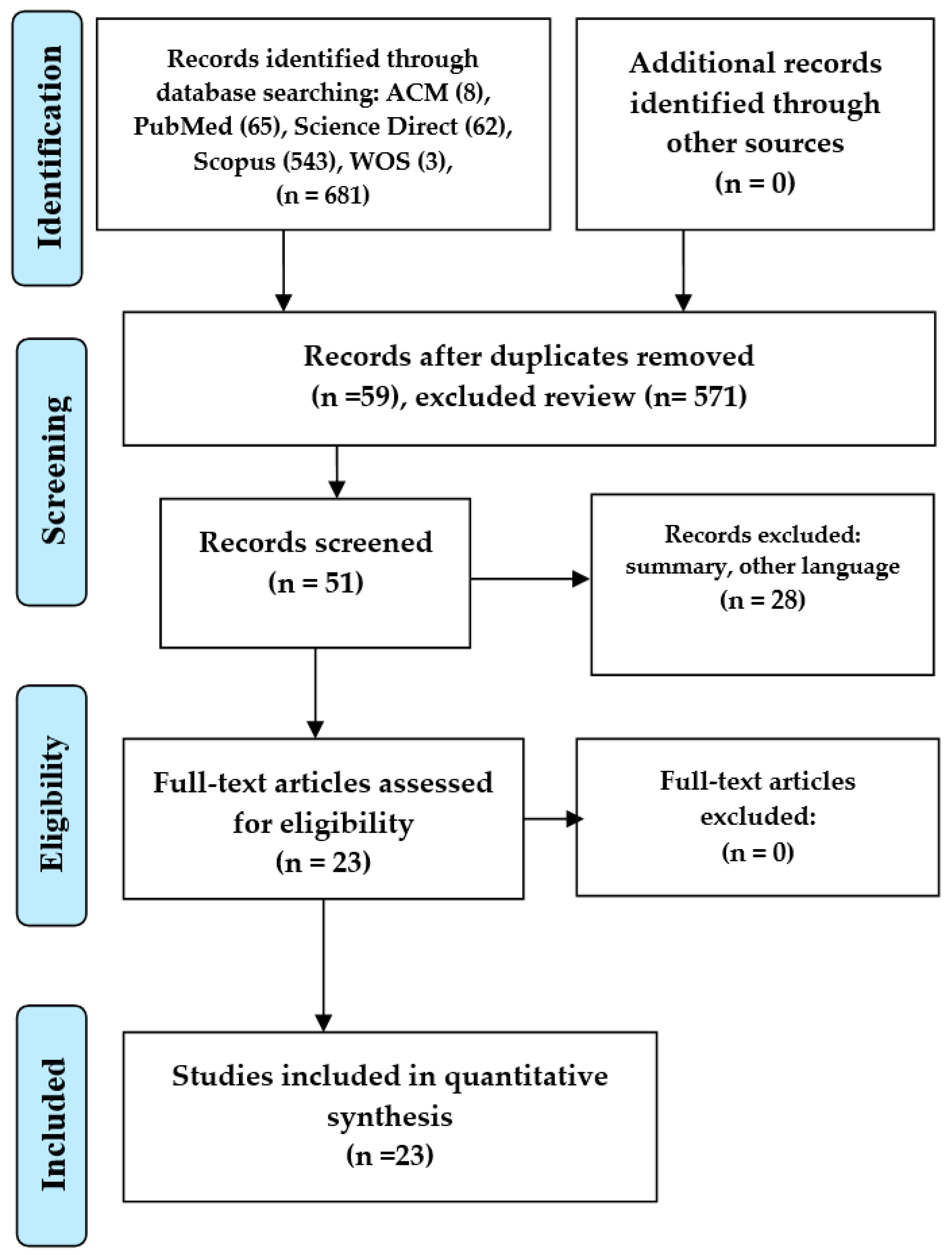
3.3. Screening of Documents
3.4. Data Extraction and Review Process
4. Results
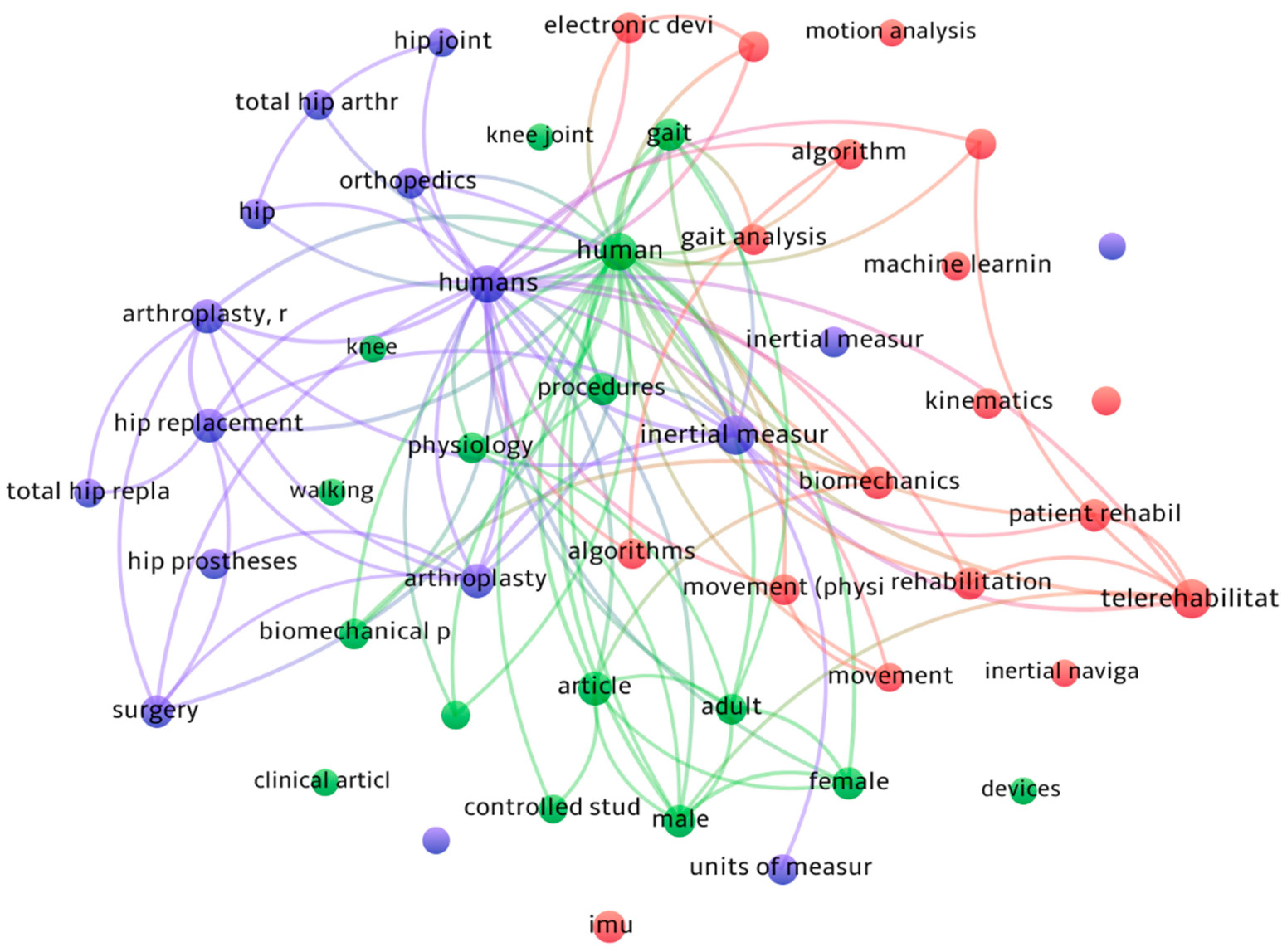
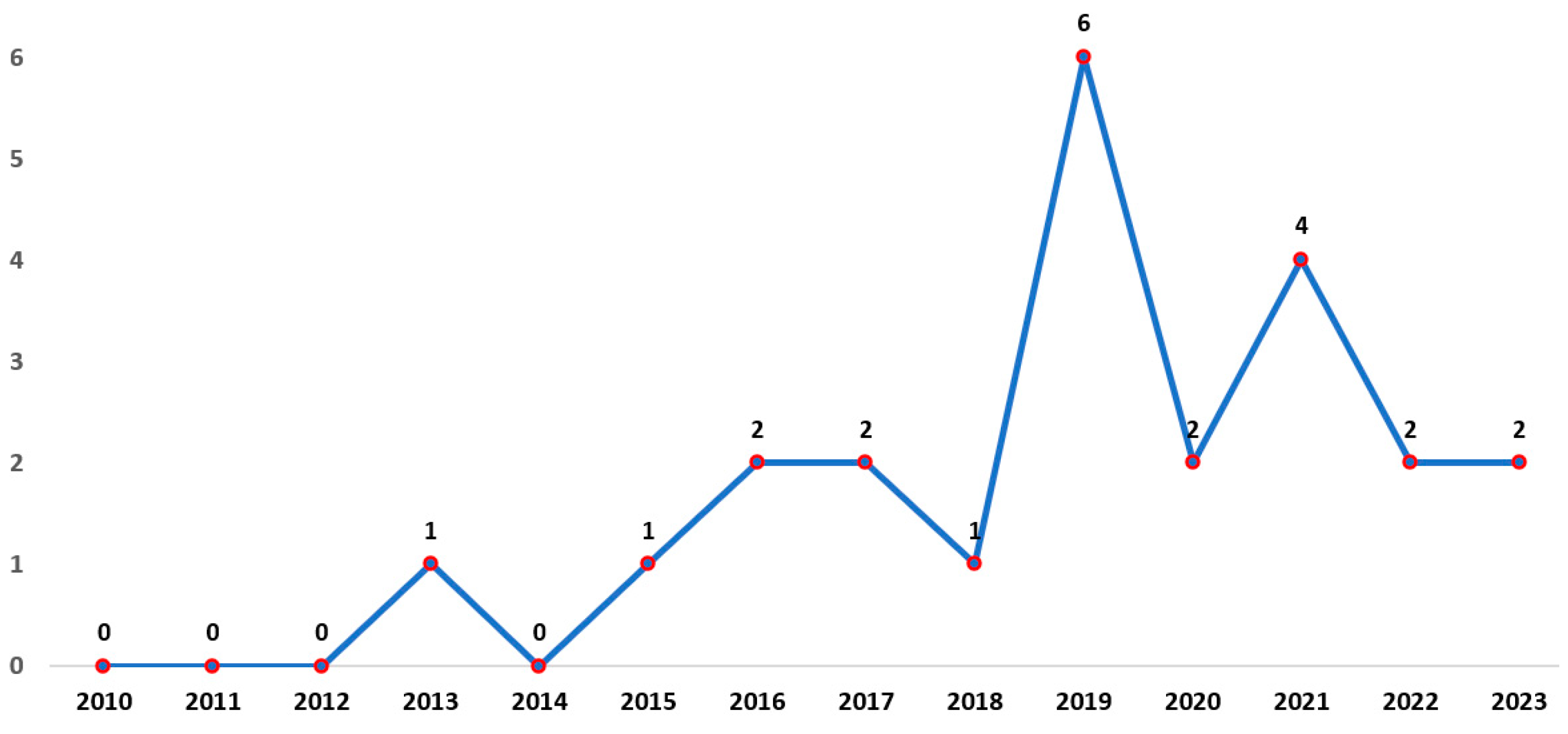
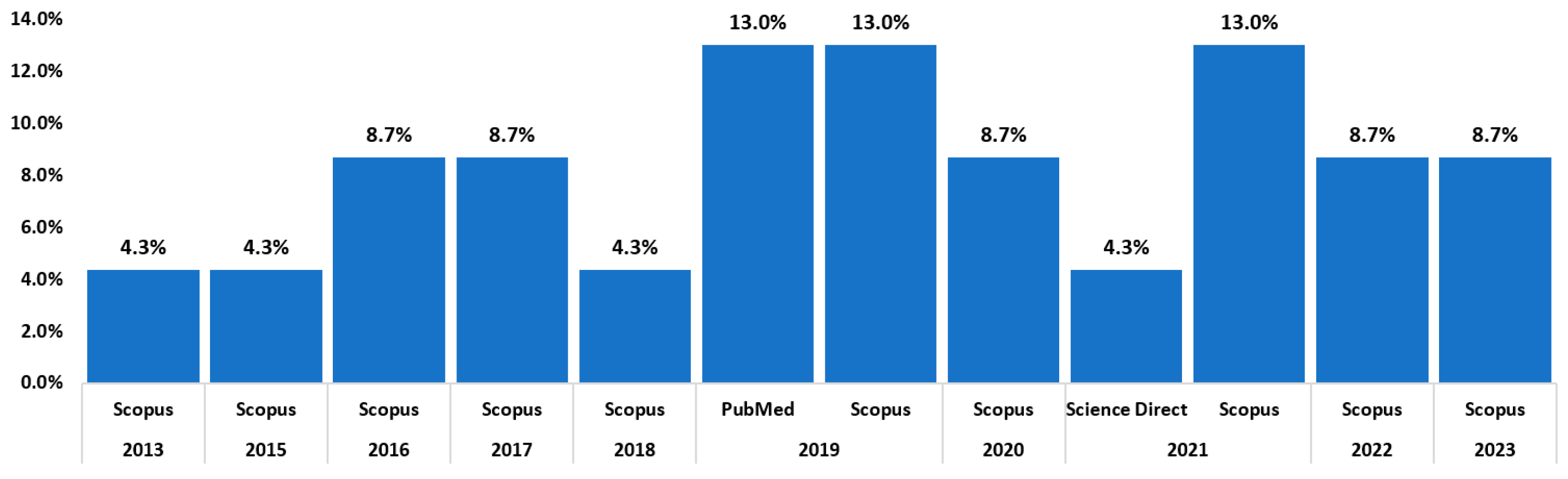
4.1. Bibliometric Analysis
4.2. Review of the Literature to Map the Studies
4.2.1. RQ1—What Are the Most Common Types of IMUs Used to Assess Movement in Hip Arthroplasty?
4.2.2. RQ2—What Are the Main Functions Performed by Inertial Sensors to Assess Movements in People Who Have Undergone Hip Arthroplasty?
4.2.3. RQ3—What Methods Are Applied in Inertial Sensors to Assess Movements in People Who Have Undergone Hip Arthroplasty?
4.2.4. RQ4—What Type of Research and Contributions Has Been Found Related to Inertial Sensors for Assessing the Motions of People Who Have Undergone Hip Arthroplasty?
4.2.5. RQ5—What Advantages Were Found in the Application of Inertial Sensors?
4.2.6. RQ6—What Disadvantages Were Found in the Application of Inertial Sensors?
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section | Item | PRISMA-ScR Checklist Item | Reported on Page # |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a scoping review. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable) the background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 1–2 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 5 |
| METHODS | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a web address), and if available, provide registration information, including the registration number. | 3–10 |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 3–10 |
| Information sources | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 3–10 |
| Search | 8 | Present the full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | 3–10 |
| Selection of sources of evidence | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | 3–10 |
| Data charting process | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was performed independently or in duplicate) and any processes for obtaining and confirming data from investigators. | 3–10 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 3–10 |
| Critical appraisal of individual sources of evidence | 12 | If performed, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | 3–10 |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 3–10 |
| RESULTS | |||
| Selection of sources of evidence | 14 | Give the number of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | 10–18 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | 10–18 |
| Critical appraisal within sources of evidence | 16 | If performed, present data on the critical appraisal of included sources of evidence (see item 12). | 10–18 |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | 10–18 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | 10–18 |
| DISCUSSION | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | 18–20 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | 20 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 20 |
| FUNDING | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | 20 |
References
- Suzuki, Y.; Hahn, M.E.; Enomoto, Y. Estimation of Foot Trajectory and Stride Length during Level Ground Running Using Foot-Mounted Inertial Measurement Units. Sensors 2022, 22, 7129. [Google Scholar] [CrossRef]
- Marotta, L.; Scheltinga, B.L.; van Middelaar, R.; Bramer, W.M.; van Beijnum, B.-J.F.; Reenalda, J.; Buurke, J.H. Accelerometer-Based Identification of Fatigue in the Lower Limbs during Cyclical Physical Exercise: A Systematic Review. Sensors 2022, 22, 3008. [Google Scholar] [CrossRef]
- Seel, T.; Raisch, J.; Schauer, T. IMU-Based Joint Angle Measurement for Gait Analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef]
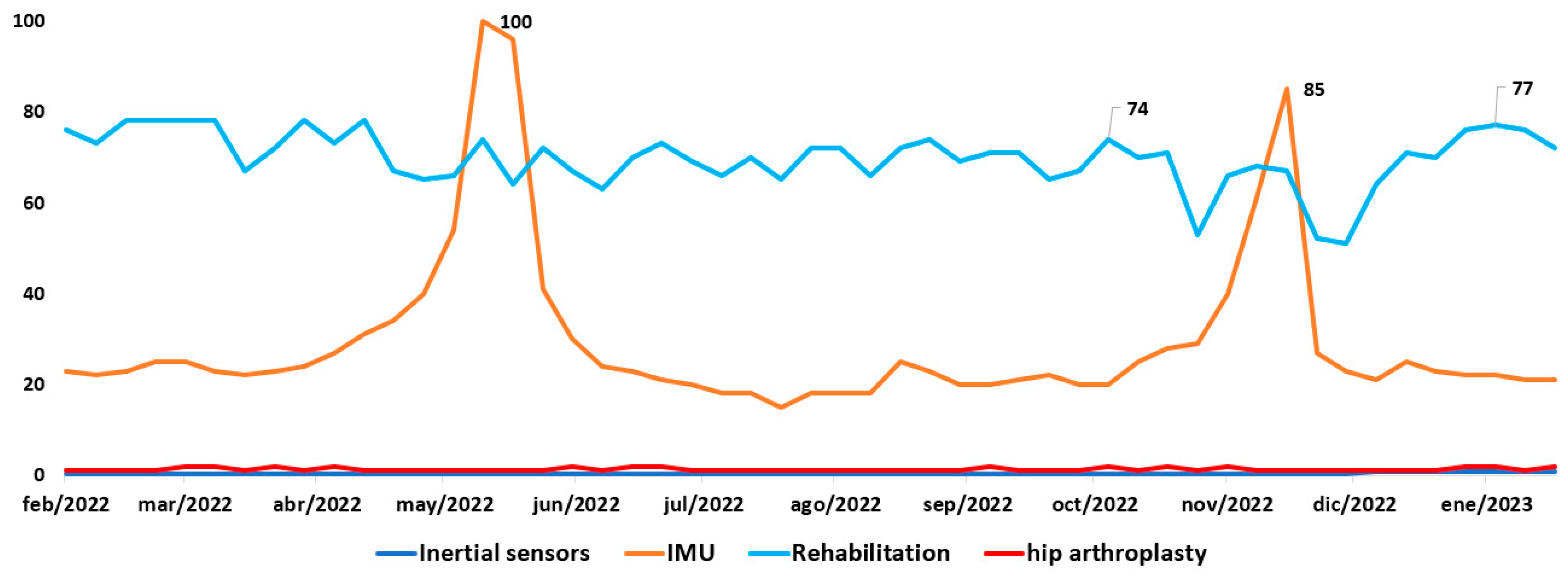
- Google Trends. IMU Trend, Inertial Sensors, Hip Arthroplasty in the Last 12 Months. 2023. Available online: https://trends.google.es/trends/explore?q=Inertialsensors,IMU,Rehabilitation,hiparthroplasty,Telerehabilitation (accessed on 26 February 2023).
- Acosta-Vargas, P.; Novillo-Villegas, S.; Salvador-Acosta, B.; Calvopina, M.; Kyriakidis, N.; Ortiz-Prado, E.; Salvador-Ullauri, L. Accessibility Analysis of Worldwide COVID-19-Related Information Portals. Int. J. Environ. Res. Public Health 2022, 19, 12102. [Google Scholar] [CrossRef]
- Zhu, J.; Liu, X.; Shi, Q.; He, T.; Sun, Z.; Guo, X.; Liu, W.; Sulaiman, O.B.; Dong, B.; Lee, C. Development trends and perspectives of future sensors and MEMS/NEMS. Micromachines 2019, 11, 7. [Google Scholar] [CrossRef]
- Leiden University. VOSviewer. 2023. Available online: https://www.vosviewer.com/ (accessed on 26 February 2023).
- Tang, H.; Zhou, Y.; Mai, B.; Zhu, B.; Chen, P.; Fu, Y.; Wang, Z. Monitoring hip posture in total hip arthroplasty using an inertial measurement unit-based hip smart trial system: An in vitro validation experiment using a fixed pelvis model. J. Biomech. 2019, 97, 109415. [Google Scholar] [CrossRef]
- Teufl, W.; Taetz, B.; Miezal, M.; Lorenz, M.; Pietschmann, J.; Jöllenbeck, T.; Fröhlich, M.; Bleser, G. Towards an inertial sensor-based wearable feedback system for patients after total hip arthroplasty: Validity and applicability for gait classification with gait kinematics-based features. Sensors 2019, 19, 5006. [Google Scholar] [CrossRef]
- Ferreira, L.C.V.; Rabelo, A.G.; Vieira, M.F.; Pereira, A.A.; Andrade, A.D.O. Gait variability and symmetry assessment with inertial sensors for quantitative discrimination of Trendelenburg sign in total hip arthroplasty patients: A pilot study based on convenience sampling. Res. Biomed. Eng. 2018, 34, 65–72. [Google Scholar] [CrossRef]
- Bolink, S.; Lenguerrand, E.; Brunton, L.R.; Wylde, V.; Gooberman-Hill, R.; Heyligers, I.C.; Blom, A.W.; Grimm, B. Assessment of physical function following total hip arthroplasty: Inertial sensor based gait analysis is supplementary to patient-reported outcome measures. Clin. Biomech. 2016, 32, 171–179. [Google Scholar] [CrossRef]
- Reh, J.; Hwang, T.-H.; Schmitz, G.; Effenberg, A.O. Dual mode gait sonification for rehabilitation after unilateral hip arthroplasty. Brain Sci. 2019, 9, 66. [Google Scholar] [CrossRef]
- Zügner, R.; Tranberg, R.; Timperley, J.; Hodgins, D.; Mohaddes, M.; Kärrholm, J. Validation of inertial measurement units with optical tracking system in patients operated with Total hip arthroplasty. BMC Musculoskelet. Disord. 2019, 20, 52. [Google Scholar] [CrossRef]
- PRISMA Statement. PRISMA for Scoping Reviews. 2021. Available online: https://www.prisma-statement.org/Extensions/ScopingReviews (accessed on 26 February 2023).
- Saha, S.K.; Barton, C.; Promite, S.; Mazza, D. Knowledge, Perceptions and Practices of Community Pharmacists Towards Antimicrobial Stewardship: A Systematic Scoping Review. Antibiotics 2019, 8, 263. [Google Scholar] [CrossRef]
- Idostatistics. Cohen’s Kappa Free Calculator. 2020. Available online: https://idostatistics.com/cohen-kappa-free-calculator/#risultati (accessed on 19 October 2022).
- PRISMA Statement. PRISMA Flow Diagram. 2021. Available online: http://prisma-statement.org/prismastatement/flowdiagram.aspx (accessed on 27 May 2021).
- Jain, Y.K.; Bha, S.K. Min max normalization based data perturbation method for privacy protection. Int. J. Comput. Commun. Technol. 2011, 2, 45–50. [Google Scholar] [CrossRef]
- Shuttleworth, M.P.; Vickers, O.; Smeeton, M.; Board, T.; Isaac, G.; Culmer, P.; Williams, S.; Kay, R.W. Inertial Tracking System for Monitoring Dual Mobility Hip Implants In Vitro. Sensors 2023, 23, 904. [Google Scholar] [CrossRef]
- Vayalapra, S.; Wang, X.; Qureshi, A.; Vepa, A.; Rahman, U.; Palit, A.; Williams, M.A.; King, R.; Elliott, M.T. Repeatability of Inertial Measurement Units for Measuring Pelvic Mobility in Patients Undergoing Total Hip Arthroplasty. Sensors 2023, 23, 377. [Google Scholar] [CrossRef]
- Kaufmann, M.; Nüesch, C.; Clauss, M.; Pagenstert, G.; Eckardt, A.; Ilchmann, T.; Stoffel, K.; Mündermann, A.; Ismailidis, P. Functional assessment of total hip arthroplasty using inertial measurement units: Improvement in gait kinematics and association with patient-reported outcome measures. J. Orthop. Res. 2022, 41, 759–770. [Google Scholar] [CrossRef]
- Wei, J.C.J.; Blaauw, B.; Van Der Pol, D.G.M.; Saldivar, M.C.; Lai, C.-F.; Dankelman, J.; Horeman, T. Design of an Affordable, Modular Implant Device for Soft Tissue Tension Assessment and Range of Motion Tracking during Total Hip Arthroplasty. IEEE J. Transl. Eng. Health Med. 2022, 10, 2500310. [Google Scholar] [CrossRef]
- Teufl, W.; Taetz, B.; Miezal, M.; Dindorf, C.; Fröhlich, M.; Trinler, U.; Hogan, A.; Bleser, G. Automated detection and explainability of pathological gait patterns using a one-class support vector machine trained on inertial measurement unit based gait data. Clin. Biomech. 2021, 89, 105452. [Google Scholar] [CrossRef]
- Chen, H.; Yang, Z.; Zhang, J.; Liu, J.; Tang, H.; Zhou, Y.; Zhu, B.; Wang, Z. An IMU-Based Real-Time Measuring System for Acetabular Prosthesis Implant Angles in THR Surgeries. IEEE Sens. J. 2021, 21, 19407–19415. [Google Scholar] [CrossRef]
- Alcaraz, J.C.; Moghaddamnia, S.; Penner, M.; Peissig, J. Monitoring the rehabilitation progress using a DCNN and kinematic data for digital healthcare. In Proceedings of the European Signal Processing Conference, Dublin, Ireland, 23–27 August 2021; pp. 1333–1337. [Google Scholar]
- Zhao, W.; Yang, S.; Luo, X. Towards rehabilitation at home after total knee replacement. Tsinghua Sci. Technol. 2021, 26, 791–799. [Google Scholar] [CrossRef]
- Bravi, M.; Gallotta, E.; Morrone, M.; Maselli, M.; Santacaterina, F.; Toglia, R.; Foti, C.; Sterzi, S.; Bressi, F.; Miccinilli, S. Concurrent validity and inter trial reliability of a single inertial measurement unit for spatial-temporal gait parameter analysis in patients with recent total hip or total knee arthroplasty. Gait Posture 2020, 76, 175–181. [Google Scholar] [CrossRef]
- Dindorf, C.; Teufl, W.; Taetz, B.; Bleser, G.; Fröhlich, M. Interpretability of input representations for gait classification in patients after total hip arthroplasty. Sensors 2020, 20, 4385. [Google Scholar] [CrossRef]
- Manupibul, U.; Vijittrakarnrung, C.; Sa-Ngasoongsong, P.; Fuangfa, P.; Jaovisidha, S.; Charoensuk, W. Innovative Force-PRO device to measure force and implant position in total hip arthroplasty. Phys. Eng. Sci. Med. 2020, 43, 109–117. [Google Scholar] [CrossRef]
- Grip, H.; Nilsson, K.G.; Häger, C.K.; Lundström, R.; Öhberg, F. Does the femoral head size in hip arthroplasty influence lower body movements during squats, gait and stair walking? A clinical pilot study based on wearable motion sensors. Sensors 2019, 19, 3240. [Google Scholar] [CrossRef]
- Chen, H.; Cao, Z.; Su, S.; Liu, J.; Wang, Z. Measurement System for Attitude of Anterior Pelvic Plane and Implantation of Prothesis in THR Surgery. IEEE Trans. Instrum. Meas. 2018, 67, 1913–1921. [Google Scholar] [CrossRef]
- Cao, Z.; Su, S.; Tang, H.; Zhou, Y.; Wang, Z.; Chen, H. IMU-based Real-time Pose Measurement system for Anterior Pelvic Plane in Total Hip Replacement Surgeries. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Jeju Island, Republic of Korea, 11–15 July 2017; pp. 1360–1363. [Google Scholar]
- Su, S.; Zhou, Y.; Wang, Z.; Chen, H. Monocular Vision-and IMU-Based System for Prosthesis Pose Estimation during Total Hip Replacement Surgery. IEEE Trans. Biomed. Circuits Syst. 2017, 11, 661–670. [Google Scholar] [CrossRef]
- Pflugi, S.; Liu, L.; Ecker, T.M.; Schumann, S.; Larissa Cullmann, J.; Siebenrock, K.; Zheng, G. A cost-effective surgical navigation solution for periacetabular osteotomy (PAO) surgery. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 271–280. [Google Scholar] [CrossRef]
- Cao, Z.; Su, S.; Chen, H.; Tang, H.; Zhou, Y.; Wang, Z. Pose measurement of Anterior Pelvic Plane based on inertial measurement unit in total hip replacement surgeries. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Orlando, FL, USA, 16–20 August 2016; Volume 2016, pp. 5801–5804. [Google Scholar]
- Su, S.; Gao, J.; Cao, Z.; Chen, H.; Wang, Z. Smart trail with camera and inertial measurement unit for intraoperative estimation of hip range of motion in total hip replacement surgery. In Proceedings of the IEEE Biomedical Circuits and Systems Conference: Engineering for Healthy Minds and Able Bodies, BioCAS 2015—Proceedings, Atlanta, GA, USA, 22–24 October 2015. [Google Scholar]
- McGinnis, R.S.; Perkins, N.C. Inertial sensor based method for identifying spherical joint center of rotation. J. Biomech. 2013, 46, 2546–2549. [Google Scholar] [CrossRef]
- Acosta-Vargas, P.; Salvador-Acosta, B.; Salvador-Ullauri, L. Dataset Inertial Sensors for Hip Arthroplasty Rehabilitation. Mendeley Data V2. 2023. Available online: https://data.mendeley.com/datasets/wtbpcrc6n6/2 (accessed on 5 April 2023).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann Intern Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]







| N° | Quality Assessment Questions | Answer |
|---|---|---|
| QA1 | Does the paper describe inertial sensors applied in hip arthroplasty? | (+1) Yes/(+0) No |
| QA2 | Does the paper specify the evaluation methods applied to inertial sensors? | (+1) Yes/(+0) No |
| QA3 | Does the paper discuss any findings of inertial sensors for hip arthroplasty evaluation? | (+1) Yes/(+0) No |
| QA4 | Are limitations described in the inertial sensors considered for hip arthroplasty treatment? | (+1) Yes/(+0) No |
| QA5 | Is the journal or conference in which the paper was published indexed in SJR? | (+1) if it is ranked Q1, (+0.75) if it is ranked Q2, (+0.50) if it is ranked Q3, (+0.25) if it is ranked Q4, (+0.0) if it is not ranked. |
| Database | String Search | Number of Studies |
|---|---|---|
| ACM Digital Library | [All: telerehabilitation and sensors] AND [All: inertial] AND [All: arthroplasty] AND [All: hip] | 8 |
| PubMed | telerehabilitation OR (sensors AND inertial) AND arthroplasty AND hip | 65 |
| ScienceDirect | (Telerehabilitation OR web) and (sensors and inertial) and arthroplasty and hip | 62 |
| Scopus | TITLE-ABS-KEY (web OR telerehabilitation OR telerehabilitation OR (sensors AND inertial) AND arthroplasty AND hip) | 543 |
| Web of Science | (((TS = (web)) OR TS = (telerehabilitation)) AND TS = (sensors AND inertial)) AND TS = (arthroplasty AND hip) | 3 |
| Total number of studies | 681 |
| ID | Publication Name | Quality Assessment | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Quartile | SJR Factor | QA1 | QA2 | QA3 | QA4 | QA5 | Score | Normalization | ||
| TeW2021 | Automated detection and explainability of pathological gait patterns using a one-class support vector machine trained on inertial measurement unit based gait data | Q1 | 0.75 | 1 | 1 | 1 | 1 | 1.00 | 5.00 | 1.0 |
| TaH2019 | Monitoring hip posture in total hip arthroplasty using an inertial measurement unit-based hip smart trial system: An in vitro validation experiment using a fixed pelvis model | Q1 | 0.8 | 1 | 1 | 1 | 1 | 1.00 | 5.00 | 1.0 |
| TeW2019 | Towards an inertial sensor-based wearable feedback system for patients after total hip arthroplasty: Validity and applicability for gait classification with gait kinematics-based features | Q2 | 0.56 | 1 | 1 | 1 | 1 | 0.75 | 4.75 | 0.8 |
| MaU2019 | Innovative Force-PRO device to measure force and implant position in total hip arthroplasty | Q1 | 0.72 | 1 | 1 | 1 | 1 | 1.00 | 5.00 | 1.0 |
| ReJ2019 | Dual Mode Gait Sonification for Rehabilitation After Unilateral Hip Arthroplasty | Q3 | 0.73 | 1 | 1 | 1 | 1 | 0.50 | 4.50 | 0.5 |
| ZuR2019 | Validation of inertial measurement units with optical tracking system in patients operated with Total hip arthroplasty | Q2 | 0.67 | 1 | 1 | 1 | 1 | 0.75 | 4.75 | 0.8 |
| KaM2022 | Functional assessment of total hip arthroplasty using inertial measurement units: Improvement in gait kinematics and association with patient-reported outcome measures | Q2 | 0.84 | 1 | 1 | 1 | 1 | 0.75 | 4.75 | 0.8 |
| WeJ2022 | Design of an Affordable, Modular Implant Device for Soft Tissue Tension Assessment and Range of Motion Tracking During Total Hip Arthroplasty | Q2 | 0.84 | 1 | 1 | 1 | 1 | 0.75 | 4.75 | 0.8 |
| PfS2016 | A cost-effective surgical navigation solution for periacetabular osteotomy (PAO) surgery | Q1 | 1.00 | 1 | 1 | 1 | 1 | 1.00 | 5 | 1 |
| ChH2021 | An IMU-Based Real-Time Measuring System for Acetabular Prosthesis Implant Angles in THR Surgeries | Q1 | 0.93 | 1 | 1 | 1 | 1 | 1.00 | 5 | 1 |
| BrM2020 | Concurrent validity and inter trial reliability of a single inertial measurement unit for spatial-temporal gait parameter analysis in patients with recent total hip or total knee arthroplasty | Q1 | 0.68 | 1 | 1 | 1 | 1 | 1.00 | 5 | 1 |
| GrH2019 | Does the femoral head size in hip arthroplasty influence lower body movements during squats, gait and stair walking? A clinical pilot study based on wearable motion sensors | Q2 | 0.56 | 1 | 1 | 1 | 1 | 0.75 | 4.75 | 0.75 |
| CaZ2017 | IMU-based Real-time Pose Measurement system for Anterior Pelvic Plane in Total Hip Replacement Surgeries | N/A | 0.00 | 1 | 1 | 1 | 1 | 0 | 4 | 0 |
| McR2013 | Inertial sensor based method for identifying spherical joint center of rotation | Q1 | 0.75 | 1 | 1 | 1 | 1 | 1.00 | 5 | 1 |
| ShM2023 | Inertial Tracking System for Monitoring Dual Mobility Hip Implants In Vitro | Q1 | 0.80 | 1 | 1 | 1 | 1 | 1.00 | 5 | 1 |
| DinC2020 | Interpretability of input representations for gait classification in patients after total hip arthroplasty | Q2 | 0.56 | 1 | 1 | 1 | 1 | 0.75 | 4.75 | 0.75 |
| ChH2018 | Measurement System for Attitude of Anterior Pelvic Plane and Implantation of Prothesis in THR Surgery | Q1 | 1.18 | 1 | 1 | 1 | 1 | 1.00 | 5 | 1 |
| AlJ2021 | Monitoring the rehabilitation progress using a DCNN and kinematic data for digital healthcare | N/A | 0.00 | 1 | 1 | 1 | 1 | 0 | 4 | 0 |
| SuS2017 | Monocular Vision-and IMU-Based System for Prosthesis Pose Estimation during Total Hip Replacement Surgery | Q1 | 1.75 | 1 | 1 | 1 | 1 | 1.00 | 5 | 1 |
| CaZ2016 | Pose measurement of Anterior Pelvic Plane based on inertial measurement unit in total hip replacement surgeries | N/A | 0.00 | 1 | 1 | 1 | 1 | 0 | 4 | 0 |
| VaS2023 | Repeatability of Inertial Measurement Units for Measuring Pelvic Mobility in Patients Undergoing Total Hip Arthroplasty | Q1 | 0.80 | 1 | 1 | 1 | 1 | 1.00 | 5 | 1 |
| SuS2015 | Smart trail with camera and inertial measurement unit for intraoperative estimation of hip range of motion in total hip replacement surgery | N/A | 0.00 | 1 | 1 | 1 | 1 | 0 | 4 | 0 |
| ZhW2021 | Towards rehabilitation at home after total knee replacement | Q1 | 1.00 | 1 | 1 | 1 | 1 | 1.00 | 5 | 1 |
| N° | ID | Scientific Articles | Reference | Year |
|---|---|---|---|---|
| 1 | ShM2023 | Inertial Tracking System for Monitoring Dual Mobility Hip Implants In Vitro | [19] | 2023 |
| 2 | VaS2023 | Repeatability of Inertial Measurement Units for Measuring Pelvic Mobility in Patients Undergoing Total Hip Arthroplasty | [20] | 2023 |
| 3 | KaM2022 | Functional assessment of total hip arthroplasty using inertial measurement units: Improvement in gait kinematics and association with patient-reported outcome measures | [21] | 2022 |
| 4 | WeJ2022 | Design of an Affordable, Modular Implant Device for Soft Tissue Tension Assessment and Range of Motion Tracking During Total Hip Arthroplasty | [22] | 2022 |
| 5 | TeW2021 | Automated detection and explainability of pathological gait patterns using a one-class support vector machine trained on inertial measurement unit based gait data | [23] | 2021 |
| 6 | ChH2021 | An IMU-Based Real-Time Measuring System for Acetabular Prosthesis Implant Angles in THR Surgeries | [24] | 2021 |
| 7 | AlJ2021 | Monitoring the rehabilitation progress using a DCNN and kinematic data for digital healthcare | [25] | 2021 |
| 8 | ZhW2021 | Towards rehabilitation at home after total knee replacement | [26] | 2021 |
| 9 | BrM2020 | Concurrent validity and inter trial reliability of a single inertial measurement unit for spatial-temporal gait parameter analysis in patients with recent total hip or total knee arthroplasty | [27] | 2020 |
| 10 | DinC2020 | Interpretability of input representations for gait classification in patients after total hip arthroplasty | [28] | 2020 |
| 11 | TaH2019 | Monitoring hip posture in total hip arthroplasty using an inertial measurement unit-based hip smart trial system: An in vitro validation experiment using a fixed pelvis model | [8] | 2019 |
| 12 | TeW2019 | Towards an inertial sensor-based wearable feedback system for patients after total hip arthroplasty: Validity and applicability for gait classification with gait kinematics-based features | [9] | 2019 |
| 13 | MaU2019 | Innovative Force-PRO device to measure force and implant position in total hip arthroplasty | [29] | 2019 |
| 14 | ReJ2019 | Dual Mode Gait Sonification for Rehabilitation After Unilateral Hip Arthroplasty | [12] | 2019 |
| 15 | ZuR2019 | Validation of inertial measurement units with optical tracking system in patients operated with Total hip arthroplasty | [13] | 2019 |
| 16 | GrH2019 | Does the femoral head size in hip arthroplasty influence lower body movements during squats, gait and stair walking? A clinical pilot study based on wearable motion sensors | [30] | 2019 |
| 17 | ChH2018 | Measurement System for Attitude of Anterior Pelvic Plane and Implantation of Prothesis in THR Surgery | [31] | 2018 |
| 18 | CaZ2017 | IMU-based Real-time Pose Measurement system for Anterior Pelvic Plane in Total Hip Replacement Surgeries | [32] | 2017 |
| 19 | SuS2017 | Monocular Vision-and IMU-Based System for Prosthesis Pose Estimation during Total Hip Replacement Surgery | [33] | 2017 |
| 20 | PfS2016 | A cost-effective surgical navigation solution for periacetabular osteotomy (PAO) surgery | [34] | 2016 |
| 21 | CaZ2016 | Pose measurement of Anterior Pelvic Plane based on inertial measurement unit in total hip replacement surgeries | [35] | 2016 |
| 22 | SuS2015 | Smart trail with camera and inertial measurement unit for intraoperative estimation of hip range of motion in total hip replacement surgery | [36] | 2015 |
| 23 | McR2013 | Inertial sensor based method for identifying spherical joint center of rotation | [37] | 2013 |
| N° | ID | Ref | Sensor Type | Main Functions | Methods Used | Research | Advantages | Limitations |
|---|---|---|---|---|---|---|---|---|
| 1 | ShM2023 | [19] | IMU | Dual mobility hip implants tracked. | Accurate inertial tracking of dual mobility hip implants. | Inertial sensors monitor hip arthroplasty. | High accuracy, real-time, non-invasive, portable, and accessible. | Drift, magnetic, calibrate, in vitro, in vivo |
| 2 | VaS2023 | [20] | IMU | IMU repeatability in hip replacement. | IMU is reliable for measuring hip mobility. | IMU is useful for assessing THA. | Non-invasive, portable, real-time, accurate, and reliable. | Inaccurate, drift, noise, interference, placement. |
| 3 | KaM2022 | [21] | IMU | Measure implant motion and position. | Data analyzed for post-surgery recovery. | Sensors produce sound for gait. | Accurate, portable, versatile, efficient, rehabilitation | Accuracy, stability, range, orientation, and cost. |
| 4 | WeJ2022 | [22] | IMU | Motion aspects, velocity, acceleration, orientation. | A hip testing system for evaluation. | Monitoring, Evaluation, Rehabilitation, Arthroplasty, IMU. | Non-invasive, accurate, portable, real-time, feedback. | Reduce noise, bias, and data. |
| 5 | TeW2021 | [23] | IMU | Measures implant angles in real-time. | We are detecting gait patterns with SVM. | Develop a single-class SVM algorithm. | Real-time gait analysis visualization. | Inaccurate joint angle measurement. |
| 6 | ChH2021 | [24] | IMU | Real-time prosthesis angle measurement. | Real-time implantation angle measurement. | Improve precision, efficiency, angles, quantify results, and attention. | Monitor, measure, real-time, acetabular, precision | Accuracy, drift, calibration, motion, interference. |
| 7 | AlJ2021 | [25] | IMU | Rehabilitation monitoring using DCNN. | Accurate gait classification, real-time feedback, and monitoring for rehabilitation | Improve accuracy, efficiency, measurements, outcomes, rehabilitation. | Improve accuracy, effectiveness, cost, and complexity. | Careful calibration, synchronization errors, combined measures, DCNNs, and training data. |
| 8 | ZhW2021 | [26] | IMU | Rehabilitation post-knee surgery, remote training. | Approaches and technologies for remote rehabilitation. | Inertial sensors, monitor, TKR, rehabilitation, personalized. | Improve effectiveness, accessibility, feedback, engagement, and compliance. | The difficulty, calibration, accuracy, comfort, and inconvenience. |
| 9 | BrM2020 | [27] | IMU | IMU gait analysis post-surgery. | IMU validated for gait measurement. | Validation, IMU, gait, parameters, implications | Convenient, efficient, accurate monitoring. | Choose wisely for gait analysis. |
| 10 | DinC2020 | [28] | IMU | Gait classification input representations compared. | Important gait characteristics identified for classification. | Inertial sensors: gait assessment, hip arthroplasty, analysis data, clinical application, insights. | Transparency, interpretability, reliability, clinical, XAI. | Accurate placement, calibration, drift, errors, complex. |
| 11 | TaH2019 | [8] | IMU | Motion, velocity, acceleration, orientation. | An intelligent hip testing system evaluates movements. | IMU system for hip rehabilitation. | Non-invasive, reliable, portable, real-time feedback. | Noise reduction and bias correction. |
| 12 | TeW2019 | [9] | IMU | We are measuring gait kinematics, classification, and balance. | Classification of gait using gait characteristics, support time, and speed. | Applicable inertial sensors for gait classification. | Small, lightweight, inexpensive, easy, and valuable. | Periodic calibration for accuracy. |
| 13 | MaU2019 | [29] | Force-PRO IMU | We are measuring force and implant motion. | IMU is reliable for post-arthroplasty posture. | Implant, rehabilitate load, movement, and arthroplasty. | Accurate, real-time, measurement, decision-making, non-invasive | Complex motion activity measurement. |
| 14 | ReJ2019 | [12] | IMU | Implant motion tracking in 3D. | We are measuring gait after surgery, using sonification to improve gait. | Sound, sensor, movement, patient, improvement. | Accurate, portable, versatile, efficient gait. | Limited accuracy, stability, range, orientation, and cost. |
| 15 | ZuR2019 | [13] | IMU | Analyze motion for abnormal deviations. | Optical data, inertial sensors, angles of movement, cross validation, accuracy. | Accurate, reliable hip arthroplasty movement. | Accurate, inertial, flexion, extension, adduction. | Accuracy, processing, sensors, movements, dependence |
| 16 | GrH2019 | [30] | IMU | Hip replacement affects body movements. | Wearable sensors track lower body movements. | Hip arthroplasty: range, motion, sensors, functional, squatting. | Non-invasive, portable, cost-effective, objective, and affordable. | They have limited, small samples, variability, mechanics, and sensors. |
| 17 | ChH2018 | [31] | IMU | Measurement system tracks pelvic plane during surgery. | Precise measurement of prosthesis position. | Inertial sensors, orthopedic surgery, accuracy, outcomes, development. | Accuracy, safety, cost, complexity, measurement | Inaccurate, external, magnetic, placement, obstruction. |
| 18 | CaZ2017 | [32] | IMU | Real-time IMU measures pelvic position. | The real-time IMU system measures the iliac bone to provide information on the anterior pelvic plane position. | IMUs improve THR surgery accuracy. | Real-time, non-invasive, accurate, cost-effective, and practical. | Inaccurate, external magnetic field, placement, obstruction, optimization. |
| 19 | SuS2017 | [33] | IMU | Measurement system for hip replacement using camera and IMU. | The proposed system refines position estimates using IMU and camera data. | Inertial sensors, monocular vision, prosthesis, surgery, accuracy. | Accuracy, safety, cost, complexity, improvement | Inaccurate, interference, temperature, humidity, limitation. |
| 20 | PfS2016 | [34] | IMU | Open-source surgical navigation using optical tracking. | Cost-effective PAO navigation solution. | Improve precision, safety, results, quantity, and rehabilitation. | Accuracy, safety, real-time, tracking, precision. | Accuracy, drift, calibration, motion, interference. |
| 21 | CaZ2016 | [35] | IMU | Improved hip arthroplasty outcomes using IMUs. | Kalman filter improves sensor accuracy. | Improve accuracy, safety, results, objective evaluations, and rehabilitation. | Easy, accurate, portable, affordable, and useful. | Errors, external interference, accuracy, position, placement. |
| 22 | SuS2015 | [36] | IMU | “Smart Trail” estimates hip motion. | “Smart Trail” system estimates hip motion. | Improve surgical precision. | Improve accuracy, safety, cost, complexity, and motion. | Inertial sensor limitations: sensitivity, drift, position, calibration, sample. |
| 23 | McR2013 | [37] | IMU | Method to locate ball joint’s center. | Inertial sensors estimate the joint center. They were validated with an optical measurement system. | Analyze kinematics, hip arthroplasty, inertial sensors, accuracy, and reliability. | Identify the center of rotation with sensors. | Inaccurate, time-consuming, impractical, spherical assumptions. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acosta-Vargas, P.; Flor, O.; Salvador-Acosta, B.; Suárez-Carreño, F.; Santórum, M.; Solorzano, S.; Salvador-Ullauri, L. Inertial Sensors for Hip Arthroplasty Rehabilitation: A Scoping Review. Sensors 2023, 23, 5048. https://doi.org/10.3390/s23115048
Acosta-Vargas P, Flor O, Salvador-Acosta B, Suárez-Carreño F, Santórum M, Solorzano S, Salvador-Ullauri L. Inertial Sensors for Hip Arthroplasty Rehabilitation: A Scoping Review. Sensors. 2023; 23(11):5048. https://doi.org/10.3390/s23115048
Chicago/Turabian StyleAcosta-Vargas, Patricia, Omar Flor, Belén Salvador-Acosta, Franyelit Suárez-Carreño, Marco Santórum, Santiago Solorzano, and Luis Salvador-Ullauri. 2023. "Inertial Sensors for Hip Arthroplasty Rehabilitation: A Scoping Review" Sensors 23, no. 11: 5048. https://doi.org/10.3390/s23115048