
Validation of SuPerSense, a Sensorized Surface for the Evaluation of Posture Perception in Supine Position

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- -
- Age over 18 years;
- -
- Certified diagnosis of ischemic or hemorrhagic stroke by a neurological medical examination;
- -
- Ability to stand alone or with the help of a physiotherapist in open- and closed-eyes conditions (OE, CE) for at least one minute.
- -
- Presence of cognitive impairment or linguistic difficulties that made it difficult to understand and follow the instructions of the experimenter;
- -
- Presence of pathological comorbidities (such as neurological, psychiatric, orthopedic, and metabolic diseases) that may affect motor performance under examination.
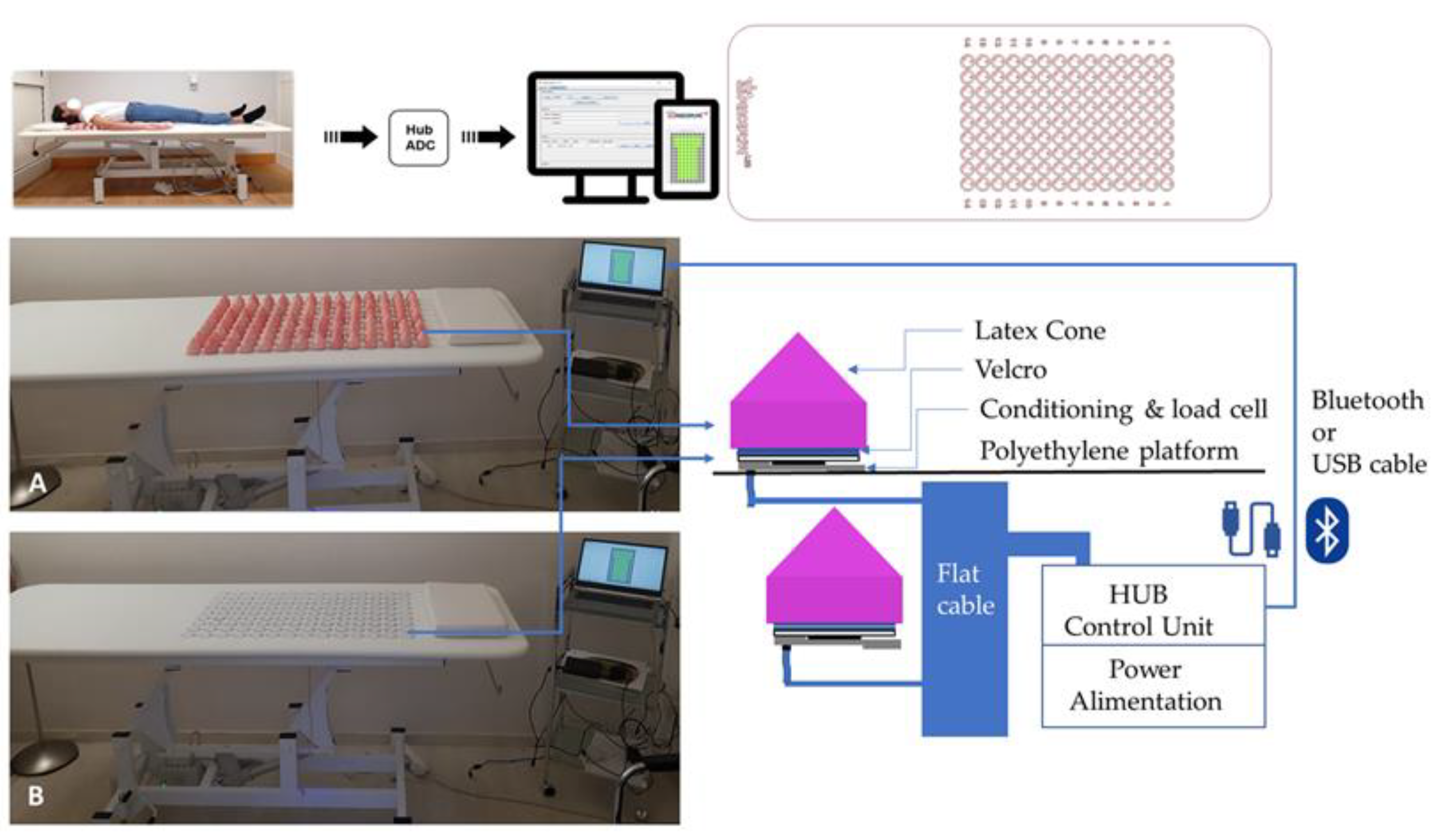
2.2. Equipment
2.3. Procedure
2.4. Data Collection and Parameters
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L. Anthology of stroke epidemiology in the 20th and 21st centuries: Assessing the past, the present, and envisioning the future. Int. J. Stroke 2019, 14, 223–237. [Google Scholar] [CrossRef]
- Langhorne, P.; O’Donnell, M.J.; Chin, S.L.; Zhang, H.; Xavier, D.; Avezum, A.; Shi, C.L. Practice patterns and outcomes after stroke across countries at different economic levels (INTERSTROKE): An international observational study. Lancet 2018, 391, 2019–2027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barra, J.; Oujamaa, L.; Chauvineau, V.; Rougier, P.; Pérennou, D. Asymmetric standing posture after stroke is related to a biased egocentric coordinate system. Neurology 2009, 72, 1582–1587. [Google Scholar] [CrossRef] [PubMed]
- Genthon, N.; Rougier, P.; Gissot, A.S.; Froger, J.; Pélissier, J.; Pérennou, D. Contribution of each lower limb to upright standing in stroke patients. Stroke 2008, 39, 1793–1799. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Is the measurement of muscle strength appropriate in patients with brain lesions? A special communication. Phys. Ther. 1989, 69, 225–230. [Google Scholar] [CrossRef]
- Pérennou, D. Weight bearing asymmetry in standing hemiparetic patients. J. Neurol. Neurosurg. Psychiatry 2005, 76, 621. [Google Scholar] [CrossRef] [Green Version]
- Marigold, D.S.; Eng, J.J. The relationship of asymmetric weight-bearing with postural sway and visual reliance in stroke. Gait Posture 2006, 23, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Van Criekinge, T.; Truijen, S.; Schröder, J.; Maebe, Z.; Blanckaert, K.; van der Waal, C.; Saeys, W. The effectiveness of trunk training on trunk control, sitting and standing balance and mobility post-stroke: A systematic review and meta-analysis. Clin. Rehabil. 2019, 33, 992–1002. [Google Scholar] [CrossRef]
- Jamal, K.; Leplaideur, S.; Rousseau, C.; Chochina, L.; Moulinet-Raillon, A.; Bonan, I. Disturbances of spatial reference frame and postural asymmetry after a chronic stroke. Exp. Brain Res. 2018, 236, 2377–2385. [Google Scholar] [CrossRef]
- Paolucci, T.; Morone, G.; Fusco, A.; Giuliani, M.; Rosati, E.; Zangrando, F.; Iosa, M. Effects of perceptive rehabilitation on balance control in patients with Parkinson’s disease. NeuroRehabilitation 2014, 34, 113–120. [Google Scholar] [CrossRef]
- Paolucci, T.; Baldari, C.; Di Franco, M.; Didona, D.; Reis, V.; Vetrano, M.; Guidetti, L. A new rehabilitation tool in fibromyalgia: The effects of perceptive rehabilitation on pain and function in a clinical randomized controlled trial. Evid.-Based Complement. Altern. Med. 2016, 2016, 7574589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paolucci, T.; Fusco, A.; Iosa, M.; Grasso, M.R.; Spadini, E.; Paolucci, S.; Morone, G. The efficacy of a perceptive rehabilitation on postural control in patients with chronic nonspecific low back pain. Int. J. Rehabil. Res. 2012, 35, 360–366. [Google Scholar] [CrossRef]
- Huang, H.C.; Chung, K.C.; Lai, D.C.; Sung, S.F. The impact of timing and dose of rehabilitation delivery on functional recovery of stroke patients. J. Chin. Med. Assoc. 2009, 72, 257–264. [Google Scholar] [CrossRef] [Green Version]
- Morone, G.; Iosa, M.; Cocchi, I.; Paolucci, T.; Arengi, A.; Bini, F.; De Angelis, D. Effects of a posture shirt with back active correction keeper on static and dynamic balance in Parkinson’s disease. J. Bodyw. Mov. Ther. 2021, 28, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, T.; Iosa, M.; Morone, G.; Fratte, M.D.; Paolucci, S.; Saraceni, V.M.; Villani, C. Romberg ratio coefficient in quiet stance and postural control in Parkinson’s disease. Neurol. Sci. 2018, 39, 1355–1360. [Google Scholar] [CrossRef]
- Tjernström, F.; Björklund, M.; Malmström, E.M. Romberg ratio in quiet stance posturography—Test to retest reliability. Gait Posture 2015, 42, 27–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scoppa, F.; Capra, R.; Gallamini, M.; Shiffer, R. Clinical stabilometry standardization: Basic definitions–acquisition interval–sampling frequency. Gait Posture 2013, 37, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Pilkar, R.; Arzouni, N.; Nolan, K.J. Postural stability during long duration quiet standing in post stroke hemiplegia. Biomed. Signal Process. Control 2018, 39, 162–168. [Google Scholar] [CrossRef]
- De Bartolo, D.; Belluscio, V.; Vannozzi, G.; Morone, G.; Antonucci, G.; Giordani, G.; Iosa, M. Sensorized assessment of dynamic locomotor imagery in people with stroke and healthy subjects. Sensors 2020, 20, 4545. [Google Scholar] [CrossRef]
- Wright, W.G.; Gurfinkel, V.S.; King, L.A.; Nutt, J.G.; Cordo, P.J.; Horak, F.B. Axial kinesthesia is impaired in Parkinson’s disease: Effects of levodopa. Exp. Neurol. 2010, 225, 202–209. [Google Scholar] [CrossRef]
- Wright, W.G.; Gurfinkel, V.S.; King, L.A.; Horak, F.B. Parkinson’s disease shows perceptuomotor asymmetry unrelated to motor symptoms. Neurosci. Lett. 2007, 417, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karnath, H.O.; Schenkel, P.; Fischer, B. Trunk orientation as the determining factor of the ‘contralateral’ deficit in the neglect syndrome and as the physical anchor of the internal representation of body orientation in space. Brain 1991, 114, 1997–2014. [Google Scholar] [CrossRef] [PubMed]
- Karnath, H.O.; Fetter, M.; Niemeier, M. Disentangling gravitational, environmental, and egocentric reference frames in spatial neglect. J. Cogn. Neurosci. 1998, 10, 680–690. [Google Scholar] [CrossRef] [PubMed]
- Matano, A.; Iosa, M.; Guariglia, C.; Pizzamiglio, L.; Paolucci, S. Does outcome of neuropsychological treatment in patients with unilateral spatial neglect after stroke affect functional outcome? Eur. J. Phys. Rehabil. Med. 2015, 51, 737–743. [Google Scholar] [PubMed]
- Pizzamiglio, L.; Committeri, G.; Galati, G.; Patria, F. Psychophysical properties of line bisection and body midline perception in unilateral neglect. Cortex 2000, 36, 469–484. [Google Scholar] [CrossRef]
- Iosa, M.; Guariglia, C.; Matano, A.; Paolucci, S.; Pizzamiglio, L. Recovery of personal neglect. Eur. J. Phys. Rehabil. Med. 2016, 52, 791–798. [Google Scholar]
- Rousseaux, M.; Honoré, J.; Vuilleumier, P.; Saj, A. Neuroanatomy of space, body, and posture perception in patients with right hemisphere stroke. Neurology 2013, 81, 1291–1297. [Google Scholar] [CrossRef]
- Fabri, M.; Polonara, G.; Mascioli, G.; Paggi, A.; Salvolini, U.; Manzoni, T. Contribution of the corpus callosum to bilateral representation of the trunk midline in the human brain: An fMRI study of callosotomized patients. Eur. J. Neurosci. 2006, 23, 3139–3148. [Google Scholar] [CrossRef]
- Ceyte, H.; Cian, C.; Nougier, V.; Olivier, I.; Trousselard, M. Role of gravity-based information on the orientation and localization of the perceived body midline. Exp. Brain Res. 2007, 176, 504–509. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| YG (n = 15) | EG (n = 15) | PG (n = 15) | KW Analysis | PG vs. EG | |
|---|---|---|---|---|---|
| Age (years) | 24.7 ± 3.2 | 57.2 ± 9.1 | 60.3 ± 10.4 | p < 0.001 | 0.267 |
| Stature (cm) | 169.0 ± 9.0 | 169.7 ± 7.4 | 173.9 ± 10.5 | p = 0.268 | 0.174 |
| Body Weight (kg) | 60.9 ± 10.8 | 72.9 ± 19.5 | 75.2 ± 14.5 | p = 0.021 | 0.436 |
| BMI (m2/kg) | 17.9 ± 2.5 | 21.4 ± 5.0 | 21.5 ± 3.2 | p = 0.016 | 0.653 |
| Condition | Parameter | YG (n = 15) | EG (n = 15) | PG L (n = 6) | PG R (n = 9) | p-Value 3 Groups | p-Value 4 Groups |
|---|---|---|---|---|---|---|---|
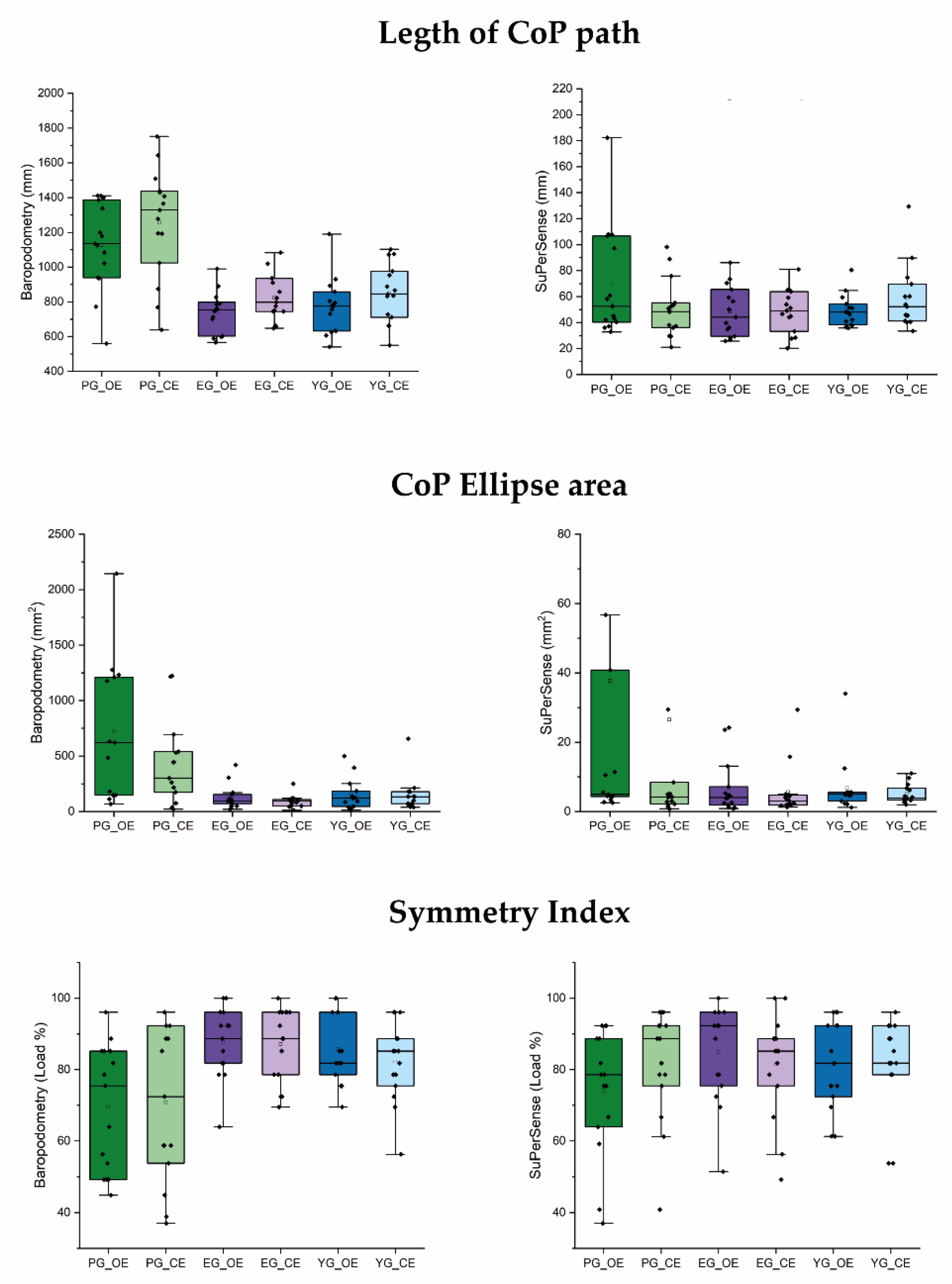
| Baropodometry | CoP Path length (mm) | 770 ± 162 | 741± 118 | 1098 ± 301 | 1145 ± 231 | <0.001 | <0.001 |
| Open Eyes | CoP Ellipse Area (mm2) | 211 ± 235 | 238 ± 295 | 523 ± 411 | 788 ± 706 | 0.004 | 0.006 |
| Symmetry Index (%) | 86 ± 10 | 88 ± 10 | 73 ± 22 | 69 ± 18 | 0.002 | 0.005 | |
| Baropodometry | CoP Path length (mm) | 851 ± 166 | 823 ± 132 | 1159 ± 355 | 1320 ± 288 | <0.001 | <0.001 |
| Closed Eyes | CoP Ellipse Area (mm2) | 156 ± 150 | 177 ± 334 | 318 ± 250 | 458 ± 461 | 0.063 | 0.102 |
| Symmetry Index (%) | 82 ± 11 | 87 ± 10 | 78 ± 20 | 66 ± 22 | 0.017 | 0.018 | |
| SuperSense | CoP Path length (mm) | 49 ± 12 | 48 ± 19 | 53 ± 24 | 81 ± 49 | 0.061 | 0.023 |
| Open Eyes | CoP Ellipse Area (mm2) | 7 ± 8 | 7 ± 7 | 6 ± 4 | 59 ± 86 | 0.071 | 0.010 |
| Symmetry Index (%) | 82 ± 12 | 85 ± 13 | 68 ± 18 | 78 ± 17 | 0.137 | 0.115 | |
| SuperSense | CoP Path length (mm) | 59 ± 25 | 49 ± 17 | 54 ± 21 | 46 ± 24 | 0.410 | 0.527 |
| Closed Eyes | CoP Ellipse Area (mm2) | 5 ± 3 | 6 ± 7 | 3 ± 1 | 42 ± 78 | 0.190 | 0.054 |
| Symmetry Index (%) | 82 ± 13 | 81 ± 15 | 80 ± 23 | 83 ± 9 | 0.997 | 0.981 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Bartolo, D.; D’amico, I.; Iosa, M.; Aloise, F.; Morone, G.; Marinozzi, F.; Bini, F.; Paolucci, S.; Spadini, E. Validation of SuPerSense, a Sensorized Surface for the Evaluation of Posture Perception in Supine Position. Sensors 2023, 23, 424. https://doi.org/10.3390/s23010424
De Bartolo D, D’amico I, Iosa M, Aloise F, Morone G, Marinozzi F, Bini F, Paolucci S, Spadini E. Validation of SuPerSense, a Sensorized Surface for the Evaluation of Posture Perception in Supine Position. Sensors. 2023; 23(1):424. https://doi.org/10.3390/s23010424
Chicago/Turabian StyleDe Bartolo, Daniela, Ilaria D’amico, Marco Iosa, Fabio Aloise, Giovanni Morone, Franco Marinozzi, Fabiano Bini, Stefano Paolucci, and Ennio Spadini. 2023. "Validation of SuPerSense, a Sensorized Surface for the Evaluation of Posture Perception in Supine Position" Sensors 23, no. 1: 424. https://doi.org/10.3390/s23010424