
Assessment of Features between Multichannel Electrohysterogram for Differentiation of Labors


Abstract
:1. Introduction
2. Materials and Methods
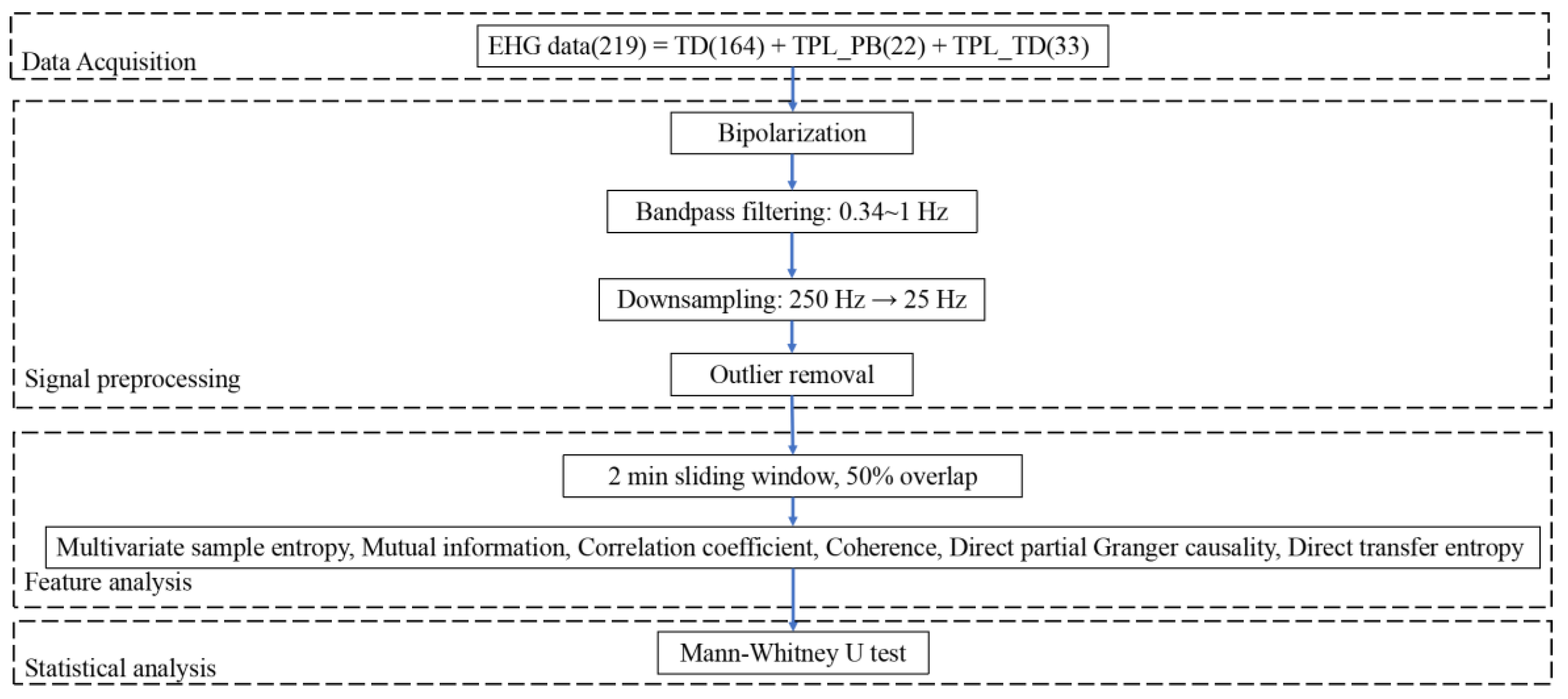
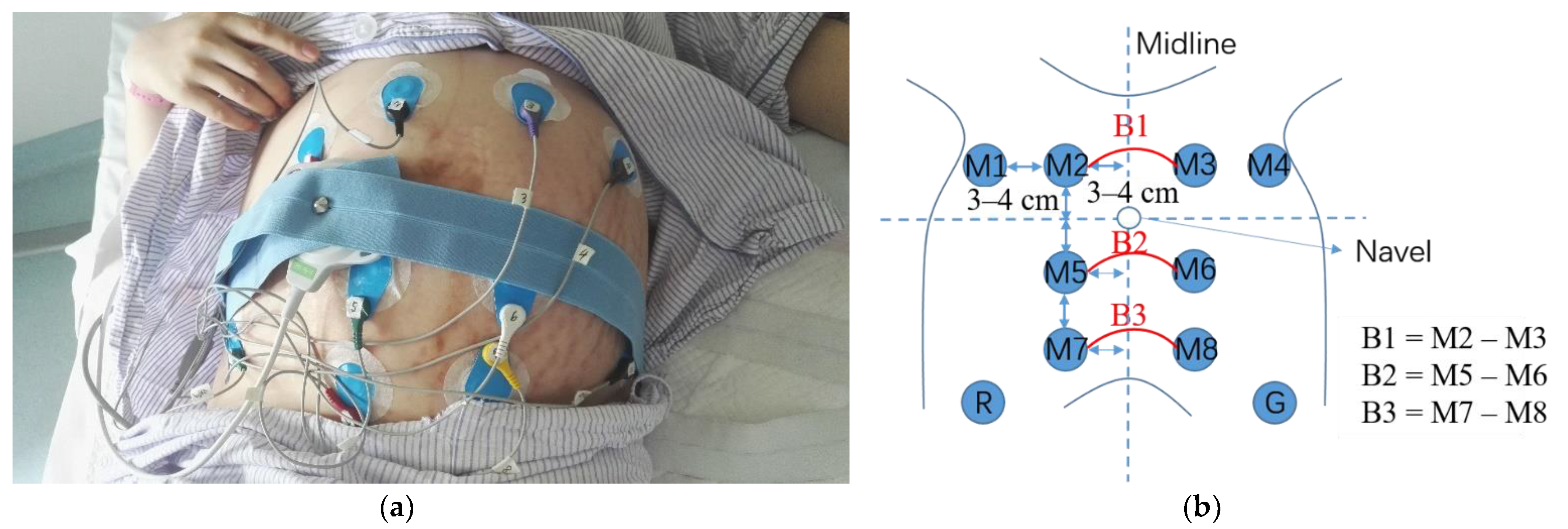
2.1. Data Acquisition
2.2. Signal Preprocessing
2.3. Feature Extraction
2.3.1. Multivariate Sample Entropy
- Create N − n (n = max{M} × max{T}) composite delay vector , where i = 1, 2, …, N − n. Compute the distance between any two composite delay vectors as the maximum of the following form:
- For a given composite delay vector and an assumed similarity threshold r, count the number of instances where , then calculate the frequency of occurrence,and define a global quantity,
- Extend the dimensionality of the multivariate delay composite vector from m to m + 1. For a given vector , calculate the number of vectors such that , then calculate the frequency of occurrence,and define
- The multivariate sample entropy is calculated as
2.3.2. Mutual Information
2.3.3. Correlation Coefficient
2.3.4. Coherence
2.3.5. Partial Granger Causality
2.3.6. Transfer Entropy
2.4. Statistical Method
3. Results
3.1. Comparison of Features between TD, TPL_PB, and TPL_TD
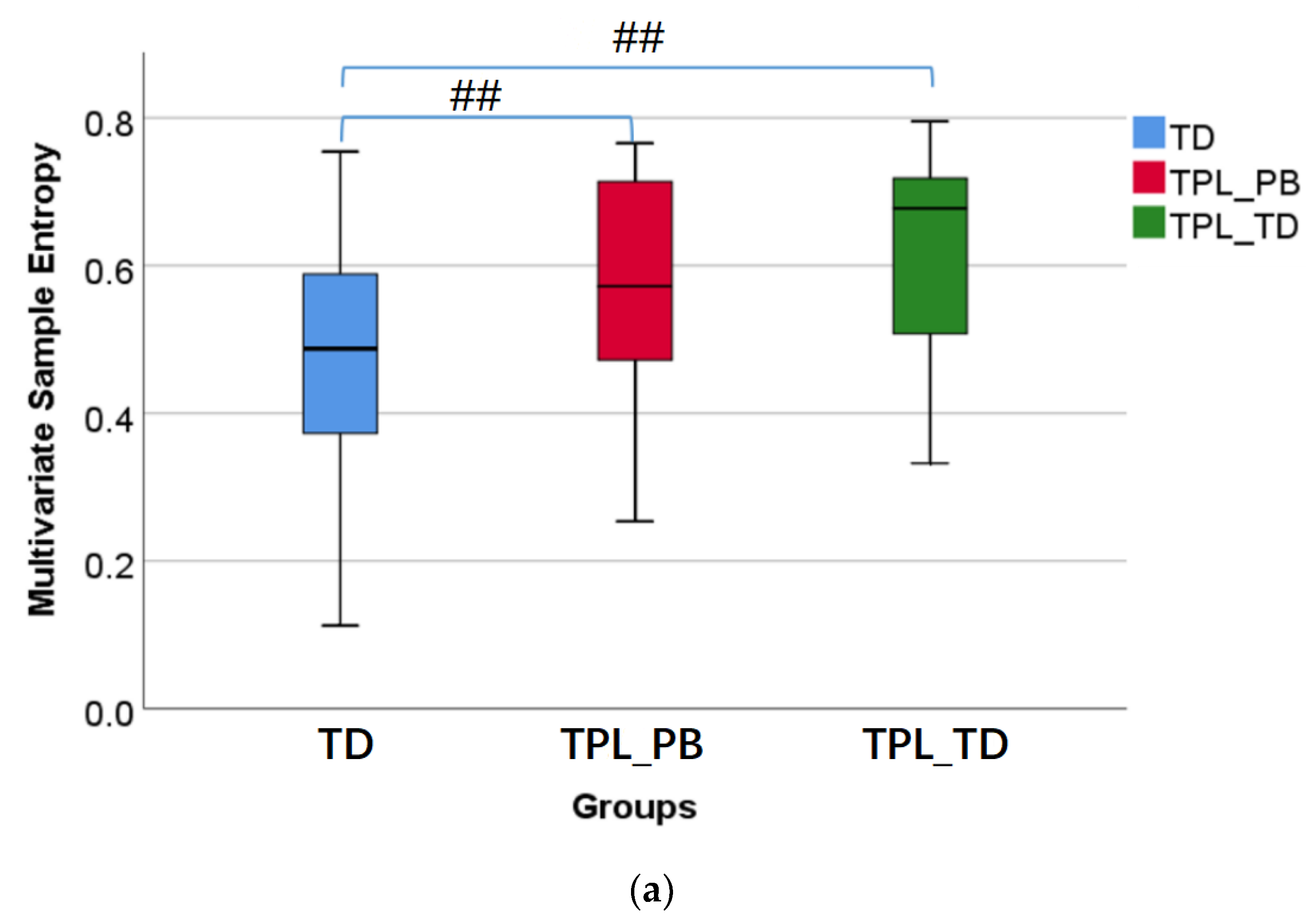
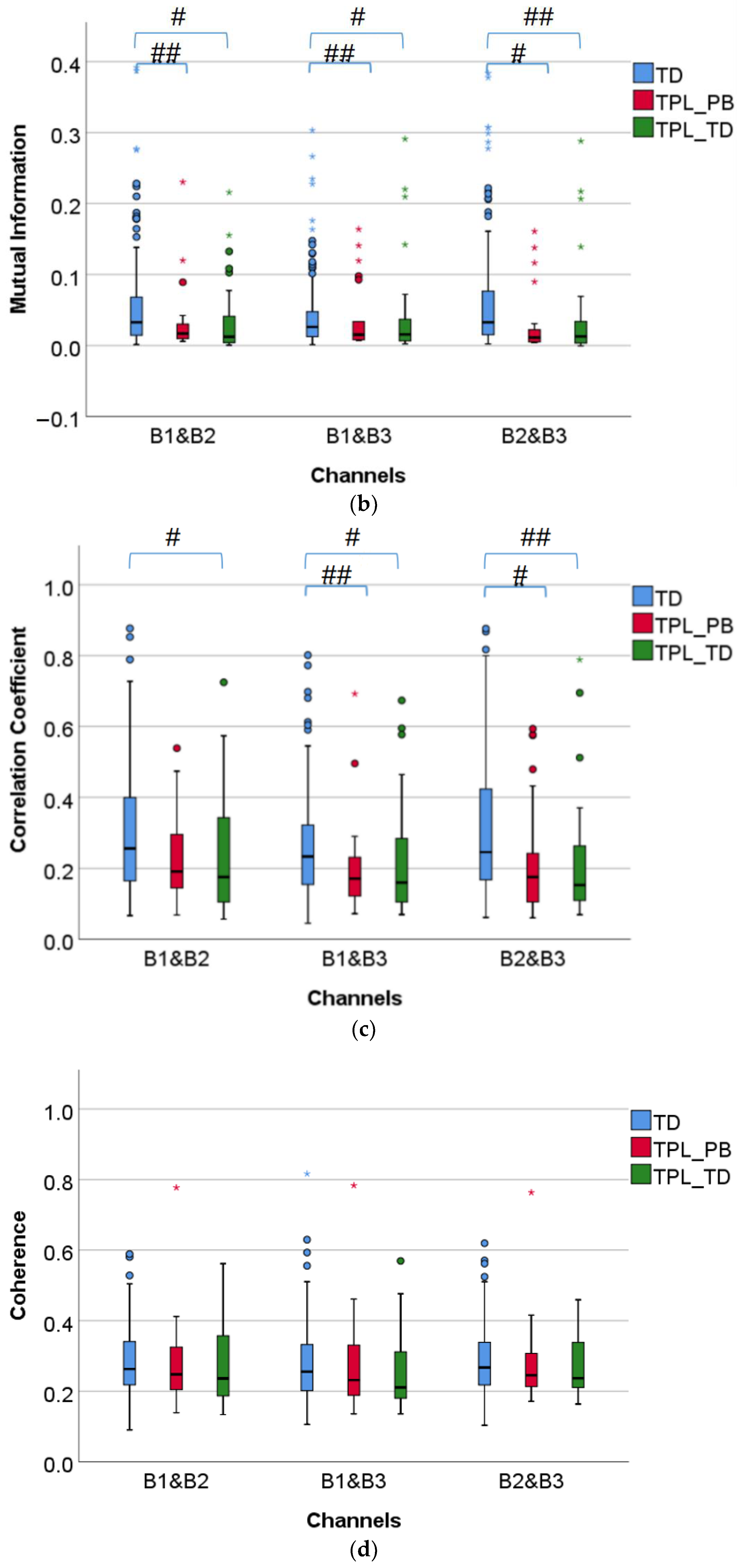
3.1.1. Comparison of Multivariate Sample Entropy, Mutual Information, Correlation Coefficient, and Coherence
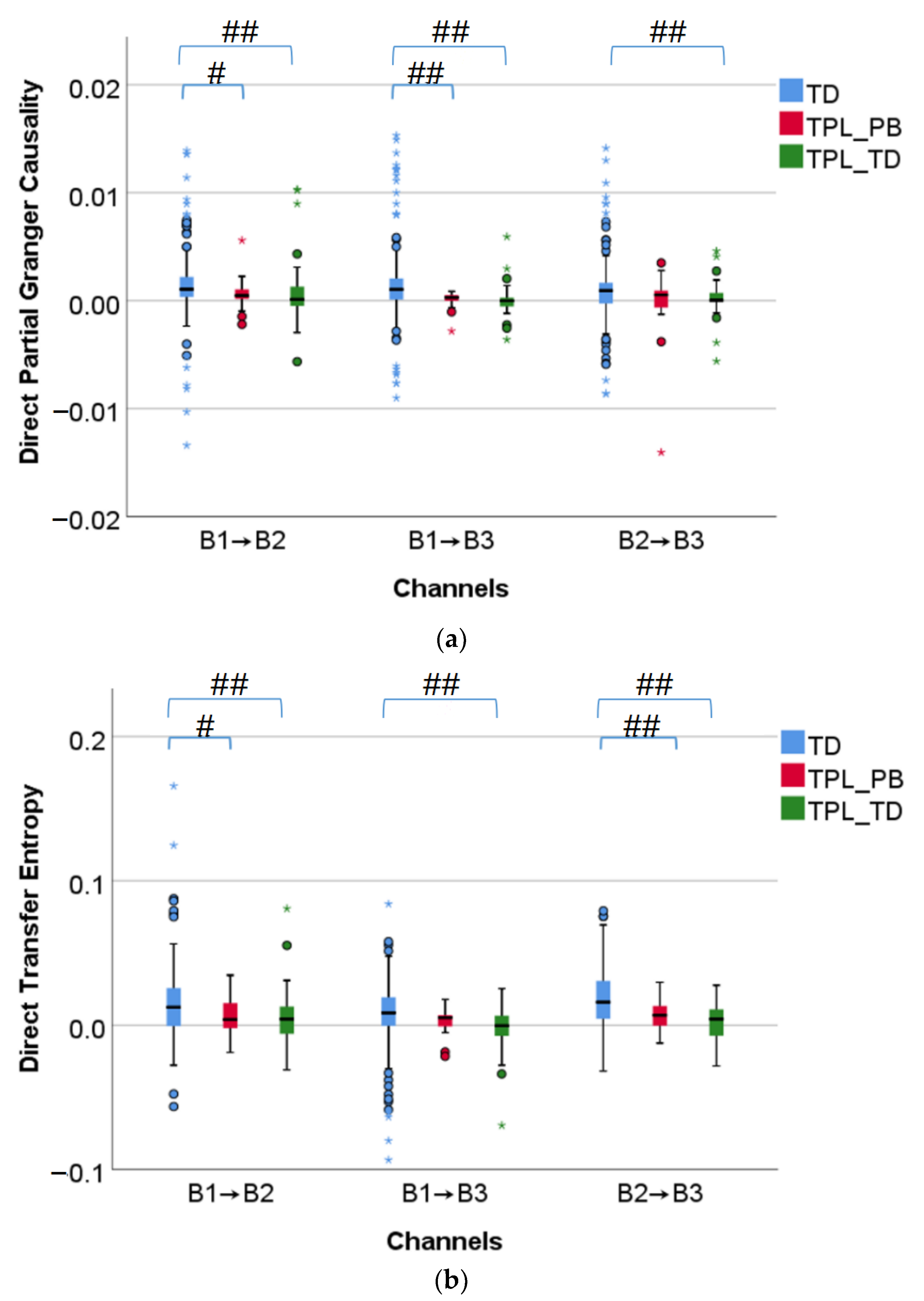
3.1.2. Comparison of Direct Partial Granger Causality and Direct Transfer Entropy
3.2. Comparison of Features between TTD ≤ 24 h and TTD > 24 h
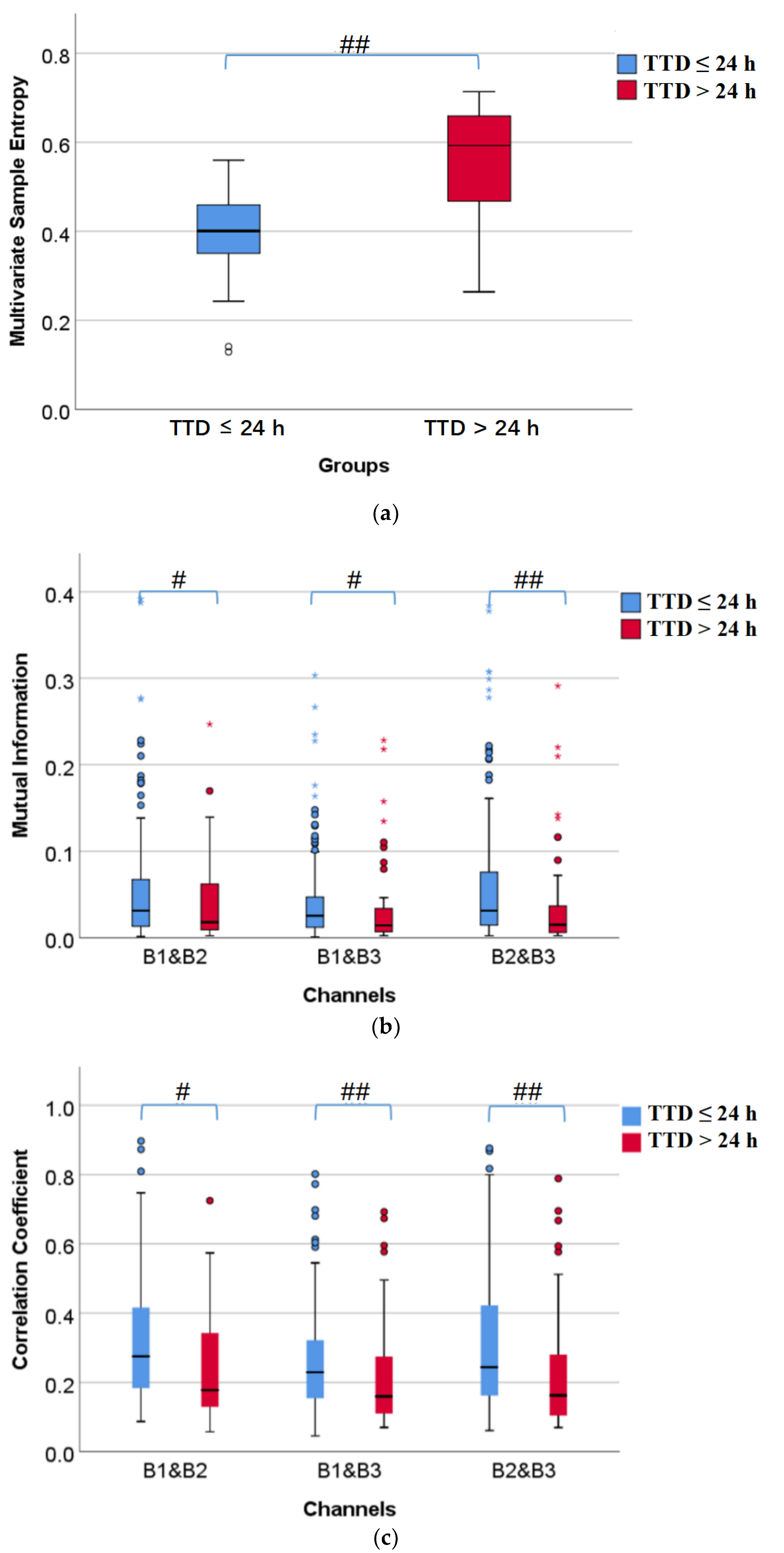
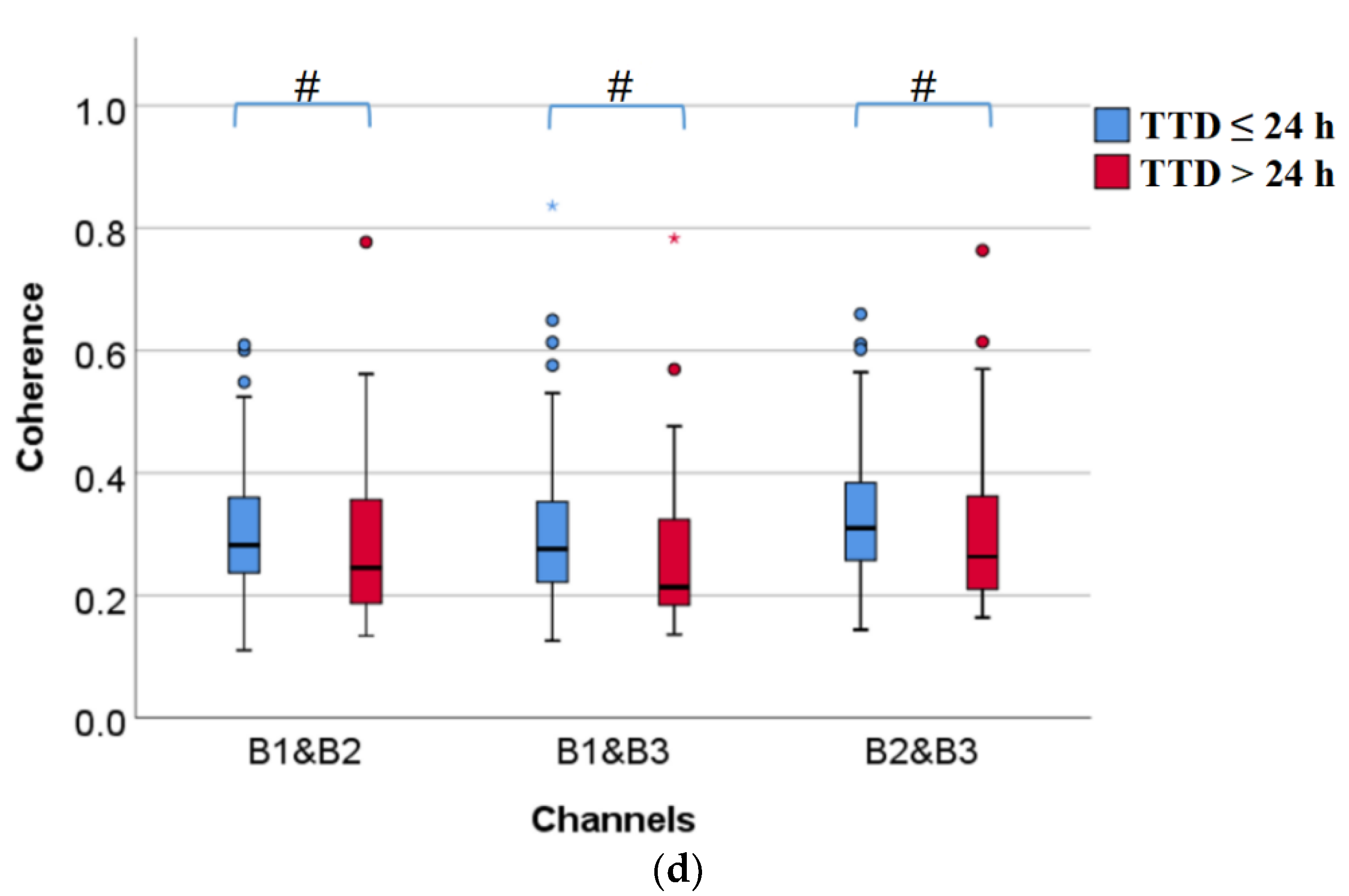
3.2.1. Comparison of Multivariate Sample Entropy, Mutual Information, Correlation Coefficient, and Coherence
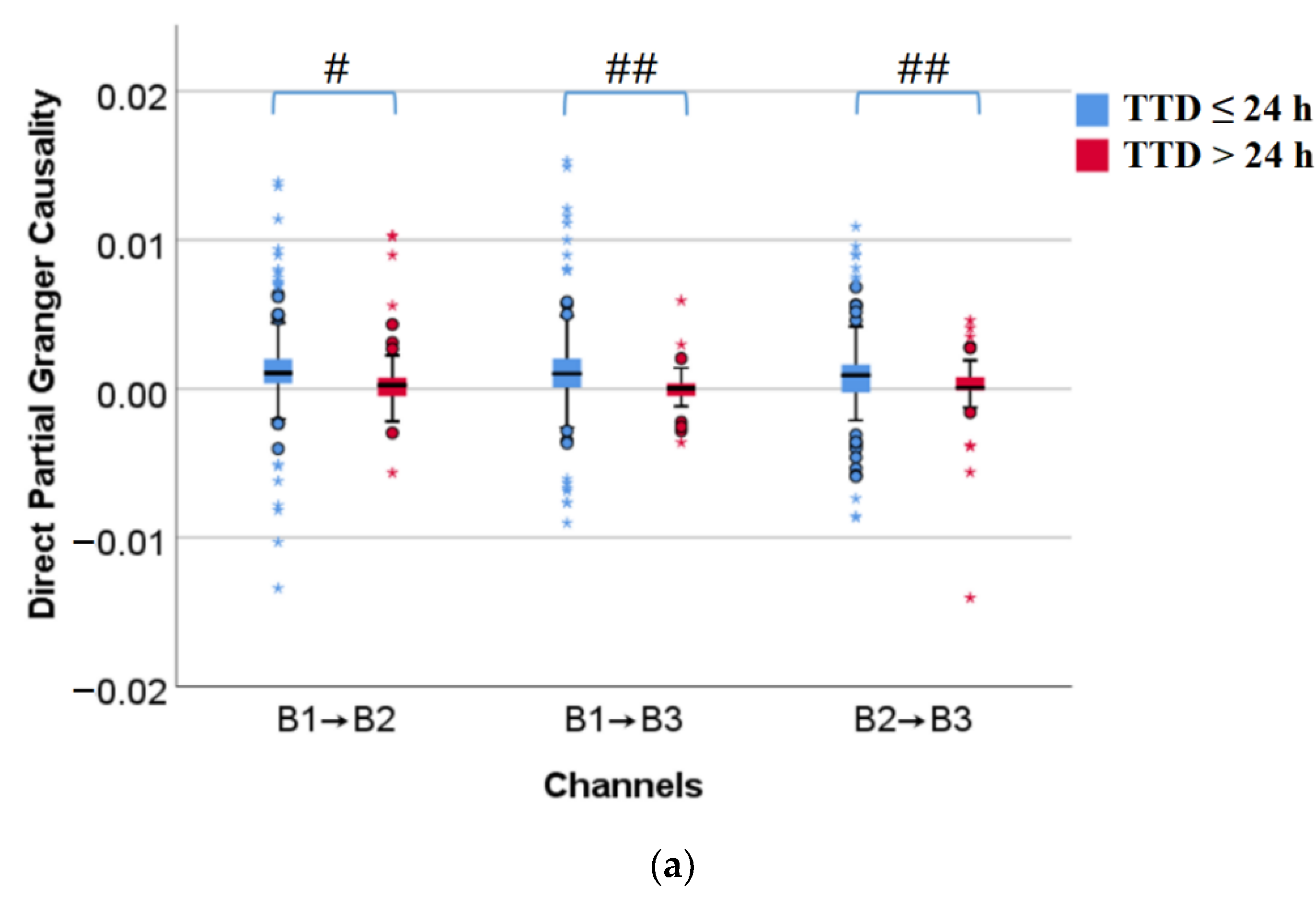
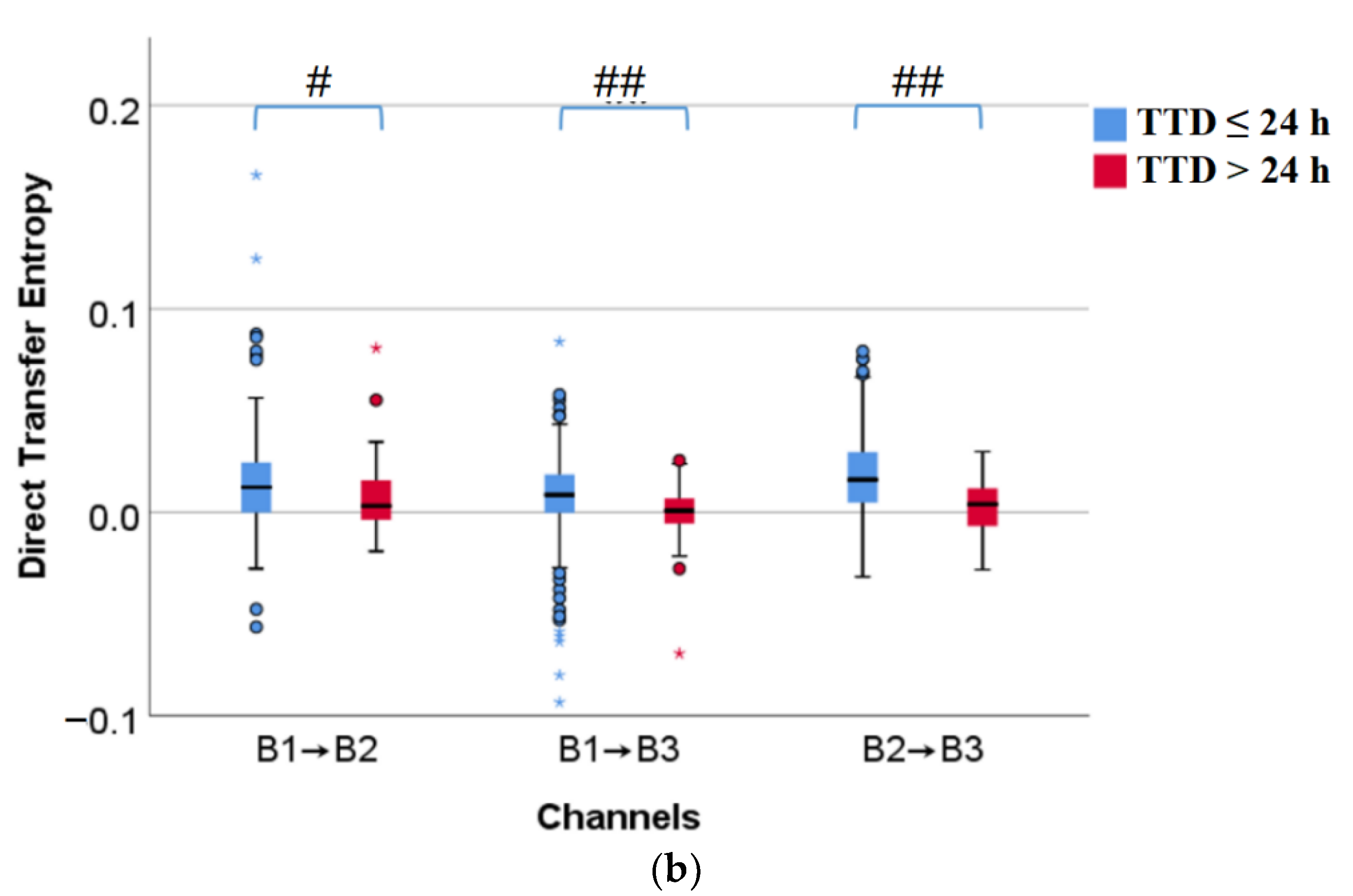
3.2.2. Comparison of Direct Partial Granger Causality and Direct Transfer Entropy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mas-Cabo, J.; Prats-Boluda, G.; Garcia-Casado, J.; Alberola-Rubio, J.; Perales, A.; Ye-Lin, Y. Design and Assessment of a Robust and Generalizable ANN-Based Classifier for the Prediction of Premature Birth by means of Multichannel Electrohysterographic Records. J. Sens. 2019, 2019, 5373810. [Google Scholar] [CrossRef]
- Lewis, M.; Passant, L.; Cooke, H.; Challis, D. Women’s experiences of antenatal transfer for threatened premature labour in NSW: A qualitative study. Women Birth 2020, 33, E535–E542. [Google Scholar] [CrossRef]
- Euliano, T.Y.; Minh, T.N.; Darmanjian, S.; McGorray, S.P.; Euliano, N.; Onkala, A.; Gregg, A.R. Monitoring uterine activity during labor: A comparison of 3 methods. Am. J. Obstet. Gynecol. 2013, 208, 66.e1–66.e6. [Google Scholar] [CrossRef] [Green Version]
- Garfield, R.E.; Maner, W.L. Biophysical methods of prediction and prevention of preterm labor: Uterine electromyography and cervical light-induced fluorescence—New obstetrical diagnostic techniques. In Preterm Birth; CRC Press: Boca Raton, FL, USA, 2006; pp. 131–144. [Google Scholar]
- Garcia-Casado, J.; Ye-Lin, Y.; Prats-Boluda, G.; Mas-Cabo, J.; Alberola-Rubio, J.; Perales, A. Electrohysterography in the diagnosis of preterm birth: A review. Physiol. Meas. 2018, 39, 02TR01. [Google Scholar] [CrossRef]
- Mas-Cabo, J.; Prats-Boluda, G.; Garcia-Casado, J.; Alberola-Rubio, J.; Monfort-Ortiz, R.; Martinez-Saez, C.; Perales, A.; Ye-Lin, Y. Electrohysterogram for ANN-Based Prediction of Imminent Labor in Women with Threatened Preterm Labor Undergoing Tocolytic Therapy. Sensors 2020, 20, 2681. [Google Scholar] [CrossRef]
- Hao, D.; Peng, J.; Wang, Y.; Liu, J.; Zhou, X.; Zheng, D. Evaluation of convolutional neural network for recognizing uterine contractions with electrohysterogram. Comput. Biol. Med. 2019, 113, 103394. [Google Scholar] [CrossRef]
- Song, X.; Qiao, X.; Hao, D.; Yang, L.; Zhou, X.; Xu, Y.; Zheng, D. Automatic recognition of uterine contractions with electrohysterogram signals based on the zero-crossing rate. Sci. Rep. 2021, 11, 1956. [Google Scholar] [CrossRef]
- Ahmed, M.U.; Chanwimalueang, T.; Thayyil, S.; Mandic, D.P. A Multivariate Multiscale Fuzzy Entropy Algorithm with Application to Uterine EMG Complexity Analysis. Entropy 2017, 19, 2. [Google Scholar] [CrossRef] [Green Version]
- Devedeux, D.; Marque, C.; Mansour, S.; Germain, G.; Duchêne, J. Uterine electromyography: A critical review. Am. J. Obstet. Gynecol. 1993, 169, 1636–1653. [Google Scholar] [CrossRef]
- Chkeir, A.; Fleury, M.-J.; Karlsson, B.; Hassan, M.; Marque, C. Patterns of electrical activity synchronization in the pregnant rat uterus. BioMedicine 2013, 3, 140–144. [Google Scholar] [CrossRef]
- Jager, F.; Libensek, S.; Gersak, K. Characterization and automatic classification of preterm and term uterine records. PLoS ONE 2018, 13, e0202125. [Google Scholar] [CrossRef] [Green Version]
- Mischi, M.; Chen, C.; Ignatenko, T.; de Lau, H.; Ding, B.; Oei, S.G.G.; Rabotti, C. Dedicated Entropy Measures for Early Assessment of Pregnancy Progression from Single-Channel Electrohysterography. IEEE Tran. Biomed. Eng. 2018, 65, 875–884. [Google Scholar] [CrossRef] [PubMed]
- You, J.; Kim, Y.; Seok, W.; Lee, S.; Sim, D.; Park, K.S.; Park, C. Multivariate Time-Frequency Analysis of Electrohysterogram for Classification of Term and Preterm Labor. J. Electr. Eng. Technol. 2019, 14, 897–916. [Google Scholar] [CrossRef]
- Naeem, S.M.; Seddik, A.F.; Eldosoky, M.A. New technique based on uterine electromyography nonlinearity for preterm delivery detection. J. Eng. Technol. Res. 2014, 6, 107–114. [Google Scholar]
- Mas-Cabo, J.; Ye-Lin, Y.; Garcia-Casado, J.; Alberola-Rubio, J.; Perales, A.; Prats-Boluda, G. Uterine contractile efficiency indexes for labor prediction: A bivariate approach from multichannel electrohysterographic records. Biomed. Signal. Proces. 2018, 46, 238–248. [Google Scholar] [CrossRef]
- Radomski, D.S. A nonlinear parameterization of multivariate electrohysterographical signals. Comput. Biol. Med. 2015, 67, 13–20. [Google Scholar] [CrossRef]
- Radomski, D.S. Reprint of ‘A nonlinear parameterization of multivariate electrohysterographical signals’. Comput. Biol. Med. 2016, 69, 254–260. [Google Scholar] [CrossRef]
- Rabotti, C.; Mischi, M. Propagation of electrical activity in uterine muscle during pregnancy: A review. Acta Physiol. 2015, 213, 406–416. [Google Scholar] [CrossRef]
- Garfield, R.E.; Murphy, L.; Gray, K.; Towe, B. Review and Study of Uterine Bioelectrical Waveforms and Vector Analysis to Identify Electrical and Mechanosensitive Transduction Control Mechanisms During Labor in Pregnant Patients. Reprod. Sci. 2021, 28, 838–856. [Google Scholar] [CrossRef]
- Mikkelsen, E.; Johansen, P.; Fuglsang-Frederiksen, A.; Uldbjerg, N. Electrohysterography of labor contractions: Propagation velocity and direction. Acta Obstet. Gyn. Scan. 2013, 92, 1070–1078. [Google Scholar] [CrossRef]
- Lange, L.; Vaeggemose, A.; Kidmose, P.; Mikkelsen, E.; Uldbjerg, N.; Johansen, P. Velocity and Directionality of the Electrohysterographic Signal Propagation. PLoS ONE 2014, 9, e86775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Hao, D.; Zheng, D. Analysis of Electrohysterographic Signal Propagation Direction during Uterine Contraction: The Application of Directed Information. In Proceedings of the 42nd Annual International Conferences of the IEEE Engineering in Medicine and Biology Society: Enabling Innovative Technologies for Global Healthcare (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 21–25. [Google Scholar]
- Ye-Lin, Y.; Garcia-Casado, J. Automatic identification of motion artifacts in EHG recording for robust analysis of uterine contractions. Comput. Math. Methods Med. 2014, 2014, 470786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hao, D.; An, Y.; Qiao, X.; Qiu, Q.; Zhou, X.; Peng, J. Development of Electrohysterogram Recording System for Monitoring Uterine Contraction. J. Healthc. Eng. 2019, 2019, 4230157. [Google Scholar] [CrossRef] [PubMed]
- David, L.; Tricia, A.; Danilo, M. A Novel Multivariate Sample Entropy Algorithm for Modeling Time Series Synchronization. Entropy 2018, 20, 82. [Google Scholar]
- Yao, C.Z.; Lin, Q.W.; Lin, J.N. A study of industrial electricity consumption based on partial Granger causality network. Phys. A Stat. Mech. Appl. 2016, 461, 629–646. [Google Scholar] [CrossRef]
- Ahmed, M.U.; Mandic, D.P. Multivariate Multiscale Entropy Analysis. IEEE Signal Processing Lett. 2012, 19, 91–94. [Google Scholar] [CrossRef] [Green Version]
- Guo, S.; Seth, A.K.; Kendrick, K.M. Partial Granger causality—Eliminating exogenous inputs and latent variables. J. Neurosci. Methods 2008, 172, 79–93. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Nemati, S.; Silva, I.; Edwards, B.A.; Butler, J.P.; Malhotra, A. Transfer Entropy Estimation and Directional Coupling Change Detection in Biomedical Time Series. Biomed. Eng. Online 2012, 11, 19. [Google Scholar] [CrossRef] [Green Version]
- Rozo, A.; Morales, J.; Moeyersons, J. Benchmarking Transfer Entropy Methods for the Study of Linear and Nonlinear Cardio-Respiratory Interactions. Entropy 2021, 23, 939. [Google Scholar] [CrossRef]
- Fele-Zorz, G.; Kavsek, G.; Novak-Antolic, Z.; Jager, F. A comparison of various linear and non-linear signal processing techniques to separate uterine EMG records of term and pre-term delivery groups. Med. Biol. Eng. Comput. 2008, 46, 911–922. [Google Scholar] [CrossRef]
- Mas-Cabo, J.; Prats-Boluda, G.; Ye-Lin, Y.; Alberola-Rubio, J.; Perales, A.; Garcia-Casado, J. Characterization of the effects of Atosiban on uterine electromyograms recorded in women with threatened preterm labor. Biomed. Signal. Proces. 2019, 52, 198–205. [Google Scholar] [CrossRef]
- Degbedzui, D.K.; Yuksel, M.E. Accurate diagnosis of term-preterm births by spectral analysis of electrohysterography signals. Comput. Biol. Med. 2020, 119, 103677. [Google Scholar] [CrossRef] [PubMed]
- Borowska, M.; Brzozowska, E.; Kuc, P.; Oczeretko, E.; Mosdorf, R.; Laudanski, P. Identification of preterm birth based on RQA analysis of electrohysterograms. Comput. Methods Programs Biomed. 2018, 153, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.; Terrien, J.; Alexandersson, A.; Marque, C.; Karlsson, B. Improving the classification rate of labor vs. normal pregnancy contractions by using EHG multichannel recordings. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Buenos Aires, Argentina, 31 August–4 September 2010; pp. 4642–4645. [Google Scholar]
- Nader, N.; Hassan, M.; Falou, W.; Diab, A.; Al-Omar, S.; Khalil, M.; Marque, C. Classification of pregnancy and labor contractions using a graph theory based analysis. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milano, Italy, 25–29 August 2015; pp. 2876–2879. [Google Scholar]
- Acharya, U.R.; Sudarshan, V.K.; Rong, S.Q.; Tan, Z.; Lim, C.M.; Koh, J.E.W.; Nayak, S.; Bhandary, S.V. Automated detection of premature delivery using empirical mode and wavelet packet decomposition techniques with uterine electromyogram signals. Comput. Biol. Med. 2017, 85, 33–42. [Google Scholar] [CrossRef]
- Ren, P.; Yao, S.; Li, J.; Valdes-Sosa, P.A.; Kendrick, K.M. Improved Prediction of Preterm Delivery Using Empirical Mode Decomposition Analysis of Uterine Electromyography Signals. PLoS ONE 2015, 10, e0132116. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Ouyang, C.; Chiang, C.; Wu, R.; Wu, H.; Yang, R. Cumulative Effect of Transcranial Direct Current Stimulation in Patients with Refractory Epilepsy and its Association with Phase Lag Index-A Preliminary Study. Epilepsia 2018, 593, S54. [Google Scholar] [CrossRef]
- Cohen, M.X. Effects of time lag and frequency matching on phase-based connectivity. J. Neurosci. Methods 2015, 250, 137–146. [Google Scholar] [CrossRef]
- Rabotti, C.; Mischi, M.; van Laar, J.O.E.H.; Oei, G.S.; Bergmans, J.W.M. Inter-electrode delay estimators for electrohysterographic propagation analysis. Physiol. Meas. 2009, 30, 745–761. [Google Scholar] [CrossRef]
- Escalona-Vargas, D.; Govindan, R.B.; Furdea, A.; Murphy, P.; Lowery, C.L.; Eswaran, H. Characterizing the Propagation of Uterine Electrophysiological Signals Recorded with a Multi-Sensor Abdominal Array in Term Pregnancies. PLoS ONE 2015, 10, e0140894. [Google Scholar] [CrossRef]
- Jager, F.; Gersak, K.; Vouk, P.; Pirnar, Z.; Trojner-Bregar, A.; Lucovnik, M.; Borovac, A. Assessing Velocity and Directionality of Uterine Electrical Activity for Preterm Birth Prediction Using EHG Surface Records. Sensors 2020, 20, 7328. [Google Scholar] [CrossRef]
- Diab, A.; Hassan, M.; Boudaoud, S.; Marque, C.; Karlsson, B. Nonlinear estimation of coupling and directionality between signals: Application to uterine EMG propagation. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 4366–4369. [Google Scholar]
- Horoba, K.; Jezewski, J.; Wrobel, J.; Matonia, A.; Czabanski, R.; Jezewski, M. Analysis of Uterine Contractile Wave Propagation in Electrohysterogram for Assessing the Risk of Preterm Birth. J. Med. Image Health 2015, 5, 1287–1294. [Google Scholar] [CrossRef]
- Planque, S. Contribution a L’etude de la Propagation du Signal Electrohysterographique. Ph.D. Thesis, Génie Biomedical Compiegne, Universite de technologie de Compiegne, Compiègne, France, 1990. [Google Scholar]
- Lammers, W.J.E.P.; Mirghani, H.; Stephen, B.; Dhanasekaran, S.; Wahab, A.; Al Sultan, M.A.H.; Abazer, F. Patterns of electrical propagation in the intact pregnant guinea pig uterus. Am. J. Physiol.-Reg. I 2008, 294, R919–R928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieto-del-Amor, F.; Prats-Boluda, G.; Martinez-De-Juan, J.L.; Diaz-Martinez, A.; Monfort-Ortiz, R.; Jose Diago-Almela, V.; Ye-Lin, Y. Optimized Feature Subset Selection Using Genetic Algorithm for Preterm Labor Prediction Based on Electrohysterography. Sensors 2021, 21, 3350. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TTD | ≤24 h | >24 h | Totalrow | |
|---|---|---|---|---|
| Group | ||||
| TD | 164 | 0 | 164 | |
| TPL_PB | 7 | 15 | 22 | |
| TPL_TD | 0 | 33 | 33 | |
| Totalcolumn | 171 | 48 | 219 | |
| Feature | Group | EHG Propagation | Totalrow | |
|---|---|---|---|---|
| Upward | Downward | |||
| Direct partial Granger causality | TD | 29 (18%) | 135 (82%) | 164 |
| TPL_PB | 7 (32%) | 15 (68%) | 22 | |
| TPL_TD | 11 (33%) | 22 (67%) | 33 | |
| Totalcolumn | 47 | 172 | 219 | |
| Direct transfer entropy | TD | 52 (32%) | 112 (68%) | 164 |
| TPL_PB | 8 (36%) | 14 (64%) | 22 | |
| TPL_TD | 15 (45%) | 18 (55%) | 33 | |
| Totalcolumn | 75 | 144 | 219 | |
| Feature | Group | EHG Propagation | Totalrow | |
|---|---|---|---|---|
| Upward | Downward | |||
| Direct partial Granger causality | TTD ≤ 24 h | 33 (19%) | 138 (81%) | 171 |
| TTD > 24 h | 14 (29%) | 34 (71%) | 48 | |
| Totalcolumn | 47 | 172 | 219 | |
| Direct transfer entropy | TTD ≤ 24 h | 58 (34%) | 113 (66%) | 171 |
| TTD > 24 h | 17 (35%) | 31 (65%) | 48 | |
| Totalcolumn | 75 | 144 | 219 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Hao, D.; Yang, L.; Zhou, X.; Ye-Lin, Y.; Yang, Y. Assessment of Features between Multichannel Electrohysterogram for Differentiation of Labors. Sensors 2022, 22, 3352. https://doi.org/10.3390/s22093352
Zhang Y, Hao D, Yang L, Zhou X, Ye-Lin Y, Yang Y. Assessment of Features between Multichannel Electrohysterogram for Differentiation of Labors. Sensors. 2022; 22(9):3352. https://doi.org/10.3390/s22093352
Chicago/Turabian StyleZhang, Yajun, Dongmei Hao, Lin Yang, Xiya Zhou, Yiyao Ye-Lin, and Yimin Yang. 2022. "Assessment of Features between Multichannel Electrohysterogram for Differentiation of Labors" Sensors 22, no. 9: 3352. https://doi.org/10.3390/s22093352