
Muscle Mass Measurement Using Machine Learning Algorithms with Electrical Impedance Myography

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
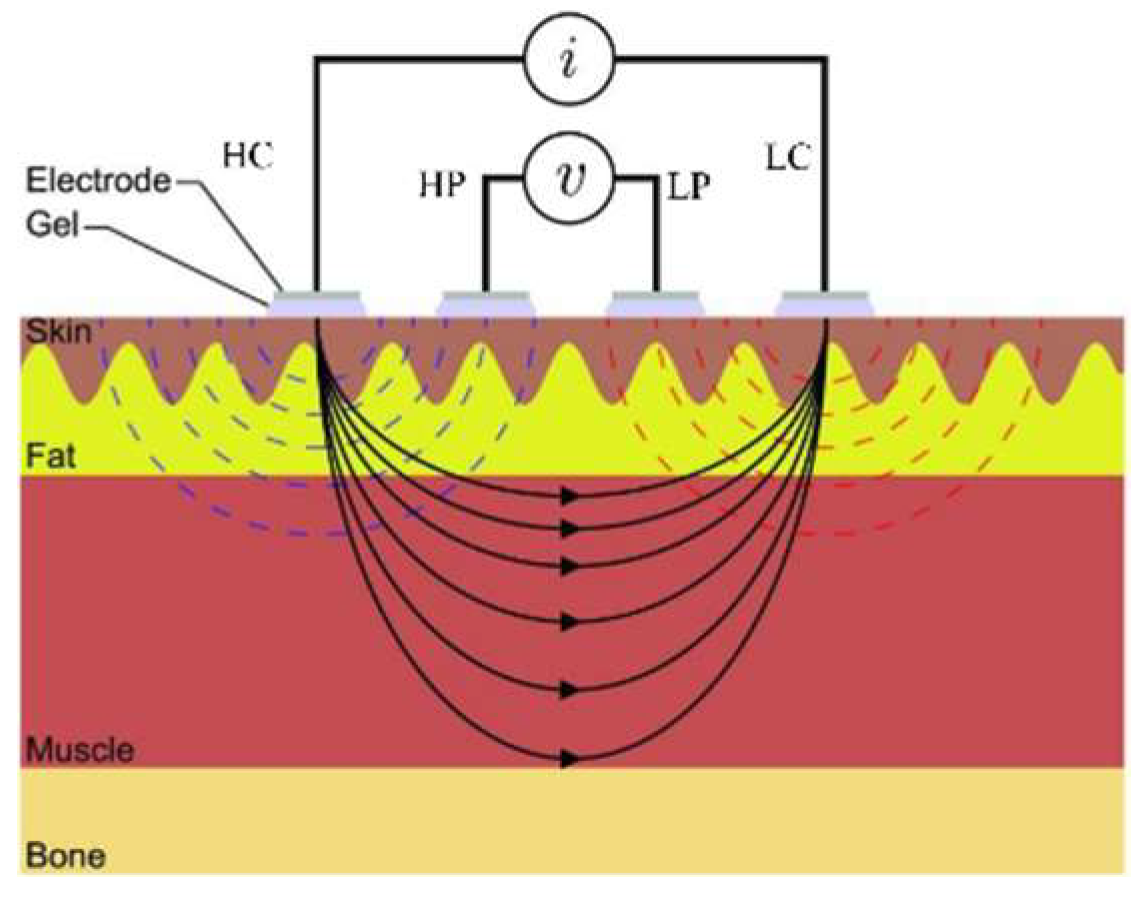
2.1. EIM Measurement System
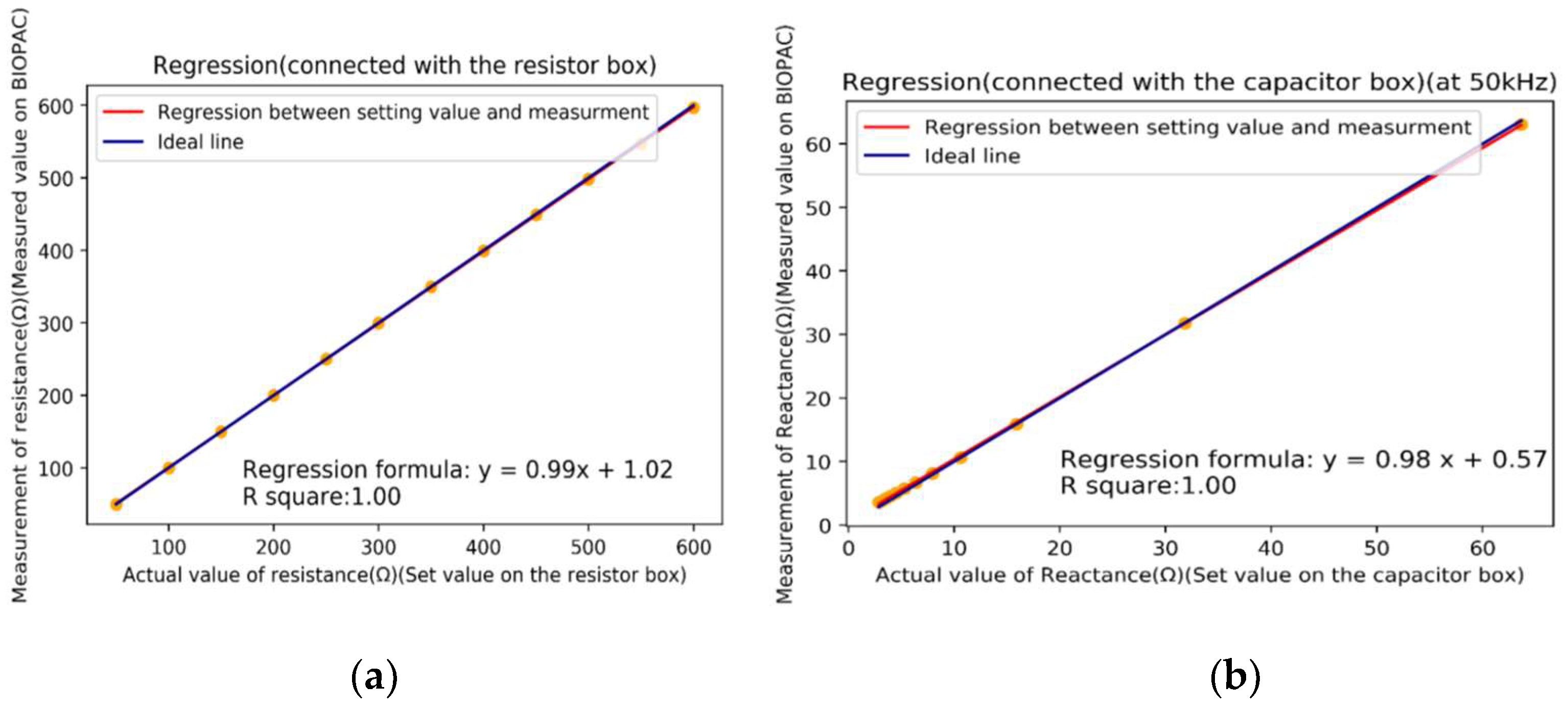
2.1.1. Calibration of EIM Measurement System
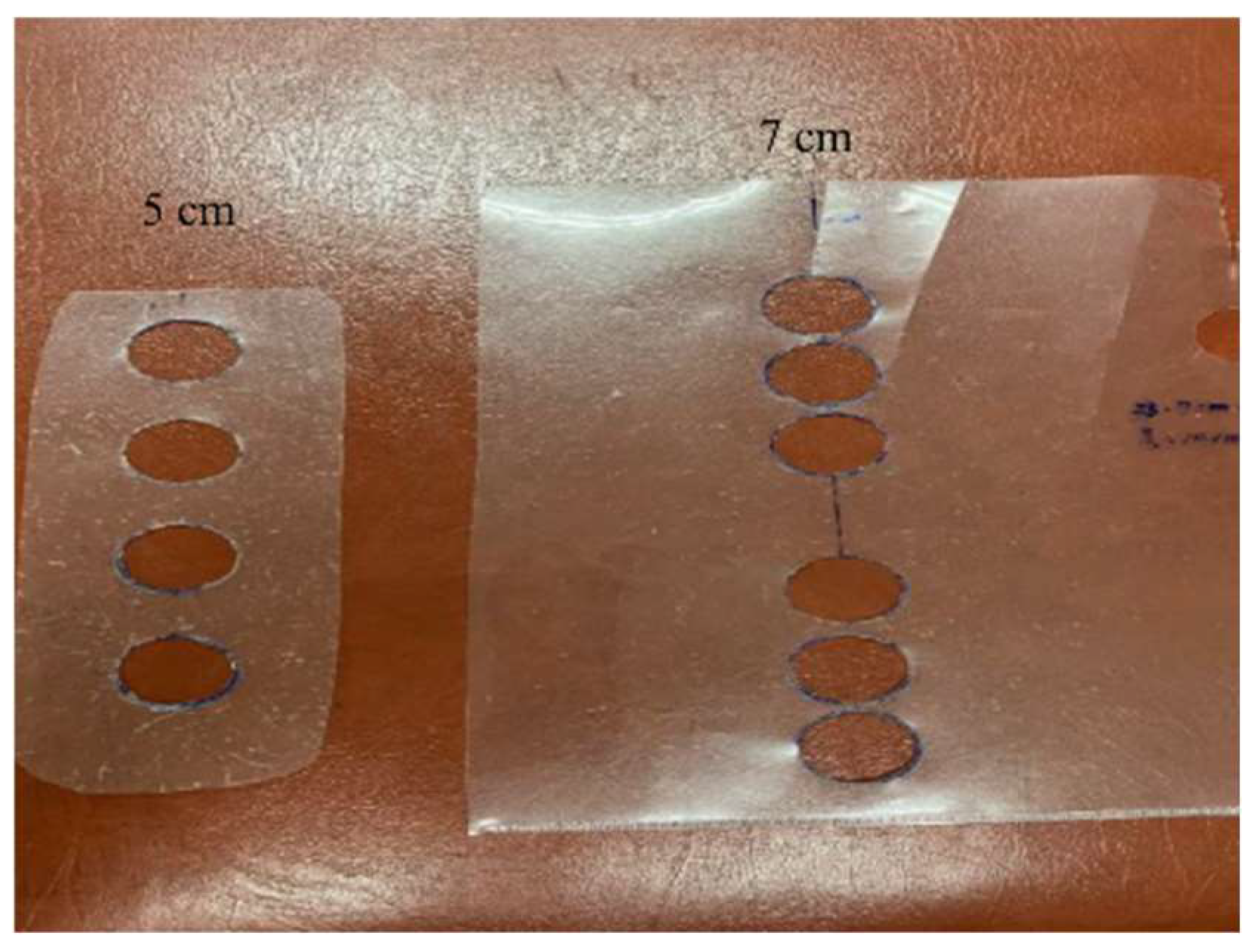
2.1.2. Placement of Electrodes
2.2. Experiment Protocol
2.3. Extracting Features
2.4. Machine Learning Models
2.4.1. Ridge Regression
2.4.2. Support Vector Regression
3. Results
3.1. Optimal Feature Sets
3.2. Performance of Regression Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EIM | electronic impedance myography |
| RFE | recursive feature elimination |
| RR | ridge regression |
| SVR | support vector regression |
| RMSE | root-mean-square-error |
| CT | computed tomography |
| MRI | magnetic resonance imaging |
| DXA | dual energy X-ray absorptiometry |
| EMG | electromyography |
| IPG | impedance plethysmography |
| EIM | impedance myography |
| ALS | amyotrophic lateral sclerosis |
| ML | machine learning |
| MoTM | total mass of thigh muscles |
| BMI | body mass index |
| REF | recursive feature elimination |
| GUI | graphic user interface |
| RMS | root mean square |
| R | resistance |
| Z | reactance |
| P | phase |
| I | impedance |
| ICC | intraclass correlation coefficient |
| TC | thigh circumference |
| CC | calf circumference |
| RF | rectus femoris |
| VL | vastus lateralis |
| MF | medial femoris |
| TA | tibialis anterior |
| ST | semitendinosus |
| BF | biceps femoris |
| GT | gastrocnemius |
| SSE | sum square error |
| r2 | regression coefficient |
References
- Department of Economic Social Affairs, United Nations. World Population Ageing 2019; United Nations: New York, NY, USA, 2019. [Google Scholar]
- National Development Council. Available online: https://www.ndc.gov.tw/Content_List.aspx?n=695E69E28C6AC7F3 (accessed on 28 April 2021).
- Kim, T.N.; Choi, K.M. Sarcopenia: Definition, epidemiology, and pathophysiology. J. Bone Metab. 2013, 20, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wall, B.T.; Dirks, M.L.; Van Loon, L.J. Skeletal muscle atrophy during short-term disuse: Implications for age-related sarcopenia. Ageing Res. Rev. 2013, 12, 898–906. [Google Scholar] [CrossRef] [PubMed]
- Kortman, H.G.J.; Wilder, S.C.; Geisbush, T.R.; Narayanaswami, P.; Rutkove, S.B. Age- and gender-associated differences in electrical impedance values of skeletal muscle. Physiol. Meas. 2013, 34, 1611–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abe, T.; Loenneke, J.P.; Thiebaud, R.S.; Fukunaga, T. Age-related site-specific muscle wasting of upper and lower extremities and trunk in Japanese men and women. Age 2014, 36, 813–821. [Google Scholar] [CrossRef]
- Abe, T.; Sakamaki, M.; Yasuda, T.; Bemben, M.G.; Kondo, M.; Kawakami, Y.; Fukunaga, T. Age-related, site-specific muscle loss in 1507 Japanese men and women aged 20 to 95 years. J. Sports Sci. Med. 2011, 10, 145–150. [Google Scholar]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.-K.; Fielding, R.A.; Martin, F.C.; Michel, J.-P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review—report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis—report of the European working group on sarcopenia in older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Boutin, R.D.; Yao, L.; Canter, R.J.; Lenchik, L. Sarcopenia: Current concepts and imaging implications. Am. J. Roentgenol. 2015, 205, W255–W266. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Wang, Z.; Baumgartner, R.N.; Ross, R. Human body composition: Advances in models and methods. Annu. Rev. Nutr. 1997, 17, 527–558. [Google Scholar] [CrossRef]
- Ross, R.; Rissanen, J.; Pedwell, H.; Clifford, J.; Shragge, P. Influence of diet and exercise on skeletal muscle and visceral adipose tissue in men. J. Appl. Physiol. 1996, 81, 2445–2455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erlandson, M.C.; Lorbergs, A.L.; Mathur, S.; Cheung, A.M. Muscle analysis using pQCT, DXA and MRI. Eur. J. Raiol. 2016, 85, 1505–1511. [Google Scholar] [CrossRef] [PubMed]
- Blake, G.M.; Fogelman, I. Technical principles of dual energy x-ray absorptiometry. Semin. Nucl. Med. 1997, 27, 210–228. [Google Scholar] [CrossRef]
- Tankisi, H.; Burke, D.; Cui, L.; Carvalho, M.; Kuwabara, S.; Nandedkar, S.D.; Rutkove, S.; Stalberg, E.; Putten, M.; Fuglsang-Frederiksen, A. Standards of instrumentation of EMG. Clin. Neurophysiol 2020, 131, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.R. The basics of electromyography. J. Neurol. Neurosurg. Psychiatry 2005, 76, ii32–ii35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birkbeck, M.; Blamire, A.M.; Whittaker, R.G.; Sayer, A.A.; Dodds, R.M. The role of novel motor unit magnetic resonance imaging to investigate motor unit activity in ageing skeletal muscle. J. Cachexia Sarcopenia Muscle 2021, 12, 17–29. [Google Scholar] [CrossRef]
- Liu, S.-H.; Lin, C.-B.; Chen, Y.; Chen, W.; Huang, T.-S.; Hsu, C.-Y. An EMG patch for the real-time monitoring of muscle-fatigue conditions during exercise. Sensors 2019, 19, 3108. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.-H.; Chang, K.-M.; Cheng, D.-C. The progression of muscle fatigue during exercise estimation with the aid of high-frequency component parameters derived from ensemble empirical mode decomposition. IEEE J. Biomed. Health Inform. 2014, 18, 1647–1658. [Google Scholar] [CrossRef]
- Clark, D.J.; Fielding, R.A. Neuromuscular contributions to age-related weakness. J. Gerontol A Biol. Sci. Med. Sci. 2012, 67, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Tian, S.-L.; Liu, Y.; Li, L.; Fu, W.-J.; Peng, C.-H. Mechanomyography is more sensitive than EMG in detecting age-related sarcopenia. J. Biomech. 2010, 43, 551–556. [Google Scholar] [CrossRef]
- Leone, A.; Rescio, G.; Manni, A.; Siciliano, P.; Caroppo, A. Comparative analysis of supervised classifiers for the evaluation of sarcopenia using a sEMG-based platform. Sensors 2022, 22, 2721. [Google Scholar] [CrossRef] [PubMed]
- Nyboer, J. Electrical impedance plethysmography: A physical and physiologic approach to peripheral vascular study. Circulation 1950, 11, 811–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamakoshi, K.I.; Shimazu, H.; Togawa, T.; Fukuoka, M.; Ito, H. Noninvasive measurement of hematocrit by electrical admittance plethysmography technique. IEEE Trans. Biomed. Eng. 1980, 27, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Khalil, S.; Mohktar, M.; Ibrahim, F. The theory and fundamentals of bioimpedance analysis in clinical status monitoring and diagnosis of diseases. Sensors 2014, 14, 10895–10928. [Google Scholar] [CrossRef] [PubMed]
- Sherwood, A.; Allen, M.T.; Fahrenberg, J.; Kelsey, R.M.; Lovallo, W.R.; Doornen, L.J.P. Methodological guideline for impedance cardiography. Psychophysiology 1990, 27, 1–23. [Google Scholar]
- Liu, S.-H.; Wang, J.-J.; Su, C.-H.; Cheng, D.-C. Improvement of left ventricular ejection time measurement in the impedance cardiography combined with the reflection photoplethysmography. Sensors 2018, 18, 3036. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.-H.; Cheng, D.-C.; Su, C.-H. A cuffless blood pressure measurement based on the impedance plethysmography technique. Sensors 2017, 17, 1176. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, B.; Rutkove, S.B. Electrical impedance myography and its applications in neuromuscular disorders. Neurotherapeutics 2017, 14, 107–118. [Google Scholar] [CrossRef]
- Tanaka, N.I.; Miyatani, M.; Masuo, Y.; Fukunaga, T.; Kanehisa, H. Applicability of a segmental bioelectrical impedance analysis for predicting the whole body skeletal muscle volume. J. Appl. Physiol. 2007, 103, 1688–1695. [Google Scholar] [CrossRef]
- Rutkove, S.B.; Caress, J.B.; Cartwright, M.S.; Burns, T.M.; Warder, J.; David, W.S.; Goyal, N.; Maragakis, N.J.; Clawson, L.; Benatar, M.; et al. Electrical impedance myography as a biomarker to assess ALS progression. Amyotroph. Lateral Scler. 2012, 13, 439–445. [Google Scholar] [CrossRef]
- Christodoulou, E.; Ma, J.; Collinsb, G.S.; Steyerberg, E.W. A systematic review shows no performance benefit of machine learning over logistic regression for clinical prediction models. J. Clin. Epidemiol. 2019, 110, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Kononenko, I. Machine learning for medical diagnosis: History, state of the art and perspective. Artif. Intell. Med. 2001, 23, 89–109. [Google Scholar] [CrossRef] [Green Version]
- Louridas, P.; Ebert, C. Machine learning. IEEE Softw. 2016, 33, 110–115. [Google Scholar] [CrossRef]
- Xin, Y.; Kong, L.; Liu, Z.; Chen, Y.; Li, Y.; Zhu, H.; Gao, M.; Hou, H.; Wang, C. Machine learning and deep learning methods for cybersecurity. IEEE Access 2018, 6, 35365–35381. [Google Scholar] [CrossRef]
- Liu, S.-H.; Liu, L.-J.; Pan, K.-L.; Chen, W.; Tan, T.-H. Using the characteristics of pulse waveform to enhance the accuracy of blood pressure measurement by a multi-dimension regression model. Appl. Sci. 2019, 9, 2922. [Google Scholar] [CrossRef] [Green Version]
- Mahajan, S.; Burman, P.; Hogarth, M. Analyzing 30-day readmission rate for heart failure using different predictive models. Stud. Health Tech. Inf. 2016, 225, 143–147. [Google Scholar]
- Kwon, H.-M.; Seo, W.-Y.; Kim, J.-M.; Shim, W.-H.; Kim, S.-H.; Hwang, G.-S. Estimation of stroke volume variance from arterial blood pressure: Using a 1-D convolutional neural network. Sensors 2021, 21, 5130. [Google Scholar] [CrossRef]
- Beam, A.L.; Kohane, I.S. Big data and machine learning in health care. JAMA 2018, 319, 1317–1318. [Google Scholar] [CrossRef]
- Chen, J.H.; Asch, S.M. Machine learning and prediction in medicine beyond the peak of inflated expectations. N. Eng. J. Med. 2017, 376, 2507–2509. [Google Scholar] [CrossRef] [Green Version]
- Frontera, W.R.; Reid, K.F.; Phillips, E.M.; Krivickas, L.S.; Hughes, V.A.; Roubenoff, R.; Fielding, R.A. Muscle fiber size and function in elderly humans: A longitudinal study. J. Appl. Physiol. 2008, 105, 637–642. [Google Scholar] [CrossRef] [Green Version]
- You, W.; Yang, Z.; Ji, G. PLS-based recursive feature elimination for high-dimensional small sample. Know. -Based Syst. 2014, 55, 15–28. [Google Scholar] [CrossRef]
- Maldonado, S.; Weber, R. A wrapper method for feature selection using Support Vector Machines. Inf. Sci. 2009, 179, 2208–2217. [Google Scholar] [CrossRef]
- Hilt, D.E.; Seegrist, D.W. Ridge, a computer program for calculating ridge regression estimates. In USDA Forest Service Research Note NE-236. Upper Darby; U.S. Department of Agriculture, Forest Service, Northeastern Forest Experiment Station: Upper Darby, PA, USA, 1977. [Google Scholar] [CrossRef]
- Smola, A.J.; Scholkopf, B. A tutorial on support vector regression. Stat. Comput. 2004, 14, 199–222. [Google Scholar] [CrossRef] [Green Version]
- Rutkove, S.B.; Kapur, K.; Zaidman, C.M.; Wu, J.S.; Pasternak, A.; Madabusi, L.; Yim, S.; Pacheck, A.; Szelag, H.; Harrington, T.; et al. Electrical impedance myography for assessment of Duchenne muscular dystrophy: EIM in DMD. Ann. Neurol. 2017, 81, 622–632. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Baumgartner, R.N.; Ross, R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. J. Appl. Physiol. 2000, 89, 465–471. [Google Scholar] [CrossRef] [Green Version]
- Blum, A.; Langley, P. Selection of relevant features and examples in machine learning. Artif. Intell. 1997, 97, 245–271. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.-H.; Lin, T.-H.; Cheng, D.-C.; Wang, J.-J. Assessment of stroke volume from brachial blood pressure using arterial characteristics. IEEE Trans. Biomed. Eng. 2015, 62, 2151–2157. [Google Scholar] [CrossRef]
- Groupprops Main Page. Available online: https://groupprops.subwiki.org/wiki/Category:Basic_definitions_in_group_theory (accessed on 15 March 2022).
- Chandrashekar, G.; Sahin, F. A Survey on Feature Selection, Comp. Electr. Eng. 2014, 40, 16–28. [Google Scholar] [CrossRef]
- Muthukrishnan, R.; Rohini, R. LASSO: A feature selection technique in predictive modeling for machine learning. In Proceedings of the 2016 IEEE International Conference on Advances in Computer Applications, Coimbatore, India, 24–24 October 2016. [Google Scholar] [CrossRef]
- Das, A.K.; Das, S.; Ghosh, A. Ensemble feature selection using bi-objective genetic algorithm. Knowl.-Based Syst. 2017, 123, 116–127. [Google Scholar] [CrossRef]
- Khalid, S.; Khalil, T.; Nasreen, S. A survey of feature selection and feature extraction techniques in machine learning. In Proceedings of the Science and Information Conference, London, UK, 27–29 August 2014. [Google Scholar]
- Aaron, R.; Esper, G.J.; Shiffman, C.A.; Bradonjic, K.; Lee, K.S.; Rutkove, S.B. Effects of age on muscle as measured by electrical impedance myography. Physiol. Meas. 2006, 27, 953–959. [Google Scholar] [CrossRef]
- Tarulli, A.W.; Duggal, N.; Esper, G.J.; Garmirian, L.P.; Fogerson, P.M.; Lin, C.H.; Rutkove, S.B. Electrical impedance myography in the assessment of disuse atrophy. Arch. Phys. Med. Rehabil. 2009, 90, 1806–1810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wróbel, M.S.; Kim, J.H.; Raj, P.; Barman, I.; Smulko, J. Utilizing pulse dynamics for non-invasive Raman spectroscopy of blood analytes. Biosens. Bioelectron. 2021, 180, 113115. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 96) | Male (N = 42) | Female (N = 54) | |
|---|---|---|---|
| Age (years) | 48.29 ± 17.91 | 44.31 ± 18.24 | 51.39 ± 17.18 |
| Height (cm) | 162.68 ± 7.51 | 168.93 ± 5.13 | 157.82 ± 5.07 |
| Weight (Kg) | 64.75 ± 11.64 | 71.10 ± 10.66 | 59.81 ± 9.91 |
| BMI (Kg/m2) | 24.40 ± 3.64 | 24.90 ± 3.38 | 24.01 ± 3.82 |
| Thigh circumference (cm) | 50.02 ± 5.34 | 50.41 ± 5.23 | 49.71 ± 5.45 |
| Calf circumference (cm) | 36.07 ± 3.13 | 37.07 ± 2.81 | 35.31 ± 3.16 |
| Muscle | Start Point | End Point |
|---|---|---|
| Vastus Lateralis | Lateral patella | Greater trochanter |
| Rectus Femoris | Midline of patella | Anterior superior iliac spine |
| Medial Femoris | Medial patella | Medial side of femur |
| Tibialis Anterior (small) | Lateral condyle of tibia | Midline of calf |
| Semitendinosus (small) | Posterior medial knee joint | Midline of gluteal fold |
| Biceps Femoris | Posterior lateral knee joint and head of fibula | Midline of gluteal fold |
| Gastrocnemius | Posterior knee joint | Midline of calf |
| Basic Information | Data Type | EIM Data | Data Type | |
|---|---|---|---|---|
| Height | Numerical | Rectus Femoris (RF) | Impedance (I) Phase (P) Resistance (R) Reactance (Z) | Numerical |
| Weight | Vastus Lateralis (VL) | |||
| BMI | Medial Femoris (MF) | |||
| Gender | Categorical | Tibialis Anterior (TA) | ||
| Thigh Circumference (TC) | Numerical | Semitendinosus (ST) | ||
| Calf Circumference (CC) | Biceps Femoris (BF) | |||
| Gastrocnemius (GT) | ||||
| Rank | Ridge Regression | SVR | ||
|---|---|---|---|---|
| Parameter | Weight Coef. (r2) Mean ± SD | Parameter | Weight Coef. (r2) Mean ± SD | |
| 1 | Height | 0.139 ± 0.151 | Height | 0.194 ± 0.189 |
| 2 | Gender | 0.087 ± 0.134 | Gender | 0.108 ± 0.166 |
| 3 | TC | 0.040 ± 0.033 | RF_R | 0.044 ± 0.090 |
| 4 | RF_R | 0.023 ± 0.097 | TC | 0.028 ± 0.051 |
| 5 | Weight | 0.009 ± 0.031 | Weight | 0.019 ± 0.030 |
| 6 | CC | 0.009 ± 0.015 | GT_P | 0.012 ± 0.041 |
| 7 | RF_Z | 0.008 ± 0.019 | TA_P | 0.009 ± 0.038 |
| 8 | TA_P | 0.001 ± 0.092 | CC | 0.008 ± 0.026 |
| 9 | VL_Z | 0.000 ± 0.036 | ||
| Features | r2 of RR | r2 of SVR |
|---|---|---|
| RF_Z/TC | 0.817 | 0.832 |
| RF_R/TC | 0.816 | 0.840 |
| VL_Z/TC | 0.815 | 0.831 |
| Features | r2 of RR | r2 of SVR |
|---|---|---|
| TA_P_Gender | 0.825 | 0.840 |
| GT_P_Gender | 0.819 | 0.832 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, K.-S.; Su, Y.-L.; Kuo, L.-C.; Yang, T.-H.; Lee, C.-L.; Chen, W.; Liu, S.-H. Muscle Mass Measurement Using Machine Learning Algorithms with Electrical Impedance Myography. Sensors 2022, 22, 3087. https://doi.org/10.3390/s22083087
Cheng K-S, Su Y-L, Kuo L-C, Yang T-H, Lee C-L, Chen W, Liu S-H. Muscle Mass Measurement Using Machine Learning Algorithms with Electrical Impedance Myography. Sensors. 2022; 22(8):3087. https://doi.org/10.3390/s22083087
Chicago/Turabian StyleCheng, Kuo-Sheng, Ya-Ling Su, Li-Chieh Kuo, Tai-Hua Yang, Chia-Lin Lee, Wenxi Chen, and Shing-Hong Liu. 2022. "Muscle Mass Measurement Using Machine Learning Algorithms with Electrical Impedance Myography" Sensors 22, no. 8: 3087. https://doi.org/10.3390/s22083087