
Multiscale Sensing of Bone-Implant Loosening for Multifunctional Smart Bone Implants: Using Capacitive Technologies for Precision Controllability

 , , ,
, , ,  , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Capacitive Sensors
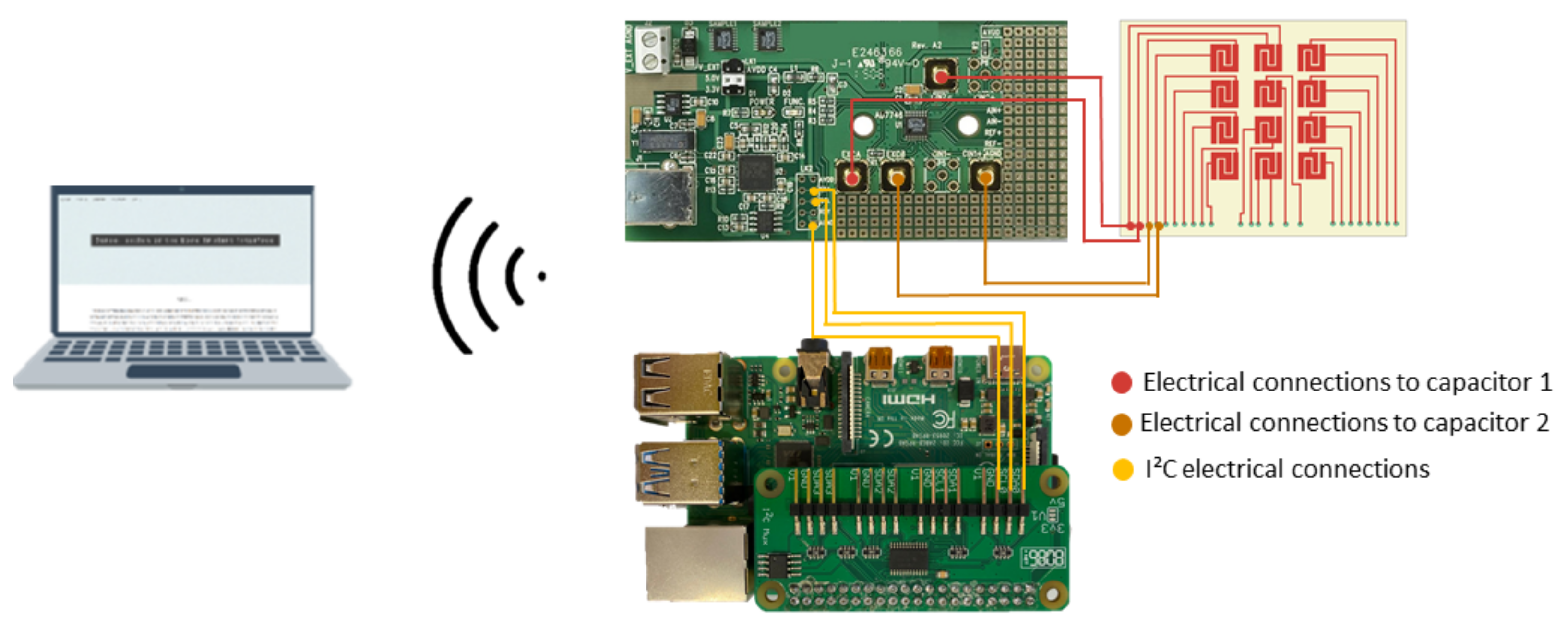
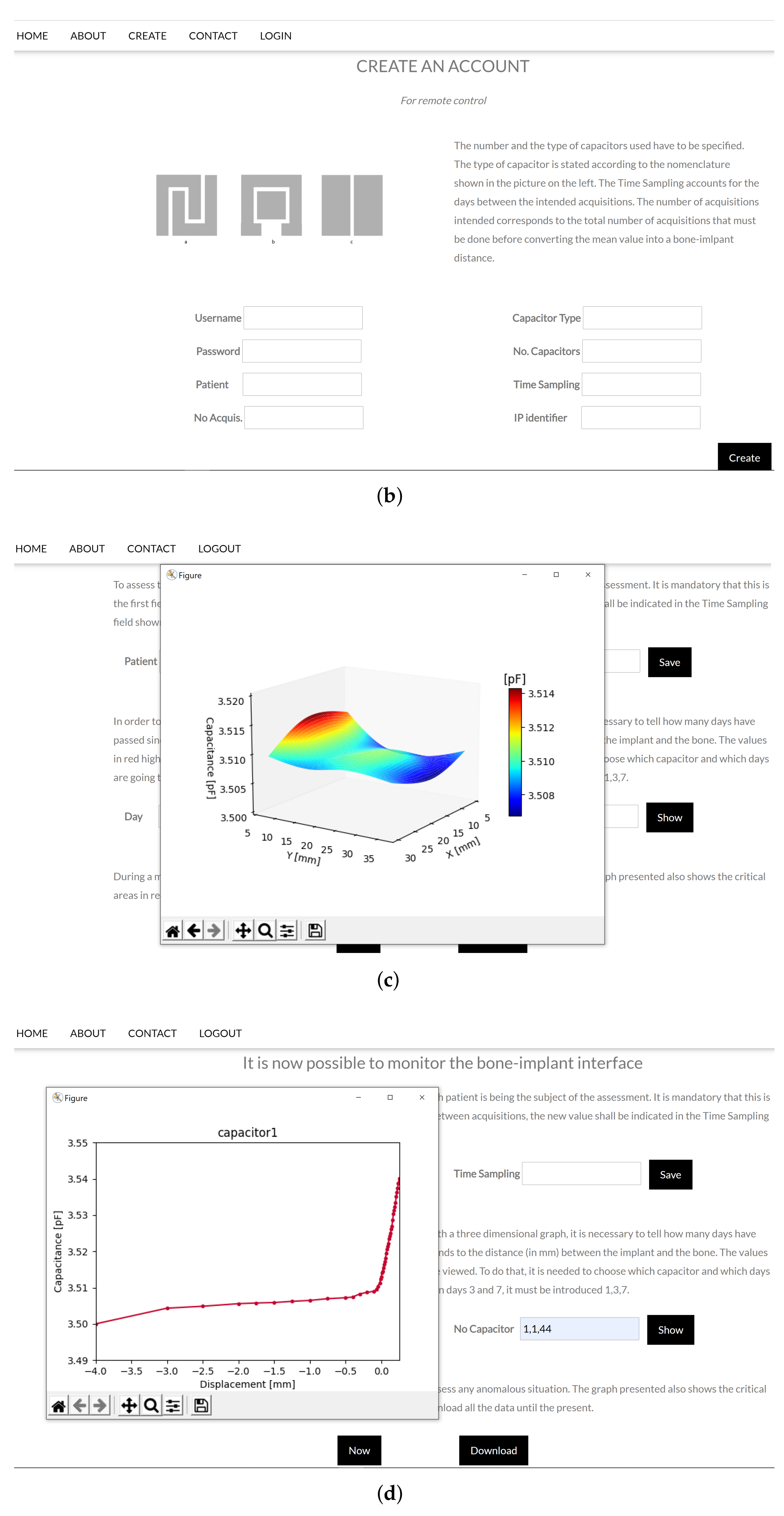
2.2. Monitoring Apparatus for Web-Based Networked Sensing
2.3. Monitoring Apparatus of the Sensing System Using Hydroxyapatite-Based Layer
2.4. Experimental Setup
2.5. Bone Samples
2.6. Hydroxyapatite Layer Characterization
2.7. Preparation of the Hydroxyapatite-Based Layer
2.8. Experimental Procedure for In Vitro Tests
3. Results
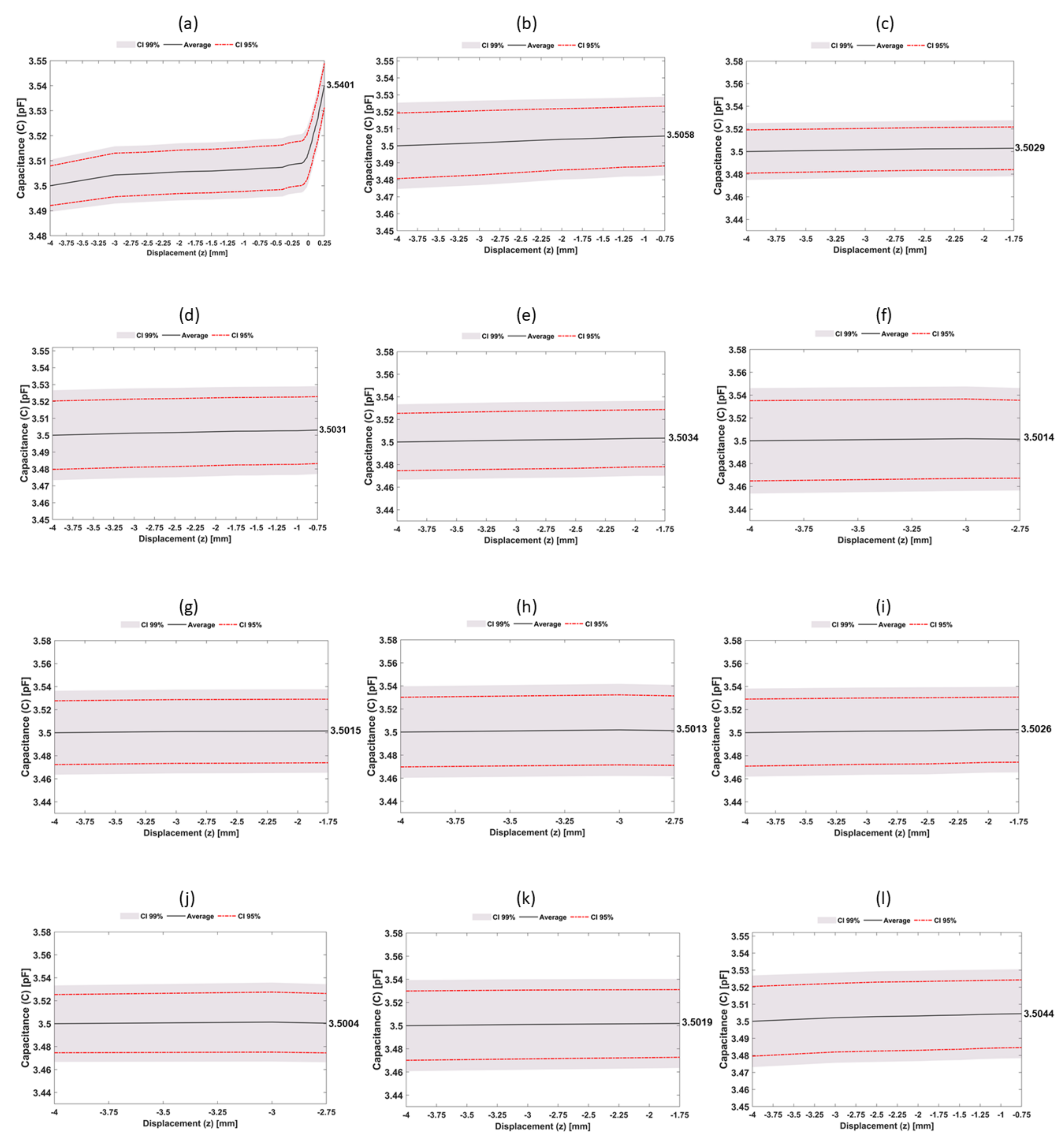
3.1. Experimental Performance of the Networked Sensing System
3.2. Experimental Performance of the Sensing System with Hydroxyapatite-Based Layer
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PCB | Printed Circuit Board |
| SEM | Scanning Electron Microscope scanning |
| UML | Unified Modeling Language |
References
- March, L.; Smith, E.U.R.; Hoy, D.G.; Cross, M.J.; Sanchez-riera, L.; Blyth, F.; Buchbinder, R.; Vos, T.; Woolf, A.D. Best Practice & Research Clinical Rheumatology Burden of disability due to musculoskeletal (MSK) disorders. Best Pract Res. Clin. Rheumatol. 2014, 28, 353–366. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Arora. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1603–1658. [Google Scholar] [CrossRef] [Green Version]
- Anandacoomarasamy, A.; Fransen, M.; March, L. Obesity and the musculoskeletal system. Curr. Opin. Rheumatol. 2009, 21, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, R.J.; Palmer, A.J.; Taylor, A.; Porter, M.L.; Malchau, H.; Glyn-Jones, S. Hip replacement. Lancet 2018, 392, 1662–1671. [Google Scholar] [CrossRef]
- Labek, G.; Thaler, M.; Janda, W.; Agreiter, M.; Stöckl, B.; Surgeon, O. Revision rates after total joint replacement cumulative results from worldwide joint register datasets. Bone Joint J. 2011, 93–293. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.J.; Robertsson, O.; Graves, S.; Price, A.J.; Arden, N.K.; Judge, A.; Beard, D.J. Knee replacement. Lancet 2012, 379, 1331–1340. [Google Scholar] [CrossRef]
- Soares dos Santos, M.P.; Bernardo, R.; Henriques, L.; Ramos, A.; Ferreira, J.A.F.; Furlani, E.P.; Torres Marques, A.; Simões, J.A.O. Towards an effective sensing technology to monitor micro-scale interface loosening of bioelectronic implants. Sci. Rep. 2021, 11, 1–17. [Google Scholar] [CrossRef]
- Sumner, D.R. Long-term implant fi xation and stress-shielding in total hip replacement. J. Biomech. 2015, 48, 797–800. [Google Scholar] [CrossRef]
- Pivec, R.; Johnson, A.J.; Mears, S.C.; Mont, M.A. Hip arthroplasty. Lancet 2012, 380, 1768–1777. [Google Scholar] [CrossRef]
- Soares dos Santos, M.P.; Ferreira, J.A.; Ramos, A.; Simões, J.A.; Morais, R.; Silva, N.M.; Santos, P.M.; Reis, M.J.; Oliveira, T. Instrumented hip implants: Electric supply systems. J. Biomech. 2013, 46, 2561–2571. [Google Scholar] [CrossRef]
- Standring, S.; Borley, N.R.; Gray, H. Gray’s Anatomy: The Anatomical Basis of Clinical Practice; Churchill Livingstone/Elsevier: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Nordin, M. ; H. Frankel, V. Basic Biomechanics of the Musculoskeletal System, 4th ed.; Lippincott Williams & Wilkin: Philadelphia, PA, USA, 2012. [Google Scholar]
- Kattimani, V.S.; Kondaka, S.; Lingamaneni, K.P. Hydroxyapatite—Past, Present, and Future in Bone Regeneration. Bone Tissue Regen. Insights 2016, 7, BTRI.S36138. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Rath, B.; Tingart, M.; Eschweiler, J. Role of implants surface modification in osseointegration: A systematic review. J. Biomed. Mater. Res. 2020, 108, 470–484. [Google Scholar] [CrossRef] [Green Version]
- Goodman, S.B.; Yao, Z.; Keeney, M.; Yang, F. The future of biologic coatings for orthopaedic implants. Biomaterials 2013, 34, 3174–3183. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, M.P.; Marote, A.; Santos, T.; Torrão, J.; Ramos, A.; Simões, J.A.; Da Cruz E Silva, O.A.; Furlani, E.P.; Vieira, S.I.; Ferreira, J.A. New cosurface capacitive stimulators for the development of active osseointegrative implantable devices. Sci. Rep. 2016, 6, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Soares Dos Santos, M.P.; Ferreira, J.A.; Ramos, A.; Simões, J.A. Active orthopaedic implants: Towards optimality. J. Franklin. Inst. 2015, 352, 813–834. [Google Scholar] [CrossRef]
- De Sousa, B.M.; Correia, C.R.; Ferreira, J.A.; Mano, J.F.; Furlani, E.P.; Soares dos Santos, M.P.; Vieira, S.I. Capacitive interdigitated system of high osteoinductive/conductive performance for personalized acting-sensing implants. NPJ Regen. Med. 2021, 6. [Google Scholar] [CrossRef]
- Cachão, J.H.; Dos Santos, M.P.; Bernardo, R.; Ramos, A.; Bader, R.; Ferreira, J.A.; Marques, A.T.; Simões, J.A. Altering the course of technologies to monitor loosening states of endoprosthetic implants. Sensors 2020, 20, 104. [Google Scholar] [CrossRef] [Green Version]
- Soares dos Santos, M.P.; Coutinho, J.; Marote, A.; Sousa, B.; Ramos, A.; Ferreira, J.A.; Bernardo, R.; Rodrigues, A.; Marques, A.T.; Cruz e Silva, O.A.; et al. Capacitive technologies for highly controlled and personalized electrical stimulation by implantable biomedical systems. Sci. Rep. 2019, 9, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.V.; Dad Ansari, M.H.; Dayan, C.B.; Giltinan, J.; Wang, S.; Yu, Y.; Kishore, V.; Laux, P.; Luch, A.; Sitti, M. Multifunctional magnetic hairbot for untethered osteogenesis, ultrasound contrast imaging and drug delivery. Biomaterials 2019, 219, 119394. [Google Scholar] [CrossRef]
- Unger, A.C.; Cabrera-Palacios, H.; Schulz, A.P.; Jürgens, C.; Paech, A. Acoustic monitoring (RFM) of total hip arthroplasty results of a cadaver study. Eur. J. Med. Res. 2009, 14, 264–271. [Google Scholar] [CrossRef] [Green Version]
- Alshuhri, A.A.; Holsgrove, T.P.; Miles, A.W.; Cunningham, J.L. Development of a non-invasive diagnostic technique for acetabular component loosening in total hip replacements. Med. Eng. Phys. 2015, 37, 739–745. [Google Scholar] [CrossRef] [Green Version]
- Alshuhri, A.A.; Holsgrove, T.P.; Miles, A.W.; Cunningham, J.L. Non-invasive vibrometry-based diagnostic detection of acetabular cup loosening in total hip replacement (THR). Med. Eng. Phys. 2017, 48, 188–195. [Google Scholar] [CrossRef] [Green Version]
- Goossens, Q.; Leuridan, S.; Henyš, P.; Roosen, J.; Pastrav, L.; Mulier, M.; Desmet, W.; Denis, K.; Vander Sloten, J. Development of an acoustic measurement protocol to monitor acetabular implant fixation in cementless total hip Arthroplasty: A preliminary study. Med. Eng. Phys. 2017, 49, 28–38. [Google Scholar] [CrossRef]
- Glaser, D.; Komistek, R.D.; Cates, H.E.; Mahfouz, M.R. Clicking and squeaking: In vivo correlation of sound and separation for different bearing surfaces. J. Bone Joint Surg 2008, 90, 112–120. [Google Scholar] [CrossRef]
- Ewald, H.; Timm, U.; Bader, R.; Kluess, D. Acoustic sensor system for loosening detection of hip implants. In Proceedings of the 2011 IEEE SENSORS, Palmerston North, New Zealand, 28 November–1 December 2011; pp. 494–497. [Google Scholar]
- Georgiou, A.P.; Cunningham, J.L. Accurate diagnosis of hip prosthesis loosening using a vibrational technique. Clin. Biomech. 2001, 16, 315–323. [Google Scholar] [CrossRef]
- Rieger, J.S.; Jaeger, S.; Schuld, C.; Kretzer, J.P.; Bitsch, R.G. A vibrational technique for diagnosing loosened total hip endoprostheses: An experimental sawbone study. Med. Eng. Phys. 2013, 35, 329–337. [Google Scholar] [CrossRef]
- Rieger, J.S.; Jaeger, S.; Kretzer, J.P.; Rupp, R.; Bitsch, R.G. Loosening detection of the femoral component of hip prostheses with extracorporeal shockwaves: A pilot study. Med. Eng. Phys. 2015, 37, 157–164. [Google Scholar] [CrossRef]
- Lannocca, M.; Varini, E.; Cappello, A.; Cristofolini, L.; Bialoblocka, E. Intra-operative evaluation of cementless hip implant stability: A prototype device based on vibration analysis. Med. Eng. Phys. 2007, 29, 886–894. [Google Scholar] [CrossRef]
- Pastrav, L.C.; Jaecques, S.V.; Jonkers, I.; Perre, G.V.D.; Mulier, M. In vivo evaluation of a vibration analysis technique for the per-operative monitoring of the fixation of hip prostheses. J. Orthop. Surg. Res. 2009, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jiang, C.C.; Lee, J.H.; Yuan, T.T. Vibration arthrometry in thé patients with failed total knee replacement. IEEE Trans. Biomed. Eng. 2000, 47, 219–227. [Google Scholar] [CrossRef]
- Ruther, C.; Nierath, H.; Ewald, H.; Cunningham, J.L.; Mittelmeier, W.; Bader, R.; Kluess, D. Investigation of an acoustic-mechanical method to detect implant loosening. Med. Eng. Phys. 2013, 35, 1669–1675. [Google Scholar] [CrossRef] [PubMed]
- Ewald, H.; Ruther, C.; Mittelmeier, W.; Bader, R.; Kluess, D. A novel in vivo sensor for loosening diagnostics in total hip replacement. In Proceedings of the 2011 IEEE SENSORS Proceedings, Limerick, Ireland, 8–31 October 2011; pp. 89–92. [Google Scholar]
- Burton, A.R.; Sun, P.; Lynch, J.P. Bio-compatible wireless inductive thin-film strain sensor for monitoring the growth and strain response of bone in osseointegrated prostheses. Struct. Health Monit. 2019, 20, 749–767. [Google Scholar] [CrossRef]
- McGilvray, K.C.; Unal, E.; Troyer, K.L.; Santoni, B.G.; Palmer, R.H.; Easley, J.T.; Demir, H.V.; Puttlitz, C.M. Implantable microelectromechanical sensors for diagnostic monitoring and post-surgical prediction of bone fracture healing. J. Orthop. Res. 2015, 33, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
- Arpaia, P.; Clemente, F.; Zanesco, A. Low-invasive diagnosis of metallic prosthesis osseointegration by electrical impedance spectroscopy. IEEE Trans. Instrum. Meas. 2007, 56, 784–789. [Google Scholar] [CrossRef]
- Arpaia, P.; Clemente, F.; Romanucci, C. In-vivo test procedure and instrument characterization for EIS-based diagnosis of prosthesis osseointegration. In Proceedings of the Conference Record—IEEE Instrumentation and Measurement Technology Conference, Warsaw, Poland, 1–3 May 2007; pp. 1–6. [Google Scholar] [CrossRef]
- Graichen, F.; Arnold, R.; Rohlmann, A.; Bergmann, G. Implantable 9-channel telemetry system for in vivo load measurements with orthopedic implants. IEEE. Trans. Biomed. Eng. 2007, 54, 253–261. [Google Scholar] [CrossRef]
- Morais, R.; Frias, C.M.; Silva, N.M.; Azevedo, J.L.; Serôdio, C.A.; Silva, P.M.; Ferreira, J.A.; Simões, J.A.; Reis, M.C. An activation circuit for battery-powered biomedical implantable systems. Sens. Actuator A Phys. 2009, 156, 229–236. [Google Scholar] [CrossRef]
- Harun, W.S.; Asri, R.I.; Alias, J.; Zulkifli, F.H.; Kadirgama, K.; Ghani, S.A.; Shariffuddin, J.H. A comprehensive review of hydroxyapatite-based coatings adhesion on metallic biomaterials. Ceram. Int. 2018, 44, 1250–1268. [Google Scholar] [CrossRef]
- Herrera, A.; Mateo, J.; Gil-Albarova, J.; Lobo-Escolar, A.; Ibarz, E.; Gabarre, S.; Más, Y.; Gracia, L. Cementless hydroxyapatite coated hip prostheses. Biomed Res. Int. 2015, 2015, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.V.; Maharjan, R.S.; Kromer, C.; Laux, P.; Luch, A.; Vats, T.; Chandrasekar, V.; Dakua, S.P.; Park, B.W. Advances in Smoking Related in Vitro Inhalation Toxicology: A Perspective Case of Challenges and Opportunities from Progresses in Lung-on-Chip Technologies. Chem. Res. Toxicol. 2021, 34, 1984–2002. [Google Scholar] [CrossRef]
- Shah, F.A.; Thomsen, P.; Palmquist, A. Osseointegration and current interpretations of the bone-implant interface. Acta Biomater. 2019, 84, 1–15. [Google Scholar] [CrossRef]
- Azami, M.; Moztarzadeh, F.; Tahriri, M. Preparation, characterization and mechanical properties of controlled porous gelatin/hydroxyapatite nanocomposite through layer solvent casting combined with freeze-drying and lamination techniques. J. Porous Mater. 2010, 17, 313–320. [Google Scholar] [CrossRef]
- Vidal, J.V.; Slabov, V.; Kholkin, A.L.; dos Santos, M.P. Hybrid Triboelectric-Electromagnetic Nanogenerators for Mechanical Energy Harvesting: A Review; Springer: Singapore, 2021; Volume 13. [Google Scholar] [CrossRef]
- Carneiro, P.; Soares dos Santos, M.P.; Rodrigues, A.; Ferreira, J.A.; Simões, J.A.; Marques, A.T.; Kholkin, A.L. Electromagnetic energy harvesting using magnetic levitation architectures: A review. Appl. Energy 2020, 260, 114–191. [Google Scholar] [CrossRef] [Green Version]
- Soares Dos Santos, M.P.; Ferreira, J.A.; Simões, J.A.; Pascoal, R.; Torrão, J.; Xue, X.; Furlani, E.P. Magnetic levitation-based electromagnetic energy harvesting: A semi-Analytical non-linear model for energy transduction. Sci. Rep. 2016, 6, 1–9. [Google Scholar] [CrossRef]
- Min, Y.; Liu, Y.; Poojari, Y.; Wu, J.C.; Hildreth, B.E.; Rosol, T.J.; Epstein, A.J. Self-doped polyaniline-based interdigitated electrodes for electrical stimulation of osteoblast cell lines. Synth. Met. 2014, 198, 308–313. [Google Scholar] [CrossRef]















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peres, I.; Rolo, P.; Ferreira, J.A.F.; Pinto, S.C.; Marques, P.A.A.P.; Ramos, A.; Soares dos Santos, M.P. Multiscale Sensing of Bone-Implant Loosening for Multifunctional Smart Bone Implants: Using Capacitive Technologies for Precision Controllability. Sensors 2022, 22, 2531. https://doi.org/10.3390/s22072531
Peres I, Rolo P, Ferreira JAF, Pinto SC, Marques PAAP, Ramos A, Soares dos Santos MP. Multiscale Sensing of Bone-Implant Loosening for Multifunctional Smart Bone Implants: Using Capacitive Technologies for Precision Controllability. Sensors. 2022; 22(7):2531. https://doi.org/10.3390/s22072531
Chicago/Turabian StylePeres, Inês, Pedro Rolo, Jorge A. F. Ferreira, Susana C. Pinto, Paula A. A. P. Marques, António Ramos, and Marco P. Soares dos Santos. 2022. "Multiscale Sensing of Bone-Implant Loosening for Multifunctional Smart Bone Implants: Using Capacitive Technologies for Precision Controllability" Sensors 22, no. 7: 2531. https://doi.org/10.3390/s22072531