
The Use of Microsensors to Assess the Daily Wear Time of Removable Orthodontic Appliances: A Prospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Study Design
- (1)
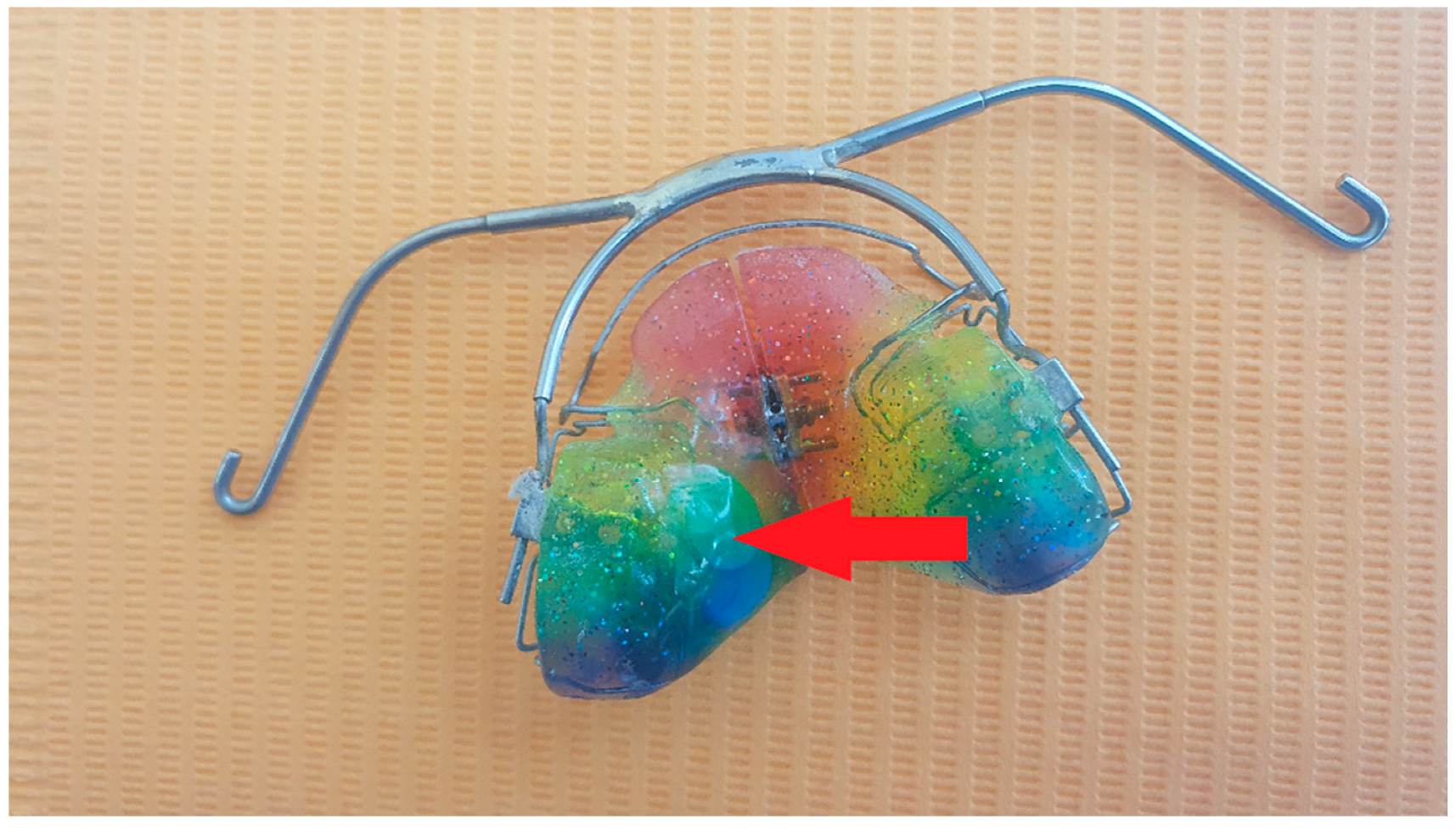
- Functional treatment using modifications to the monoblock appliance;
- (2)
- Active treatment using a lower or upper Schwarz appliance (S); or
- (3)
- Functional active treatment using the twin block appliance combined with headgear (TB + HG).
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
- (1)
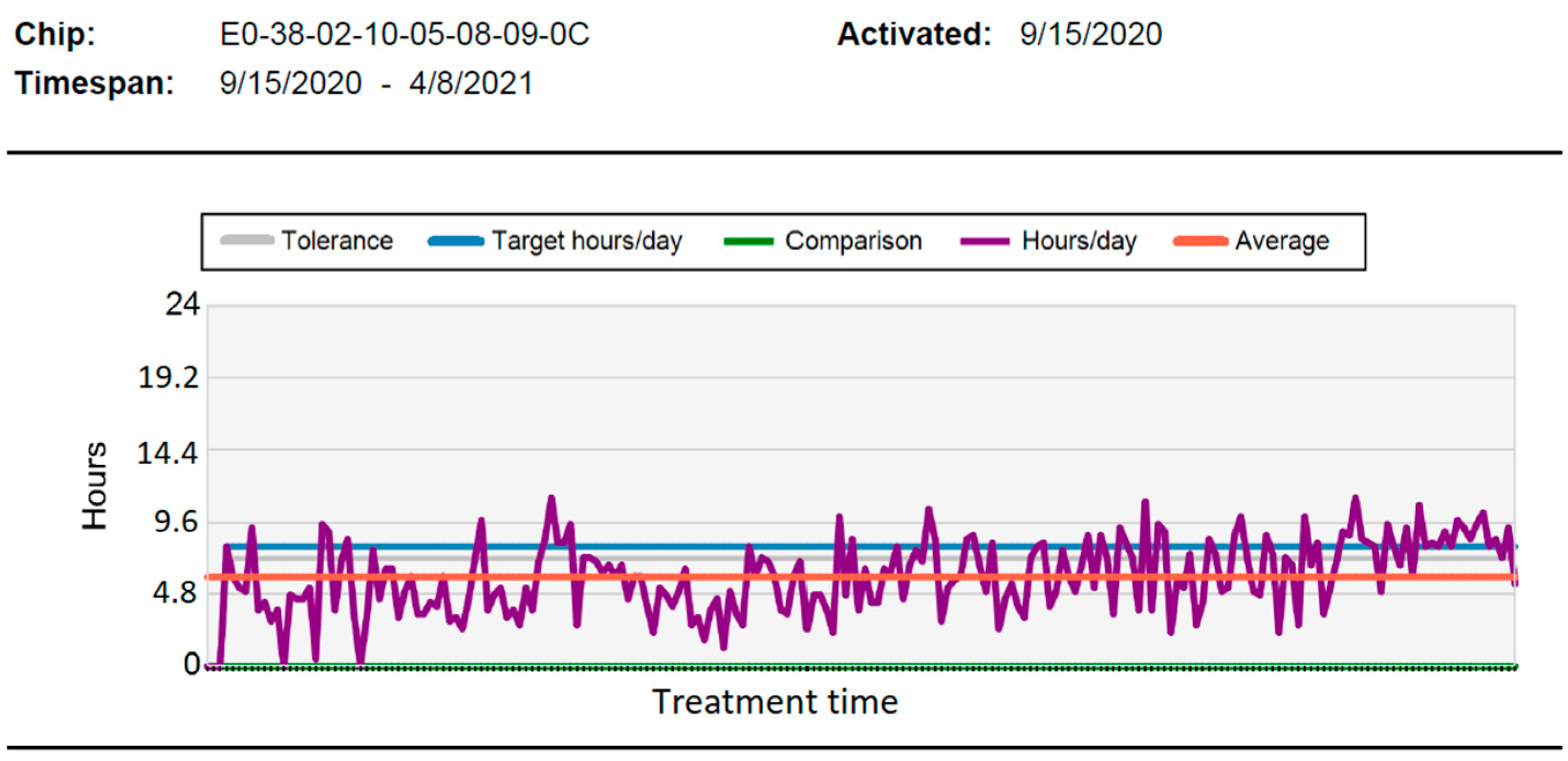
- Children treated under compulsory health insurance wear removable orthodontic appliances for much shorter periods of time than recommended; very poor patient compliance, nearly 54% of the required 12 h per day, probably significantly reduces the effectiveness of orthodontic treatment.
- (2)
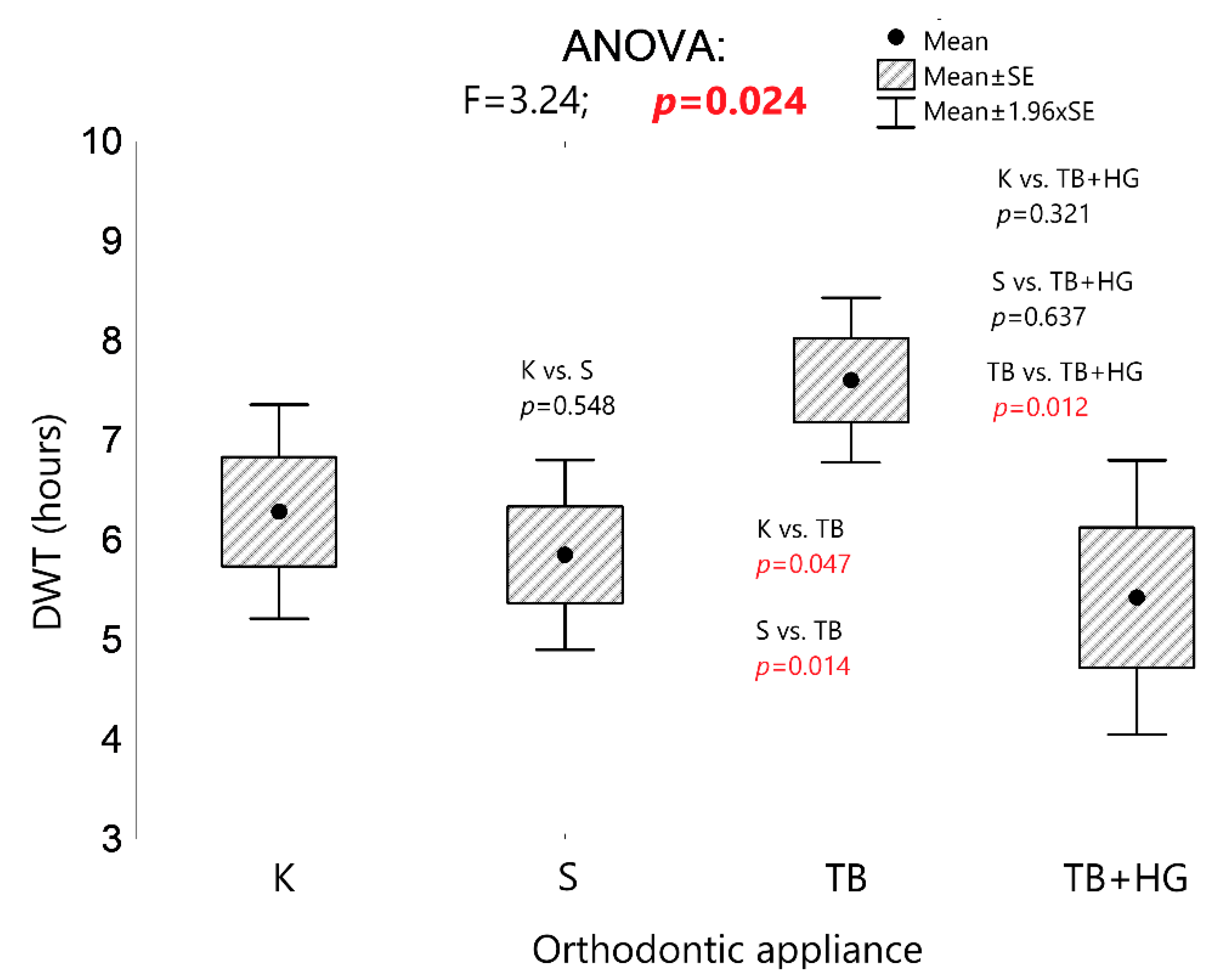
- Since patients treated with removable appliances are most willing to use a twin block appliance (TB), this appliance is most often chosen for functional treatment in orthodontics.
- (3)
- Further research should focus on how best to encourage patients to adhere to treatment recommendations in order to increase the effectiveness of orthodontic treatment with removable appliances.
- (4)
- Microsensors are a valuable tool that allows for the verification of previously conducted research and the conclusions resulting therefrom but also for carrying out research that was once impossible, which is of key importance for the development of orthodontics in the future.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Proffit, W.R. Contemporary Orthodontics, 5th ed.; Elsevier/Mosby: St. Louis, MO, USA, 2013; ISBN 9780323083171. [Google Scholar]
- Koretsi, V.; Zymperdikas, V.F.; Papageorgiou, S.N.; Papadopoulos, M.A. Treatment Effects of Removable Functional Appliances in Patients with Class II Malocclusion: A Systematic Review and Meta-Analysis. Eur. J. Orthod. 2015, 37, 418–434. [Google Scholar] [CrossRef] [PubMed]
- Tausche, E.; Luck, O.; Harzer, W. Prevalence of Malocclusions in the Early Mixed Dentition and Orthodontic Treatment Need. Eur. J. Orthod. 2004, 26, 237–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernas, A.J.; Banting, D.W.; Short, L.L. Effectiveness of Phase I Orthodontic Treatment in an Undergraduate Teaching Clinic. J. Dent. Educ. 2007, 71, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Franchi, L.; Pavoni, C.; Faltin, K.; McNamara, J.A.; Cozza, P. Long-Term Skeletal and Dental Effects and Treatment Timing for Functional Appliances in Class II Malocclusion. Angle Orthod. 2013, 83, 334–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schott, T.C.; Göz, G. Die Einstellung Junger Patienten Zu Tragezeit, Tragezeitverordnung Und Elektronischer Tragezeitmessung von Herausnehmbaren Apparaturen—Ergebnisse Einer Fragebogenstudie. J. Orofac. Orthop. 2010, 71, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Brierley, C.A.; Benson, P.E.; Sandler, J. How Accurate Are TheraMon® Microsensors at Measuring Intraoral Wear-Time? Recorded vs. Actual Wear Times in Five Volunteers. J. Orthod. 2017, 44, 241–248. [Google Scholar] [CrossRef]
- Schott, T.C.; Ludwig, B. Microelectronic Wear-Time Documentation of Removable Orthodontic Devices Detects Heterogeneous Wear Behavior and Individualizes Treatment Planning. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Schott, T.C.; Schlipf, C.; Glasl, B.; Schwarzer, C.L.; Weber, J.; Ludwig, B. Quantification of Patient Compliance with Hawley Retainers and Removable Functional Appliances during the Retention Phase. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 533–540. [Google Scholar] [CrossRef]
- Schäfer, K.; Ludwig, B.; Meyer-Gutknecht, H.; Schott, T.C. Quantifying Patient Adherence during Active Orthodontic Treatment with Removable Appliances Using Microelectronic Wear-Time Documentation. Eur. J. Orthod. 2015, 37, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Tsomos, G.; Ludwig, B.; Grossen, J.; Pazera, P.; Gkantidis, N. Objective Assessment of Patient Compliance with Removable Orthodontic Appliances: A Cross-Sectional Cohort Study. Angle Orthod. 2014, 84, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Pauls, A.; Nienkemper, M.; Panayotidis, A.; Wilmes, B.; Drescher, D. Effects of Wear Time Recording on the Patient’s Compliance. Angle Orthod. 2013, 83, 1002–1008. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, A.; Witt, E.; Sahm, G.; Schneider, S. Correlates of Objective Patient Compliance with Removable Appliance Wear. Am. J. Orthod. Dentofac. Orthop. 1993, 104, 378–386. [Google Scholar] [CrossRef]
- Sergl, H.G.; Zentner, A. A Comparative Assessment of Acceptance of Different Types of Functional Appliances. Eur. J. Orthod. 1998, 20, 517–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandão, M.; Pinho, H.S.; Urias, D. Clinical and Quantitative Assessment of Headgear Compliance: A Pilot Study. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 239–244. [Google Scholar] [CrossRef]
- Bos, A.; Kleverlaan, C.J.; Hoogstraten, J.; Prahl-Andersen, B.; Kuitert, R. Comparing Subjective and Objective Measures of Headgear Compliance. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 801–805. [Google Scholar] [CrossRef]
- Cureton, S.L.; Regennitter, F.J.; Yancey, J.M. Clinical versus Quantitative Assessment of Headgear Compliance. Am. J. Orthod. Dentofac. Orthop. 1993, 104, 277–284. [Google Scholar] [CrossRef]
- Al-Moghrabi, D.; Salazar, F.C.; Pandis, N.; Fleming, P.S. Compliance with Removable Orthodontic Appliances and Adjuncts: A Systematic Review and Meta-Analysis. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 17–32. [Google Scholar] [CrossRef]
- Al-Kurwi, A.S.A.; Bos, A.; Kuitert, R.B. Overjet Reduction in Relation to Wear Time with the van Beek Activator Combined with a Microsensor. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 277–283. [Google Scholar] [CrossRef]
- Miguel, J.A.M.; Sales, H.X.; Quintão, C.C.; Oliveira, B.H.; Feu, D. Factors Associated with Orthodontic Treatment Seeking by 12–15-Year-Old Children at a State University-Funded Clinic. J. Orthod. 2010, 37, 100–106. [Google Scholar] [CrossRef]
- El-Huni, A.; Colonio Salazar, F.B.; Sharma, P.K.; Fleming, P.S. Understanding Factors Influencing Compliance with Removable Functional Appliances: A Qualitative Study. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 173–181. [Google Scholar] [CrossRef]
- Daniels, A.S.; Seacat, J.D.; Inglehart, M.R. Orthodontic Treatment Motivation and Cooperation: A Cross-Sectional Analysis of Adolescent Patients’ and Parents’ Responses. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 780–787. [Google Scholar] [CrossRef]
- Aǧar, U.; Doruk, C.; Altuǧ Biçakçi, A.; Büküşoǧlu, N. The Role of Psycho-Social Factors in Headgear Compliance. Eur. J. Orthod. 2005, 27, 263–267. [Google Scholar] [CrossRef]
- Clemmer, E.J.; Hayes, E.W. Patient Cooperation in Wearing Orthodontic Headgear. Am. J. Orthod. 1979, 75, 517–524. [Google Scholar] [CrossRef]
- Hyun, P.; Preston, C.B.; Al-Jewair, T.S.; Park-Hyun, E.; Tabbaa, S. Patient Compliance with Hawley Retainers Fitted with the SMARTH Sensor: A Prospective Clinical Pilot Study. Angle Orthod. 2015, 85, 263–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.Y.; Will, L.A.; Niederman, R. Analysis of Efficacy of Functional Appliances on Mandibular Growth. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 470–476. [Google Scholar] [CrossRef]
- Sarul, M.; Kawala, B.; Kozanecka, A.; Łyczek, J.; Antoszewska-Smith, J. Objectively Measured Compliance during Early Orthodontic Treatment: Do Treatment Needs Have an Impact? Adv. Clin. Exp. Med. 2017, 26, 83–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarul, M.; Antoszewska-Smith, J.; Park, H.S. Self-Perception of Smile Attractiveness as a Reliable Predictor of Increased Patient Compliance with an Orthodontist. Adv. Clin. Exp. Med. 2019, 28, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Woolass, K.F.; Shaw, W.C.; Viader, P.H.; Lewis, A.S. The Prediction of Patient Co-Operation in Orthodontic Treatment. Eur. J. Orthod. 1988, 10, 235–243. [Google Scholar] [CrossRef]
- Albino, J.E.N.; Lawrence, S.D.; Lopes, C.E.; Nash, L.B.; Tedesco, L.A. Cooperation of Adolescents in Orthodontic Treatment. J. Behav. Med. 1991, 14, 53–70. [Google Scholar] [CrossRef]
- Amado, J.; Sierra, A.M.; Gallón, A.; Álvarez, C.; Baccetti, T. Relationship between Personality Traits and Cooperation. Angle Orthod. 2008, 78, 688–691. [Google Scholar] [CrossRef] [Green Version]
- Dinwiddie, R.; Müller, W.G. Adolescent Treatment Compliance in Asthma. J. R. Soc. Med. 2002, 95, 68–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, K.; Wright, J.; Conboy, F.; Sanjie, Y.W.; Mandall, N.; Chadwick, S.; Connolly, I.; Cook, P.; Birnie, D.; Hammond, M.; et al. Effectiveness of Early Orthodontic Treatment with the Twin-Block Appliance: A Multicenter, Randomized, Controlled Trial. Part 1: Dental and Skeletal Effects. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 234–243. [Google Scholar] [CrossRef]
- O’Brien, K.; Wright, J.; Conboy, F.; Chadwick, S.; Connolly, I.; Cook, P.; Birnie, D.; Hammond, M.; Harradine, N.; Lewis, D.; et al. Effectiveness of Early Orthodontic Treatment with the Twin-Block Appliance: A Multicenter, Randomized, Controlled Trial. Part 2: Psychosocial Effects. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 488–494. [Google Scholar] [CrossRef]
- O’Brien, K.; Wright, J.; Conboy, F.; Sanjie, Y.W.; Mandall, N.; Chadwick, S.; Connolly, I.; Cook, P.; Birnie, D.; Hammond, M.; et al. Effectiveness of Treatment for Class II Malocclusion with the Herbst or Twin-Block Appliances: A Randomized, Controlled Trial. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 128–137. [Google Scholar] [CrossRef]
- Sarul, M.; Nahajowski, M.; Gawin, G.; Antoszewska-Smith, J. Does Daily Wear Time of Twin Block Reliably Predict Its Efficiency of Class II Treatment? J. Orofac. Orthop. 2021, 1–10. [Google Scholar] [CrossRef]
- Schott, T.C.; Ludwig, B. Quantification of Wear-Time Adherence of Removable Appliances in Young Orthodontic Patients in Relation to Their BMI: A Preliminary Study. Patient Prefer. Adherence 2014, 8, 1587–1595. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
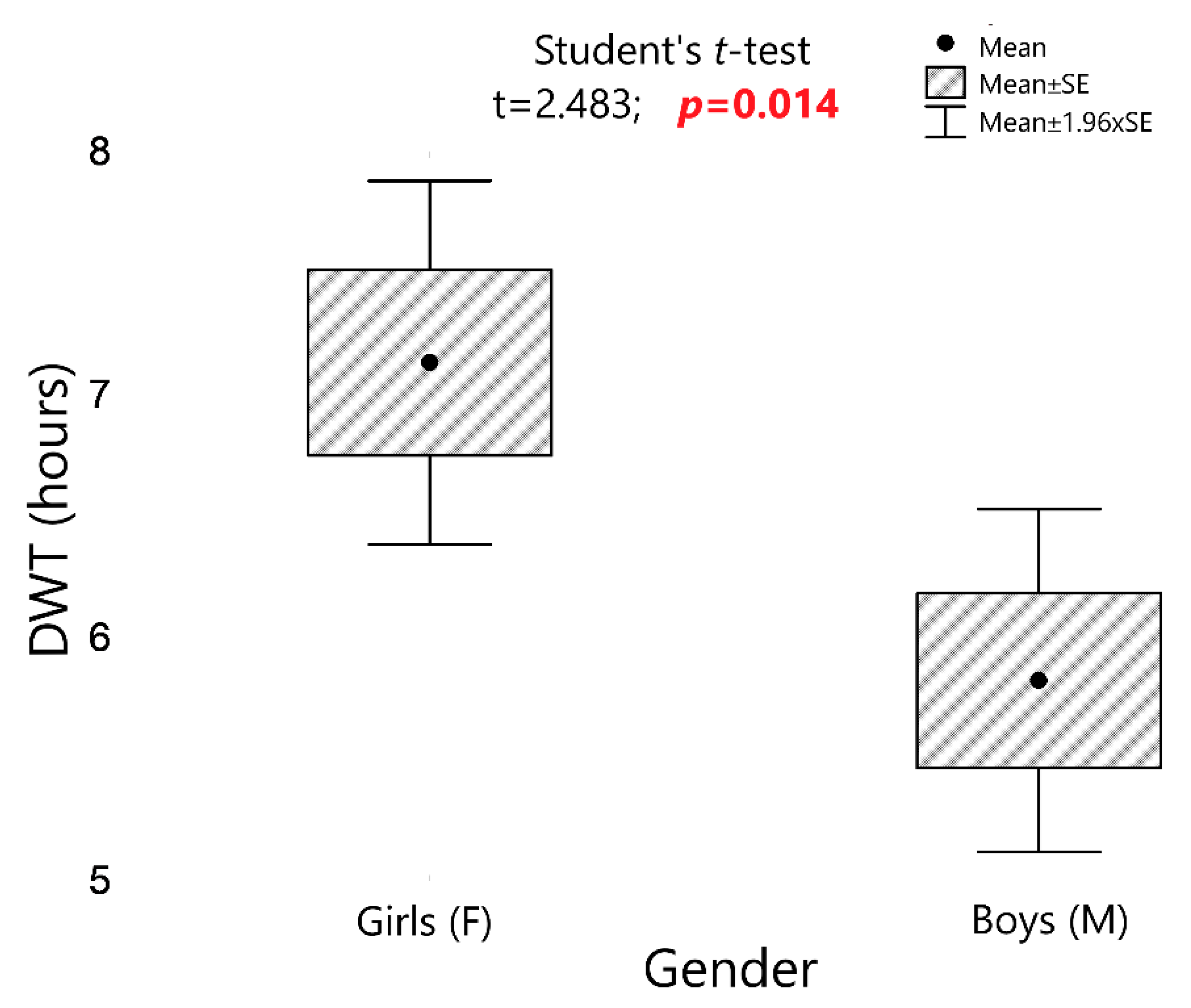
| Study Group/Type of Appliance | Gender | N | Mean ± SE | 95% CI |
|---|---|---|---|---|
| K | F | 29 | 7.2 ± 0.6 | 6.6–7.8 |
| K | M | 22 | 5.1 ± 0.7 | 4.4–5.8 |
| S | F | 21 | 6.4 ± 0.7 | 5.6–7.1 |
| S | M | 18 | 5.3 ± 0.8 | 4.5–6.1 |
| TB | F | 28 | 8.1 ± 0.6 | 7.4–8.7 |
| TB | M | 27 | 7.1 ± 0.6 | 6.5–7.8 |
| TB+HG | F | 9 | 5.8 ± 1.1 | 4.7–6.9 |
| TB+HG | M | 13 | 5.2 ± 0.9 | 4.2–6.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nahajowski, M.; Lis, J.; Sarul, M. The Use of Microsensors to Assess the Daily Wear Time of Removable Orthodontic Appliances: A Prospective Cohort Study. Sensors 2022, 22, 2435. https://doi.org/10.3390/s22072435
Nahajowski M, Lis J, Sarul M. The Use of Microsensors to Assess the Daily Wear Time of Removable Orthodontic Appliances: A Prospective Cohort Study. Sensors. 2022; 22(7):2435. https://doi.org/10.3390/s22072435
Chicago/Turabian StyleNahajowski, Marek, Joanna Lis, and Michał Sarul. 2022. "The Use of Microsensors to Assess the Daily Wear Time of Removable Orthodontic Appliances: A Prospective Cohort Study" Sensors 22, no. 7: 2435. https://doi.org/10.3390/s22072435