
Neurofeedback Therapy for Sensory Over-Responsiveness—A Feasibility Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instrumentation
2.2.1. Screening Measure
2.2.2. Primary Outcome Measure
2.2.3. Secondary Outcome Measures
2.2.4. Intervention
2.3. Procedure
2.4. Statistical Analyses
3. Results
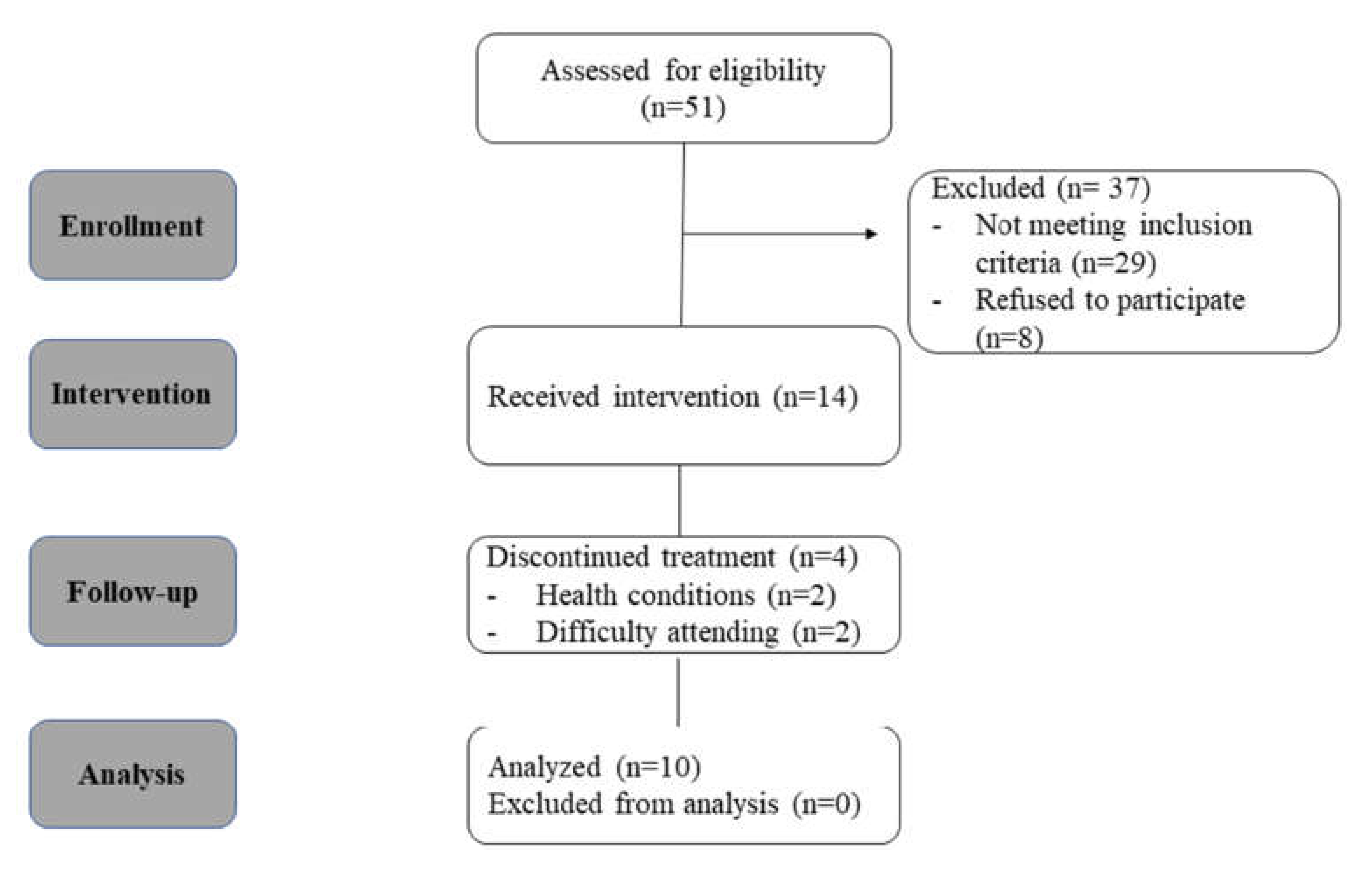
3.1. Sample Dropout
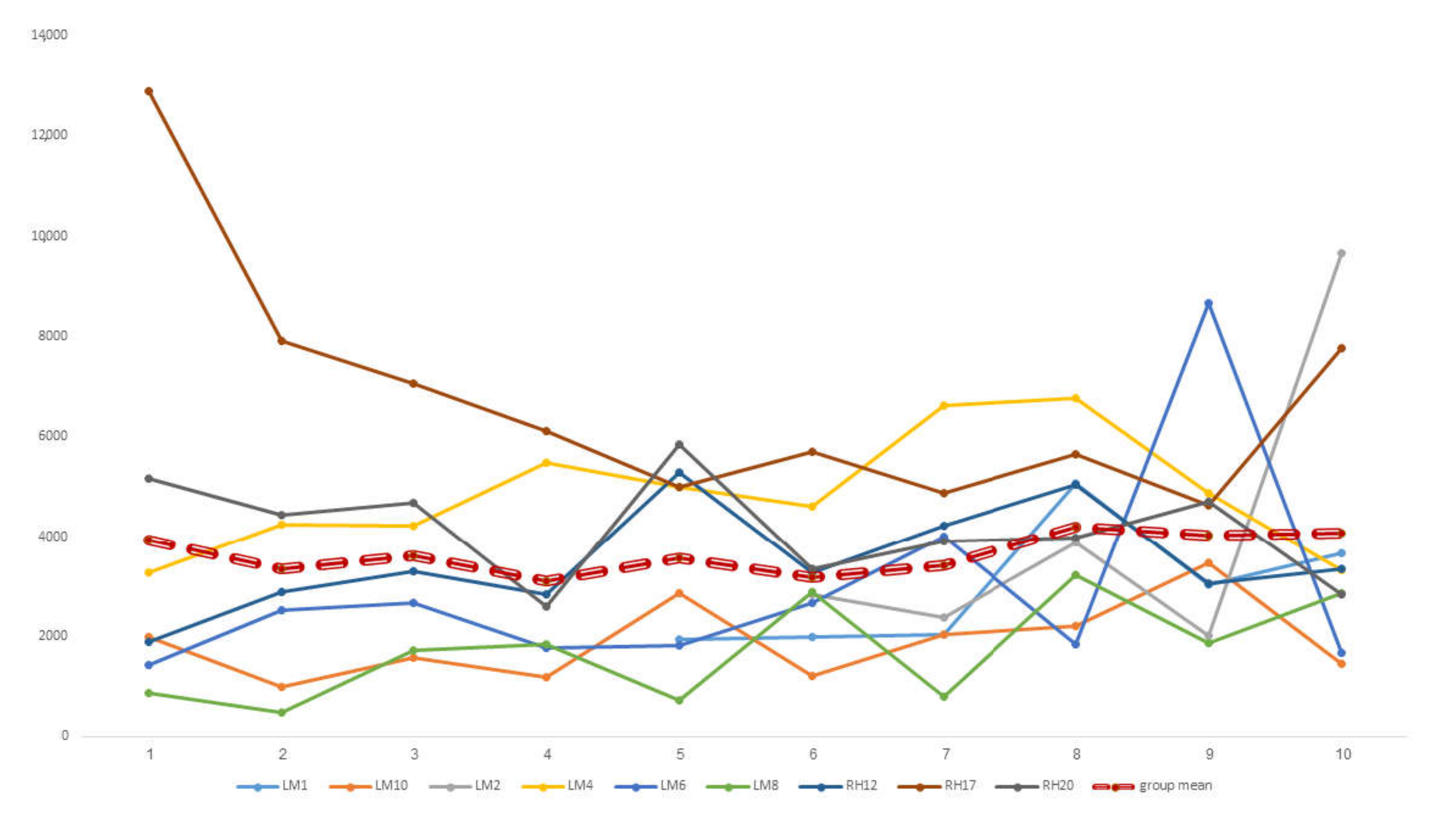
3.2. Upregulating Alpha during Training
3.3. Primary Outcomes Measure
3.4. Secondary Outcome Measures
3.4.1. Neurofeedback and Life Satisfaction
3.4.2. Neurofeedback and Pain Sensitivity
3.4.3. Neurofeedback and Anxiety
3.4.4. Neurofeedback and Achieving Personalized Goals
3.5. Correlations between Primary and Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Domain | Item # | Checklist Item | Reported on Page # |
|---|---|---|---|
| Re-experiment | |||
| 1a | Pre-register experimental protocol and planned analyses | p. 3 | |
| 1b | Justify sample size Control groups | p. 4 | |
| Control groups | |||
| 2a | Employ control group(s) or control condition(s) | Control condition: T1 p. 3 | |
| 2b | When leveraging experimental designs where a double-blind is possible, use a double-blind | ||
| 2c | Blind those who rate the outcomes, and when possible, the statisticians involved | p. 3 | |
| 2d | Examine to what extent participants and experimenters remain blinded | ||
| 2e | In clinical efficacy studies, employ a standard-of-care intervention group as a benchmark for improvement | ||
| Control measures | |||
| 3a | Collect data on psychosocial factors | p. 7; p. 5 | |
| 3b | Report whether participants were provided with a strategy | p. 6 | |
| 3c | Report the strategies participants used | ||
| 3d | Report methods used for online-data processing and artefact correction | p. 4 | |
| 3e | Report condition and group effects for artefacts | ||
| Feedback specifications | |||
| 4a | Report how the online-feature extraction was defined | ||
| 4b | Report and justify the reinforcement schedule | p. 6 | |
| 4c | Report the feedback modality and content | p. 6 | |
| 4d | Collect and report all brain activity variable(s) and/or contrasts used for feedback, as displayed to experimental participants | p. 6 | |
| 4e | Report the hardware and software used | p. 6. | |
| Outcome measures | |||
| pre-experiment | 5a | Report neurofeedback regulation success based on the feedback signal | p. 9 |
| 5b | Plot within-session and between-session regulation blocks of feedback variable(s), as well as pre-to-post resting baselines or contrasts | p. 8 | |
| 5c | Statistically compare the experimental condition/group to the control condition(s)/group(s) (not only each group to baseline measures) | Table 2, Table 3 | |
| pre-experiment | 6a | Include measures of clinical or behavioural significance, defined a priori, and describe whether they were reached | p. 9 |
| 6b | Run correlational analyses between regulation success and behavioural outcomes | p. 10 | |
| Data Storage | |||
| 7a | Upload all materials, analysis scripts, code, and raw data used for analyses, as well as final values, to an open access data repository, when feasible |
References
- ICDL. Regulatory Sensory Processing Disorder Access 1. In Diagnostic Manual for Infancy and Early Childhood: Mental Health, Developmental, Regulatory–Sensory Processing and Language Disorders and Learning Challenges (ICDL–DMIC); The Interdisciplinary Council on Development and Learning, Inc.: Bethesda, MD, USA, 2005. [Google Scholar]
- Miller, L.J.; Anzalone, M.E.; Lane, S.J.; Cermak, S.A.; Osten, E.T. Concept Evolution in Sensory Integration: A Proposed Nosology for Diagnosis. Am. J. Occup. Ther. 2007, 61, 135–140. [Google Scholar] [CrossRef] [Green Version]
- PDM Task Force. PDM, Psychodynamic Diagnostic Manual; Alliance of Psychoanalytic Organizations: Silver Spring, MD, USA, 2006. [Google Scholar]
- Zero, Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood, Revised (DC:0–3R); Anxiety: Current Trends in Theory and Research; Academic Press: New York, NY, USA, 1972; pp. 3–19.
- Bar-Shalita, T.; Deutsch, L.; Honigman, L.; Weissman-Fogel, I. Ecological aspects of pain in sensory modulation disorder. Res. Dev. Disabil. 2015, 45–46, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Meredith, P.J.; Rappel, G.; Strong, J.; Bailey, K.J. Sensory Sensitivity and Strategies for Coping with Pain. Am. J. Occup. Ther. 2015, 69, 6904240010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bar-Shalita, T.; Vatine, J.-J.; Seltzer, Z.; Parush, S. Psychophysical correlates in children with sensory modulation disorder (SMD). Physiol. Behav. 2009, 98, 631–639. [Google Scholar] [CrossRef]
- Bar-Shalita, T.; Vatine, J.-J.; Parush, S.; Deutsch, L.; Seltzer, Z. Psychophysical correlates in adults with sensory modulation disorder. Disabil. Rehabil. 2011, 34, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Bar-Shalita, T.; Vatine, J.-J.; Yarnitsky, D.; Parush, S.; Weissman-Fogel, I. Atypical central pain processing in sensory modulation disorder: Absence of temporal summation and higher after-sensation. Exp. Brain Res. 2014, 232, 587–595. [Google Scholar] [CrossRef]
- Weissman-Fogel, I.; Granovsky, Y.; Bar-Shalita, T. Sensory Over-Responsiveness among Healthy Subjects is Associated with a Pronociceptive State. Pain Pract. 2018, 18, 473–486. [Google Scholar] [CrossRef] [PubMed]
- Bar-Shalita, T.; Ben-Ziv, N.; Granovsky, Y.; Weissman-Fogel, I. An Exploratory Study Testing Autonomic Reactivity to Pain in Women with Sensory Over-Responsiveness. Brain Sci. 2020, 10, 819. [Google Scholar] [CrossRef]
- Schaaf, R.C.; Benevides, T.W.; Blanche, E.; Brett-Green, B.A.; Burke, J.; Cohn, E.; Koomar, J.; Lane, S.J.; Miller, L.J.; May-Benson, T.A.; et al. Parasympathetic functions in children with sensory processing disorder. Front. Integr. Neurosci. 2010, 4, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bar-Shalita, T.; Granovsky, Y.; Parush, S.; Weissman-Fogel, I. Sensory Modulation Disorder (SMD) and Pain: A New Perspective. Front. Integr. Neurosci. 2019, 13, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bar-Shalita, T.; Cermak, S.A. Atypical Sensory Modulation and Psychological Distress in the General Population. Am. J. Occup. Ther. 2016, 70, 7004250010. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, K.L.H.; Baranek, G.; Copeland, W.E.; Compton, S.; Zucker, N.; Dawson, G.; Egger, H. Sensory Over-Responsivity: An Early Risk Factor for Anxiety and Behavioral Challenges in Young Children. J. Abnorm. Child Psychol. 2019, 47, 1075–1088. [Google Scholar] [CrossRef]
- Kinnealey, M.; Koenig, K.P.; Smith, S. Relationships Between Sensory Modulation and Social Supports and Health-Related Quality of Life. Am. J. Occup. Ther. 2011, 65, 320–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chadwick, A.; Frazier, A.; Khan, T.W.; Young, E. Understanding the Psychological, Physiological, and Genetic Factors Affecting Precision Pain Medicine: A Narrative Review. J. Pain Res. 2021, 14, 3145–3161. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.S.; Ben-Sasson, A.; Briggs-Gowan, M.J. Sensory Over-Responsivity, Psychopathology, and Family Impairment in School-Aged Children. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 1210–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosbey, J.; Johnston, S.S.; Dunn, M.L. Sensory Processing Disorders and Social Participation. Am. J. Occup. Ther. 2010, 64, 462–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, R.R.; Miller, L.J.; Milberger, S.; McIntosh, D.N. Prevalence of Parents’ Perceptions of Sensory Processing Disorders Among Kindergarten Children. Am. J. Occup. Ther. 2004, 58, 287–293. [Google Scholar] [CrossRef] [Green Version]
- Ben-Sasson, A.; Carter, A.S.; Briggs-Gowan, M.J. Sensory Over-Responsivity in Elementary School: Prevalence and Social-Emotional Correlates. J. Abnorm. Child Psychol. 2009, 37, 705–716. [Google Scholar] [CrossRef]
- Granovsky, Y.; Shor, M.; Shifrin, A.; Sprecher, E.; Yarnitsky, D.; Bar-Shalita, T. Assessment of Responsiveness to Everyday Non-Noxious Stimuli in Pain-Free Migraineurs with vs. without Aura. J. Pain 2018, 19, 943–951. [Google Scholar] [CrossRef]
- Mouraux, A.; Diukova, A.; Lee, M.C.; Wise, R.G.; Iannetti, G.D. A multisensory investigation of the functional significance of the “pain matrix”. Neuroimage 2011, 54, 2237–2249. [Google Scholar] [CrossRef]
- Schrepf, A.; Williams, D.A.; Gallop, R.; Naliboff, B.D.; Basu, N.; Kaplan, C.; Harper, D.E.; Landis, J.R.; Clemens, J.Q.; Strachan, E.; et al. Sensory sensitivity and symptom severity represent unique dimensions of chronic pain: A MAPP Research Network study. Pain 2018, 159, 2002–2011. [Google Scholar] [CrossRef] [PubMed]
- Senkowski, D.; Höfle, M.; Engel, A.K. Crossmodal shaping of pain: A multisensory approach to nociception. Trends Cogn. Sci. 2014, 18, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Carrillo-De-La-Peña, M.; Vallet, M.; Pérez, M.; Gómez-Perretta, C. Intensity Dependence of Auditory-Evoked Cortical Potentials in Fibromyalgia Patients: A Test of the Generalized Hypervigilance Hypothesis. J. Pain 2006, 7, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Geisser, M.E.; Glass, J.M.; Rajcevska, L.D.; Clauw, D.J.; Williams, D.A.; Kileny, P.R.; Gracely, R.H. A Psychophysical Study of Auditory and Pressure Sensitivity in Patients with Fibromyalgia and Healthy Controls. J. Pain 2008, 9, 417–422. [Google Scholar] [CrossRef]
- Hollins, M.; Harper, D.; Gallagher, S.; Owings, E.W.; Lim, P.F.; Miller, V.; Siddiqi, M.Q.; Maixner, W. Perceived intensity and unpleasantness of cutaneous and auditory stimuli: An evaluation of the generalized hypervigilance hypothesis. Pain 2009, 141, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Inal, Ö.; Aras, B.; Salar, S. Investigation of the relationship between kinesiophobia and sensory processing in fibromyalgia patients. Somatosens. Mot. Res. 2020, 37, 92–96. [Google Scholar] [CrossRef]
- Borini, C.A.; Gatti, F.R.; Grezos, R.M.L.; Fragoso, Y.D. Odors as triggering and worsening factors in migraine. Rev. Neurociências 2008, 16, 38–40. [Google Scholar] [CrossRef]
- Friedman, D.I.; De Ver Dye, T. Migraine and the environment. Headache J. Head Face Pain 2009, 49, 941–952. [Google Scholar] [CrossRef]
- Schwedt, T.J. Multisensory integration in migraine. Curr. Opin. Neurol. 2013, 26, 248–253. [Google Scholar] [CrossRef] [Green Version]
- Vanagaite, J.; Pareja, J.A.; St⊘Ren, O.; White, L.R.; Sanc, T.; Stovner, L.J. Light-Induced Discomfort and Pain in Migraine. Cephalalgia 1997, 17, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Bar-Shalita, T.; Livshitz, A.; Levin-Meltz, Y.; Rand, D.; Deutsch, L.; Vatine, J.-J. Sensory modulation dysfunction is associated with Complex Regional Pain Syndrome. PLoS ONE 2018, 13, e0201354. [Google Scholar] [CrossRef]
- Kim, J.A.; Davis, K.D. Neural Oscillations: Understanding a Neural Code of Pain. Neuroscientist 2021, 27, 544–570. [Google Scholar] [CrossRef]
- Koziol, L.F.; Budding, D.E.; Chidekel, D. Sensory Integration, Sensory Processing, and Sensory Modulation Disorders: Putative Functional Neuroanatomic Underpinnings. Cerebellum 2011, 10, 770–792. [Google Scholar] [CrossRef]
- Noseda, R.; Burstein, R. Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, cortical spreading depression, sensitization, and modulation of pain. PAIN 2013, 154, S44–S53. [Google Scholar] [CrossRef] [Green Version]
- Cohen, M.X. Where does EEG come from and what does it mean? Trends Neurosci. 2017, 40, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Jensen, O.; Mazaheri, A. Shaping Functional Architecture by Oscillatory Alpha Activity: Gating by Inhibition. Front. Hum. Neurosci. 2010, 4, 186. [Google Scholar] [CrossRef] [Green Version]
- Babiloni, C.; Babiloni, F.; Carducci, F.; Cincotti, F.; Rosciarelli, F.; Arendt-Nielsen, L.; Chen, A.C.; Rossini, P.M. Human brain oscillatory activity phase-locked to painful electrical stimulations: A multi-channel EEG study. Hum. Brain Mapp. 2002, 15, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.-F.; Arendt-Nielsen, L.; Graven-Nielsen, T.; Chen, A.C. Psychophysical and EEG responses to repeated experimental muscle pain in humans: Pain intensity encodes EEG activity. Brain Res. Bull. 2003, 59, 533–543. [Google Scholar] [CrossRef]
- Giehl, J.; Meyer-Brandis, G.; Kunz, M.; Lautenbacher, S. Responses to tonic heat pain in the ongoing EEG under conditions of controlled attention. Somatosens. Mot. Res. 2014, 31, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.; Bartling, J.; Pachur, D.; Woikowsky-Biedau, S.; Lautenbacher, S. EEG responses to tonic heat pain. Exp. Brain Res. 2006, 173, 14–24. [Google Scholar] [CrossRef]
- Hassan, M.A.; Fraser, M.; Conway, B.A.; Allan, D.B.; Vuckovic, A. The mechanism of neurofeedback training for treatment of central neuropathic pain in paraplegia: A pilot study. BMC Neurol. 2015, 15, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kayıran, S.; Dursun, E.; Dursun, N.; Ermutlu, N.; Karamürsel, S. Neurofeedback Intervention in Fibromyalgia Syndrome; a Randomized, Controlled, Rater Blind Clinical Trial. Appl. Psychophysiol. Biofeedback 2010, 35, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Mayaud, L.; Wu, H.; Barthélemy, Q.; Favennec, P.; Delpierre, Y.; Congedo, M.; Dupeyron, A.; Ritz, M. Alpha-phase synchrony EEG training for multi-resistant chronic low back pain patients: An open-label pilot study. Eur. Spine J. 2019, 28, 2487–2501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, K.; Henshaw, J.; Sutherland, H.; Taylor, J.R.; Casson, A.J.; Lopez-Diaz, K.; Brown, C.A.; Jones, A.K.P.; Sivan, M.; Trujillo-Barreto, N.J. Using EEG Alpha States to Understand Learning During Alpha Neurofeedback Training for Chronic Pain. Front. Neurosci. 2021, 14, 1448. [Google Scholar] [CrossRef] [PubMed]
- Granovsky, Y.; Weissman-Fogel, I.; Bar-Shalita, T. Resting-State Electroencephalography in Participants with Sensory Overresponsiveness: An Exploratory Study. Am. J. Occup. Ther. 2019, 73, 7301205100p1. [Google Scholar] [CrossRef]
- Kosek, E.; Clauw, D.; Nijs, J.; Baron, R.; Gilron, I.; Harris, R.E.; Mico, J.-A.; Rice, A.S.; Sterling, M. Chronic nociplastic pain affecting the musculoskeletal system: Clinical criteria and grading system. Pain 2021, 162, 2629–2634. [Google Scholar] [CrossRef]
- Micoulaud-Franchi, J.A.; Jeunet, C.; Pelissolo, A.; Ros, T. EEG Neurofeedback for Anxiety Disorders and Post-Traumatic Stress Disorders: A Blueprint for a Promising Brain-Based Therapy. Curr. Psychiatry Rep. 2021, 23, 84. [Google Scholar] [CrossRef]
- Ros, T.; Enriquez-Geppert, S.; Zotev, V.; Young, K.D.; Wood, G.; Whitfield-Gabrieli, S.; Wan, F.; Vuilleumier, P.; Vialatte, F.; Van De Ville, D.; et al. Consensus on the reporting and experimental design of clinical and cognitive-behavioural neurofeedback studies (CRED-nf checklist). Brain 2020, 143, 1674–1685. [Google Scholar] [CrossRef] [Green Version]
- Ros, T.; Baars, B.J.; Lanius, R.A.; Vuilleumier, P. Tuning pathological brain oscillations with neurofeedback: A systems neuroscience framework. Front. Hum. Neurosci. 2014, 8, 1008. [Google Scholar] [CrossRef] [Green Version]
- Roy, R.; De La Vega, R.; Jensen, M.P.; Miró, J. Neurofeedback for Pain Management: A Systematic Review. Front. Neurosci. 2020, 14, 671. [Google Scholar] [CrossRef]
- Bagdasaryan, J.; Le Van Quyen, M. Experiencing your brain: Neurofeedback as a new bridge between neuroscience and phenomenology. Front. Hum. Neurosci. 2013, 7, 680. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.-L.; Fang, S.-C.; Chen, S.-C.; Tai, C.-J.; Tsai, P.-S. Effects of Neurofeedback on Fibromyalgia: A Randomized Controlled Trial. Pain Manag. Nurs. 2021, 2, 755–763. [Google Scholar] [CrossRef]
- Patel, K.; Sutherland, H.; Henshaw, J.; Taylor, J.R.; Brown, C.A.; Casson, A.J.; Trujillo-Barreton, N.J.; Jones, A.K.P.; Sivan, M. Effects of neurofeedback in the management of chronic pain: A systematic review and meta-analysis of clinical trials. Eur. J. Pain 2020, 24, 1440–1457. [Google Scholar] [CrossRef]
- Prinsloo, S.; Novy, D.; Driver, L.; Lyle, R.; Ramondetta, L.; Eng, C.; Lopez, G.; Li, Y.; Cohen, L. The Long-Term Impact of Neurofeedback on Symptom Burden and Interference in Patients with Chronic Chemotherapy-Induced Neuropathy: Analysis of a Randomized Controlled Trial. J. Pain Symptom Manag. 2018, 55, 1276–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.P.; Sherlin, L.H.; Askew, R.; Fregni, F.; Witkop, G.; Gianas, A.; Howe, J.; Hakimian, S. Effects of non-pharmacological pain treatments on brain states. Clin. Neurophysiol. 2013, 124, 2016–2024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farahani, D.M.; Tavallaie, S.A.; Ahmadi, K.; Ashtiani, A.F.; Sheikh, M.; Yahaghi, E. Comparison of Neurofeedback and Transcutaneous Electrical Nerve Stimulation Efficacy on Treatment of Primary Headaches: A Randomized Controlled Clinical Trial. Iran. Red Crescent Med. J. 2014, 16, e17799. [Google Scholar] [CrossRef] [Green Version]
- Volf, N.; Belousova, L.; Knyazev, G.; Kulikov, A. Gender differences in association between serotonin transporter gene polymorphism and resting-state EEG activity. Neuroscience 2015, 284, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Kuo, M.-F.; Paulus, W.; Nitsche, M.A. Sex differences in cortical neuroplasticity in humans. Neuroreport 2006, 17, 1703–1707. [Google Scholar] [CrossRef] [PubMed]
- Assayag, N.; Bonneh, Y.; Parush, S.; Mell, H.; Neeman, R.K.; Bar-Shalita, T. Perceived Sensitivity to Pain and Responsiveness to Non-noxious Sensation in Substance Use Disorder. Pain Med. 2020, 21, 1902–1912. [Google Scholar] [CrossRef]
- Fernández-Serrano, M.J.; Perez-Garcia, M.; Perales, J.C.; Verdejo-Garcia, A. Prevalence of executive dysfunction in cocaine, heroin and alcohol users enrolled in therapeutic communities. Eur. J. Pharmacol. 2010, 626, 104–112. [Google Scholar] [CrossRef]
- Dimpfel, W.; Schober, F. The influence of caffeine on human EEG under resting condition and during mental loads. Klin. Wochenschr. 1993, 71, 197–207. [Google Scholar] [CrossRef]
- Kähkönen, S.; Wilenius, J.; Nikulin, V.V.; Ollikainen, M.; Ilmoniemi, R.J. Alcohol Reduces Prefrontal Cortical Excitability in Humans: A Combined TMS and EEG Study. Neuropsychopharmacology 2003, 28, 747–754. [Google Scholar] [CrossRef]
- Lansbergen, M.M.; Van Dongen-Boomsma, M.; Buitelaar, J.K.; Slaats-Willemse, D. ADHD and EEG-neurofeedback: A double-blind randomized placebo-controlled feasibility study. J. Neural Transm. 2011, 118, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Perreau-Linck, E.; Lessard, N.; Levesque, J.; Beauregard, M. Effects of Neurofeedback Training on Inhibitory Capacities in ADHD Children: A Single-Blind, Randomized, Placebo-Controlled Study. J. Neurother. 2010, 14, 229–242. [Google Scholar] [CrossRef] [Green Version]
- Kalig-Amir, M.; Berger, I.; Rigbi, A.; Bar-Shalita, T. An exploratory study of parent–child association in sensory modulation disorder involving ADHD-related symptoms. Pediatr. Res. 2019, 86, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Mazor-Karsenty, T.; Parush, S.; Bonneh, Y.; Shalev, L. Comparing the executive attention of adult females with ADHD to that of females with sensory modulation disorder (SMD) under aversive and non-aversive auditory conditions. Res. Dev. Disabil. 2015, 37, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Mazor-Karsenty, T.; Parush, S.; Shalev, L. Sustained attention in sensory modulation disorder and attention deficit/hyperactivity disorder. Res. Dev. Disabil. 2019, 88, 22–29. [Google Scholar] [CrossRef]
- Parush, S.; Sohmer, H.; Steinberg, A.; Kaitz, M. Somatosensory function in boys with ADHD and tactile defensiveness. Physiol. Behav. 2007, 90, 553–558. [Google Scholar] [CrossRef]
- Bar-Shalita, T.; Seltzer, Z.; Vatine, J.-J.; Yochman, A.; Parush, S. Development and psychometric properties of the Sensory Responsiveness Questionnaire (SRQ). Disabil. Rehabil. 2009, 31, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Kropotov, J. Functional Neuromarkers for Psychiatry: Applications for Diagnosis and Treatment; Academic Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Babiloni, C.; Barry, R.J.; Başar, E.; Blinowska, K.J.; Cichocki, A.; Drinkenburg, W.H.; Klimesch, W.; Knight, R.T.; da Silva, F.L.; Nunez, P.; et al. International Federation of Clinical Neurophysiology (IFCN)—EEG research workgroup: Recommendations on frequency and topographic analysis of resting state EEG rhythms. Part 1: Applications in clinical research studies. Clin. Neurophysiol. 2020, 131, 285–307. [Google Scholar] [CrossRef]
- Diener, E.D.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Anaby, D.; Jarus, T.; Backman, C.L.; Zumbo, B.D. The Role of Occupational Characteristics and Occupational Imbalance in Explaining Well-being. Appl. Res. Qual. Life 2010, 5, 81–104. [Google Scholar] [CrossRef]
- Ruscheweyh, R.; Marziniak, M.; Stumpenhorst, F.; Reinholz, J.; Knecht, S. Pain sensitivity can be assessed by self-rating: Development and validation of the Pain Sensitivity Questionnaire. Pain 2009, 146, 65–74. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. Manual for the State-Trait Anxietry, Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Kiresuk, T.J.; Sherman, R.E. Goal attainment scaling: A general method for evaluating comprehensive community mental health programs. Community Ment. Health J. 1968, 4, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Mailloux, Z.; May-Benson, T.A.; Summers, C.A.; Miller, L.J.; Brett-Green, B.; Burke, J.P.; Cohn, E.S.; Koomar, J.A.; Parham, L.D.; Roley, S.S.; et al. Goal Attainment Scaling as a Measure of Meaningful Outcomes for Children with Sensory Integration Disorders. Am. J. Occup. Ther. 2007, 61, 254–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shefler, G.; Canetti, L.; Wiseman, H. Psychometric properties of goal-attainment scaling in the assessment of mann’s time-limited psychotherapy. J. Clin. Psychol. 2001, 57, 971–979. [Google Scholar] [CrossRef]
- Rockwood, K.; Howlett, S.; Stadnyk, K.; Carver, D.; Powell, C.; Stolee, P. Responsiveness of goal attainment scaling in a randomized controlled trial of comprehensive geriatric assessment. J. Clin. Epidemiol. 2003, 56, 736–743. [Google Scholar] [CrossRef]
- Rockwood, K.; Stadnyk, K.; Carver, D.; MacPherson, K.M.; Beanlands, H.E.; Powell, C.; Stolee, P.; Thomas, V.S.; Tonks, R.S. A Clinimetric Evaluation of Specialized Geriatric Care for Rural Dwelling, Frail Older People. J. Am. Geriatr. Soc. 2000, 48, 1080–1085. [Google Scholar] [CrossRef]
- Issachar, G.; Bar-Shalita, T.; Baruch, Y.; Horing, B.; Portnoy, S. Design and Implementation of a Novel Subject-Specific Neurofeedback Evaluation and Treatment System. Ann. Biomed. Eng. 2019, 47, 1203–1211. [Google Scholar] [CrossRef]
- Gruzelier, J.H.; Holmes, P.; Hirst, L.; Bulpin, K.; Rahman, S.; Van Run, C.; Leach, J. Replication of elite music performance enhancement following alpha/theta neurofeedback and application to novice performance and improvisation with SMR benefits. Biol. Psychol. 2014, 95, 96–107. [Google Scholar] [CrossRef]
- Gruzelier, J.H.; Thompson, T.; Redding, E.; Brandt, R.; Steffert, T. Application of alpha/theta neurofeedback and heart rate variability training to young contemporary dancers: State anxiety and creativity. Int. J. Psychophysiol. 2014, 93, 105–111. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health Research. NIHR Evaluation, Trials and Studies Coordination Centre: Glossary; NICE: London, UK, 2012. [Google Scholar]
- Orsmond, G.I.; Cohn, E.S. The distinctive features of a feasibility study: Objectives and guiding questions. OTJR Occup. Particip. Health 2015, 35, 169–177. [Google Scholar] [CrossRef]
- Jacobson, N.S.; Follette, W.C.; Revenstorf, D. Psychotherapy outcome research: Methods for reporting variability and evaluating clinical significance. Behav. Ther. 1984, 15, 336–352. [Google Scholar] [CrossRef]
- Schelly, D.; Ohl, A. Examining Clinical Meaningfulness in Randomized Controlled Trials: Revisiting the Well Elderly II. Am. J. Occup. Ther. 2019, 73, 7301205120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elbogen, E.B.; Alsobrooks, A.; Battles, S.; Molloy, K.; Dennis, P.A.; Beckham, J.C.; McLean, S.A.; Keith, J.R.; Russoniello, C. Mobile Neurofeedback for Pain Management in Veterans with TBI and PTSD. Pain Med. 2020, 22, 329–337. [Google Scholar] [CrossRef]
- Furman, A.J.; Meeker, T.; Rietschel, J.C.; Yoo, S.; Muthulingam, J.; Prokhorenko, M.; Keaser, M.L.; Goodman, R.N.; Mazaheri, A.; Seminowicz, D.A. Cerebral peak alpha frequency predicts individual differences in pain sensitivity. NeuroImage 2018, 167, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Furman, A.J.; Prokhorenko, M.; Keaser, M.L.; Zhang, J.; Chen, S.; Mazaheri, A.; Seminowicz, D.A. Sensorimotor Peak Alpha Frequency Is a Reliable Biomarker of Prolonged Pain Sensitivity. Cereb. Cortex 2020, 30, 6069–6082. [Google Scholar] [CrossRef]
- Knyazev, G.G. Motivation, emotion, and their inhibitory control mirrored in brain oscillations. Neurosci. Biobehav. Rev. 2007, 31, 377–395. [Google Scholar] [CrossRef]
- Nunez, P.; Srinivasan, R. Electric Fields of the Brain; Oxford University Press: New York, NY, USA, 2005. [Google Scholar]
- Klimesch, W. EEG alpha and theta oscillations reflect cognitive and memory performance: A review and analysis. Brain Res. Rev. 1999, 29, 169–195. [Google Scholar] [CrossRef]
- Mölle, M.; Marshall, L.; Fehm, H.L.; Born, J. EEG theta synchronization conjoined with alpha desynchronization indicate intentional encoding. Eur. J. Neurosci. 2002, 15, 923–928. [Google Scholar] [CrossRef]
- Neuper, C.; Grabner, R.H.; Fink, A.; Neubauer, A.C. Long-term stability and consistency of EEG event-related (de-)synchronization across different cognitive tasks. Clin. Neurophysiol. 2005, 116, 1681–1694. [Google Scholar] [CrossRef]
- Pfurtscheller, G. Spatiotemporal analysis of alpha frequency components with the ERD technique. Brain Topogr. 1989, 2, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Antaramian, S. The importance of very high life satisfaction for students’ academic success. Cogent Educ. 2017, 4, 1307622. [Google Scholar] [CrossRef]
- Pavot, W.; Diener, E. Review of the satisfaction with life scale. In Assessing Well-Being; Springer: Dordrecht, The Netherlands, 2009; pp. 101–117. [Google Scholar]
- Hauner, K.K.; Mineka, S.; Voss, J.; Paller, K. Exposure therapy triggers lasting reorganization of neural fear processing. Proc. Natl. Acad. Sci. USA 2012, 109, 9203–9208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becerra, J.; Fernández, T.; Harmony, T.; Caballero, M.; Garcia, F.; Fernández-Bouzas, A.; Santiago-Rodriguez, E.; Prado-Alcalá, R. Follow-up study of learning-disabled children treated with neurofeedback or placebo. Clin. EEG Neurosci. 2006, 37, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Hsu, D.; Beggs, J.M. Neuronal avalanches and criticality: A dynamical model for homeostasis. Neurocomputing 2006, 69, 1134–1136. [Google Scholar] [CrossRef]



| Characteristics | Mean | SD | % | |
|---|---|---|---|---|
| Age | 33.11 | 6.47 | ||
| SRQ-IS | Hedonic | 1.63 | 0.37 | |
| Aversive | 2.86 | 0.27 | ||
| Education | University | 55.6 | ||
| College | 22.2 | |||
| Post-graduate | 22.2 |
| Bands | T1 | T2 | T3 | T4 | RMA Significance | T1 vs. T3 Comparison | T2 vs. T3 Comparison | T1 vs. T4 Comparison | T2 vs. T4 Comparison | T3 vs. T4 Comparison | T2 vs. T3 Cohen’s d | T2 vs. T4 Cohen’s d | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p | p | p | p | p | p | |||||||
| Delta (1–4 Hz) | 16.06 (9.02) | 19.36 (17.48) | 16.08 (9.75) | 25.19 (15.21) | 4.56 | 0.01 | >0.05 | >0.05 | 0.019 | >0.05 | 0.019 | 0.29 | 0.801 |
| Theta (4–8 Hz) | 5.08 (3.00) | 4.87 (2.43) | 5.38 (3.16) | 8.40 (3.65) | 7.12 | <0.001 | >0.05 | >0.05 | 0.005 | 0.003 | 0.012 | 0.51 | 1.126 |
| Alpha (8–12 Hz) | 11.93 (9.44) | 11.60 (8.11) | 12.27 (10.31) | 12.03 (7.60) | >0.05 | 0.43 | 0.14 | ||||||
| Beta (12–30 Hz) | 2.28 (1.06) | 2.25 (0.80) | 2.30 (1.06) | 5.82 (5.16) | 3.63 | 0.02 | >0.05 | >0.05 | 0.056 | 0.064 | 0.058 | 0.42 | 0.684 |
| Gamma (>30 Hz) | 0.16 (0.04) | 0.14 (0.05) | 0.15 (0.07) | 1.42 (2.05) | 3.32 | 0.03 | >0.05 | >0.05 | 0.073 | 0.084 | 0.071 | 0.019 | 0.637 |
| Measurement | Score Range | Time 1 | Time 2 | Time 3 | Time 4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | MED | IRQ | Mean (SD) | MED | IRQ | Mean (SD) | MED | IRQ | Mean (SD) | MED | IRQ | |||
| PSQ | Total * | 0–10 | 5.45 (1.90) | 5.46 | 3.87–7.01 | 5.90 (2.13) | 6.00 | 4.46–7.51 | 5.36 (2.03) | 5.42 | 3.89–6.96 | 5.31 (2.00) | 5.14 | 3.89–6.69 |
| Minor | 0–10 | 4.84 (1.89) | 4.64 | 3.39–6.32 | 5.05 (2.19) | 5.14 | 3.25–6.42 | 4.40 (1.82) | 4.42 | 3.00–5.71 | 4.35 (1.88) | 4.42 | 2.92–5.21 | |
| Moderate | 0–10 | 6.05 (2.00) | 6.14 | 4.35–7.71 | 6.74 (2.24) | 7.14 | 5.03–8.32 | 6.32 (2.38) | 7.00 | 3.82–8.42 | 6.27 (2.32) | 6.50 | 4.50–8.10 | |
| SWLS ^ | 5–35 | 21.10 (6.26) | 19.25 | 17.25–26 | 20.40 (7.07) | 22.50 | 14.50–24.50 | 22.10 (7.43) | 23.00 | 15.00–27.00 | 23.30 (7.11) | 24.50 | 17.75–29.00 | |
| GAS *,^ | −2–+2 | −2 (0.0) | −2 | −2–−2 | −1.85 (0.33) | −2 | −2–−1.87 | −0.15 (0.68) | −0.25 | −1 −0.62 | −0.40 (1.32) | −0.5 | −1.62–0.62 | |
| STAI | State | 20–80 | 45.4 (1.90) | 5.46 | 40.75–48.5 | 46.40 (4.92) | 45.50 | 4300.−47.25 | 47.20 (3.35) | 47.50 | 44.75–50.25 | 46.50 (4.94) | 48.00 | 48–50 |
| Trait | 20–80 | 46.40 (4.29) | 47.00 | 41.75–50.25 | 45.90 (5.08) | 46.50 | 40.75–49.50 | 44.30 (4.94) | 44.00 | 39.75–47.00 | 43.80 (3.52) | 43.50 | 40.75–46.25 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamed, R.; Mizrachi, L.; Granovsky, Y.; Issachar, G.; Yuval-Greenberg, S.; Bar-Shalita, T. Neurofeedback Therapy for Sensory Over-Responsiveness—A Feasibility Study. Sensors 2022, 22, 1845. https://doi.org/10.3390/s22051845
Hamed R, Mizrachi L, Granovsky Y, Issachar G, Yuval-Greenberg S, Bar-Shalita T. Neurofeedback Therapy for Sensory Over-Responsiveness—A Feasibility Study. Sensors. 2022; 22(5):1845. https://doi.org/10.3390/s22051845
Chicago/Turabian StyleHamed, Ruba, Limor Mizrachi, Yelena Granovsky, Gil Issachar, Shlomit Yuval-Greenberg, and Tami Bar-Shalita. 2022. "Neurofeedback Therapy for Sensory Over-Responsiveness—A Feasibility Study" Sensors 22, no. 5: 1845. https://doi.org/10.3390/s22051845