
A Long Short-Term Memory Biomarker-Based Prediction Framework for Alzheimer’s Disease

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
- Projecting future clinical variations in biomarker values, only utilizing initial/benchmark information/data.
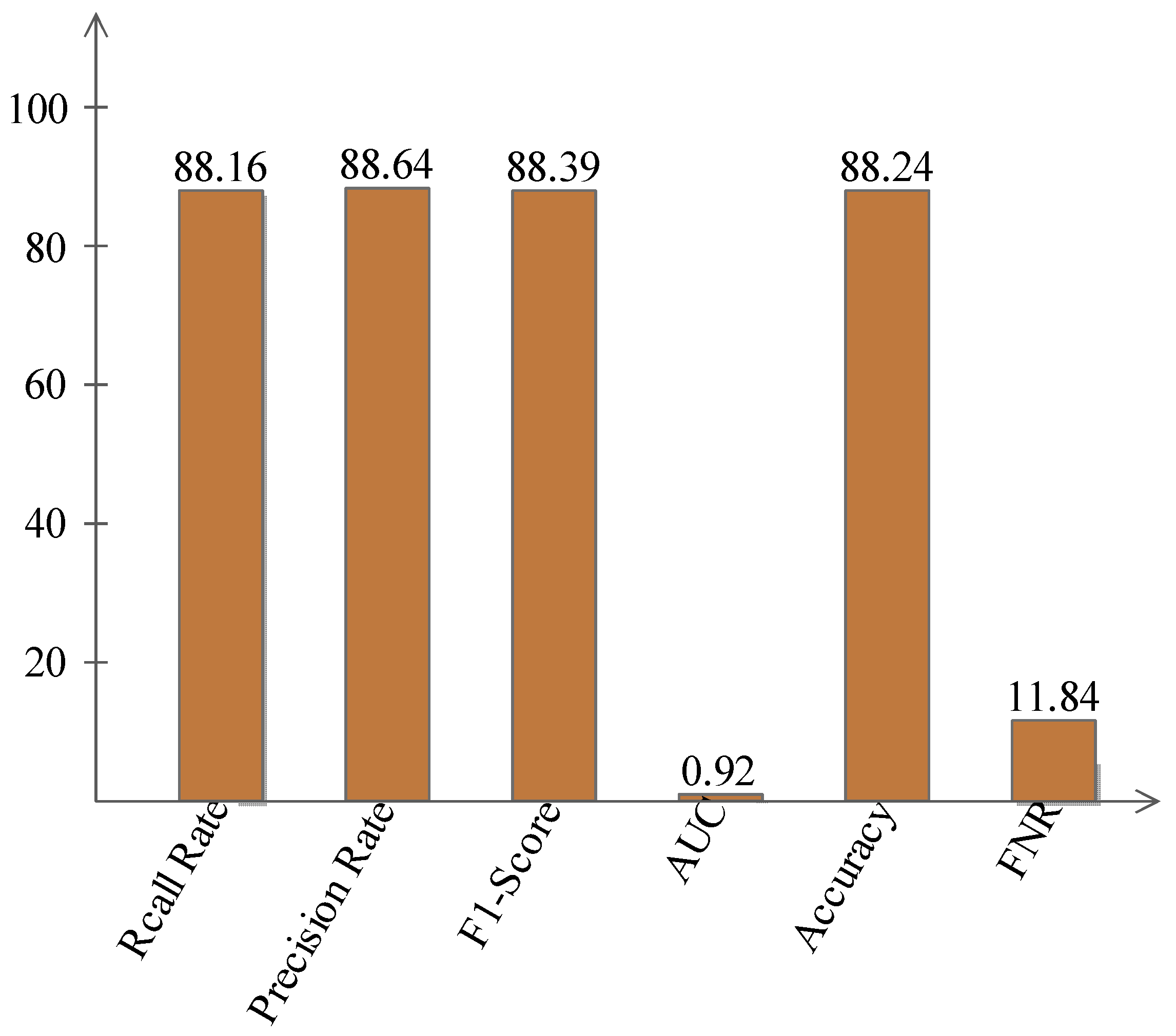
- RNN is performed to predict biomarker values and then rankings, followed by a fully connected neural network model (multi-layer perceptron) for classification, in which an accuracy of 88.24% is achieved.
- Identifying the strongest indicators of transformation in unimodal and multimodal settings.
- This study is significant for medical practitioners and health care workers in the early prediction and detection of Alzheimer’s disease; moreover, future researchers can adopt this model as a basis for their studies to further contribute to the development of algorithms for predicting Alzheimer’s disease in the future.
- This study also serves as a training tool for medical institutions to educate and train their students regarding the early prediction and development of Alzheimer’s disease.
2. Literature Review
3. Proposed Methodology
3.1. ADNI Dataset
3.2. RNN-LSTM
3.3. Multi-Layer Perceptron (MLP)
- It takes the data sources, duplicates them by their loads, and calculates their total
- It adds an inclination factor, the number 1 duplicated by a weight
- It feeds the aggregate through the enactment work
- The result is the perceptron yield
4. Results and Discussion
4.1. Results
4.2. Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ML | Machine Learning |
| AD | Alzheimer’s Disease |
| NM | Neuropsychological Measures |
| MRI | Magnetic Resonance Imaging |
| RNN | Recurrent Neural Network |
| LSTM | Long Short-Term Memory |
| MCI | Mild Cognitive Impairment |
| CNN | Convolutional Neural Network |
| MLP | Multi-Layer Perceptron |
| ANN | Artificial Neural Network |
References
- Alzheimer’s Association. 2019 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2019, 15, 321–387. [Google Scholar] [CrossRef]
- Zhan, L.; Zhou, J.; Wang, Y.; Jin, Y.; Jahanshad, N.; Prasad, G.; Nir, T.M.; Leonardo, C.D.; Ye, J.; Thompson, P.M. Comparison of nine tractography algorithms for detecting abnormal structural brain networks in Alzheimer’s disease. Front. Aging Neurosci. 2015, 7, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, F.; Liu, M.; Alzheimer’s Disease Neuroimaging Initiative. A hybrid convolutional and recurrent neural network for hippocampus analysis in Alzheimer’s disease. J. Neurosci. Methods 2019, 323, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yao, L.; Wang, X.; Monaghan, J.; Mcalpine, D.; Zhang, Y. A survey on deep learning-based non-invasive brain signals: Recent advances and new frontiers. J. Neural Eng. 2021, 18, 031002. [Google Scholar] [CrossRef] [PubMed]
- Wee, C.-Y.; Yap, P.-T.; Zhang, D.; Denny, K.; Browndyke, J.N.; Potter, G.G.; Welsh-Bohmer, K.A.; Wang, L.; Shen, D. Identification of MCI individuals using structural and functional connectivity networks. Neuroimage 2012, 59, 2045–2056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharif, M.I.; Alhussein, M.; Aurangzeb, K.; Raza, M. A decision support system for multimodal brain tumor classification using deep learning. Complex Intell. Syst. 2021, 2420. [Google Scholar] [CrossRef]
- Hussain, U.N.; Khan, M.A.; Lali, I.U.; Javed, K.; Ashraf, I.; Tariq, J.; Ali, H.; Din, A. A Unified design of ACO and skewness based brain tumor segmentation and classification from MRI scans. J. Control. Eng. Appl. Inform. 2020, 22, 43–55. [Google Scholar]
- Sharif, M.I.; Li, J.P.; Khan, M.A.; Saleem, M.A. Active deep neural network features selection for segmentation and recognition of brain tumors using MRI images. Pattern Recognit. Lett. 2020, 129, 181–189. [Google Scholar] [CrossRef]
- Nazar, U.; Khan, M.A.; Lali, I.U.; Lin, H.; Ali, H.; Ashraf, I.; Tariq, J. Review of automated computerized methods for brain tumor segmentation and classification. Curr. Med. Imaging 2020, 16, 823–834. [Google Scholar] [CrossRef]
- Khan, M.A.; Rubab, S.; Kashif, A.; Sharif, M.I.; Muhammad, N.; Shah, J.H.; Zhang, Y.-D.; Satapathy, S.C. Lungs cancer classification from CT images: An integrated design of contrast based classical features fusion and selection. Pattern Recognit. Lett. 2020, 129, 77–85. [Google Scholar] [CrossRef]
- Stebbins, G.; Murphy, C. Diffusion tensor imaging in Alzheimer’s disease and mild cognitive impairment. Behav. Neurol. 2009, 21, 39–49. [Google Scholar] [CrossRef]
- Khan, M.A.; Ashraf, I.; Alhaisoni, M.; Damaševičius, R.; Scherer, R.; Rehman, A.; Bukhari, S.A.C. Multimodal brain tumor classification using deep learning and robust feature selection: A machine learning application for radiologists. Diagnostics 2020, 10, 565. [Google Scholar] [CrossRef]
- Zhang, D.; Shen, D.; Alzheimer’s Disease Neuroimaging Initiative. Multi-modal multi-task learning for joint prediction of multiple regression and classification variables in Alzheimer’s disease. NeuroImage 2012, 59, 895–907. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.A.; Hussain, N.; Majid, A.; Alhaisoni, M.; Bukhari, S.A.C.; Kadry, S.; Nam, Y.; Zhang, Y.D. Classification of positive COVID-19 CT scans using deep learning. Comput. Mater. Contin. 2021, 66, 2923–2938. [Google Scholar] [CrossRef]
- Khan, M.A.; Kadry, S.; Zhang, Y.-D.; Akram, T.; Sharif, M.; Rehman, A.; Saba, T. Prediction of COVID-19-pneumonia based on selected deep features and one class kernel extreme learning machine. Comput. Electr. Eng. 2021, 90, 106960. [Google Scholar] [CrossRef]
- Lawrence, E.; Vegvari, C.; Ower, A.; Hadjichrysanthou, C.; De Wolf, F.; Anderson, R.M. A systematic review of longitudinal studies which measure Alzheimer’s disease biomarkers. J. Alzheimer’s Dis. 2017, 59, 1359–1379. [Google Scholar] [CrossRef] [Green Version]
- Rehman, A.; Khan, M.A.; Saba, T.; Mehmood, Z.; Tariq, U.; Ayesha, N. Microscopic brain tumor detection and classification using 3D CNN and feature selection architecture. Microsc. Res. Tech. 2021, 84, 133–149. [Google Scholar] [CrossRef]
- Franzmeier, N.; Koutsouleris, N.; Benzinger, T.; Goate, A.; Karch, C.M.; Fagan, A.M.; McDade, E.; Duering, M.; Dichgans, M.; Levin, J. Predicting sporadic Alzheimer’s disease progression via inherited Alzheimer’s disease-informed machine-learning. Alzheimer’s Dement. 2020, 16, 501–511. [Google Scholar] [CrossRef]
- Militello, C.; Rundo, L.; Dimarco, M.; Orlando, A.; Conti, V.; Woitek, R.; D’Angelo, I.; Bartolotta, T.V.; Russo, G. Semi-automated and interactive segmentation of contrast-enhancing masses on breast DCE-MRI using spatial fuzzy clustering. Biomed. Signal Process. Control. 2022, 71, 103113. [Google Scholar] [CrossRef]
- Rundo, L.; Han, C.; Zhang, J.; Hataya, R.; Nagano, Y.; Militello, C.; Ferretti, C.; Nobile, M.S.; Tangherloni, A.; Gilardi, M.C. CNN-based prostate zonal segmentation on T2-weighted MR images: A cross-dataset study. In Neural Approaches to Dynamics of Signal Exchanges; Springer: Berlin/Heidelberg, Germany, 2020; pp. 269–280. [Google Scholar]
- Rundo, L.; Militello, C.; Vitabile, S.; Russo, G.; Sala, E.; Gilardi, M.C. A survey on nature-inspired medical image analysis: A step further in biomedical data integration. Fundam. Inform. 2020, 171, 345–365. [Google Scholar] [CrossRef]
- Zemouri, R.; Zerhouni, N.; Racoceanu, D. Deep learning in the biomedical applications: Recent and future status. Appl. Sci. 2019, 9, 1526. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.A.; Muhammad, K.; Sharif, M.; Akram, T.; Albuquerque, V. Multi-Class Skin Lesion Detection and Classification via Teledermatology. IEEE J. Biomed. Health Inform. 2021, 25, 4267–4275. [Google Scholar] [CrossRef]
- Khan, M.A.; Zhang, Y.-D.; Sharif, M.; Akram, T. Pixels to classes: Intelligent learning framework for multiclass skin lesion localization and classification. Comput. Electr. Eng. 2021, 90, 106956. [Google Scholar] [CrossRef]
- Kawahara, J.; BenTaieb, A.; Hamarneh, G. Deep features to classify skin lesions. In Proceedings of the 2016 IEEE 13th International Symposium on Biomedical Imaging (ISBI), Prague, Czech Republic, 13–16 April 2016; pp. 1397–1400. [Google Scholar]
- Khan, M.A.; Lali, I.U.; Rehman, A.; Ishaq, M.; Sharif, M.; Saba, T.; Zahoor, S.; Akram, T. Brain tumor detection and classification: A framework of marker-based watershed algorithm and multilevel priority features selection. Microsc. Res. Tech. 2019, 82, 909–922. [Google Scholar] [CrossRef]
- Khan, M.-A.; Majid, A.; Hussain, N.; Alhaisoni, M.; Zhang, Y.-D.; Kadry, S.; Nam, Y. Multiclass Stomach Diseases Classification Using Deep Learning Features Optimization. Comput. Mater. Contin. 2021, 67, 3381–3399. [Google Scholar] [CrossRef]
- Rauf, H.T.; Lali, M.I.U.; Khan, M.A.; Kadry, S.; Alolaiyan, H.; Razaq, A.; Irfan, R. Time series forecasting of COVID-19 transmission in Asia Pacific countries using deep neural networks. Pers. Ubiquitous Comput. 2021, 2737. [Google Scholar] [CrossRef]
- Bai, X.; Yang, M.; Huang, T.; Dou, Z.; Yu, R.; Xu, Y. Deep-person: Learning discriminative deep features for person re-identification. Pattern Recognit. 2020, 98, 107036. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.A.; Akram, T.; Zhang, Y.-D.; Sharif, M. Attributes based skin lesion detection and recognition: A mask RCNN and transfer learning-based deep learning framework. Pattern Recognit. Lett. 2021, 143, 58–66. [Google Scholar] [CrossRef]
- Varga, D. No-Reference Image Quality Assessment with Convolutional Neural Networks and Decision Fusion. Appl. Sci. 2022, 12, 101. [Google Scholar] [CrossRef]
- Zemouri, R.; Racoceanu, D. Innovative deep learning approach for biomedical data instantiation and visualization. In Deep Learning for Biomedical Data Analysis; Springer: Berlin/Heidelberg, Germany, 2021; pp. 171–196. [Google Scholar]
- Baltres, A.; Al Masry, Z.; Zemouri, R.; Valmary-Degano, S.; Arnould, L.; Zerhouni, N.; Devalland, C. Prediction of Oncotype DX recurrence score using deep multi-layer perceptrons in estrogen receptor-positive, HER2-negative breast cancer. Breast Cancer 2020, 27, 1007–1016. [Google Scholar] [CrossRef]
- Zemouri, R.; Omri, N.; Devalland, C.; Arnould, L.; Morello, B.; Zerhouni, N.; Fnaiech, F. Breast cancer diagnosis based on joint variable selection and constructive deep neural network. In Proceedings of the 2018 IEEE 4th Middle East Conference on Biomedical Engineering (MECBME), Tunis, Tunisia, 28–30 March 2018; pp. 159–164. [Google Scholar]
- Nawaz, M.; Nazir, T.; Javed, A.; Tariq, U.; Yong, H.-S.; Khan, M.A.; Cha, J. An Efficient Deep Learning Approach to Automatic Glaucoma Detection Using Optic Disc and Optic Cup Localization. Sensors 2022, 22, 434. [Google Scholar] [CrossRef]
- Syed, H.H.; Khan, M.A.; Tariq, U.; Armghan, A.; Alenezi, F.; Khan, J.A.; Rho, S.; Kadry, S.; Rajinikanth, V. A Rapid Artificial Intelligence-Based Computer-Aided Diagnosis System for COVID-19 Classification from CT Images. Behav. Neurol. 2021, 2021, 2560388. [Google Scholar] [CrossRef]
- Zemouri, R.; Omri, N.; Morello, B.; Devalland, C.; Arnould, L.; Zerhouni, N.; Fnaiech, F. Constructive deep neural network for breast cancer diagnosis. IFAC-PapersOnLine 2018, 51, 98–103. [Google Scholar] [CrossRef]
- Basheera, S.; Ram, M.S.S. Convolution neural network–based Alzheimer’s disease classification using hybrid enhanced independent component analysis based segmented gray matter of T2 weighted magnetic resonance imaging with clinical valuation. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2019, 5, 974–986. [Google Scholar] [CrossRef]
- Basheera, S.; Ram, M.S.S. A novel CNN based Alzheimer’s disease classification using hybrid enhanced ICA segmented gray matter of MRI. Comput. Med. Imaging Graph. 2020, 81, 101713. [Google Scholar] [CrossRef]
- Tabarestani, S.; Aghili, M.; Eslami, M.; Cabrerizo, M.; Barreto, A.; Rishe, N.; Curiel, R.E.; Loewenstein, D.; Duara, R.; Adjouadi, M. A distributed multitask multimodal approach for the prediction of Alzheimer’s disease in a longitudinal study. NeuroImage 2020, 206, 116317. [Google Scholar] [CrossRef]
- Lei, B.; Yang, M.; Yang, P.; Zhou, F.; Hou, W.; Zou, W.; Li, X.; Wang, T.; Xiao, X.; Wang, S. Deep and joint learning of longitudinal data for Alzheimer’s disease prediction. Pattern Recognit. 2020, 102, 107247. [Google Scholar] [CrossRef]
- Minhas, S.; Khanum, A.; Riaz, F.; Khan, S.A.; Alvi, A. Predicting progression from mild cognitive impairment to Alzheimer’s disease using autoregressive modelling of longitudinal and multimodal biomarkers. IEEE J. Biomed. Health Inform. 2017, 22, 818–825. [Google Scholar] [CrossRef]
- Gomar, J.J.; Bobes-Bascaran, M.T.; Conejero-Goldberg, C.; Davies, P.; Goldberg, T.E.; Alzheimer’s Disease Neuroimaging Initiative. Utility of combinations of biomarkers, cognitive markers, and risk factors to predict conversion from mild cognitive impairment to Alzheimer disease in patients in the Alzheimer’s disease neuroimaging initiative. Arch. Gen. Psychiatry 2011, 68, 961–969. [Google Scholar] [CrossRef] [Green Version]
- Arco, J.E.; Ramírez, J.; Górriz, J.M.; Puntonet, C.G.; Ruz, M. Short-term prediction of MCI to AD conversion based on longitudinal MRI analysis and neuropsychological tests. In Innovation in Medicine and Healthcare 2015; Springer: Berlin/Heidelberg, Germany, 2016; pp. 385–394. [Google Scholar]
- Albright, J.; Alzheimer’s Disease Neuroimaging Initiative. Forecasting the progression of Alzheimer’s disease using neural networks and a novel preprocessing algorithm. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2019, 5, 483–491. [Google Scholar] [CrossRef]
- Gomar, J.J.; Conejero-Goldberg, C.; Davies, P.; Goldberg, T.E.; Alzheimer’s Disease Neuroimaging Initiative. Extension and refinement of the predictive value of different classes of markers in ADNI: Four-year follow-up data. Alzheimer’s Dement. 2014, 10, 704–712. [Google Scholar] [CrossRef] [Green Version]
- Zhao, K.; Duka, B.; Xie, H.; Oathes, D.J.; Calhoun, V.; Zhang, Y. A dynamic graph convolutional neural network framework reveals new insights into connectome dysfunctions in ADHD. NeuroImage 2022, 246, 118774. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, H.; Adeli, E.; Chen, X.; Liu, M.; Shen, D. Multiview feature learning with multiatlas-based functional connectivity networks for MCI diagnosis. IEEE Trans. Cybern. 2020, 1–12. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
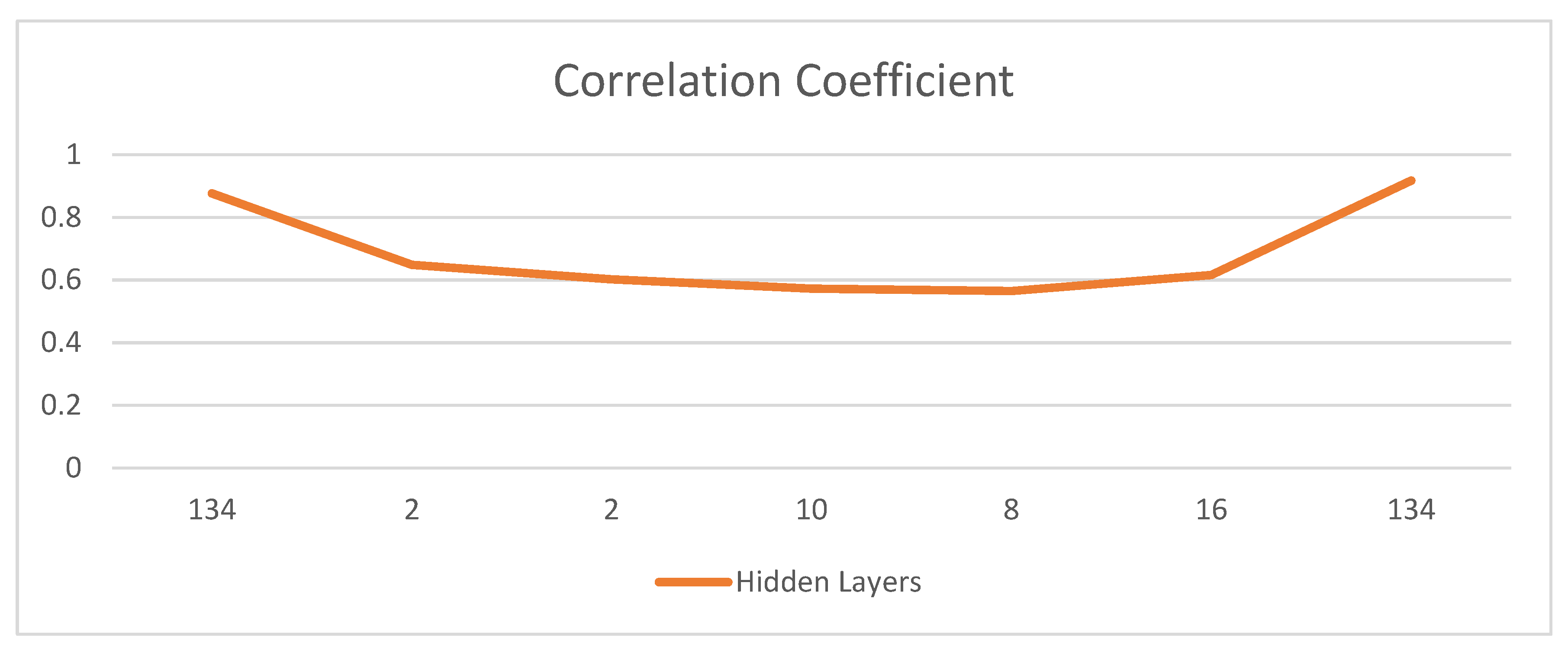
| Trials | Hidden Layers | Learning Rate | Momentum | Cross-Validation Folds | Correlation Coefficient | RMSError | Accuracy |
|---|---|---|---|---|---|---|---|
| 1 | 134 | 0.3 | 0.2 | 10 | 0.8767 | 0.13 | 86.97 |
| 2 | 2 | 0.1 | 0.1 | 10 | 0.6487 | 0.37 | 63.36 |
| 3 | 2 | 0.3 | 0.2 | 5 | 0.602 | 0.40 | 70 |
| 4 | 10 | 0.3 | 0.2 | 5 | 0.5722 | 0.45 | 55.37 |
| 5 | 8 | 0.3 | 0.2 | 10 | 0.565 | 0.46 | 48 |
| 6 | 2, 4, 8, 16 | 0.3 | 0.2 | 10 | 0.6163 | 0.38 | 61.92 |
| 7 | 134 | 0.3 | 0.2 | 5 | 0.9172 | 0.12 | 88.24 |
| Trials | Hidden Layers | Root Mean Square Error |
|---|---|---|
| 1 | 134 (10-Fold Cross-Validations) | 0.13 |
| 2 | 2 | 0.37 |
| 3 | 2 | 0.40 |
| 4 | 10 | 0.45 |
| 5 | 8 | 0.46 |
| 6 | 2, 4, 8, 16 | 0.38 |
| 7 | 134 (5-Fold Cross-Validations) | 0.12 |
| Results Comparison | ||||
|---|---|---|---|---|
| Author | Biomarkers | Sample Size | Duration (Years) | Accuracy/Precision (%) |
| Minhas et al. (2017) [42] | NM & MRI | 54 MCIp & 65 MCIs | 2 | 84.29 |
| Minhas et al. (2017) [42] | NM | 37 MCIp & 65 MCIs | 3 | 83.26 |
| Arco et al. (2016) [44] | MRI & NM | 73 MCIp & 61 MCIs | 1 | 73.95 |
| Albright et al. (2019) [45] | NM & MRI | 110 Patients | 2 | 86.6 |
| Our Results | NM & MRI | 167 MCIp & 100 MCIs | 3 | 88.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aqeel, A.; Hassan, A.; Khan, M.A.; Rehman, S.; Tariq, U.; Kadry, S.; Majumdar, A.; Thinnukool, O. A Long Short-Term Memory Biomarker-Based Prediction Framework for Alzheimer’s Disease. Sensors 2022, 22, 1475. https://doi.org/10.3390/s22041475
Aqeel A, Hassan A, Khan MA, Rehman S, Tariq U, Kadry S, Majumdar A, Thinnukool O. A Long Short-Term Memory Biomarker-Based Prediction Framework for Alzheimer’s Disease. Sensors. 2022; 22(4):1475. https://doi.org/10.3390/s22041475
Chicago/Turabian StyleAqeel, Anza, Ali Hassan, Muhammad Attique Khan, Saad Rehman, Usman Tariq, Seifedine Kadry, Arnab Majumdar, and Orawit Thinnukool. 2022. "A Long Short-Term Memory Biomarker-Based Prediction Framework for Alzheimer’s Disease" Sensors 22, no. 4: 1475. https://doi.org/10.3390/s22041475