
Reliability and Validity of an Inertial Measurement System to Quantify Lower Extremity Joint Angle in Functional Movements


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
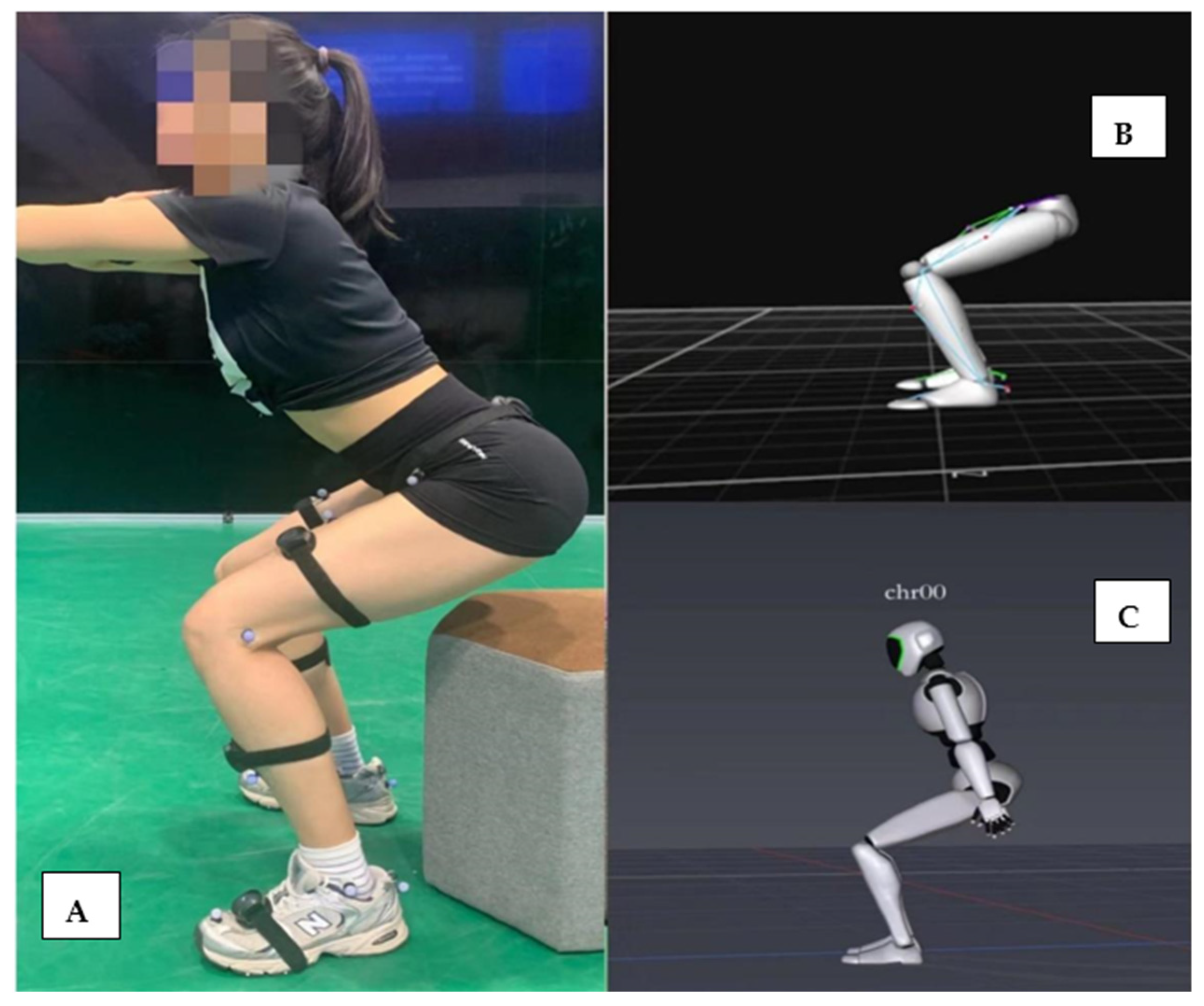
2.2. Instrumentation
2.3. Experimental Protocol
2.4. Data Processing and Analysis
2.5. Statistical Analysis
3. Results
3.1. Concurrent Validity
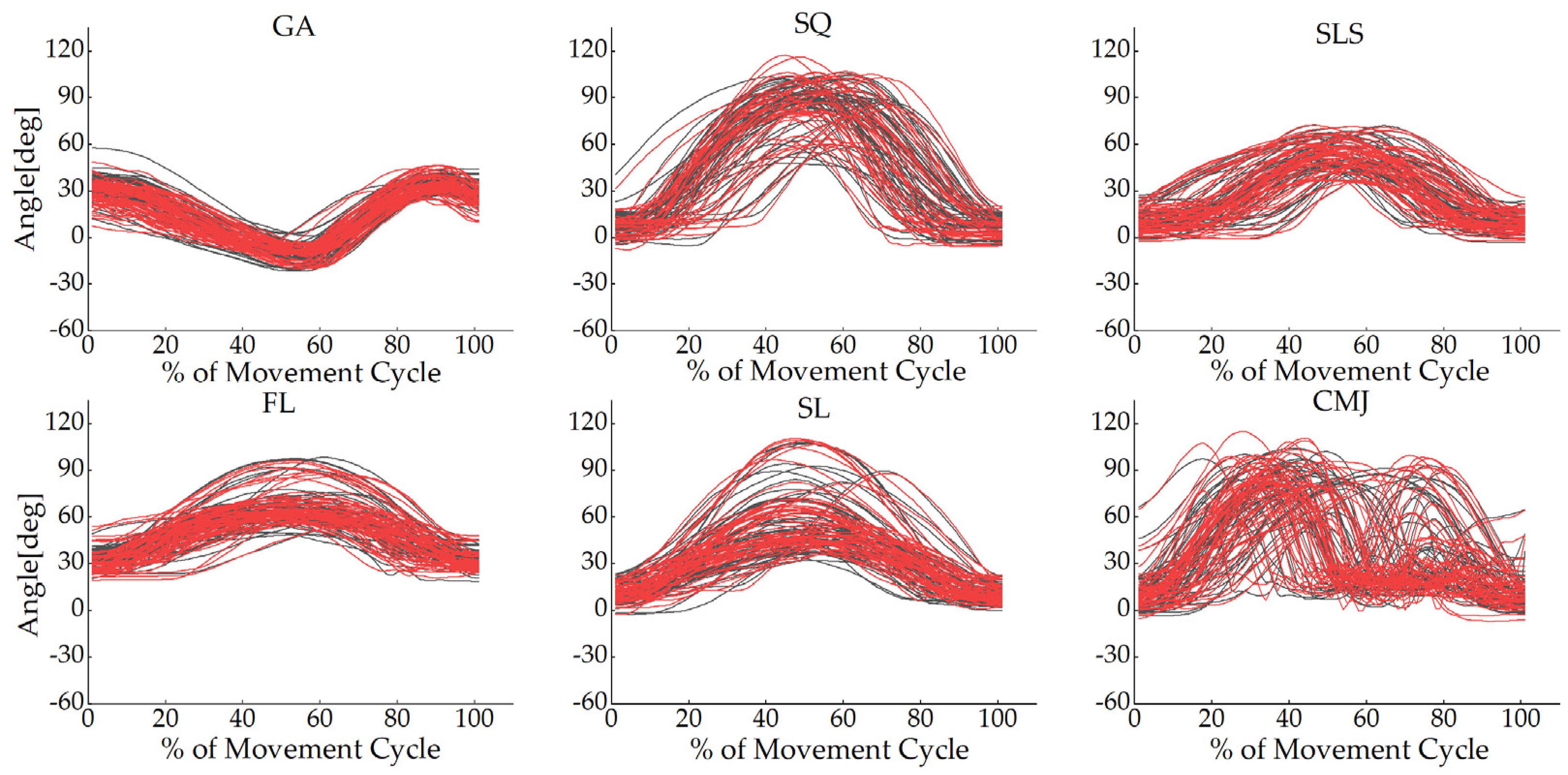
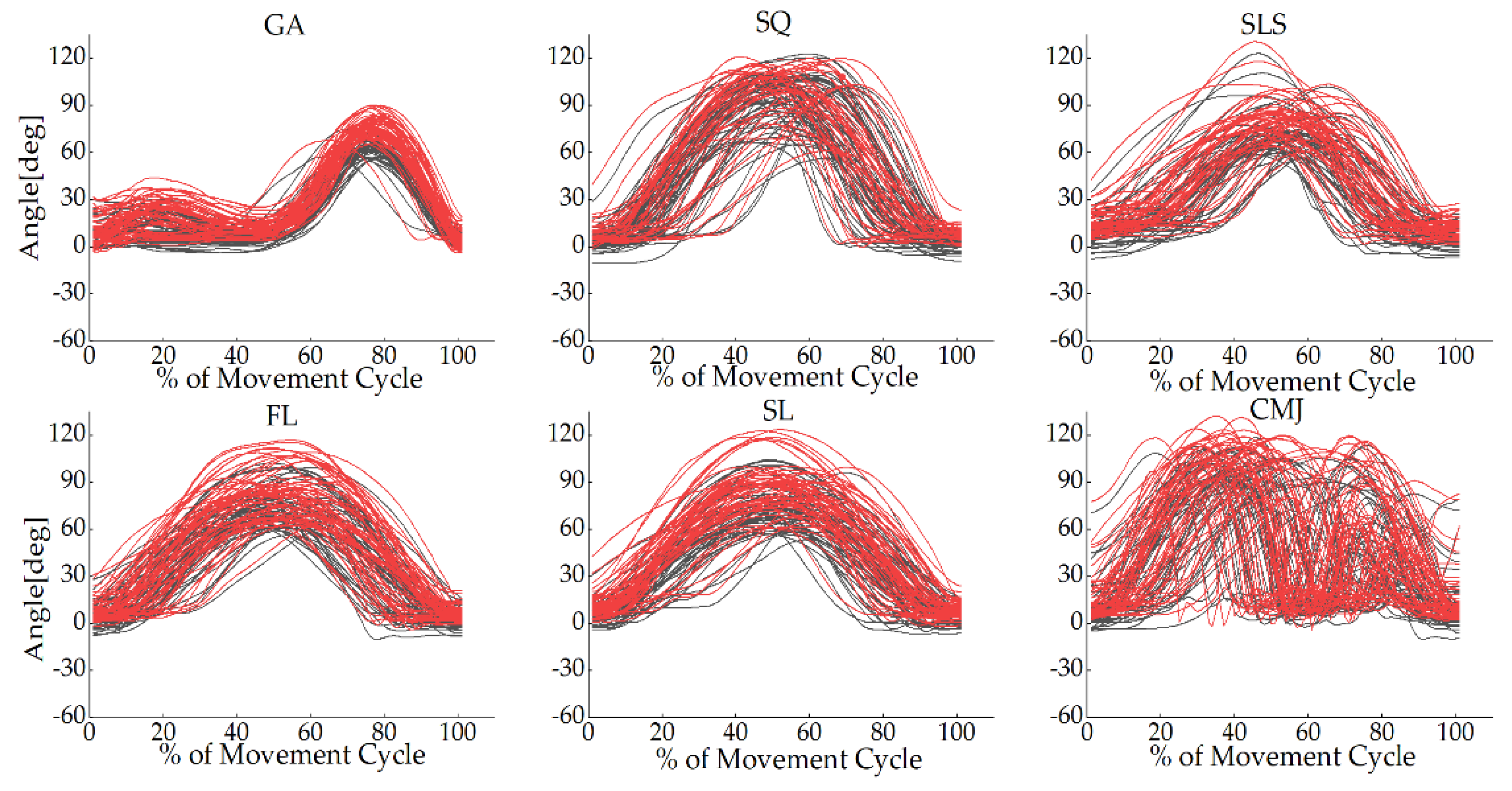
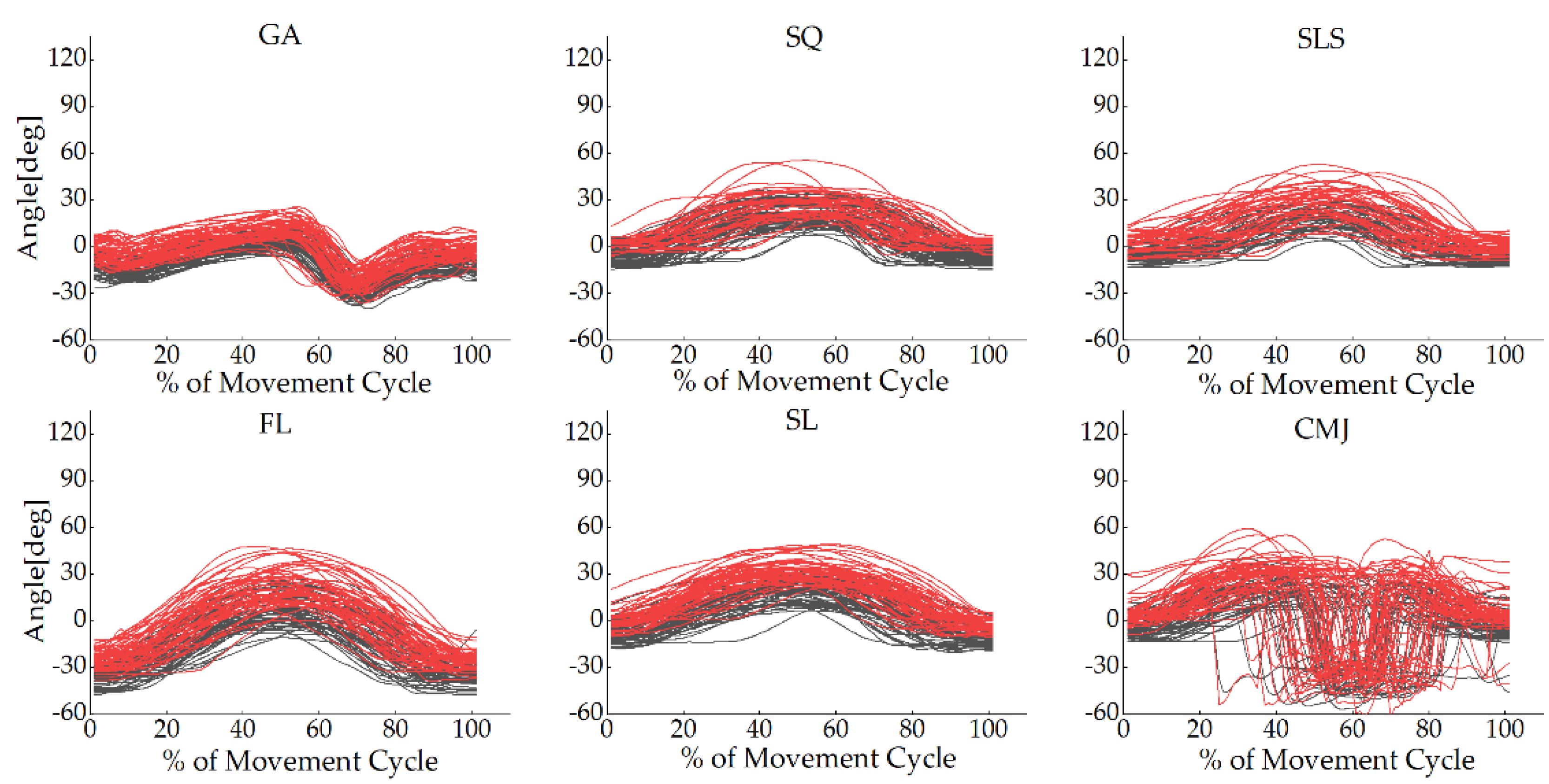
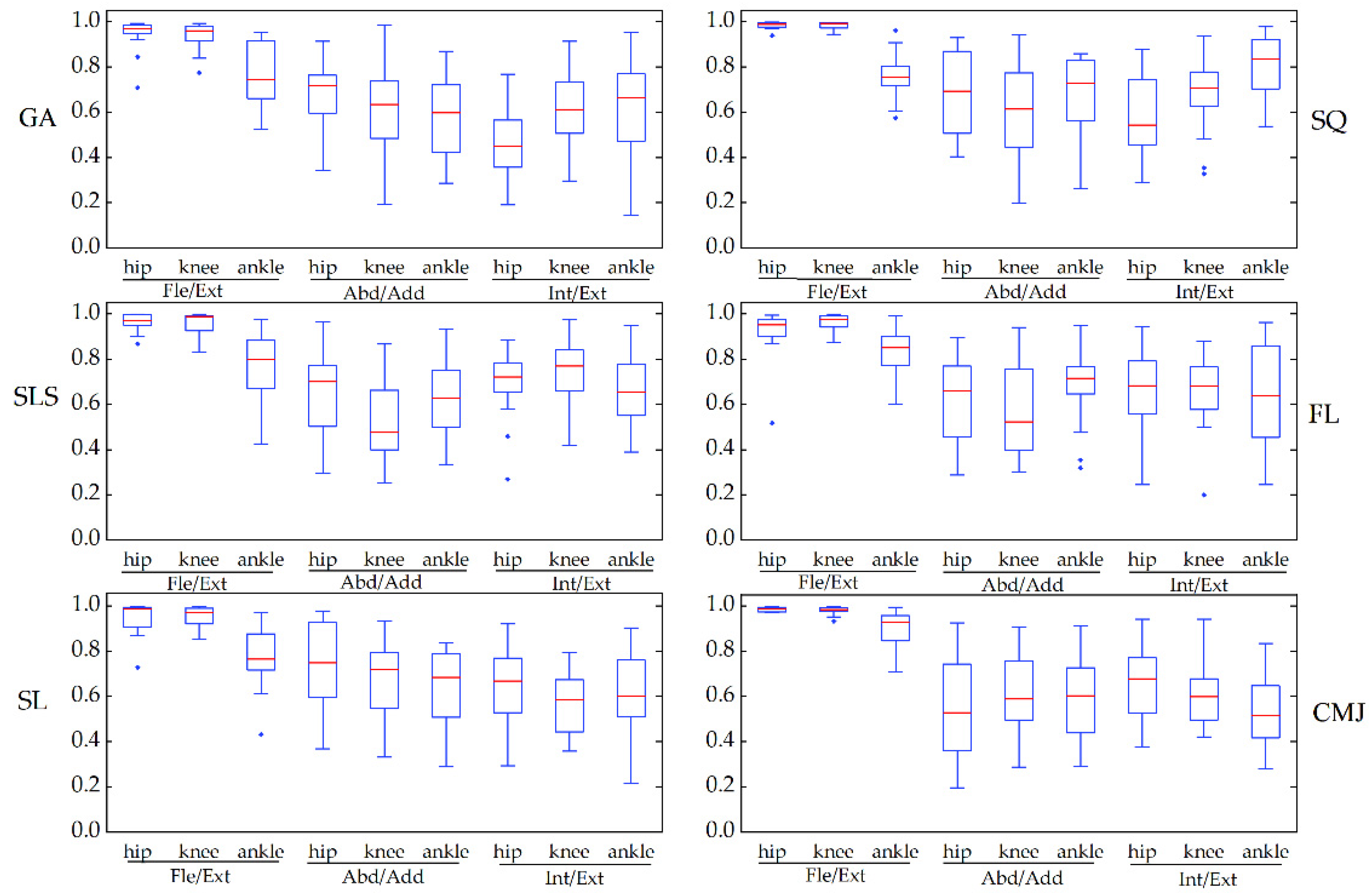
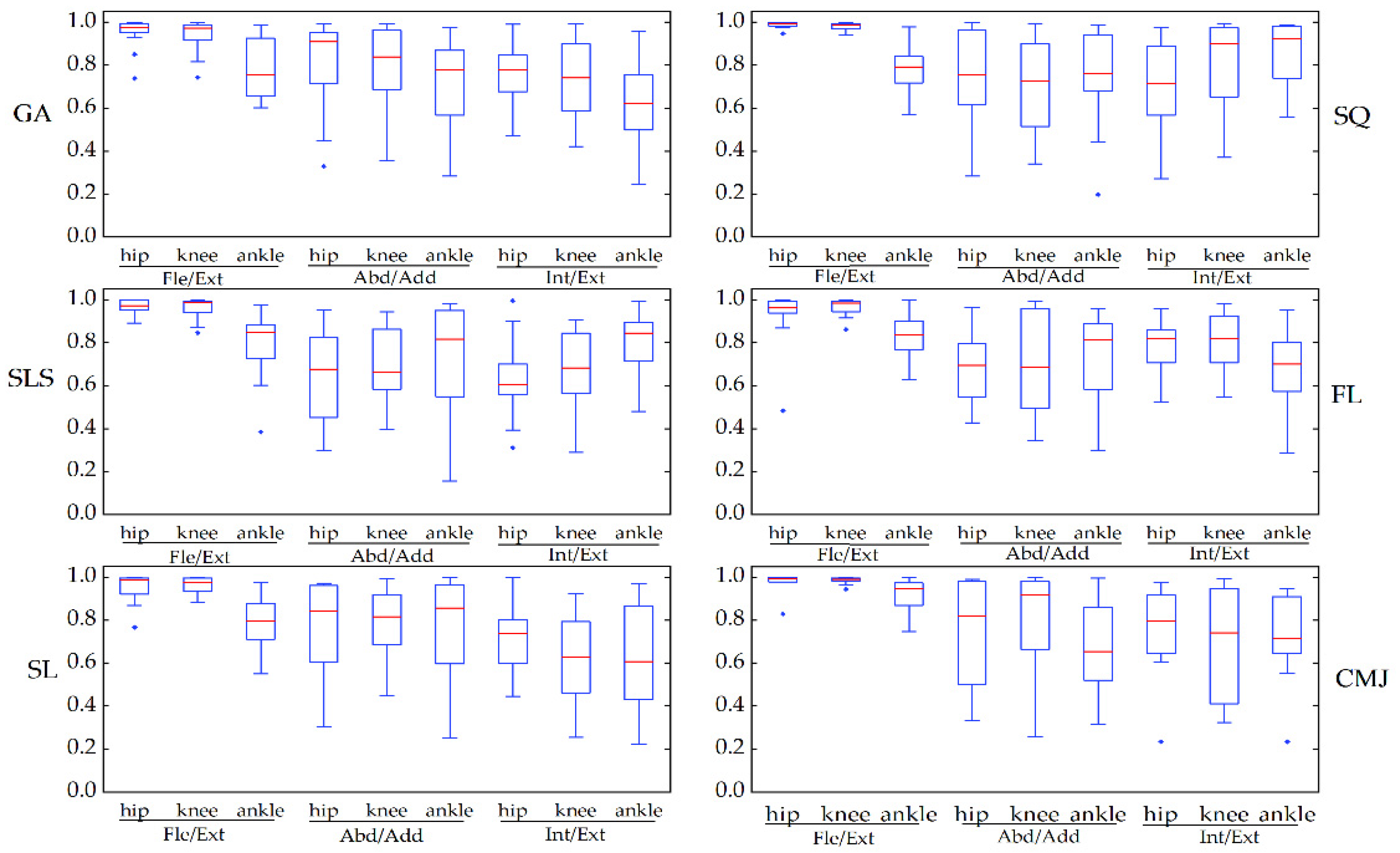
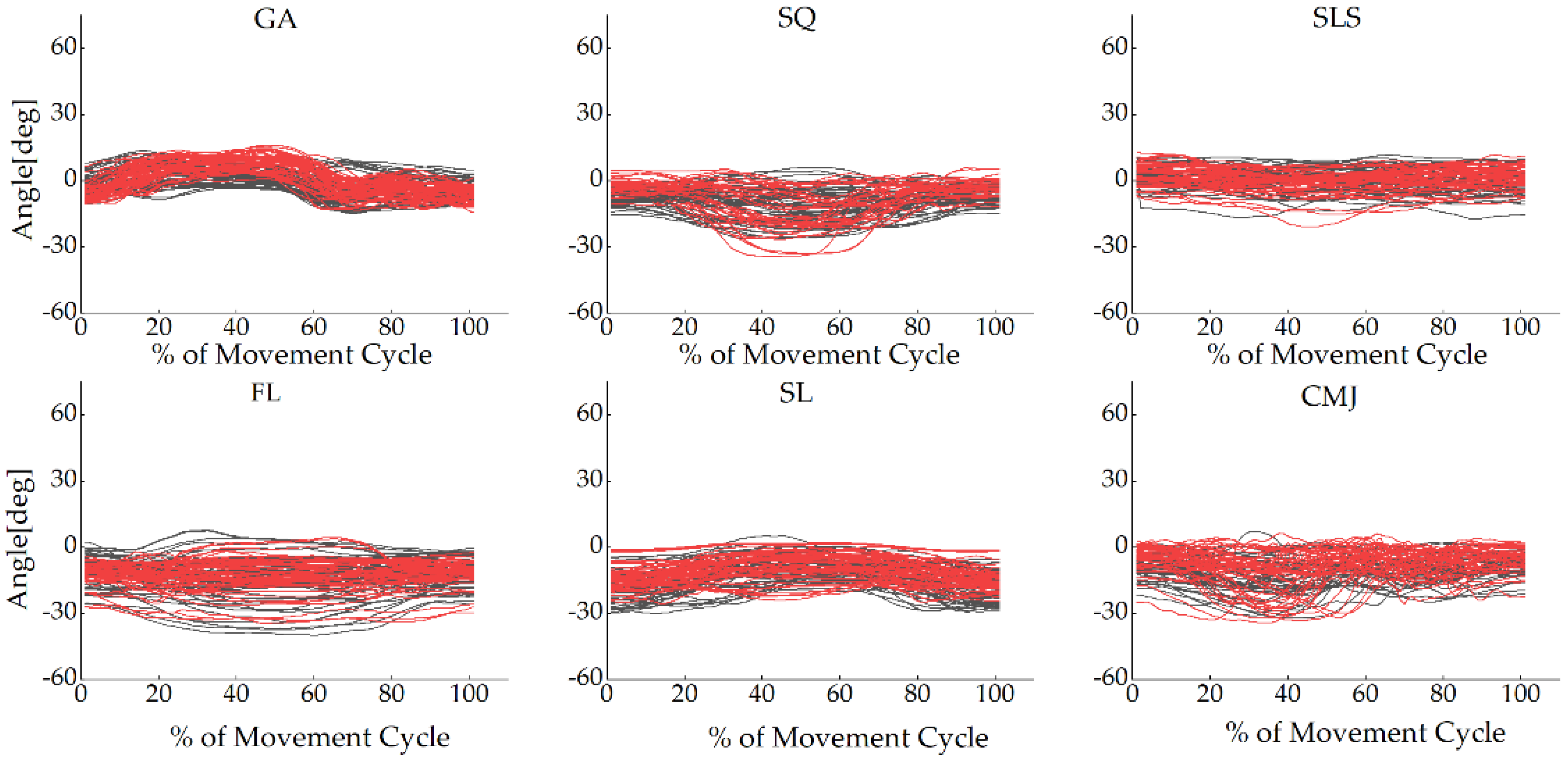
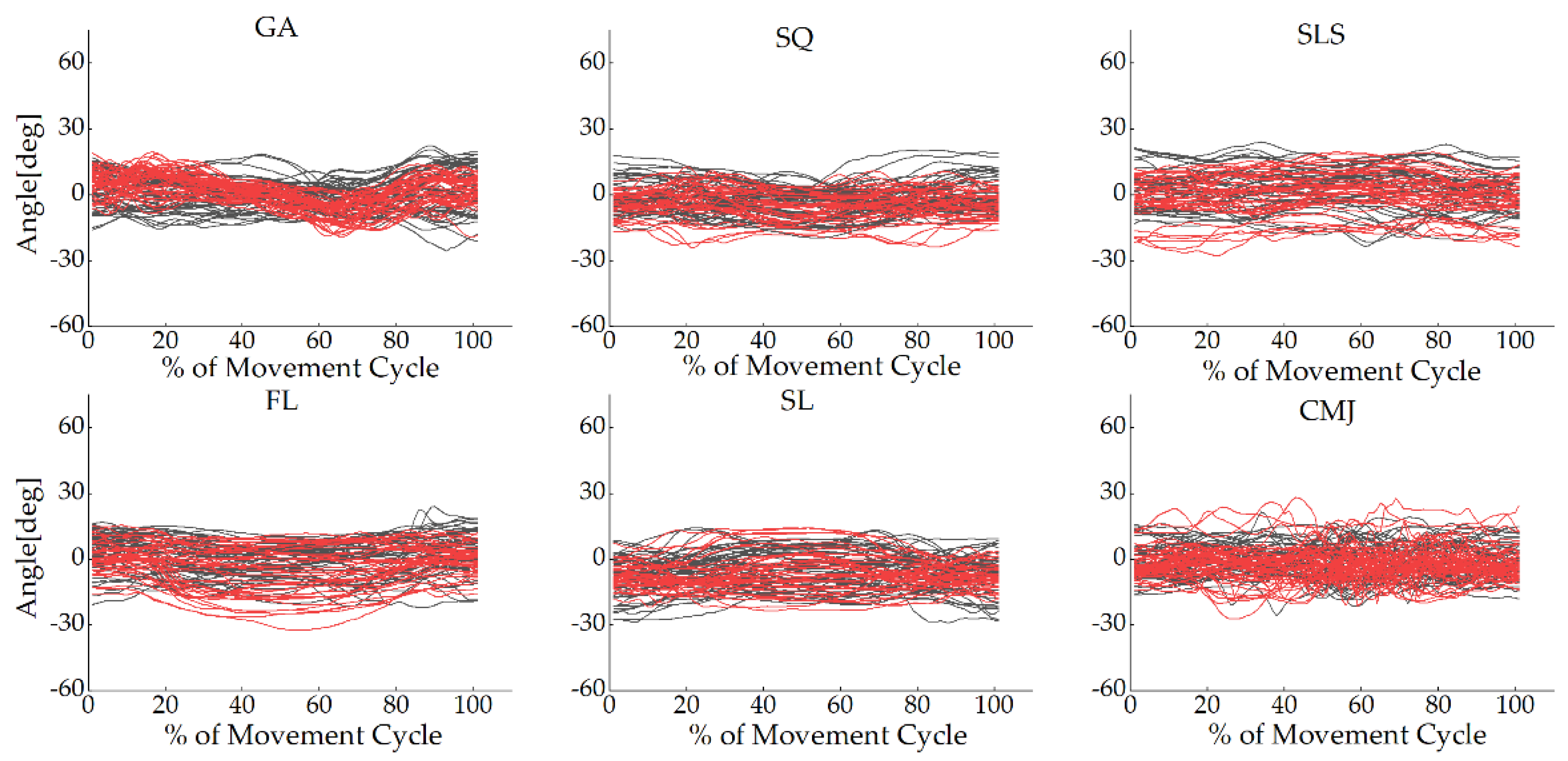
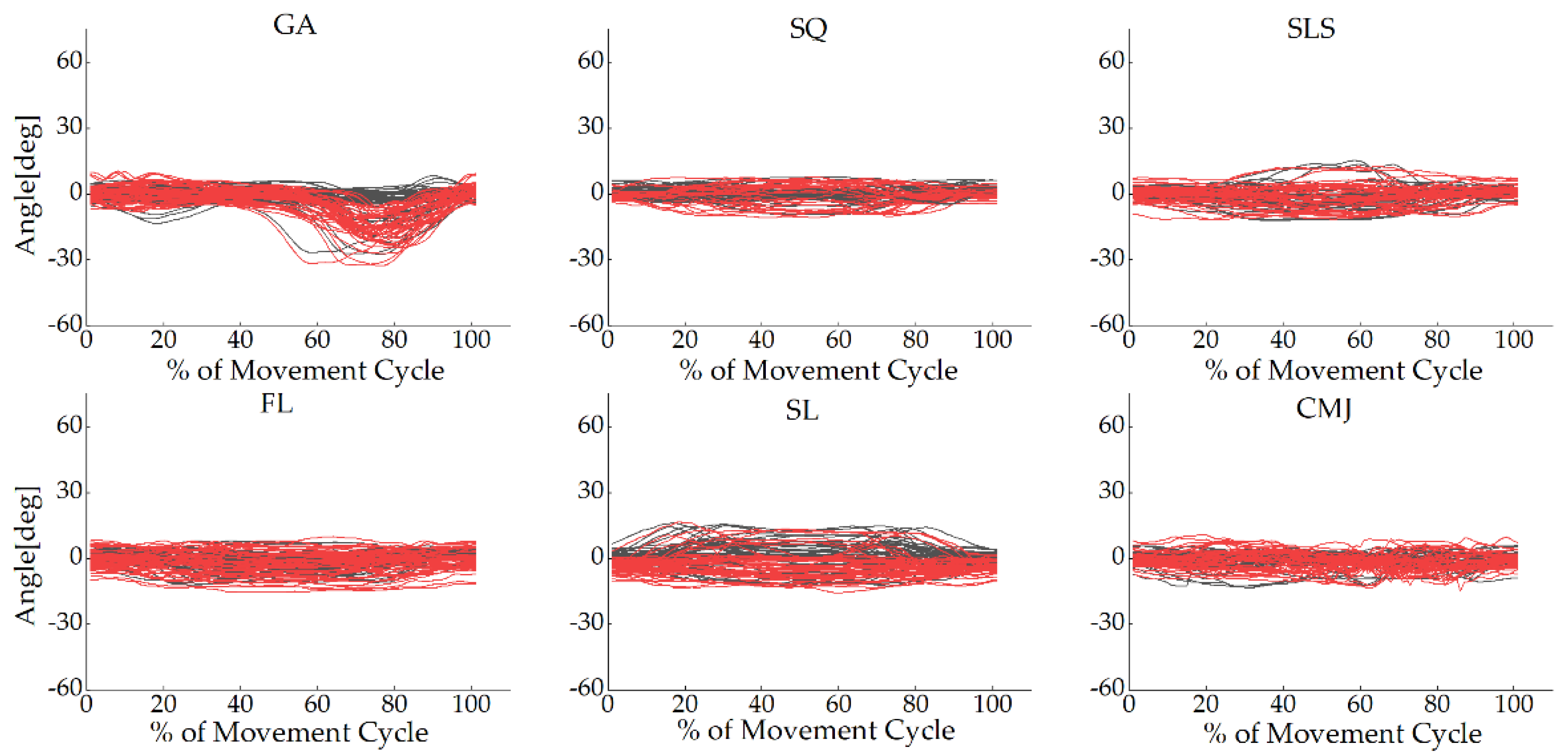
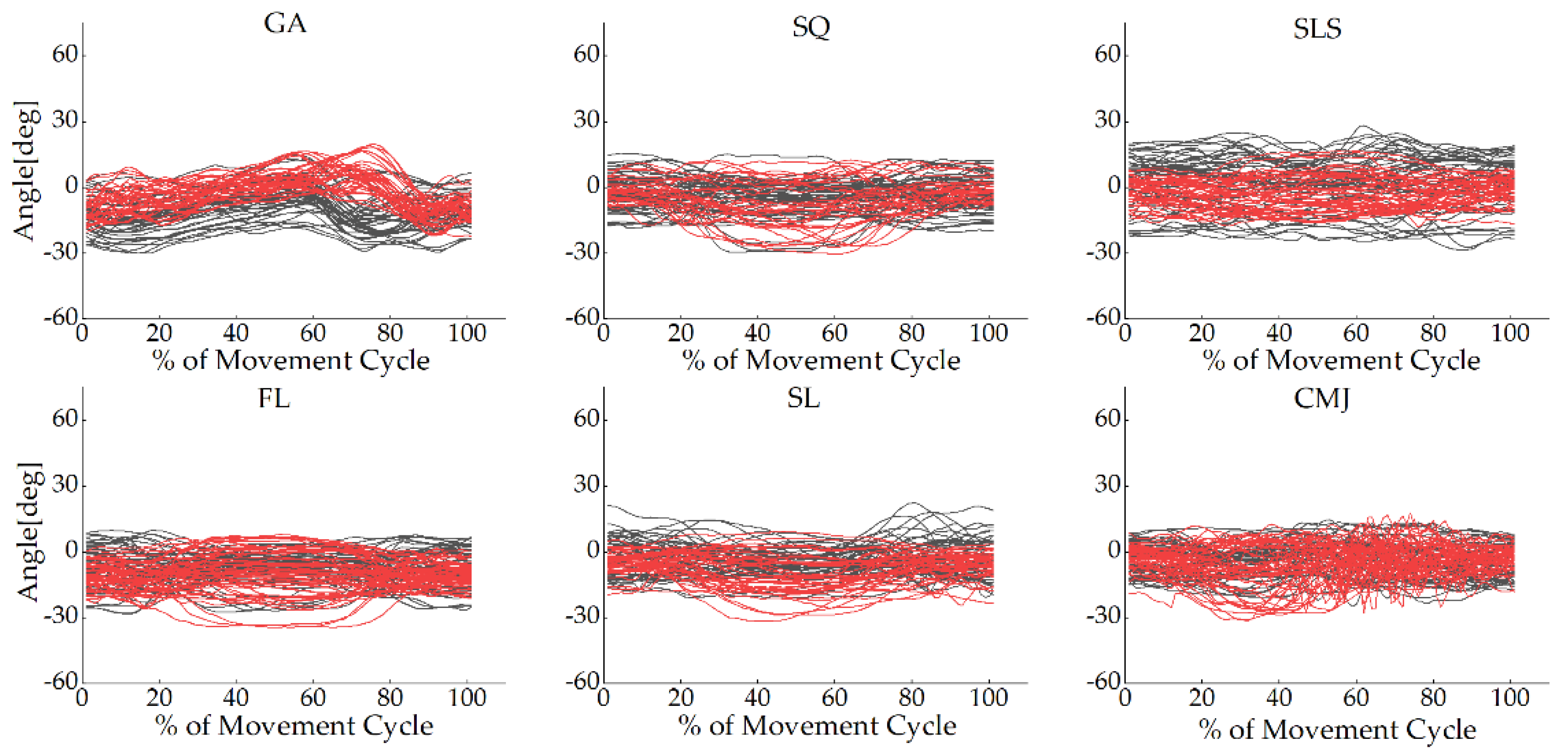
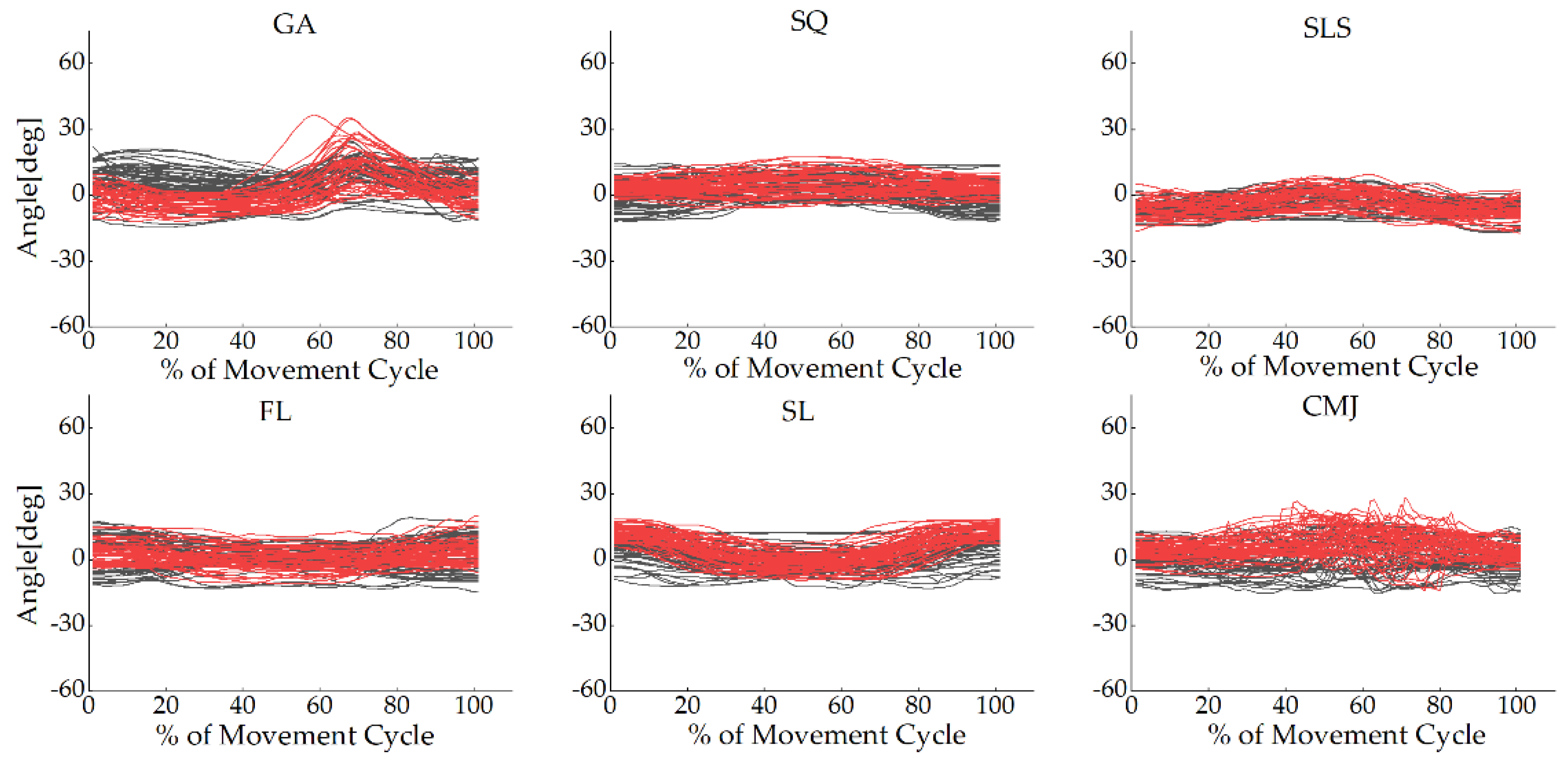
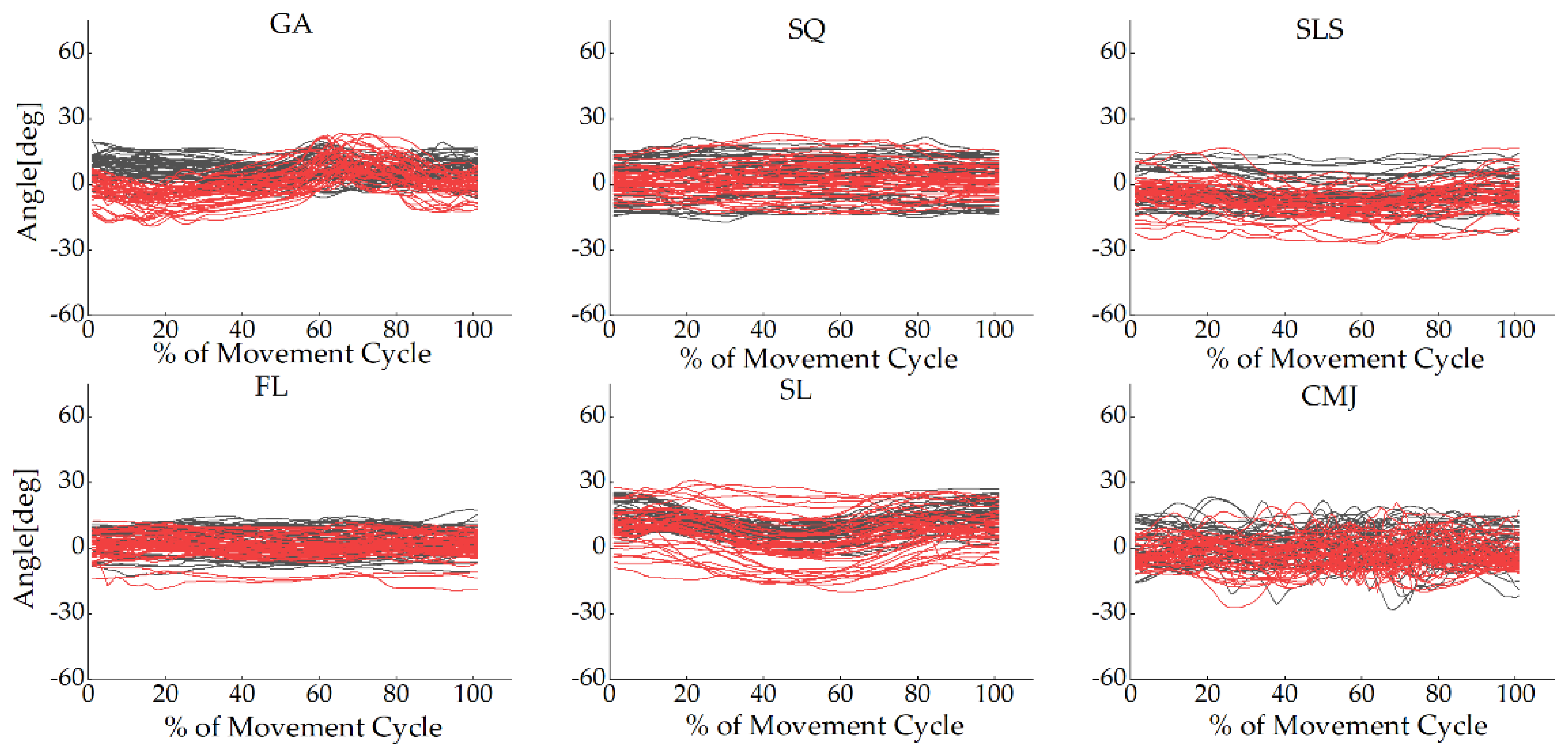
3.1.1. Waveform Analysis
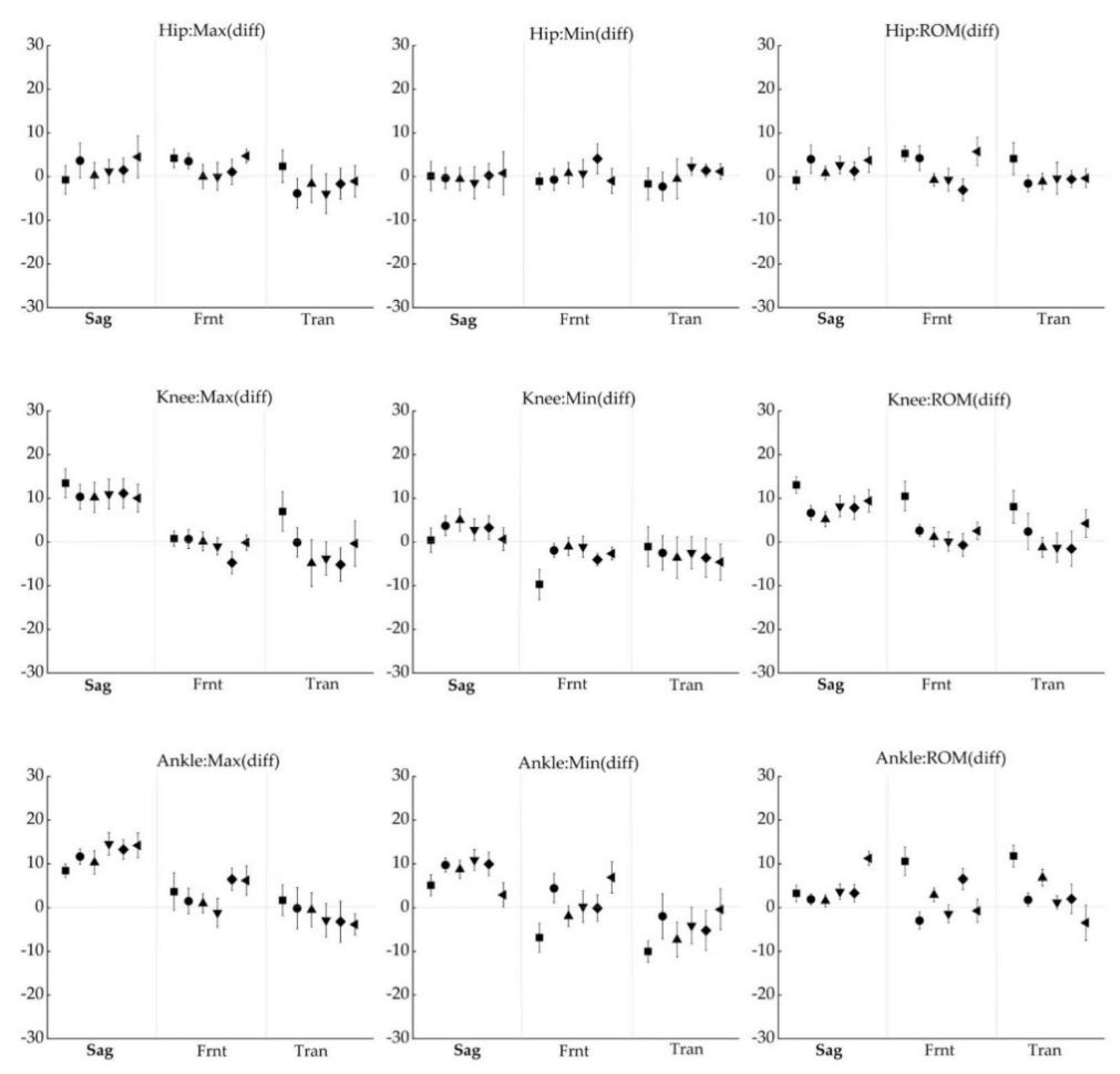
3.1.2. Difference Analysis
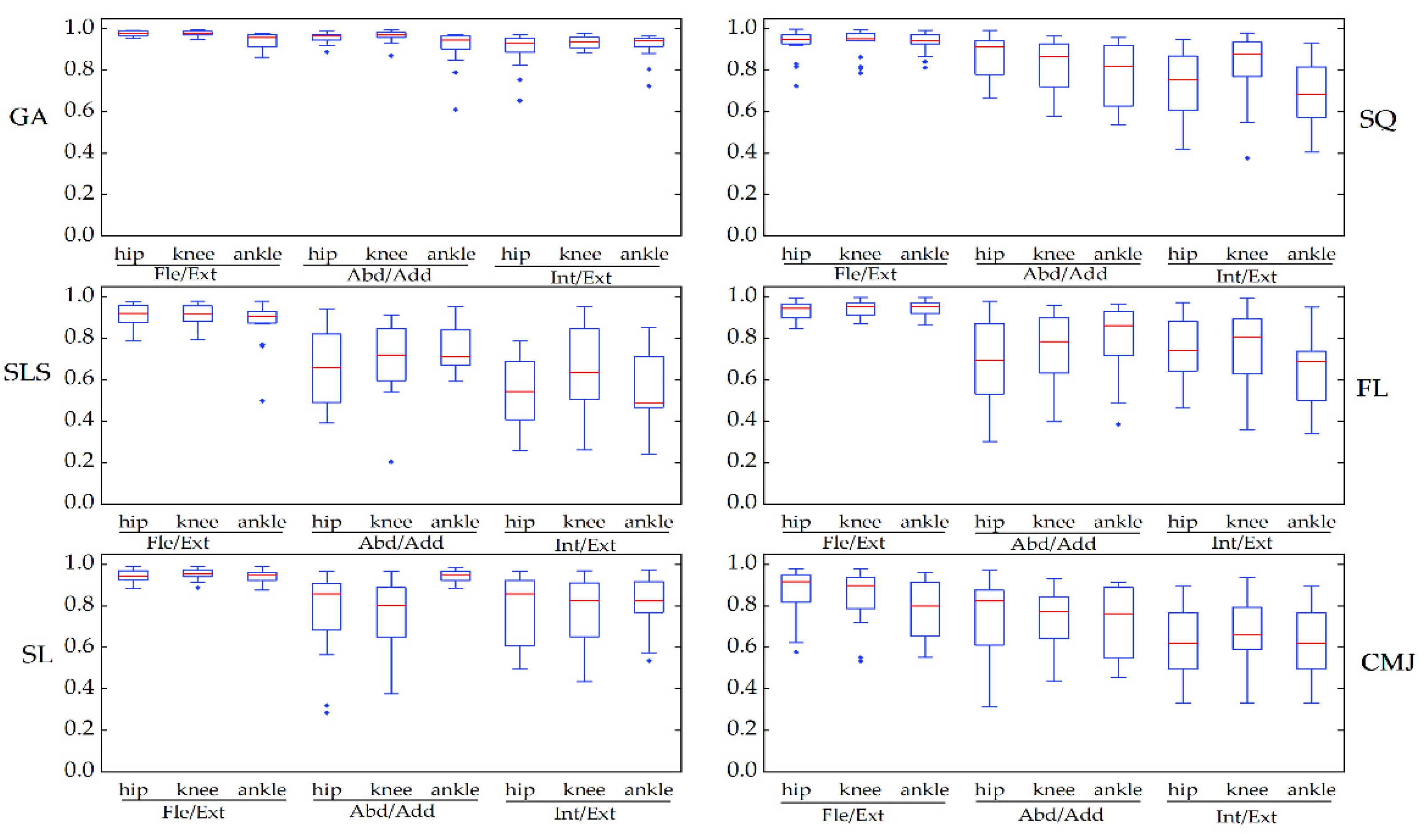
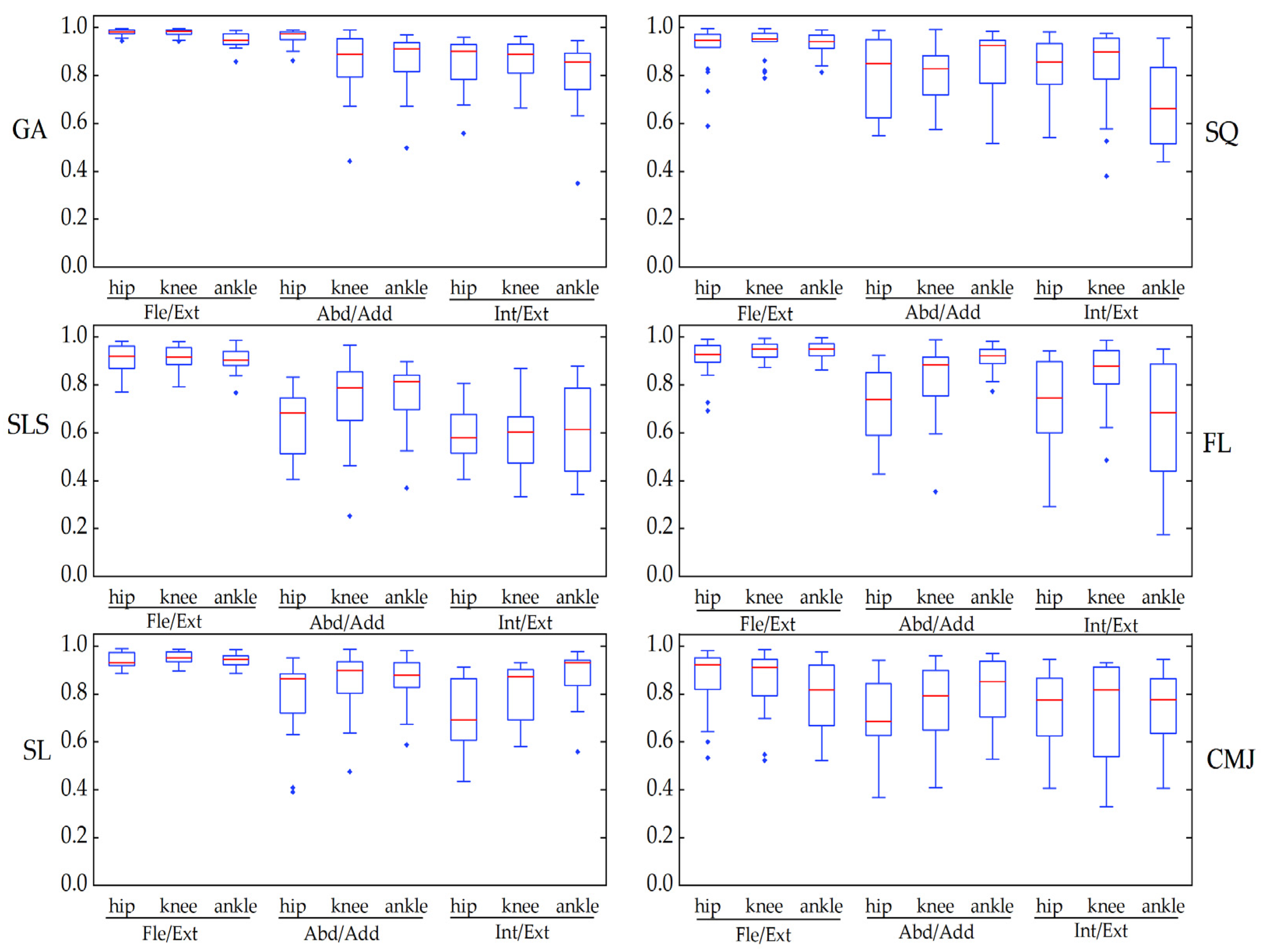
3.2. Reliability
4. Discussion
4.1. Concurrent Validity
4.2. Reliability
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A






Appendix B


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GA | SQ | SLS | FL | SL | CMJ | |||
|---|---|---|---|---|---|---|---|---|
| Max | Hip | Fle/Ext | 0.82 | 1.00 | 0.97 | 0.90 | 0.99 | 0.85 |
| Abd/Add | 0.96 | 0.99 | 0.92 | 0.96 | 0.82 | 0.99 | ||
| Int/Ext | 0.92 | 0.97 | 0.98 | 0.98 | 0.98 | 0.94 | ||
| Knee | Fle/Ext | 0.95 | 0.99 | 0.98 | 0.99 | 0.97 | 0.96 | |
| Abd/Add | 0.98 | 0.99 | 0.98 | 1.00 | 1.00 | 0.96 | ||
| Int/Ext | 0.98 | 0.99 | 0.98 | 0.99 | 0.98 | 0.99 | ||
| Ankle | Fle/Ext | 0.95 | 0.96 | 0.97 | 0.99 | 0.94 | 0.98 | |
| Abd/Add | 0.93 | 0.99 | 0.94 | 0.99 | 0.99 | 0.97 | ||
| Int/Ext | 0.93 | 1.00 | 0.98 | 0.98 | 0.98 | 0.93 | ||
| Min | Hip | Fle/Ext | 0.99 | 0.91 | 0.93 | 0.95 | 0.93 | 0.64 |
| Abd/Add | 0.98 | 0.99 | 0.91 | 0.97 | 0.98 | 0.97 | ||
| Int/Ext | 0.89 | 0.99 | 0.99 | 0.98 | 0.97 | 0.97 | ||
| Knee | Fle/Ext | 0.95 | 0.94 | 0.95 | 0.98 | 0.95 | 0.92 | |
| Abd/Add | 0.99 | 1.00 | 0.99 | 1.00 | 1.00 | 1.00 | ||
| Int/Ext | 0.98 | 0.99 | 0.98 | 0.99 | 0.97 | 0.98 | ||
| Ankle | Fle/Ext | 0.88 | 0.97 | 0.98 | 0.99 | 0.98 | 0.93 | |
| Abd/Add | 0.98 | 1.00 | 0.99 | 1.00 | 0.98 | 0.99 | ||
| Int/Ext | 0.96 | 1.00 | 0.99 | 0.99 | 0.98 | 0.92 | ||
| ROM | Hip | Fle/Ext | 0.78 | 0.98 | 0.94 | 0.93 | 0.98 | 0.94 |
| Abd/Add | 0.92 | 0.98 | 0.77 | 0.84 | 0.84 | 0.88 | ||
| Int/Ext | 0.65 | 0.94 | 0.78 | 0.96 | 0.80 | 0.91 | ||
| Knee | Fle/Ext | 0.92 | 0.98 | 0.95 | 0.99 | 0.96 | 0.95 | |
| Abd/Add | 0.99 | 1.00 | 0.95 | 1.00 | 0.99 | 0.99 | ||
| Int/Ext | 0.87 | 0.99 | 0.70 | 0.99 | 0.96 | 0.97 | ||
| Ankle | Fle/Ext | 0.76 | 0.95 | 0.95 | 0.98 | 0.91 | 0.97 | |
| Abd/Add | 0.94 | 0.99 | 0.89 | 0.97 | 0.95 | 0.95 | ||
| Int/Ext | 0.67 | 9.93 | 0.64 | 0.90 | 0.98 | 0.86 |
References
- Cook, G.; Burton, L.; Hoogenboom, B.J.; Voight, M. Functional Movement Screening: The Use of Fundamental Movements as an Assessment of Function—Part 1. Int. J. Sports Phys. Ther. 2014, 9, 396–409. [Google Scholar]
- Kianifar, R.; Lee, A.; Raina, S.; Kulic, D. Automated Assessment of Dynamic Knee Valgus and Risk of Knee Injury during the Single Leg Squat. IEEE J. Transl. Eng. Health Med. 2017, 5, 2736559. [Google Scholar] [CrossRef]
- Wong, W.Y.; Wong, M.S.; Lo, K.H. Clinical Applications of Sensors for Human Posture and Movement Analysis: A Review. Prosthet. Orthot. Int. 2007, 31, 62–75. [Google Scholar] [CrossRef]
- Komnik, I.; Weiss, S.; Fantini Pagani, C.H.; Potthast, W. Motion Analysis of Patients after Knee Arthroplasty during Activities of Daily Living—A Systematic Review. Gait Posture 2015, 41, 370–377. [Google Scholar] [CrossRef]
- Fong, D.T.; Chan, Y.Y. The Use of Wearable Inertial Motion Sensors in Human Lower Limb Biomechanics Studies: A Systematic Review. Sensors 2010, 10, 11556–11565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picerno, P. 25 Years of Lower Limb Joint Kinematics by Using Inertial and Magnetic Sensors: A Review of Methodological Approaches. Gait Posture 2017, 51, 239–246. [Google Scholar] [CrossRef]
- Ferrari, A.; Cutti, A.G.; Garofalo, P.; Raggi, M.; Heijboer, M.; Cappello, A.; Davalli, A. First in Vivo Assessment of “Outwalk”: A Novel Protocol for Clinical Gait Analysis Based on Inertial and Magnetic Sensors. Med. Biol. Eng. Comput. 2010, 48, 1–15. [Google Scholar] [CrossRef]
- Picerno, P.; Cereatti, A.; Cappozzo, A. Joint Kinematics Estimate Using Wearable Inertial and Magnetic Sensing Modules. Gait Posture 2008, 28, 588–595. [Google Scholar] [CrossRef]
- Favre, J.; Aissaoui, R.; Jolles, B.M.; de Guise, J.A.; Aminian, K. Functional Calibration Procedure for 3d Knee Joint Angle Description Using Inertial Sensors. J. Biomech. 2009, 42, 2330–2335. [Google Scholar] [CrossRef]
- Panero, E.; Digo, E.; Agostini, V.; Gastaldi, L. Comparison of Different Motion Capture Setups for Gait Analysis: Validation of Spatio-Temporal Parameters Estimation. In Proceedings of the 2018 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rome, Italy, 11–13 June 2018. [Google Scholar]
- Zhang, J.T.; Novak, A.C.; Brouwer, B.; Li, Q. Concurrent Validation of Xsens Mvn Measurement of Lower Limb Joint Angular Kinematics. Physiol. Meas. 2013, 34, N63–N69. [Google Scholar] [CrossRef]
- Washabaugh, E.P.; Kalyanaraman, T.; Adamczyk, P.G.; Claflin, E.S.; Krishnan, C. Validity and Repeatability of Inertial Measurement Units for Measuring Gait Parameters. Gait Posture 2017, 55, 87–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobsar, D.; Charlton, J.M.; Tse, C.T.F.; Esculier, J.F.; Graffos, A.; Krowchuk, N.M.; Thatcher, D.; Hunt, M.A. Validity and Reliability of Wearable Inertial Sensors in Healthy Adult Walking: A Systematic Review and Meta-Analysis. J. Neuroeng. Rehabil. 2020, 17, 62. [Google Scholar] [CrossRef] [PubMed]
- Bolink, S.A.; Naisas, H.; Senden, R.; Essers, H.; Heyligers, I.C.; Meijer, K.; Grimm, B. Validity of an Inertial Measurement Unit to Assess Pelvic Orientation Angles during Gait, Sit-Stand Transfers and Step-up Transfers: Comparison with an Optoelectronic Motion Capture System. Med. Eng. Phys. 2016, 38, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Tak, I.; Wiertz, W.P.; Barendrecht, M.; Langhout, R. Validity of a New 3-D Motion Analysis Tool for the Assessment of Knee, Hip and Spine Joint Angles During the Single Leg Squat. Sensors 2020, 20, 4539. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.E.; Gross, M.M. Concurrent Validation of Magnetic and Inertial Measurement Units in Estimating Upper Body Posture During Gait. Measurement 2016, 82, 240–245. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Validation of Inertial Measurement Units with an Optoelectronic System for Whole-Body Motion Analysis. Med. Biol. Eng. Comput. 2017, 55, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial Measurement Units for Clinical Movement Analysis: Reliability and Concurrent Validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwer, N.P.; Yeung, T.; Bobbert, M.F.; Besier, T.F. 3d Trunk Orientation Measured Using Inertial Measurement Units During Anatomical and Dynamic Sports Motions. Scand. J. Med. Sci. Sports 2021, 31, 358–370. [Google Scholar] [CrossRef]
- NOITOM. Axis Neuron Userguide. Available online: https://shopcdn.noitom.com.cn/article/36.html (accessed on 10 August 2021).
- China Global Television Network. Available online: https://news.cgtn.com/news/3067544d31494464776c6d636a4e6e62684a4856/share_p.html (accessed on 21 August 2021).
- Cision Prweb. Available online: https://www.prweb.com/releases/short_film_twenty_one_points_features_vfx_magic_created_with_perception_neuron_motion_capture_that_makes_high_quality_3d_animation_possible_for_directors_at_any_budget/prweb15858480.htm (accessed on 20 August 2021).
- Kim, H.S.; Hong, N.; Kim, M.; Yoon, S.G.; Yu, H.W.; Kong, H.J.; Kim, S.J.; Chai, Y.J.; Choi, H.J.; Choi, J.Y.; et al. Application of a Perception Neuron(®) System in Simulation-Based Surgical Training. J. Clin. Med. 2019, 8, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sers, R.; Forrester, S.; Moss, E.; Ward, S.; Ma, J.; Zecca, M. Validity of the Perception Neuron Inertial Motion Capture System for Upper Body Motion Analysis. Measurement 2020, 149, 107024. [Google Scholar] [CrossRef]
- Van der Straaten, R.; Wesseling, M.; Jonkers, I.; Vanwanseele, B.; Bruijnes, A.; Malcorps, J.; Bellemans, J.; Truijen, J.; De Baets, L.; Timmermans, A. Functional Movement Assessment by Means of Inertial Sensor Technology to Discriminate between Movement Behaviour of Healthy Controls and Persons with Knee Osteoarthritis. J. Neuroeng. Rehabil. 2020, 17, 65. [Google Scholar] [CrossRef]
- Point, Natural. Optitrack System-Optitrack Documentation Wiki (Motive Version 2.1). Available online: https://v21.wiki.optitrack.com/index.php?title=OptiTrack_Documentation_Wiki (accessed on 7 August 2021).
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of Lower Extremity Kinematics during Level Walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef]
- Dingenen, B.; Malfait, B.; Vanrenterghem, J.; Verschueren, S.M.; Staes, F. The Reliability and Validity of the Measurement of Lateral Trunk Motion in Two-Dimensional Video Analysis during Unipodal Functional Screening Tests in Elite Female Athletes. Phys. Ther. Sport 2013, 15, 117–123. [Google Scholar] [CrossRef]
- Carse, B.; Meadows, B.; Bowers, R.; Rowe, P. Affordable Clinical Gait Analysis: An Assessment of the Marker Tracking Accuracy of a New Low-Cost Optical 3d Motion Analysis System. Physiotherapy 2013, 99, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Cutti, A.G.; Cappello, A. A New Formulation of the Coefficient of Multiple Correlation to Assess the Similarity of Waveforms Measured Synchronously by Different Motion Analysis Protocols. Gait Posture 2010, 31, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Takeda, R.; Tadano, S.; Natorigawa, A.; Todoh, M.; Yoshinari, S. Gait Posture Estimation Using Wearable Acceleration and Gyro Sensor. J. Biomech. 2009, 42, 2486–2494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Noort, J.C.; Ferrari, A.; Cutti, A.G.; Becher, J.G.; Harlaar, J. Gait Analysis in Children with Cerebral Palsy Via Inertial and Magnetic Sensors. Med. Biol. Eng. Comput. 2013, 51, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Cloete, T.; Scheffer, C. Benchmarking of a Full-Body Inertial Motion Capture System for Clinical Gait Analysis. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008. [Google Scholar]
- Cooper, G.; Sheret, I.; McMillan, L.; Siliverdis, K.; Sha, N.; Hodgins, D.; Kenney, L.; Howard, D. Inertial Sensor-Based Knee Flexion/Extension Angle Estimation. J. Biomech. 2009, 42, 2678–2685. [Google Scholar] [CrossRef] [Green Version]
- Favre, J.; Jolles, B.M.; Aissaoui, R.; Aminian, K. Ambulatory Measurement of 3d Knee Joint Angle. J. Biomech. 2008, 41, 1029–1035. [Google Scholar] [CrossRef]
- Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity of Inertial Sensor Based 3d Joint Kinematics of Static and Dynamic Sport and Physiotherapy Specific Movements. PLoS ONE 2019, 14, e0213064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, A.; Deluzio, K.; Li, Q. Assessment of Anatomical Frame Variation Effect on Joint Angles: A Linear Perturbation Approach. J. Biomech. 2011, 44, 2838–2842. [Google Scholar] [CrossRef] [PubMed]
- Della Croce, U.; Cappozzo, A.; Kerrigan, D.C. Pelvis and Lower Limb Anatomical Landmark Calibration Precision and Its Propagation to Bone Geometry and Joint Angles. Med. Biol. Eng. Comput. 1999, 37, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Seel, T.; Raisch, J.; Schauer, T. Imu-Based Joint Angle Measurement for Gait Analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef] [Green Version]
- Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity, Test-Retest Reliability and Long-Term Stability of Magnetometer Free Inertial Sensor Based 3d Joint Kinematics. Sensors 2018, 18, 1980. [Google Scholar] [CrossRef] [Green Version]
- Leardini, A.; Chiari, L.; Della Croce, U.; Cappozzo, A. Human Movement Analysis Using Stereophotogrammetry. Part 3. Soft Tissue Artifact Assessment and Compensation. Gait Posture 2005, 21, 212–225. [Google Scholar] [CrossRef]
- Fiorentino, N.M.; Atkins, P.R.; Kutschke, M.J.; Goebel, J.M.; Foreman, K.B.; Anderson, A.E. Soft Tissue Artifact Causes Significant Errors in the Calculation of Joint Angles and Range of Motion at the Hip. Gait Posture 2017, 55, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Karatsidis, A.; Jung, M.; Schepers, H.M.; Bellusci, G.; de Zee, M.; Veltink, P.H.; Andersen, M.S. Musculoskeletal Model-Based Inverse Dynamic Analysis under Ambulatory Conditions Using Inertial Motion Capture. Med. Eng. Phys. 2019, 65, 68–77. [Google Scholar] [CrossRef] [Green Version]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The Reliability of Three-Dimensional Kinematic Gait Measurements: A Systematic Review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.S. Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef] [Green Version]








| Hip | Knee | Ankle | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Fle/Ext | Abd/Add | Int/Ext | Fle/Ext | Abd/Add | Int/Ext | Fle/Ext | Abd/Add | Int/Ext | ||
| RSME (before) | GA | 6.48 ± 3.51 | 6.26 ± 2.48 | 8.91 ± 2.44 | 9.29 ± 4.59 | 5.97 ± 3.05 | 10.80 ± 4.57 | 8.79 ± 3.25 | 9.08 ± 3.60 | 10.18 ± 3.11 |
| SQ | 6.32 ± 2.39 | 4.66 ± 1.88 | 7.08 ± 4.46 | 11.04 ± 7.10 | 4.09 ± 2.38 | 7.29 ± 3.42 | 10.93 ± 3.12 | 6.27 ± 3.99 | 8.77 ± 6.10 | |
| SLS | 5.20 ± 3.02 | 5.62 ± 3.43 | 8.42 ± 4.55 | 9.12 ± 6.32 | 4.09 ± 1.76 | 10.97 ± 3.74 | 9.78 ± 4.88 | 4.40 ± 2.09 | 8.40 ± 5.52 | |
| FL | 5.85 ± 3.02 | 5.59 ± 3.34 | 9.31 ± 5.64 | 9.49 ± 5.50 | 4.22 ± 2.33 | 7.49 ± 4.72 | 13.14 ± 4.51 | 5.99 ± 3.77 | 5.98 ± 3.02 | |
| SL | 5.36 ± 2.77 | 6.10 ± 3.94 | 8.21 ± 3.23 | 10.36 ± 6.05 | 5.66 ± 2.72 | 9.00 ± 4.94 | 11.64 ± 3.56 | 6.90 ± 2.96 | 9.48 ± 5.33 | |
| CMJ | 7.44 ± 5.82 | 5.55 ± 1.85 | 8.31 ± 4.19 | 9.16 ± 4.59 | 3.57 ± 1.56 | 9.75 ± 5.60 | 12.12 ± 4.44 | 8.28 ± 4.30 | 8.25 ± 2.98 | |
| RSME (after) | GA | 5.49 ± 4.07 | 3.29 ± 2.40 | 5.15 ± 3.34 | 7.83 ± 5.05 | 3.56 ± 3.20 | 7.54 ± 5.82 | 8.31 ± 3.52 | 6.87 ± 4.48 | 7.09 ± 3.98 |
| SQ | 4.96 ± 2.43 | 2.95 ± 2.25 | 5.42 ± 4.89 | 8.02 ± 5.13 | 3.03 ± 2.47 | 4.97 ± 4.37 | 10.78 ± 3.23 | 5.40 ± 4.47 | 8.16 ± 6.50 | |
| SLS | 4.69 ± 3.31 | 4.54 ± 3.44 | 7.20 ± 5.03 | 8.42 ± 6.34 | 3.06 ± 1.83 | 9.95 ± 4.26 | 9.68 ± 4.86 | 3.40 ± 2.45 | 6.59 ± 6.40 | |
| FL | 5.17 ± 3.34 | 4.69 ± 3.35 | 7.46 ± 6.22 | 8.19 ± 5.79 | 3.34 ± 2.55 | 6.12 ± 5.12 | 12.83 ± 4.67 | 5.28 ± 4.09 | 5.24 ± 3.38 | |
| SL | 4.52 ± 3.24 | 5.10 ± 4.22 | 6.21 ± 4.16 | 9.29 ± 6.20 | 4.74 ± 2.97 | 7.40 ± 5.20 | 11.38 ± 3.68 | 5.46 ± 3.41 | 8.33 ± 5.74 | |
| CMJ | 5.59 ± 5.32 | 3.58 ± 2.35 | 6.03 ± 4.68 | 7.77 ± 4.90 | 2.08 ± 1.92 | 7.13 ± 6.59 | 11.07 ± 4.86 | 6.34 ± 4.70 | 5.53 ± 3.65 | |
| Hip | Knee | Ankle | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Fle/Ext | Abd/Add | Int/Ext | Fle/Ext | Abd/Add | Int/Ext | Fle/Ext | Abd/Add | Int/Ext | ||
| RSME (IMU) | GA | 4.21 ± 1.19 | 2.32 ± 0.78 | 2.88 ± 0.89 | 6.33 ± 2.19 | 1.82 ± 0.69 | 3.29 ± 0.85 | 4.14 ± 1.24 | 2.91 ± 1.04 | 3.00 ± 0.61 |
| SQ | 11.78 ± 3.72 | 2.28 ± 1.01 | 2.39 ± 0.69 | 13.87 ± 4.92 | 1.59 ± 0.45 | 2.74 ± 0.97 | 4.60 ± 1.62 | 1.48 ± 0.67 | 1.98 ± 0.49 | |
| SLS | 8.92 ± 2.64 | 2.35 ± 0.83 | 3.36 ± 1.03 | 13.81 ± 4.18 | 1.86 ± 0.64 | 2.91 ± 0.75 | 6.56 ± 2.69 | 3.08 ± 0.95 | 4.61 ± 1.33 | |
| FL | 5.55 ± 1.77 | 1.93 ± 0.62 | 3.09 ± 1.53 | 11.38 ± 4.24 | 1.59 ± 0.64 | 2.51 ± 0.73 | 7.17 ± 2.86 | 1.77 ± 0.64 | 2.37 ± 0.77 | |
| SL | 6.86 ± 3.15 | 2.34 ± 0.83 | 2.82 ± 1.02 | 10.38 ± 3.45 | 1.63 ± 0.88 | 2.61 ± 0.80 | 5.12 ± 1.65 | 2.24 ± 0.86 | 2.96 ± 0.85 | |
| CMJ | 15.18 ± 5.63 | 3.43 ± 1.63 | 4.00 ± 1.29 | 21.34 ± 7.60 | 2.26 ± 0.68 | 4.28 ± 1.15 | 16.11 ± 5.82 | 3.45 ± 1.01 | 3.96 ± 1.30 | |
| RSME (OptiTrack) | GA | 4.08 ± 1.48 | 1.55 ± 0.63 | 3.08 ± 0.75 | 5.04 ± 1.99 | 1.25 ± 0.59 | 2.95 ± 1.08 | 3.70 ± 1.12 | 1.87 ± 0.62 | 2.23 ± 0.56 |
| SQ | 12.12 ± 5.45 | 1.97 ± 0.74 | 2.38 ± 0.92 | 13.87 ± 6.24 | 1.13 ± 0.57 | 2.46 ± 0.85 | 4.43 ± 1.54 | 1.66 ± 0.48 | 1.49 ± 0.52 | |
| SLS | 8.59 ± 2.45 | 3.19 ± 1.62 | 4.21 ± 1.37 | 12.50 ± 3.86 | 1.62 ± 0.82 | 4.46 ± 1.44 | 5.37 ± 1.86 | 2.64 ± 1.57 | 1.96 ± 0.73 | |
| FL | 5.79 ± 2.44 | 2.64 ± 1.08 | 3.06 ± 1.58 | 10.29 ± 3.37 | 1.26 ± 0.69 | 2.68 ± 1.14 | 6.71 ± 2.46 | 1.69 ± 0.73 | 1.71 ± 0.55 | |
| SL | 6.96 ± 4.04 | 3.17 ± 1.64 | 3.33 ± 0.83 | 9.50 ± 3.38 | 1.59 ± 0.83 | 3.22 ± 1.15 | 4.84 ± 1.46 | 1.70 ± 0.84 | 2.11 ± 0.89 | |
| CMJ | 15.67 ± 7.19 | 2.82 ± 0.99 | 4.21 ± 1.66 | 19.19 ± 7.06 | 1.53 ± 0.88 | 3.70 ± 1.12 | 13.30 ± 5.44 | 3.67 ± 1.75 | 4.55 ± 1.74 | |
| GA | SQ | SLS | FL | SL | CMJ | |||
|---|---|---|---|---|---|---|---|---|
| Max | Hip | Fle/Ext | 0.97 | 0.99 | 0.97 | 0.99 | 0.99 | 0.97 |
| Abd/Add | 0.93 | 0.98 | 0.97 | 0.97 | 0.98 | 0.97 | ||
| Int/Ext | 0.93 | 0.98 | 0.98 | 0.97 | 0.99 | 0.97 | ||
| Knee | Fle/Ext | 0.97 | 1.00 | 0.97 | 0.99 | 0.99 | 0.97 | |
| Abd/Add | 0.98 | 0.99 | 0.99 | 0.99 | 1.00 | 0.99 | ||
| Int/Ext | 0.98 | 0.99 | 0.98 | 0.98 | 0.98 | 0.96 | ||
| Ankle | Fle/Ext | 0.96 | 0.99 | 0.93 | 0.99 | 0.97 | 0.97 | |
| Abd/Add | 0.96 | 0.99 | 0.94 | 0.98 | 0.98 | 0.94 | ||
| Int/Ext | 0.94 | 0.99 | 0.93 | 0.98 | 0.99 | 0.96 | ||
| Min | Hip | Fle/Ext | 0.98 | 0.94 | 0.93 | 0.97 | 0.89 | 0.87 |
| Abd/Add | 0.89 | 1.00 | 0.97 | 0.99 | 0.97 | 0.99 | ||
| Int/Ext | 0.96 | 0.99 | 0.98 | 0.98 | 0.98 | 0.95 | ||
| Knee | Fle/Ext | 0.95 | 0.93 | 0.89 | 0.84 | 0.92 | 0.87 | |
| Abd/Add | 0.97 | 0.99 | 0.98 | 0.98 | 0.98 | 0.97 | ||
| Int/Ext | 0.94 | 1.00 | 0.99 | 0.99 | 0.99 | 0.99 | ||
| Ankle | Fle/Ext | 0.92 | 0.98 | 0.71 | 0.99 | 0.95 | 0.97 | |
| Abd/Add | 0.97 | 0.98 | 0.91 | 0.98 | 0.98 | 0.97 | ||
| Int/Ext | 0.91 | 0.99 | 0.88 | 0.99 | 0.98 | 0.93 | ||
| ROM | Hip | Fle/Ext | 0.97 | 0.99 | 0.93 | 0.98 | 0.99 | 0.94 |
| Abd/Add | 0.94 | 0.99 | 0.94 | 0.95 | 0.94 | 0.97 | ||
| Int/Ext | 0.93 | 0.94 | 0.63 | 0.94 | 0.92 | 0.89 | ||
| Knee | Fle/Ext | 0.92 | 0.99 | 0.93 | 0.98 | 0.97 | 0.97 | |
| Abd/Add | 0.97 | 0.94 | 0.97 | 0.91 | 0.99 | 0.73 | ||
| Int/Ext | 0.92 | 0.99 | 0.89 | 0.97 | 0.97 | 0.96 | ||
| Ankle | Fle/Ext | 0.91 | 0.99 | 0.97 | 0.99 | 0.94 | 0.98 | |
| Abd/Add | 0.94 | 0.96 | 0.86 | 0.96 | 0.98 | 0.94 | ||
| Int/Ext | 0.90 | 0.82 | 0.57 | 0.78 | 0.98 | 0.90 | ||
| Technologies | Pros | Cons |
|---|---|---|
| IMU | Simple to use | No precise absolute positioning |
| Very lightweight | Extremely magnetically sensitive | |
| Extremely large recording volume | Calibration errors | |
| Easy and quick calibration | Positional and rotational errors | |
| Works just fine over WiFi | ||
| Almost no disconnecting or data loss during hours of operation | ||
| Cheaper | ||
| OptiTrack | High precision | Recording volume limited |
| Capture rates are high | Markers can be occluded | |
| Easily recreates complex movement | Extensive post-processing may be necessary to handle marker swap, missing data, and noisy data | |
| High cost of the hardware |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shuai, Z.; Dong, A.; Liu, H.; Cui, Y. Reliability and Validity of an Inertial Measurement System to Quantify Lower Extremity Joint Angle in Functional Movements. Sensors 2022, 22, 863. https://doi.org/10.3390/s22030863
Shuai Z, Dong A, Liu H, Cui Y. Reliability and Validity of an Inertial Measurement System to Quantify Lower Extremity Joint Angle in Functional Movements. Sensors. 2022; 22(3):863. https://doi.org/10.3390/s22030863
Chicago/Turabian StyleShuai, Zhenyu, Anqi Dong, Haoyang Liu, and Yixiong Cui. 2022. "Reliability and Validity of an Inertial Measurement System to Quantify Lower Extremity Joint Angle in Functional Movements" Sensors 22, no. 3: 863. https://doi.org/10.3390/s22030863