
Correlating Personal Resourcefulness and Psychomotor Skills: An Analysis of Stress, Visual Attention and Technical Metrics

 , , , ,
, , , ,
Abstract
:1. Introduction
1.1. Modulators of Attention
1.2. Modulators of Stress
1.3. Goals of This Study
2. Materials and Methods
2.1. Subjects
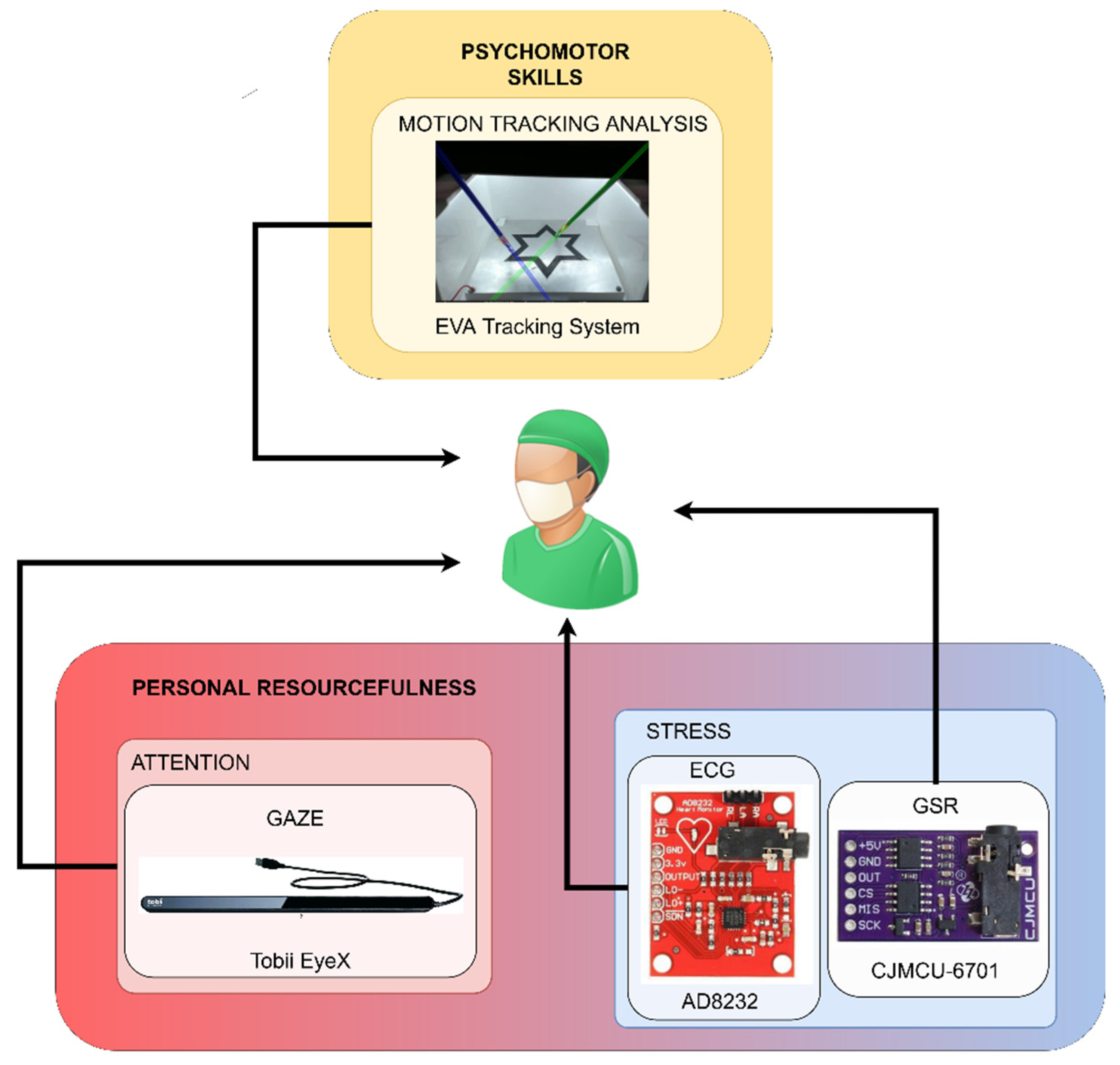
2.2. Experimental Setup
2.3. Monitoring Application Description
2.3.1. Stress Module
2.3.2. Attention Module
2.3.3. Performance Module
2.4. Data Analysis
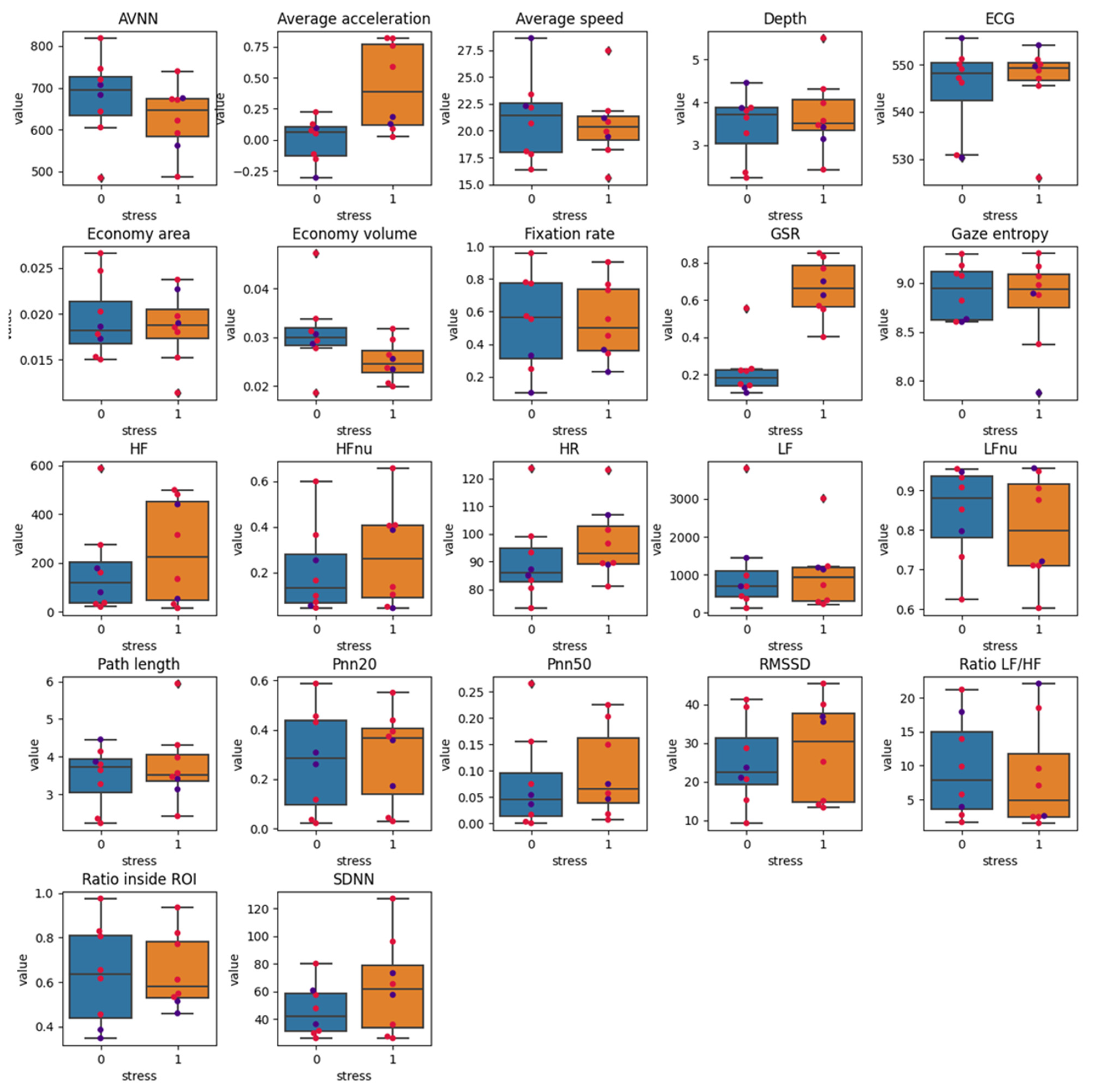
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rutherford, D.N.; D’Angelo, A.L.D.; Law, K.E.; Pugh, C.M. Advanced Engineering Technology for Measuring Performance. Surg. Clin. N. Am. 2015, 95, 813–826. [Google Scholar] [CrossRef] [PubMed]
- Yule, S.; Flin, R.; Paterson-Brown, S.; Maran, N. Non-technical skills for surgeons in the operating room: A review of the literature. Surgery 2006, 139, 140–149. [Google Scholar] [CrossRef]
- Agha, R.A.; Fowler, A.J.; Sevdalis, N. The role of non-technical skills in surgery. Ann. Med. Surg. 2015, 4, 422–427. [Google Scholar] [CrossRef]
- O’Neil, H.F.; Perez, R.S.; Baker, E.L. Teaching and Measuring Cognitive Readiness; Springer: Boston, MA, USA, 2014; ISBN 9781461475798. [Google Scholar]
- Pugh, C.M.; DaRosa, D.A. Use of Cognitive Task Analysis to Guide the Development of Performance-Based Assessments for IntraOperative Decision Making. Mil. Med. 2013, 170, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiegmann, D.A.; ElBardissi, A.W.; Dearani, J.A.; Daly, R.C.; Sundt, T.M. Disruptions in surgical flow and their relationship to surgical errors: An exploratory investigation. Surgery 2007, 142, 658–665. [Google Scholar] [CrossRef]
- Dedy, N.J.; Fecso, A.B.; Szasz, P.; Bonrath, E.M.; Grantcharov, T.P. Implementation of an effective strategy for teaching nontechnical skills in the operating room. A single-blinded nonrandomized trial. Ann. Surg. 2016, 263, 937–941. [Google Scholar] [CrossRef]
- Anton, N.E.; Bean, E.A.; Hammonds, S.C.; Stefanidis, D. Application of mental skills training in surgery: A review of its effectiveness and proposed next steps. J. Laparoendosc. Adv. Surg. Tech. 2017, 27, 459–469. [Google Scholar] [CrossRef]
- Datta, V.; Chang, A.; Mackay, S.; Darzi, A. The relationship between motion analysis and surgical technical assessments. Am. J. Surg. 2002, 184, 70–73. [Google Scholar] [CrossRef]
- Dosis, A.; Aggarwal, R.; Bello, F.; Moorthy, K.; Munz, Y.; Gillies, D.; Darzi, A. Synchronized video and motion analysis for the assessment of procedures in the operating theater. Arch. Surg. 2005, 140, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Chmarra, M.K.; Bakker, N.H.; Grimbergen, C.A.; Dankelman, J. TrEndo, a device for tracking minimally invasive surgical instruments in training setups. Sens. Actuators A Phys. 2006, 126, 328–334. [Google Scholar] [CrossRef]
- Oropesa, I.; Sánchez-González, P.; Chmarra, M.K.; Lamata, P.; Fernández, Á.; Sánchez-Margallo, J.A.; Jansen, F.W.; Dankelman, J.; Sánchez-Margallo, F.M.; Gómez, E.J. EVA: Laparoscopic instrument tracking based on endoscopic video analysis for psychomotor skills assessment. Surg. Endosc. 2013, 27, 1029–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chmarra, M.K.; Klein, S.; De Winter, J.C.F.; Jansen, F.W.; Dankelman, J. Objective classification of residents based on their psychomotor laparoscopic skills. Surg. Endosc. 2010, 24, 1031–1039. [Google Scholar] [CrossRef] [Green Version]
- Fried, G.M.; Feldman, L.S. Objective assessment of technical performance. World J. Surg. 2008, 32, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Li, M.M.; George, J. A systematic review of low-cost laparoscopic simulators. Surg. Endosc. 2017, 31, 38–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, R.H. Why Johnny cannot operate. Surgery 2009, 146, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.; Mishra, A.; Aggarwal, R.; Grantcharov, T.P. Non-technical skills assessment in surgery. Surg. Oncol. 2011, 20, 169–177. [Google Scholar] [CrossRef]
- Norman, G.R.; Grierson, L.E.M.; Sherbino, J.; Hamstra, S.J.; Schmidt, H.G.; Mamede, S. Expertise in Medicine and Surgery. In The Cambridge Handbook of Expertise and Expert Performance; Cambridge University Press: Cambridge, UK, 2018; pp. 331–355. [Google Scholar]
- Brunckhorst, O.; Shahid, S.; Aydin, A.; McIlhenny, C.; Khan, S.; Raza, S.J.; Sahai, A.; Brewin, J.; Bello, F.; Kneebone, R.; et al. Simulation-based ureteroscopy skills training curriculum with integration of technical and non-technical skills: A randomised controlled trial. Surg. Endosc. 2015, 29, 2728–2735. [Google Scholar] [CrossRef] [PubMed]
- Madani, A.; Vassiliou, M.C.; Watanabe, Y.; Al-Halabi, B.; Al-Rowais, M.S.; Deckelbaum, D.L.; Fried, G.M.; Feldman, L.S. What Are the Principles That Guide Behaviors in the Operating Room? Ann. Surg. 2017, 265, 255–267. [Google Scholar] [CrossRef]
- Stefanidis, D.; Anton, N.E.; Howley, L.D.; Bean, E.; Yurco, A.; Pimentel, M.E.; Davis, C.K. Effectiveness of a comprehensive mental skills curriculum in enhancing surgical performance: Results of a randomized controlled trial. Am. J. Surg. 2017, 213, 318–324. [Google Scholar] [CrossRef] [Green Version]
- Law, B.; Lomax, A.J.; Atkins, M.S.; Mackenzie, C.L.; Kirkpatrick, A.E. Eye gaze patterns differentiate novice and experts in a virtual laparoscopic surgery training environment. In Proceedings of the 2004 Symposium on Eye Tracking Research and Applications, San Antonio, TX, USA, 22–24 March 2004; pp. 41–48. [Google Scholar]
- Wilson, M.; McGrath, J.; Vine, S.; Brewer, J.; Defriend, D.; Masters, R. Psychomotor control in a virtual laparoscopic surgery training environment: Gaze control parameters differentiate novices from experts. Surg. Endosc. 2010, 24, 2458–2464. [Google Scholar] [CrossRef] [Green Version]
- Wilson, M.R.; Vine, S.J.; Bright, E.; Masters, R.S.W.; Defriend, D.; McGrath, J.S. Gaze training enhances laparoscopic technical skill acquisition and multi-tasking performance: A randomized, controlled study. Surg. Endosc. 2011, 25, 3737–3739. [Google Scholar] [CrossRef] [Green Version]
- Jacob, R.J.K.; Karn, K.S. Eye Tracking in Human-Computer Interaction and Usability Research. Ready to Deliver the Promises. In The Mind’s Eye: Cognitive and Applied Aspects of Eye Movement Research; Elsevier: Amsterdam, The Netherlands, 2003; pp. 573–605. ISBN 9780080518923. [Google Scholar]
- Zhang, Q.; Wang, Z.; Chi, J.; Zhang, P.; Yang, Y. Design and calibration for gaze tracking system. In Proceedings of the IEEE 2nd International Conference on Information Management and Engineering: ICIME’10, Chengdu, China, 16–18 April 2010; pp. 16–18. [Google Scholar]
- Land, R.; Meyer, J.H.F. The Scalpel and the ‘Mask’: Threshold Concepts and Surgical Education. In Surgical Education; Fry, H., Kneebone, R., Eds.; Springer: Dordrecht, The Netherlands, 2011; pp. 91–106. [Google Scholar]
- Richstone, L.; Schwartz, M.J.; Seideman, C.; Cadeddu, J.; Marshall, S.; Kavoussi, L.R. Eye metrics as an objective assessment of surgical skill. Ann. Surg. 2010, 252, 177–182. [Google Scholar] [CrossRef]
- Koh, R.Y.I.; Park, T.; Wickens, C.D.; Ong, L.T.; Chia, S.N. Differences in Attentional Strategies by Novice and Experienced Operating Theatre Scrub Nurses. J. Exp. Psychol. Appl. 2011, 17, 233–246. [Google Scholar] [CrossRef] [Green Version]
- Tomizawa, Y.; Aoki, H.; Suzuki, S.; Matayoshi, T.; Yozu, R. Eye-tracking analysis of skilled performance in clinical extracorporeal circulation. J. Artif. Organs 2012, 15, 146–157. [Google Scholar] [CrossRef]
- Erridge, S.; Ashraf, H.; Purkayastha, S.; Darzi, A.; Sodergren, M.H. Comparison of gaze behaviour of trainee and experienced surgeons during laparoscopic gastric bypass. Br. J. Surg. 2018, 105, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Roach, V.A.; Fraser, G.M.; Kryklywy, J.H.; Mitchell, D.G.V.; Wilson, T.D. Time limits in testing: An analysis of eye movements and visual attention in spatial problem solving. Anat. Sci. Educ. 2017, 10, 528–537. [Google Scholar] [CrossRef] [PubMed]
- Sundelin, T.; Lekander, M.; Kecklund, G.; Van Someren, E.J.W.; Olsson, A.; Axelsson, J. Cues of Fatigue: Effects of Sleep Deprivation on Facial Appearance. Sleep 2013, 36, 1355–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Mittal, S. Yawning and its physiological significance. Int. J. Appl. Basic Med. Res. 2013, 3, 11–15. [Google Scholar] [CrossRef]
- Schleicher, R.; Galley, N.; Briest, S.; Galley, L. Blinks and saccades as indicators of fatigue in sleepiness warnings: Looking tired? Ergonomics 2008, 51, 982–1010. [Google Scholar] [CrossRef]
- Arora, S.; Sevdalis, N.; Nestel, D.; Woloshynowych, M.; Darzi, A.; Kneebone, R. The impact of stress on surgical performance: A systematic review of the literature. Surgery 2010, 147, 318–330. [Google Scholar] [CrossRef]
- Wetzel, C.M.; Kneebone, R.L.; Woloshynowych, M.; Nestel, D.; Moorthy, K.; Kidd, J.; Darzi, A. The effects of stress on surgical performance. Am. J. Surg. 2006, 191, 5–10. [Google Scholar] [CrossRef]
- Crewther, B.T.; Shetty, K.; Jarchi, D.; Selvadurai, S.; Cook, C.J.; Leff, D.R.; Darzi, A.; Yang, G.Z. Skill acquisition and stress adaptations following laparoscopic surgery training and detraining in novice surgeons. Surg. Endosc. 2016, 30, 2961–2968. [Google Scholar] [CrossRef] [PubMed]
- LaPorta, A.J.; McKee, J.; Hoang, T.; Horst, A.; McBeth, P.; Gillman, L.M.; Kirkpatrick, A.W. Stress Inoculation: Preparing Outside the Box in Surgical Resuscitation and Education. Curr. Trauma Rep. 2017, 3, 135–143. [Google Scholar] [CrossRef]
- Abe, T.; Dar, F.; Amnattrakul, P.; Aydin, A.; Raison, N.; Shinohara, N.; Khan, M.S.; Ahmed, K.; Dasgupta, P. The effect of repeated full immersion simulation training in ureterorenoscopy on mental workload of novice operators. BMC Med. Educ. 2019, 19, 39. [Google Scholar] [CrossRef] [Green Version]
- Causer, J.; Vickers, J.N.; Snelgrove, R.; Arsenault, G.; Harvey, A. Performing under pressure: Quiet eye training improves surgical knot-tying performance. Surgery 2014, 156, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.; Robinson, A.; Allen, S.; Nathan, E.; Coghlan, E.; Leung, Y. Designing meditation for doctor well-being: Can ‘Om’ help obstetrics and gynaecology doctors? Australas. Psychiatry 2020, 28, 342–347. [Google Scholar] [CrossRef]
- Anton, N.E.; Bean, E.A.; Myers, E.; Stefanidis, D. Optimizing learner engagement during mental skills training: A pilot study of small group vs. individualized training. Am. J. Surg. 2020, 219, 335–339. [Google Scholar] [CrossRef]
- Stefanidis, D.; Anton, N.E.; McRary, G.; Howley, L.D.; Pimentel, M.; Davis, C.; Yurco, A.M.; Sevdalis, N.; Brown, C. Implementation results of a novel comprehensive mental skills curriculum during simulator training. Am. J. Surg. 2017, 213, 353–361. [Google Scholar] [CrossRef] [Green Version]
- Timberlake, M.D.; Stefanidis, D.; Gardner, A.K. Examining the impact of surgical coaching on trainee physiologic response and basic skill acquisition. Surg. Endosc. 2018, 302, 4183–4190. [Google Scholar] [CrossRef]
- Goldberg, M.B.; Mazzei, M.; Maher, Z.; Fish, J.H.; Milner, R.; Yu, D.; Goldberg, A.J. Optimizing performance through stress training—An educational strategy for surgical residents. Am. J. Surg. 2018, 216, 618–623. [Google Scholar] [CrossRef]
- Anton, N.E.; Beane, J.; Yurco, A.M.; Howley, L.D.; Bean, E.; Myers, E.M.; Stefanidis, D. Mental skills training effectively minimizes operative performance deterioration under stressful conditions: Results of a randomized controlled study. Am. J. Surg. 2018, 215, 214–221. [Google Scholar] [CrossRef]
- Lemaire, J.B.; Wallace, J.E.; Lewin, A.M.; de Grood, J.; Schaefer, J.P. The effect of a biofeedback-based stress management tool on physician stress: A randomized controlled clinical trial. Open Med. 2011, 5, e156–e163. [Google Scholar]
- Alobid, I.; De Pablo, J.; Mullol, J.; Centellas, S.; Parramon, G.; Carrasco, J.; Armario, A.; Bernal-Sprekelsen, M. Increased cardiovascular and anxiety outcomes but not endocrine biomarkers of stress during performance of endoscopic sinus surgery: A pilot study among novice surgeons. Arch. Otolaryngol.-Head Neck Surg. 2011, 137, 487–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, K.I.; Amawi, F.; Bhalla, A.; Peacock, O.; Williams, J.P.; Lund, J.N. Assessing surgeon stress when operating using heart rate variability and the State Trait Anxiety Inventory: Will surgery be the death of us? Colorectal Dis. 2015, 17, 335–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Böhm, B.; Rötting, N.; Schwenk, W.; Grebe, S.; Mansmann, U. A prospective randomized trial on heart rate variability of the surgical team during laparoscopic and conventional sigmoid resection. Arch. Surg. 2001, 136, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Marrelli, M.; Gentile, S.; Palmieri, F.; Paduano, F.; Tatullo, M. Correlation between surgeon’s experience, surgery complexity and the alteration of stress related physiological parameters. PLoS ONE 2014, 9, e112444. [Google Scholar] [CrossRef]
- Weenk, M.; Alken, A.P.B.; Engelen, L.J.L.P.G.; Bredie, S.J.H.; van de Belt, T.H.; van Goor, H. Stress measurement in surgeons and residents using a smart patch. Am. J. Surg. 2018, 216, 361–368. [Google Scholar] [CrossRef]
- Grantcharov, P.D.; Boillat, T.; Elkabany, S.; Wac, K.; Rivas, H. Acute mental stress and surgical performance. BJS Open 2019, 3, 119–125. [Google Scholar] [CrossRef]
- Dishman, R.K.; Nakamura, Y.; Garcia, M.E.; Thompson, R.W.; Dunn, A.L.; Blair, S.N. Heart rate variability, trait anxiety, and perceived stress among physically fit men and women. Int. J. Psychophysiol. 2000, 37, 121–133. [Google Scholar] [CrossRef]
- Zhai, J.; Barreto, A. Stress recognition using non-invasive technology. In Proceedings of the FLAIRS 2006 Nineteenth International Florida Artificial Intelligence Research Society Conference, Melbourne Beach, FL, USA, 11–13 May 2006; Volume 1, pp. 395–401. [Google Scholar]
- Acharya, U.R.; Joseph, K.P.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef]
- Borrego, A.; Latorre, J.; Alcaniz, M.; Llorens, R. Reliability of the Empatica E4 wristband to measure electrodermal activity to emotional stimuli. In Proceedings of the International Conference on Virtual Rehabilitation, ICVR, Tel Aviv, Israel, 21–24 July 2019. [Google Scholar]
- Smith, W.D.; Chung, Y.H.; Berguer, R. A virtual instrument ergonomics workstation for measuring the mental workload of performing video-endoscopic surgery. Stud. Health Technol. Inform. 2000, 70, 309–315. [Google Scholar] [CrossRef]
- Hoedemaeker, M. Summary Description of Workload Indicators: WP1 Workload Measures; University of Leeds: Leeds, UK, 2002. [Google Scholar]
- Ershad, M.; Rege, R.; Fey, A.M. Meaningful Assessment of Robotic Surgical Style using the Wisdom of Crowds. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 1037–1048. [Google Scholar] [CrossRef] [PubMed]
- Hurley, A.M.; Kennedy, P.J.; O’Connor, L.; Dinan, T.G.; Cryan, J.F.; Boylan, G.; O’Reilly, B.A. SOS save our surgeons: Stress levels reduced by robotic surgery. Gynecol. Surg. 2015, 12, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Ruiz, N.; Taib, R.; Choi, E.; Chen, F. Galvanic skin response (GSR) as an index of cognitive load. In Proceedings of the Conference on Human Factors in Computing Systems, San Jose, CA, USA, 28 April–3 May 2007; pp. 2651–2656. [Google Scholar]
- Schuetz, M.; Gockel, I.; Beardi, J.; Hakman, P.; Dunschede, F.; Moenk, S.; Heinrichs, W.; Junginger, T. Three different types of surgeon-specific stress reactions identified by laparoscopic simulation in a virtual scenario. Surg. Endosc. 2008, 22, 1263–1267. [Google Scholar] [CrossRef]
- Wilson, C.; Chahine, S.; Cristancho, S.; Aquil, S.; Mandurah, M.; Levine, M.; Sener, A. Unusual suspects: Real-time physiological evaluation of stressors during laparoscopic donor nephrectomy. Can. Urol. Assoc. J. 2020, 15, 205–209. [Google Scholar] [CrossRef]
- Bakker, J.; Pechenizkiy, M.; Sidorova, N. What’s your current stress level? Detection of stress patterns from GSR sensor data. In Proceedings of the IEEE International Conference on Data Mining, ICDM, Vancouver, BC, Canada, 11 December 2011. [Google Scholar]
- Georgiou, K.; Larentzakis, A.; Papavassiliou, A.G. Surgeons’ and surgical trainees’ acute stress in real operations or simulation: A systematic review. Surgeon 2017, 15, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Bartolomeo, L.; Lin, Z.; Zecca, M.; Sessa, S.; Ishii, H.; Xu, H.; Uemura, M.; Tomikawa, M.; Hashizume, M.; Takanishi, A. Surface EMG and heartbeat analysis preliminary results in surgical training: Dry boxes and live tissue. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Boston, MA, USA, 30 August–3 September 2011; pp. 1113–1116. [Google Scholar]
- Duru, D.G.; Duru, A.D.; Barkana, D.E.; Sanli, O.; Ozkan, M. Assessment of surgeon’s stress level and alertness using EEG during laparoscopic simple nephrectomy. In Proceedings of the International IEEE/EMBS Conference on Neural Engineering, NER, San Diego, CA, USA, 6–8 November 2013; pp. 452–455. [Google Scholar]
- Morales, J.M.; Ruiz-Rabelo, J.F.; Diaz-Piedra, C.; Di Stasi, L.L. Detecting Mental Workload in Surgical Teams Using a Wearable Single-Channel Electroencephalographic Device. J. Surg. Educ. 2019, 76, 1107–1115. [Google Scholar] [CrossRef]
- Al-Shargie, F.; Kiguchi, M.; Badruddin, N.; Dass, S.C.; Hani, A.F.M.; Tang, T.B. Mental stress assessment using simultaneous measurement of EEG and fNIRS. Biomed. Opt. Express 2016. [Google Scholar] [CrossRef] [Green Version]
- Al-Shargie, F.; Tang, T.B.; Kiguchi, M. Assessment of mental stress effects on prefrontal cortical activities using canonical correlation analysis: An fNIRS-EEG study. Biomed. Opt. Express 2017. [Google Scholar] [CrossRef]
- Shetty, K.; Leff, D.R.; Orihuela-Espina, F.; Yang, G.Z.; Darzi, A. Persistent prefrontal engagement despite improvements in laparoscopic technical skill. JAMA Surg. 2016, 151, 682–684. [Google Scholar] [CrossRef] [Green Version]
- Arora, S.; Sevdalis, N.; Aggarwal, R.; Sirimanna, P.; Darzi, A.; Kneebone, R. Stress impairs psychomotor performance in novice laparoscopic surgeons. Surg. Endosc. 2010, 24, 2588–2599. [Google Scholar] [CrossRef]
- Arora, S.; Aggarwal, R.; Moran, A.; Sirimanna, P.; Crochet, P.; Darzi, A.; Kneebone, R.; Sevdalis, N. Mental practice: Effective stress management training for novice surgeons. J. Am. Coll. Surg. 2011, 212, 225–233. [Google Scholar] [CrossRef]
- Maher, Z.; Milner, R.; Cripe, J.; Gaughan, J.; Fish, J.; Goldberg, A.J. Stress training for the surgical resident. Am. J. Surg. 2013, 205, 169–274. [Google Scholar] [CrossRef]
- Wetzel, C.M.; George, A.; Hanna, G.B.; Athanasiou, T.; Black, S.A.; Kneebone, R.L.; Nestel, D.; Woloshynowych, M. Stress management training for surgeons-a randomized, controlled, intervention study. Ann. Surg. 2011, 253, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Krohne, H.W.; De Bruin, J.T.; El-Giamal, M.; Schmukle, S.C. The assessment of surgery-related coping: The coping with surgical stress scale (COSS). Psychol. Health 2000, 15, 135–159. [Google Scholar] [CrossRef]
- Arora, S.; Tierney, T.; Sevdalis, N.; Aggarwal, R.; Nestel, D.; Woloshynowych, M.; Darzi, A.; Kneebone, R. The imperial stress assessment tool (ISAT): A feasible, reliable and valid approach to measuring stress in the operating room. World J. Surg. 2010, 34, 1756–1763. [Google Scholar] [CrossRef]
- Wilson, M.S.; Middlebrook, A.; Sutton, C.; Stone, R.; McCloy, R.F. MIST VR: A virtual reality trainer for laparoscopic surgery assesses performance. Ann. R. Coll. Surg. Engl. 1997, 79, 403–404. [Google Scholar] [PubMed]
- Platte, K.; Alleblas, C.C.J.; Inthout, J.; Nieboer, T.E. Measuring fatigue and stress in laparoscopic surgery: Validity and reliability of the star-track test. Minim. Invasive Ther. Allied Technol. 2019, 28, 57–64. [Google Scholar] [CrossRef]
- Kildebro, N.; Amirian, I.; Gögenur, I.; Rosenberg, J. Test re-test reliability and construct validity of the star-track test of manual dexterity. PeerJ 2015, 3, e917. [Google Scholar] [CrossRef] [Green Version]
- Frankenhaeuser, M.; Lundberg, U. The influence of cognitive set on performance and arousal under different noise loads. Motiv. Emot. 1977, 1, 139–149. [Google Scholar] [CrossRef]
- Wijsman, J.; Grundlehner, B.; Penders, J.; Hermens, H. Trapezius muscle EMG as predictor of mental stress. In Proceedings of the Wireless Health 2010, WH’10, San Diego, CA, USA, 5–6 October 2010; pp. 155–163. [Google Scholar]
- Cao, C.G.L.; Zhou, M.; Jones, D.B.; Schwaitzberg, S.D. Can surgeons think and operate with haptics at the same time? J. Gastrointest. Surg. 2007, 11, 1564–1569. [Google Scholar] [CrossRef]
- Sharma, N.; Gedeon, T. Objective measures, sensors and computational techniques for stress recognition and classification: A survey. Comput. Methods Programs Biomed. 2012, 108, 1287–1301. [Google Scholar] [CrossRef] [PubMed]
- Analog Devices AD8232 Datasheet. Available online: https://www.analog.com/media/en/technical-documentation/data-sheets/AD8232.pdf (accessed on 25 March 2020).
- BangGood CJMCU-6701 Datasheet. Available online: http://img.banggood.com/file/products/20181017011131CJMCU-6701.pdf (accessed on 25 March 2020).
- Pope, B. How to perform 3- or 5-lead monitoring. Nursing 2002. [Google Scholar] [CrossRef]
- Oropesa, I.; Escamirosa, F.P.; Sánchez-Margallo, J.A.; Enciso, S.; Rodríguez-Vila, B.; Martínez, A.M.; Sánchez-Margallo, F.M.; Gómez, E.J.; Sánchez-González, P. Interpretation of motion analysis of laparoscopic instruments based on principal component analysis in box trainer settings. Surg. Endosc. 2018, 32, 3096–3107. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate—A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B-Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Erdfelder, E.; FAul, F.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioural Science; Academic Press: Cambridge, MA, USA, 1988; ISBN 0805802835. [Google Scholar]
- Lane, J.D.; Pieper, C.F.; Phillips-Bute, B.G.; Bryant, J.E.; Kuhn, C.M. Caffeine affects cardiovascular and neuroendocrine activation at work and home. Psychosom. Med. 2002, 64, 595–603. [Google Scholar] [CrossRef]
- Chen, H.E.; Sonntag, C.C.; Pepley, D.F.; Prabhu, R.S.; Han, D.C.; Moore, J.Z.; Miller, S.R. Looks can be deceiving: Gaze pattern differences between novices and experts during placement of central lines. Am. J. Surg. 2019, 217, 362–367. [Google Scholar] [CrossRef]
- Marín-Conesa, E.; Sánchez-Ferrer, F.; Grima-Murcia, M.D.; Sánchez-Ferrer, M.L. The Application of a System of Eye Tracking in Laparoscopic Surgery: A New Didactic Tool to Visual Instructions. Front. Surg. 2021, 8, 643611. [Google Scholar] [CrossRef]
- Oropesa, I.; Sánchez-González, P.; Lamata, P.; Chmarra, M.K.; Pagador, J.B.; Sánchez-Margallo, J.A.; Sánchez-Margallo, F.M.; Gómez, E.J. Methods and tools for objective assessment of psychomotor skills in laparoscopic surgery. J. Surg. Res. 2011, 171, 81–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flin, R.; Martin, L.; Goeters, K.M.; Hormann, H.J.; Amalberti, R.; Valot, C.; Nijhuis, H. Development of the NOTECHS (non-technical skills) system for assessing pilots’ CRM skills. Hum. Factors Aerosp. Saf. 2003, 3, 97–119. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metric | Description | Formula |
|---|---|---|
| Time-domain metrics | ||
| AVNN | Average value of NN intervals (ms). | |
| SDNN | Standard deviation of NN intervals. | |
| RMSSD | Root mean square of successive differences between successive NN intervals. | |
| PNN20 | Ratio of the number of pairs of consecutive NN intervals differing by more than 20 ms over the total number of NN intervals. | |
| PNN50 | Ratio of the number of pairs of consecutive NN intervals differing by more than 50 ms over the total number of NN intervals. | |
| Frequency-domain metrics | ||
| LF | Absolute power of the signal in low frequency bands. | |
| HF | Absolute power of the signal in high frequency bands. | |
| LF-HF ratio | Ratio between the total energy in low frequency and the total energy in the high frequency. | |
| LFnu | Normalized spectral LF index. | |
| HFnu | Normalized spectral HF index | |
| MAPs. | Definition | Formulae |
|---|---|---|
| Time (T) | Total time to perform a task (s) | T |
| Path length (PL) | Total path covered by the instrument in the setting (m) | |
| Average speed (S) | Rate of change of the instrument’s position in the setting (mm/s). Results are measured for the total magnitude and in each Cartesian direction of the box trainer. | |
| Average acceleration (A) | Rate of change of the instrument’s velocity within the setting (mm/s2) | |
| Economy of area (EOA) | Relationship between maximum surface area (task plane) occupied by the instrument and total path length | |
| Economy of volume (EOV) | Relationship between maximum volume occupied by the instrument in the setting and total path length | |
| Depth (D) | Total path length travelled in the instrument’s axis direction (m) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guzmán-García, C.; Sánchez-González, P.; Margallo, J.A.S.; Snoriguzzi, N.; Rabazo, J.C.; Margallo, F.M.S.; Gómez, E.J.; Oropesa, I. Correlating Personal Resourcefulness and Psychomotor Skills: An Analysis of Stress, Visual Attention and Technical Metrics. Sensors 2022, 22, 837. https://doi.org/10.3390/s22030837
Guzmán-García C, Sánchez-González P, Margallo JAS, Snoriguzzi N, Rabazo JC, Margallo FMS, Gómez EJ, Oropesa I. Correlating Personal Resourcefulness and Psychomotor Skills: An Analysis of Stress, Visual Attention and Technical Metrics. Sensors. 2022; 22(3):837. https://doi.org/10.3390/s22030837
Chicago/Turabian StyleGuzmán-García, Carmen, Patricia Sánchez-González, Juan A. Sánchez Margallo, Nicola Snoriguzzi, José Castillo Rabazo, Francisco M. Sánchez Margallo, Enrique J. Gómez, and Ignacio Oropesa. 2022. "Correlating Personal Resourcefulness and Psychomotor Skills: An Analysis of Stress, Visual Attention and Technical Metrics" Sensors 22, no. 3: 837. https://doi.org/10.3390/s22030837