
Non-Invasive Monitoring of Human Health by Photoacoustic Spectroscopy


Abstract
:1. Introduction
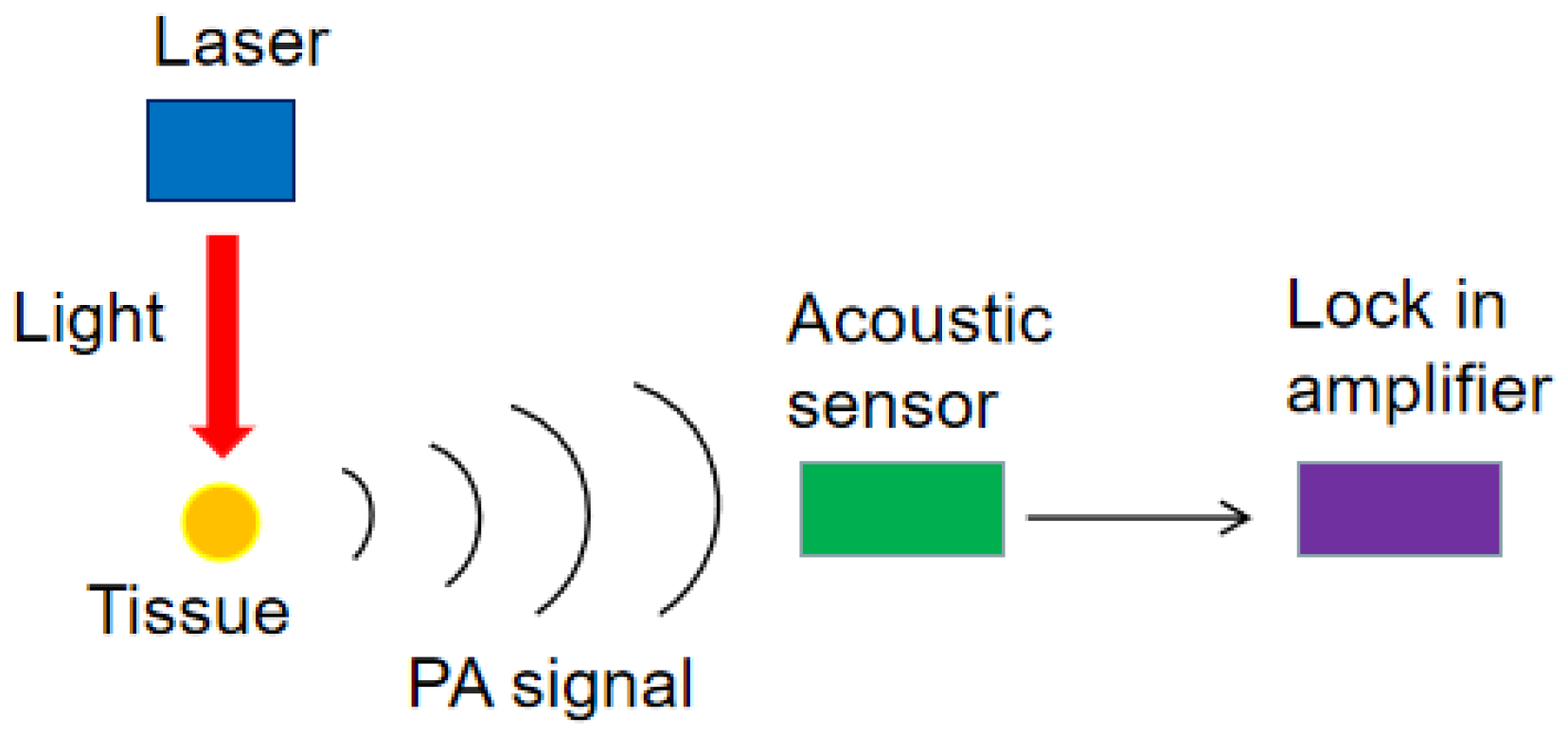
2. Photoacoustic Spectroscopy
3. Non-Invasive Monitoring Methods Based on Photoacoustic Spectroscopy
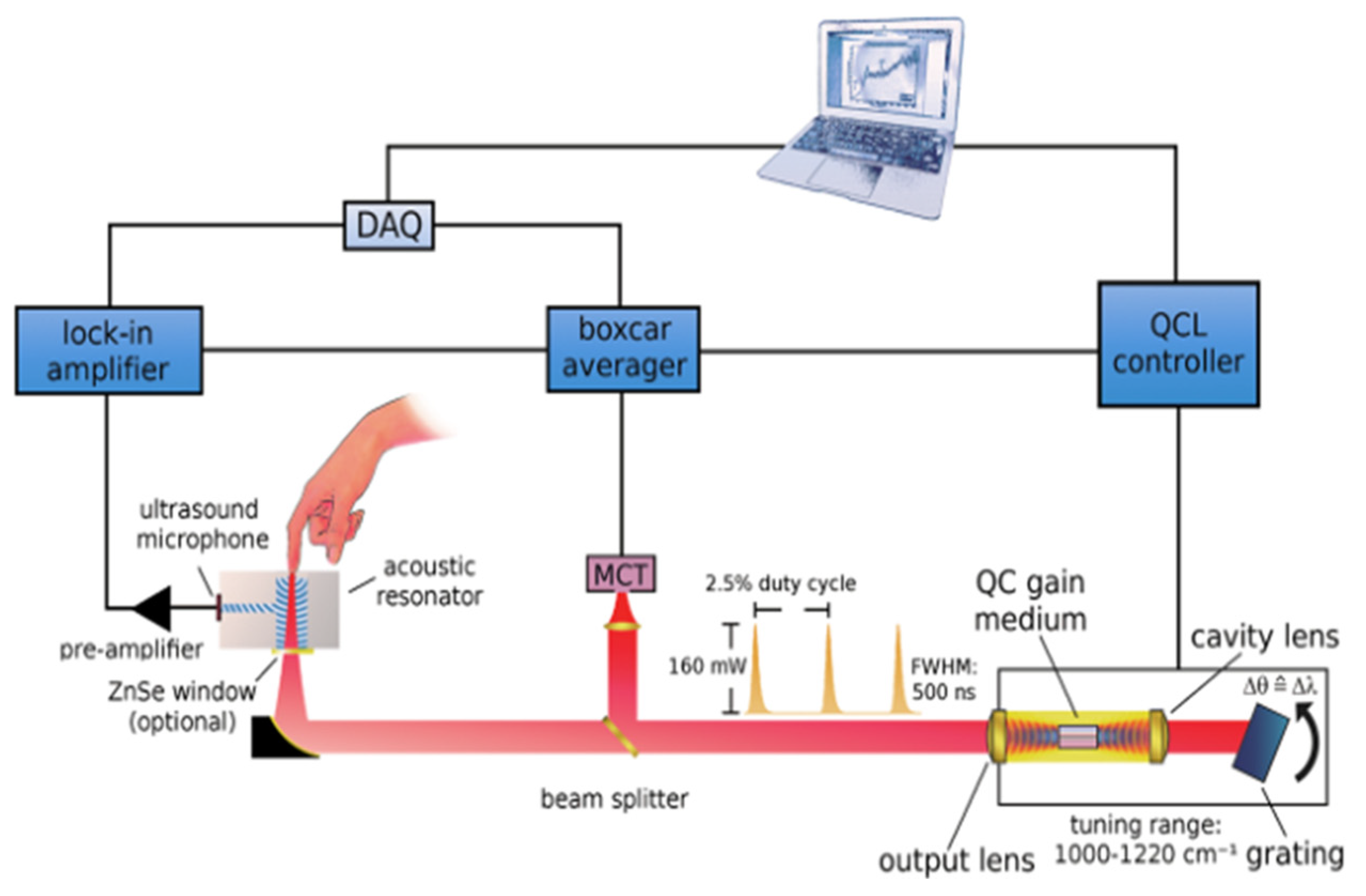
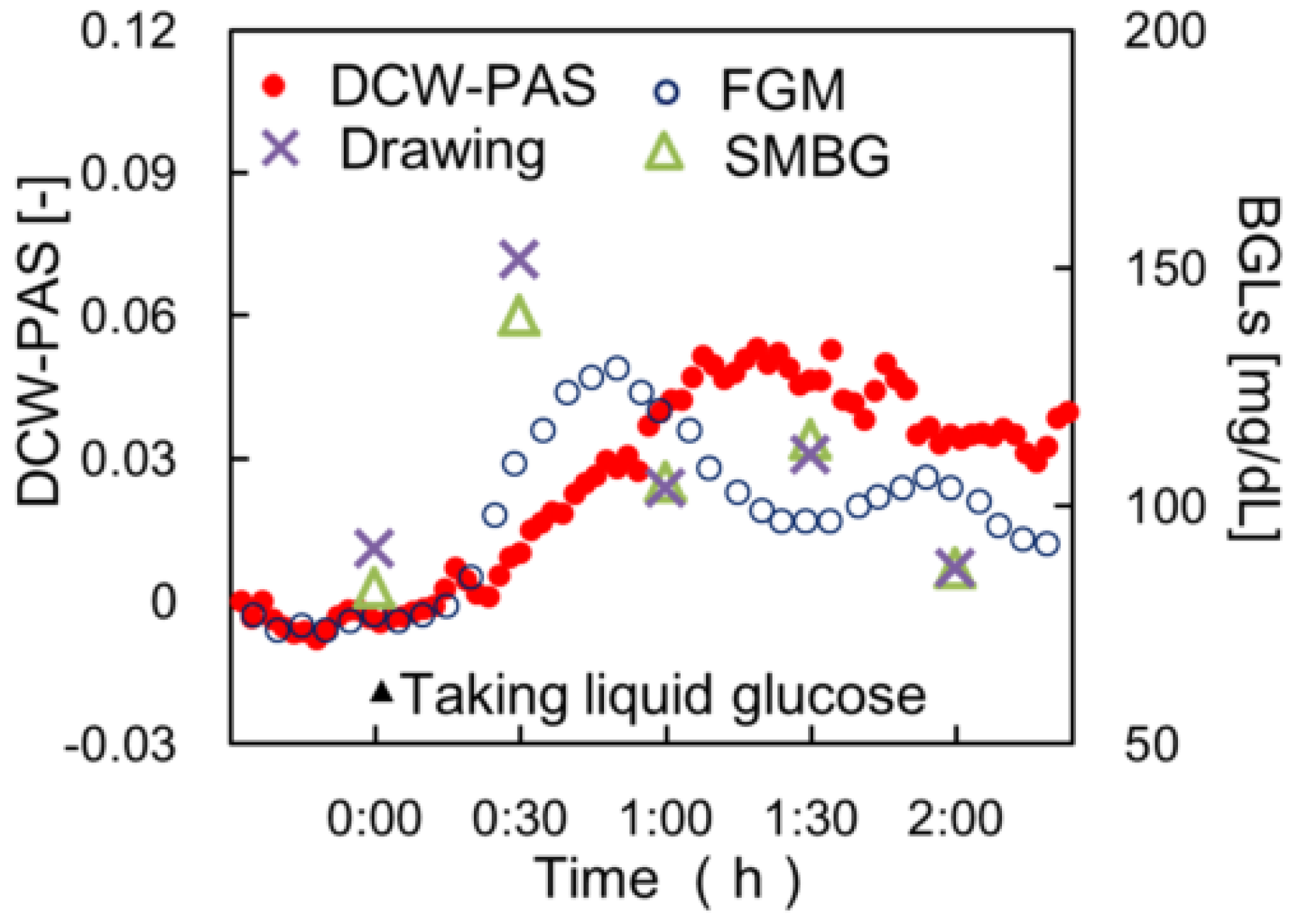
3.1. Non-Invasive Monitoring of Blood Glucose by Photoacoustic Spectroscopy
3.2. Non-Invasive Monitoring of Lipid by Photoacoustic Spectroscopy
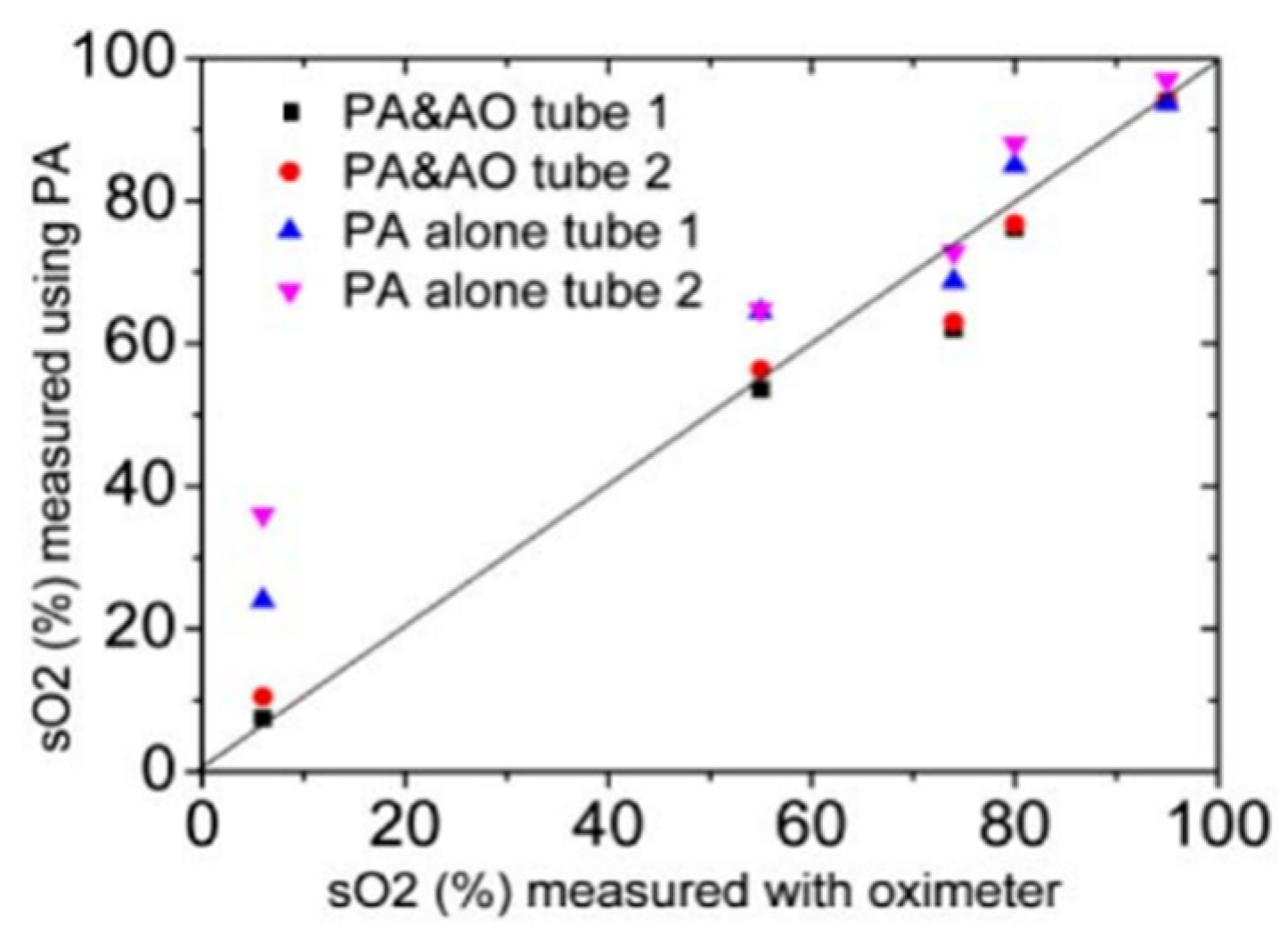
3.3. Non-Invasive Monitoring of Blood Oxygen by Photoacoustic Spectroscopy
3.4. Non-Invasive Monitoring of Cancer Cells by Photoacoustic Spectroscopy
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Whiting, D.R.; Guariguata, L.; Weil, C.; Shaw, J. IDF Diabetes Atlas: Global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res. Clin. Pract. 2011, 94, 311–321. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics Overview 2019: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, R.; Liu, S.; Jin, H.; Luo, Y.; Zheng, Z.; Gao, F.; Zheng, Y. Noninvasive Electromagnetic Wave Sensing of Glucose. Sensors 2019, 19, 1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciudin, A.; Hernandez, C.; Simo, R. Non-Invasive Methods of Glucose Measurement: Current Status and Future Perspectives. Curr. Diabetes Rev. 2011, 8, 48–54. [Google Scholar] [CrossRef]
- Inayat, F.; Rai, A.B. Acute hepatitis C virus infection related to capillary blood glucose meter. Saudi Med. J. 2016, 37, 93–95. [Google Scholar] [CrossRef]
- Yeaw, J.; Lee, W.C.; Aagren, M.; Christensen, T. Cost of self-monitoring of blood glucose in the United States among patients on an insulin regimen for diabetes. J. Manag. Care Pharm. 2012, 18, 21–32. [Google Scholar] [CrossRef]
- Mintz, G.S.; Guagliumi, G. Intravascular imaging in coronary artery disease. Lancet 2017, 390, 793–809. [Google Scholar] [CrossRef]
- Sangha, G.S.; Goergen, C.J. Photoacoustic tomography: Applications for atherosclerosis imaging. J. Opt. UK 2016, 18, 084005. [Google Scholar] [CrossRef]
- Cosottini, M.; Pingitore, A.; Puglioli, M.; Michelassi, M.C.; Lupi, G.; Abbruzzese, A.; Calabrese, R.; Lombardi, M.; Parenti, G.; Bartolozzi, C. Contrast-enhanced three-dimensional magnetic resonance angiography of atherosclerotic internal carotid stenosis as the noninvasive imaging modality in revascularization decision making. Stroke 2003, 34, 660. [Google Scholar] [CrossRef] [Green Version]
- Berg, W.A.; Gutierrez, L.; Nessaiver, M.S.; Carter, W.B.; Bhargavan, M.; Lewis, R.S.; Ioffe, O.B. Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer. Radiology 2004, 233, 830–849. [Google Scholar] [CrossRef]
- Ray, A.; Yoon, H.K.; Lee, Y.E.K.; Kopelman, R.; Wang, X.D. Sonophoric nanoprobe aided pH measurement in vivo using photoacoustic spectroscopy. Analyst 2013, 138, 3126–3130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, B.D.; Schiebler, M.L.; Sommer, G.; Kauczor, H.U.; Biederer, J.; Kruser, T.J.; Carr, J.C.; Hazen, G. Cost-effectiveness of lung MRI in lung cancer screening. Eur. Radiol. 2020, 30, 1738–1746. [Google Scholar] [CrossRef] [PubMed]
- Paul, A.B.; Oklu, R.; Saini, S.; Prabhakar, A.M. How Much Is That Head CT? Price Transparency and Variability in Radiology. J. Am. Coll. Radiol. 2015, 12, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Kiekkas, P.; Alimoutsi, A.; Tseko, F.; Bakalis, N.; Stefanopoulos, N.; Fotis, T.; Konstantinou, E. Knowledge of pulse oximetry: Comparison among intensive care, anesthesiology and emergency nurses. J. Clin. Nurs. 2013, 22, 828–837. [Google Scholar] [CrossRef] [PubMed]
- Pandey, R.; Paidi, S.K.; Valdez, T.A.; Zhang, C.; Spegazzini, N.; Dasari, R.R.; Barman, I. Noninvasive Monitoring of Blood Glucose with Raman Spectroscopy. Acc. Chem. Res. 2017, 50, 264–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czamara, K.; Majzner, K.; Pacia, M.Z.; Kochan, K.; Baranska, M. Raman spectroscopy of lipids: A review. J. Raman. Spectrosc. 2015, 1, 4–20. [Google Scholar] [CrossRef]
- Atkins, C.G.; Buckley, K.; Turner, R.F.B.; Blades, M.W. Raman Spectroscopy of Blood and Blood Components. Appl. Spectrosc. 2017, 71, 767–793. [Google Scholar] [CrossRef]
- Sim, J.Y.; Ahn, C.G.; Jeong, E.J.; Kim, B.K. Microscopic Photoacoustic Spectroscopy for Non-Invasive Glucose Monitoring Invulnerable to Skin Secretion Products. Sci. Rep. 2018, 8, 1059. [Google Scholar] [CrossRef] [Green Version]
- Rassel, S.; Xu, C.; Zhang, S.; Ban, D. Noninvasive blood glucose detection using a quantum cascade laser. Analyst 2020, 145, 2441–2456. [Google Scholar] [CrossRef]
- Tanaka, Y.; Tajima, T.; Seyama, M.; Waki, K. Differential Continuous Wave Photoacoustic Spectroscopy for Non-Invasive Glucose Monitoring. IEEE Sens. J. 2020, 20, 4453–4458. [Google Scholar] [CrossRef]
- Liu, J.; Liu, R.; Xu, K.X. Accuracy of Noninvasive Glucose Sensing Based on Near-Infrared Spectroscopy. Appl. Spectrosc. 2015, 69, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.T.; Chen, H.; Xiong, D.M.; Huang, G.; Ai, H.; Liang, Y.; Yan, X.Y.; Gan, Y.; Chen, C.; Chao, R.B.; et al. Noninvasive Measurement of Glucose in Artificial Plasma with Near-Infrared and Raman Spectroscopy. Appl. Spectrosc. 2014, 68, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Tang, Y.; Yao, J. Photoacoustic tomography of blood oxygenation: A mini review. Photoacoustic 2018, 10, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.Y.; Fan, X.; Li, Y.Y.; Qu, L.L.; Qin, H.Y.; Cao, Y.N.; Li, H.T. Multispectral Photoacoustic Tomography and Its Development in Biomedical Application. Prog. Chem. 2015, 27, 1459–1469. [Google Scholar]
- Lin, L.; Tong, X.; Hu, P.; Invernizzi, M.; Lai, L.L.; Wang, L.V. Photoacoustic Computed Tomography of Breast Cancer in Response to Neoadjuvant Chemotherapy. Adv. Sci. 2021, 8, 2003396. [Google Scholar] [CrossRef] [PubMed]
- Nandy, S.; Mostafa, A.; Hagemann, I.S.; Powell, M.A.; Amidi, E.; Robinson, K.; Mutch, D.G.; Siegel, C.; Zhu, Q. Evaluation of Ovarian Cancer: Initial Application of Coregistered Photoacoustic Tomography and US. Radiology 2018, 289, 740–747. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Y.; Yang, S.H. Reflection-mode photoacoustic microscopy using a hollow focused ultrasound transducer for in vivo imaging of blood vessels. Chinese Phys. B 2012, 21, 054211. [Google Scholar] [CrossRef]
- Min, T.; Yong, Z.; Zhang, R.; Wang, L.V. Noninvasive photoacoustic microscopy of methemoglobin in vivo. J. Biomed. Opt. 2015, 20, 036007. [Google Scholar]
- Favazza, C.P.; Jassim, O.W.; Cornelius, L.A.; Wang, L.V. In vivo photoacoustic microscopy of human cutaneous microvasculature and a nevus. J. Biomed. Opt. 2011, 16, 016015. [Google Scholar] [CrossRef]
- Dizeux, A.; Payen, T.; Le Guillou-Buffello, D.; Comperat, E.; Gennisson, J.-L.; Tanter, M.; Oelze, M.; Bridal, S.L. In Vivo Multiparametric Ultrasound Imaging of Structural and Functional Tumor Modifications during Therapy. Ultrasound Med. Biol. 2017, 43, 2000–2012. [Google Scholar] [CrossRef]
- Zhou, Y.F. Noninvasive Treatment of Breast Cancer Using High-Intensity Focused Ultrasound. J. Med. Imaging Health Inform. 2013, 3, 141–156. [Google Scholar] [CrossRef]
- Wu, F. High intensity focused ultrasound: A noninvasive therapy for locally advanced pancreatic cancer. World J. Gastroenterol. 2014, 20, 16480–16488. [Google Scholar] [CrossRef] [PubMed]
- Bayer, C.L.; Joshi, P.P.; Emelianov, S.Y. Photoacoustic imaging: A potential tool to detect early indicators of metastasis. Expert Rev. Med. Devices 2013, 10, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, H.; Wang, L.V. Photoacoustic imaging and characterization of the microvasculature. J. Biomed. Opt. 2010, 15, 011101. [Google Scholar]
- Erfanzadeh, M.; Zhu, Q. Photoacoustic imaging with low-cost sources; A review. Photoacoustics 2019, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dumitras, D.C.; Petrus, M.; Bratu, A.M.; Popa, C. Applications of Near Infrared Photoacoustic Spectroscopy for Analysis of Human Respiration: A Review. Molecules 2020, 25, 1728. [Google Scholar] [CrossRef]
- Iskander-Rizk, S.; van der Steen, A.F.W.; van Soest, G. Photoacoustic imaging for guidance of interventions in cardiovascular medicine. Phys. Med. Biol. 2019, 64, 16TR01. [Google Scholar] [CrossRef] [Green Version]
- Beard, P. Biomedical photoacoustic imaging. Interface Focus Theme Suppl. J. R. Soc. Interface 2011, 1, 602. [Google Scholar] [CrossRef]
- Viengerov, M.L. New method of gas analysis based on Tyndall-Roentgen opto-acoustic effect. Dokl. Akad. Nauk SSSR 1938, 19, 8. [Google Scholar]
- Kreuzer, L.B. Ultralow Gas Concentration Infrared Absorption Spectroscopy. J. Appl. Phys. 1971, 42, 2934–2943. [Google Scholar] [CrossRef]
- Pleitez, M.A.; Lieblein, T.; Bauer, A.; Hertzberg, O.; von Lilienfeld-Toal, H.; Mantele, W. In vivo noninvasive monitoring of glucose concentration in human epidermis by mid-infrared pulsed photoacoustic spectroscopy. Anal. Chem. 2013, 85, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Kottmann, J.; Rey, J.M.; Luginbuhl, J.; Reichmann, E.; Sigrist, M.W. Glucose sensing in human epidermis using mid-infrared photoacoustic detection. Biomed. Opt. Express 2012, 3, 667–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kottmann, J.; Grob, U.; Rey, J.M.; Sigrist, M.W. Mid-infrared fiber-coupled photoacoustic sensor for biomedical applications. Sensors 2013, 13, 535–549. [Google Scholar] [CrossRef]
- Liakat, S.; Bors, K.A.; Xu, L.; Woods, C.M.; Doyle, J.; Gmachl, C.F. Noninvasive in vivo glucose sensing on human subjects using mid-infrared light. Biomed. Opt. Express 2014, 5, 2397–2404. [Google Scholar] [CrossRef]
- Orfanakis, M.; Tserevelakis, G.J.; Zacharakis, G. A Cost-Efficient Multiwavelength LED-Based System for Quantitative Photoacoustic Measurements. Sensors 2021, 21, 4888. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Gao, F.; Feng, X.; Liu, S.; Kishor, R.; Luo, Y.; Zheng, Y. Noninvasive photoacoustic measurement of glucose by data fusion. Analyst 2017, 142, 2892–2896. [Google Scholar] [CrossRef]
- Zhang, R.; Luo, Y.; Jin, H.; Gao, F.; Zheng, Y. Time-domain photoacoustic waveform analysis for glucose measurement. Analyst 2021, 145, 7964–7972. [Google Scholar] [CrossRef]
- Zhang, Y.J.; Chen, S.; Yu, Y.L.; Wang, J.H. A miniaturized photoacoustic device with laptop readout for point-of-care testing of blood glucose. Talanta 2020, 209, 120527. [Google Scholar] [CrossRef]
- Prakash, J.; Seyedebrahimi, M.M.; Ghazaryan, A.; Malekzadeh-Najafabadi, J.; Gujrati, V.; Ntziachristos, V. Short-wavelength optoacoustic spectroscopy based on water muting. Proc. Natl. Acad. Sci. USA 2020, 117, 4007–4014. [Google Scholar] [CrossRef] [Green Version]
- Clarke, W.L.; Cox, D.; Gonder-Frederick, L.A.; Carter, W.; Pohl, S.L. Evaluating clinical accuracy of systems for self-monitoring of blood glucose. Diabetes Care 1987, 10, 622–628. [Google Scholar] [CrossRef]
- Wu, M.; Jansen, K.; van der Steen, A.F.; van Soest, G. Specific imaging of atherosclerotic plaque lipids with two-wavelength intravascular photoacoustics. Biomed. Opt. Express 2015, 6, 3276–3286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, T.J.; Hall, A.; Dhillon, A.P.; Owen, J.S.; Beard, P.C. Spectroscopic photoacoustic imaging of lipid-rich plaques in the human aorta in the 740 to 1400 nm wavelength range. J. Biomed. Opt. 2012, 17, 061209. [Google Scholar] [CrossRef] [PubMed]
- Jansen, K.; Wu, M.; van der Steen, A.F.W.; van Soest, G. Lipid detection in atherosclerotic human coronaries by spectroscopic intravascular photoacoustic imaging. Opt. Express 2013, 21, 21472–21484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, K.; van der Steen, A.F.; Wu, M.; van Beusekom, H.M.; Springeling, G.; Li, X.; Zhou, Q.; Shung, K.K.; de Kleijn, D.P.; van Soest, G. Spectroscopic intravascular photoacoustic imaging of lipids in atherosclerosis. J. Biomed. Opt. 2014, 19, 026006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, K.; Wu, M.; Steen, A.; Soest, G.V.J.P. Photoacoustic imaging of human coronary atherosclerosis in two spectral bands. Photoacoustics 2014, 2, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Wang, H.W.; Sturek, M.; Cheng, J.X. Bond-selective imaging of deep tissue through the optical window between 1600 and 1850 nm. J. Biophotonics 2012, 5, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Iskander-Rizk, S.; Visscher, M.; Moerman, A.M.; Korteland, S.A.; Van der Heiden, K.; Van der Steen, A.F.W.; Van Soest, G. Micro Spectroscopic Photoacoustic (mu sPA) imaging of advanced carotid atherosclerosis. Photoacoustics 2021, 22, 100261. [Google Scholar] [CrossRef]
- He, Y.; Shi, J.; Pleitez, M.A.; Maslov, K.; Wagenaar, D.A.; Wang, L.V. Label-free imaging of lipid-rich biological tissues by mid-infrared photoacoustic microscopy. J. Biomed. Opt. 2020, 25, 106506. [Google Scholar] [CrossRef]
- Dasa, M.K.; Markos, C.; Maria, M.; Petersen, C.R.; Moselund, P.M.; Bang, O. High-pulse energy supercontinuum laser for high-resolution spectroscopic photoacoustic imaging of lipids in the 1650-1850 nm region. Biomed. Opt. Express 2018, 9, 1762–1770. [Google Scholar] [CrossRef] [Green Version]
- Laufer, J.; Elwell, C.; Delpy, D.; Beard, P. In vitro measurements of absolute blood oxygen saturation using pulsed near-infrared photoacoustic spectroscopy: Accuracy and resolution. Phys. Med. Biol. 2005, 50, 4409–4428. [Google Scholar] [CrossRef] [Green Version]
- Narotam, P.K.; Morrison, J.F.; Nathoo, N. Brain Tissue Oxygen Monitoring in Traumatic Brain Injury and Major Trauma: Outcome Analysis of a Brain Tissue Oxygen-Directed Therapy. J. Neurosurg. 2009, 111, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Chung, F.; Liao, P.; Elsaid, H.; Islam, S.; Shapiro, C.M.; Sun, Y. Oxygen desaturation index from nocturnal oximetry: A sensitive and specific tool to detect sleep-disordered breathing in surgical patients. Anesth. Analg. 2012, 114, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.S.; Mandelis, A.; Guo, X.; Lashkari, B.; Kellnberger, S.; Ntziachristos, V. Wavelength-Modulated Differential Photoacoustic Spectroscopy (WM-DPAS) for noninvasive early cancer detection and tissue hypoxia monitoring. J. Biophotonics 2016, 9, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Ling, L.; Gang, L. Wavelength selection method based on test analysis of variance: Application to oximetry. Anal Methods UK 2014, 6, 1082–1089. [Google Scholar]
- Kiguna, S.; Masanori, F.; Takeshi, H.; Shinpei, O.; Toshihiro, K.; Hidenori, S.; Kenichi, F.; Miya, I. Measurement of blood-oxygen saturation using a photoacoustic technique in the rabbit hypoxemia model. J. Clin. Monit. Comput. 2018, 33, 269–279. [Google Scholar]
- Hussain, A.; Petersen, W.; Staley, J.; Hondebrink, E.; Steenbergen, W. Quantitative blood oxygen saturation imaging using combined photoacoustics and acousto-optics. Opt. Lett. 2016, 41, 1720–1723. [Google Scholar] [CrossRef] [Green Version]
- Gao, F.; Peng, Q.; Feng, X.; Gao, B.; Zheng, Y. Single-Wavelength Blood Oxygen Saturation Sensing with Combined Optical Absorption and Scattering. IEEE Sens. J. 2016, 16, 1943–1948. [Google Scholar] [CrossRef]
- Lashkari, B.; Choi, S.s.S.; Dovlo, E.; Dhody, S.; Mandelis, A. Frequency-Domain Photoacoustic Phase Spectroscopy: A Fluence-Independent Approach for Quantitative Probing of Hemoglobin Oxygen Saturation. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 127–136. [Google Scholar] [CrossRef]
- Oh, J.T.; Li, M.L.; Zhang, H.F.; Maslov, K.; Stoica, G.; Wang, L.V. Three-dimensional imaging of skin melanoma in vivo by dual-wavelength photoacoustic microscopy. J. Biomed. Opt. 2006, 11, 34032. [Google Scholar] [CrossRef]
- Galanzha, E.I.; Menyaev, Y.A.; Yadem, A.C.; Sarimollaoglu, M.; Juratli, M.A.; Nedosekin, D.A.; Foster, S.R.; Jamshidi-Parsian, A.; Siegel, E.R.; Makhoul, I.; et al. In vivo liquid biopsy using Cytophone platform for photoacoustic detection of circulating tumor cells in patients with melanoma. Sci. Transl. Med. 2019, 11, 496. [Google Scholar] [CrossRef]
- Rodrigues, J.; Amin, A.; Raghushaker, C.R.; Chandra, S.; Joshi, M.B.; Prasad, K.; Rai, S.; Nayak, S.G.; Ray, S.; Mahato, K.K. Exploring photoacoustic spectroscopy-based machine learning together with metabolomics to assess breast tumor progression in a xenograft model ex vivo. Lab. Investig. 2021, 101, 952–965. [Google Scholar] [CrossRef] [PubMed]
- Priya, M.; Satish Rao, B.S.; Chandra, S.; Datta, A.; Nayak, S.G.; Mahato, K.K. Monitoring breast tumor progression by photoacoustic measurements: A xenograft mice model study. J. Biomed. Opt. 2015, 20, 105002. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.D.; Qiao, H.; Dai, Q.H.; Ma, C. Deep learning in photoacoustic imaging: A review. J. Biomed. Opt. 2021, 26, 040901. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technology | Wavelength | Range | Target | Measurement Error | |
|---|---|---|---|---|---|
| Continuous wavelength | [42] | 8200–10,000 nm | 50–300 mg/dL | Skin/in vivo | 7–15 mg/dL (RMSE) |
| [43] | 9130–9900 nm | >100 mg/dL | ISF/in vitro | - | |
| [44] | 9130–9900 nm | >57 mg/dL | Glucose solution and skin/in vitro and in vivo | - | |
| [45] | 8000–10,000 nm | 75–160 mg/dL | Skin/in vivo | 16% (outside of the clinical region based on the Clarke grid [51]) | |
| Dual wavelength | [21] | 1382 and 1610 nm | 50–300 mg/dL | Skin/in vivo | 19–48 mg/dL (standard error), <10% (outside of the clinical region based on the Clarke grid) |
| Single wavelength | [48] | 1600 nm | >30 mg/dL | Human blood serum/in vitro | 9.84 mg/dL (RMSE), 14.9 mg/dL (standard deviation) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, Y.; Yin, Y.; Li, C.; Liu, H.; Shi, J. Non-Invasive Monitoring of Human Health by Photoacoustic Spectroscopy. Sensors 2022, 22, 1155. https://doi.org/10.3390/s22031155
Jin Y, Yin Y, Li C, Liu H, Shi J. Non-Invasive Monitoring of Human Health by Photoacoustic Spectroscopy. Sensors. 2022; 22(3):1155. https://doi.org/10.3390/s22031155
Chicago/Turabian StyleJin, Yongyong, Yonggang Yin, Chiye Li, Hongying Liu, and Junhui Shi. 2022. "Non-Invasive Monitoring of Human Health by Photoacoustic Spectroscopy" Sensors 22, no. 3: 1155. https://doi.org/10.3390/s22031155