
Mueller Matrix Microscopy for In Vivo Scar Tissue Diagnostics and Treatment Evaluation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Mueller Formalism
2.2. Polarization Staining
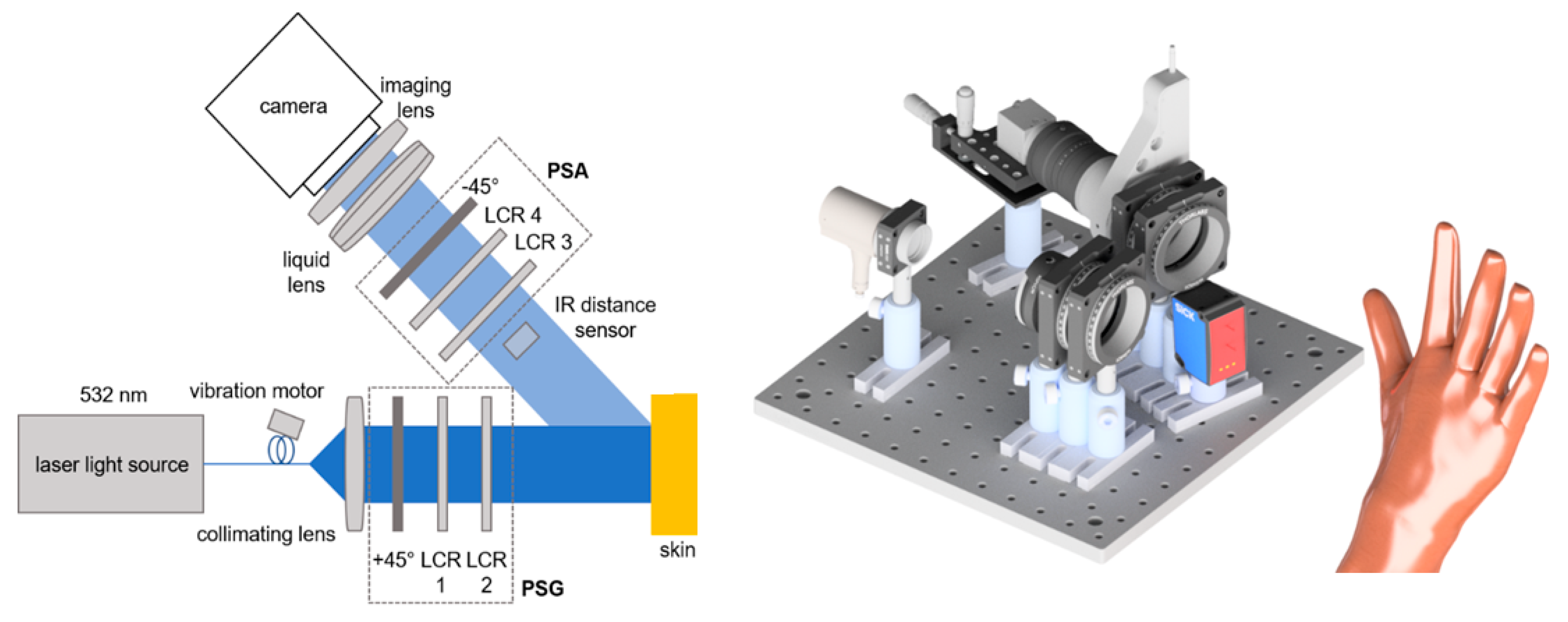
2.3. Mueller Matrix Polarimeter
3. Results
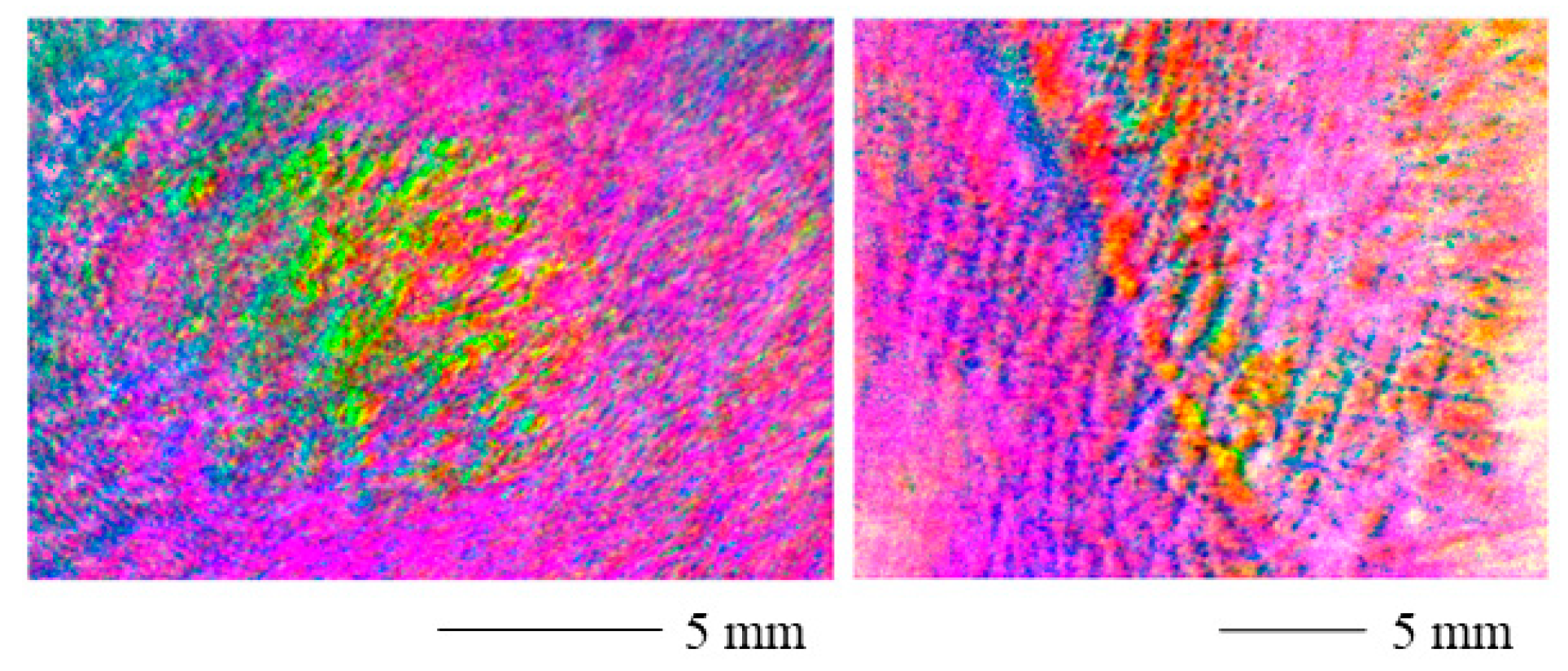
3.1. Scar Imaging
3.2. Wound Healing Monitoring
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Block, L.; Gosain, A.; King, T.W. Emerging Therapies for Scar Prevention. Adv. Wound Care 2015, 4, 607–614. [Google Scholar] [CrossRef] [Green Version]
- Marghoob, N.G.; Liopyris, K.; Jaimes, N. Dermoscopy: A Review of the Structures That Facilitate Melanoma Detection. J. Am. Osteopath. Assoc. 2019, 119, 380–390. [Google Scholar] [CrossRef]
- Yoo, M.G.; Kim, I.-H. Keloids and hypertrophic scars: Characteristic vascular structures visualized by using dermoscopy. Ann. Dermatol. 2014, 26, 603–609. [Google Scholar] [CrossRef] [Green Version]
- Trace, A.P.; Enos, C.W.; Mantel, A.; Harvey, V.M. Keloids and Hypertrophic Scars: A Spectrum of Clinical Challenges. Am. J. Clin. Dermatol. 2016, 17, 201–223. [Google Scholar] [CrossRef] [PubMed]
- Choo, A.M.H.; Ong, Y.S.; Issa, F. Scar Assessment Tools: How Do They Compare? Front. Surg. 2021, 8, 643098. [Google Scholar] [CrossRef] [PubMed]
- Brissett, A.E.; Sherris, D.A. Scar contractures, hypertrophic scars, and keloids. Facial Plast. Surg. 2001, 17, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Carswell, L.; Borger, J. Hypertrophic Scarring Keloids; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ogawa, R.; Akaishi, S.; Hyakusoku, H. Differential and exclusive diagnosis of diseases that resemble keloids and hypertrophic scars. Ann. Plast. Surg. 2009, 62, 660–664. [Google Scholar] [CrossRef]
- Becker, A.; Fricke, D.; Roth, B.; Glasmacher, B. Assuring Quality of Scaffolds in Musculoskeletal Tissue Engineering. Curr. Dir. Biomed. Eng. 2021, 7, 179–182. [Google Scholar] [CrossRef]
- Peyvasteh, M.; Popov, A.; Bykov, A.; Pierangelo, A.; Novikova, T.; Meglinski, I. Evolution of raw meat polarization-based properties by means of Mueller matrix imaging. J. Biophotonics 2021, 14, e202000376. [Google Scholar] [CrossRef]
- Jütte, L.; Sharma, G.; Fricke, D.; Franke, M.; Wollweber, M.; Roth, B. Mueller Matrix-Based Approach for the Ex Vivo Detection of Riboflavin-Treated Transparent Biotissue. Appl. Sci. 2021, 11, 11515. [Google Scholar] [CrossRef]
- Ushenko, V.A.; Hogan, B.T.; Dubolazov, A.; Piavchenko, G.; Kuznetsov, S.L.; Ushenko, A.G.; Ushenko, Y.O.; Gorsky, M.; Bykov, A.; Meglinski, I. 3D Mueller matrix mapping of layered distributions of depolarisation degree for analysis of prostate adenoma and carcinoma diffuse tissues. Sci. Rep. 2021, 11, 5162. [Google Scholar] [CrossRef] [PubMed]
- Alali, S.; Vitkin, A. Polarized light imaging in biomedicine: Emerging Mueller matrix methodologies for bulk tissue assessment. J. Biomed. Opt. 2015, 20, 61104. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Khaliq, A.; Iqbal, M.; Khan, S. Mueller matrix polarimetry for characterization of skin tissue samples: A review. Photodiagnosis Photodyn. Ther. 2020, 30, 101708. [Google Scholar] [CrossRef] [PubMed]
- Zhai, H.; Huang, R.; Shao, C.; He, H.; Ma, H. A quantitative and non-contact technique to detect skin water content based on Mueller matrix polarimetry. In Proceedings of the Polarized Light and Optical Angular Momentum for Biomedical Diagnostics, Online Only, USA, 6–11 March 2021; Ramella-Roman, J.C., Ed.; SPIE: Bellingham, WA, USA, 2021; p. 29. ISBN 9781510641273. [Google Scholar]
- Shi, Y.; Sun, Y.; Huang, R.; Zhou, Y.; Zhai, H.; Fan, Z.; Ou, Z.; Huang, P.; He, H.; He, C.; et al. A quantitative technique to analyze and evaluate microstructures of skin hair follicles based on mueller matrix polarimetry. Front. Phys. 2022, 10, 847656. [Google Scholar] [CrossRef]
- Dong, Y.; He, H.; Sheng, W.; Wu, J.; Ma, H. A quantitative and non-contact technique to characterise microstructural variations of skin tissues during photo-damaging process based on Mueller matrix polarimetry. Sci. Rep. 2017, 7, 14702. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, I.; Ahmad, M.; Khan, K.; Ikram, M. Polarimetry based partial least square classification of ex vivo healthy and basal cell carcinoma human skin tissues. Photodiagnosis Photodyn. Ther. 2016, 14, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Pham, H.T.-T.; Nguyen, A.L.-T.; Vo, T.-V.; Huynh, K.-C.; Phan, Q.-H. Optical parameters of human blood plasma, collagen, and calfskin based on the Stokes-Mueller technique. Appl. Opt. 2018, 57, 4353–4359. [Google Scholar] [CrossRef] [PubMed]
- Louie, D.C.; Phillips, J.; Tchvialeva, L.; Kalia, S.; Lui, H.; Wang, W.; Lee, T.K. Degree of optical polarization as a tool for detecting melanoma: Proof of principle. J. Biomed. Opt. 2018, 23, 1–7. [Google Scholar] [CrossRef]
- Louie, D.C.; Tchvialeva, L.; Kalia, S.; Lui, H.; Lee, T. Constructing a portable optical polarimetry probe for in-vivo skin cancer detection. J. Biomed. Opt. 2021, 26, 035001. [Google Scholar] [CrossRef]
- Luu, N.T.; Le, T.-H.; Phan, Q.-H.; Pham, T.-T.-H. Characterization of Mueller matrix elements for classifying human skin cancer utilizing random forest algorithm. J. Biomed. Opt. 2021, 26, 075001. [Google Scholar] [CrossRef]
- Ghassemi, P.; Lemaillet, P.; Germer, T.A.; Shupp, J.W.; Venna, S.S.; Boisvert, M.E.; Flanagan, K.E.; Jordan, M.H.; Ramella-Roman, J.C. Out-of-plane Stokes imaging polarimeter for early skin cancer diagnosis. J. Biomed. Opt. 2012, 17, 76014. [Google Scholar] [CrossRef] [PubMed]
- Fricke, D.; Becker, A.; Jütte, L.; Bode, M.; de Cassan, D.; Wollweber, M.; Glasmacher, B.; Roth, B. Mueller Matrix Measurement of Electrospun Fiber Scaffolds for Tissue Engineering. Polymers 2019, 11, 2062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bickel, W.S.; Bailey, W.M. Stokes vectors, Mueller matrices, and polarized scattered light. Am. J. Phys. 1985, 53, 468–478. [Google Scholar] [CrossRef]
- Ivanov, D.; Dremin, V.; Bykov, A.; Borisova, E.; Genova, T.; Popov, A.; Ossikovski, R.; Novikova, T.; Meglinski, I. Colon cancer detection by using Poincaré sphere and 2D polarimetric mapping of ex vivo colon samples. J. Biophotonics 2020, 13, e202000082. [Google Scholar] [CrossRef]
- Fricke, D. Development of a Dermoscopic Camera with Mueller Matrix Imaging. Ph.D. Thesis, Leibniz University Hannover, Hannover, Germany, 2020. [Google Scholar]
- Cameron, B.D.; Li, Y.; Nezhuvingal, A. Determination of optical scattering properties in turbid media using Mueller matrix imaging. J. Biomed. Opt. 2006, 11, 54031. [Google Scholar] [CrossRef] [PubMed]
- Compain, E.; Poirier, S.; Drevillon, B. General and self-consistent method for the calibration of polarization modulators, polarimeters, and mueller-matrix ellipsometers. Appl. Opt. 1999, 38, 3490–3502. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.-Y.; Chipman, R.A. Interpretation of Mueller matrices based on polar decomposition. J. Opt. Soc. Am. A 1996, 13, 1106. [Google Scholar] [CrossRef]
- Novikova, T.; Kim, M.; Ryung Lee, H.; Ossikovski, R.; Malfait-Jobart, A.; Lamarque, D. Optical diagnosis of gastric tissue biopsies with Mueller microscopy and statistical analysis. J. Eur. Opt. Society-Rapid Publ. 2022, 18, 10. [Google Scholar] [CrossRef]
- Zhai, H.; Sun, Y.; He, H.; Chen, B.; He, C.; Wang, Y.; Ma, H. Distinguishing tissue structures via polarization staining images based on different combinations of Mueller matrix polar decomposition parameters. Opt. Lasers Eng. 2022, 152, 106955. [Google Scholar] [CrossRef]
- Maity, A.; Pattanaik, A.; Sagnika, S.; Pani, S. A Comparative Study on Approaches to Speckle Noise Reduction in Images. In Proceedings of the 2015 International Conference on Computational Intelligence & Networks (CINE), Odisha, India, 12–13 January 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 148–155, ISBN 978-1-4799-7548-8. [Google Scholar]
- Jütte, L.; Sharma, G.; Patel, H.; Roth, B. Registration of polarimetric images for in vivo skin diagnostics. J. Biomed. Opt. 2022, 27, 096001. [Google Scholar] [CrossRef]
- Van Zuijlen, P.P.; Ruurda, J.J.; van Veen, H.A.; van Marle, J.; van Trier, A.J.; Groenevelt, F.; Kreis, R.W.; Middelkoop, E. Collagen morphology in human skin and scar tissue: No adaptations in response to mechanical loading at joints. Burns 2003, 29, 423–431. [Google Scholar] [CrossRef]
- Atkinson, G.A.; Ernst, J.D. High-sensitivity analysis of polarization by surface reflection. Mach. Vis. Appl. 2018, 29, 1171–1189. [Google Scholar] [CrossRef] [Green Version]
- Phan, Q.-H.; Lo, Y.-L. An application of Mueller matrix polarimetry for characterising properties of thin film with surface roughness. MATEC Web Conf. 2015, 32, 5006. [Google Scholar] [CrossRef] [Green Version]
- Luo, D.A.; Barraza, E.T.; Kudenov, M.W. Mueller matrix polarimetry on plasma sprayed thermal barrier coatings for porosity measurement. Appl. Opt. 2017, 56, 9770–9778. [Google Scholar] [CrossRef]
- Guo, W.; Song, J.; Zeng, N.; Ma, H. Mueller Matrix Imaging Optimized by Uniform Illumination. Front. Phys. 2022, 10, 931958. [Google Scholar] [CrossRef]
- Meglinskii, I.V.; Bashkatov, A.N.; Genina, E.A.; Churmakov, D.Y.; Tuchin, V.V. Study of the possibility of increasing the probing depth by the method of reflection confocal microscopy upon immersion clearing of near-surface human skin layers. Quantum Electron. 2002, 32, 875–882. [Google Scholar] [CrossRef] [Green Version]
- Fricke, D.; Denker, E.; Heratizadeh, A.; Werfel, T.; Wollweber, M.; Roth, B. Non-Contact Dermatoscope with Ultra-Bright Light Source and Liquid Lens-Based Autofocus Function. Appl. Sci. 2019, 9, 2177. [Google Scholar] [CrossRef] [Green Version]
- Meinhardt-Wollweber, M.; Heratizadeh, A.; Basu, C.; Günther, A.; Schlangen, S.; Roth, B. A non-contact remote digital der moscope to support cancer screening and diagnosis of inflammatory skin disease. Biomed. Phys. Eng. Express 2017, 3, 055005. [Google Scholar] [CrossRef]
- Varkentin, A.; Mazurenka, M.; Blumenröther, E.; Behrendt, L.; Emmert, S.; Morgner, U.; Wollweber, M.; Rahlves, M.; Roth, B. Trimodal system for in vivo skin cancer screening with combined optical coherence tomography-Raman and colocalized optoacoustic measurements. J. Biophotonics 2018, 11, e201700288. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | H | V | P | M | R | L |
| Polarization | horizontal | vertical | linear +45° | linear −45° | right circular | left circular |
| Colour channel | R | G | B |
| Polarization parameter | Retardance | Polarizance | Depolarization Power |
| Day | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|
| Pearson coefficient | −1.1469 | −1.0464 | −0.9031 | −0.4783 | −0.5967 | |
| Kurtosis | 20.6685 | 4.4356 | 4.1774 | 2.9353 | 3.3881 | |
| Pearson coefficient | 0.9390 | 0.6858 | 0.6586 | 0.6572 | 0.5807 | |
| Kurtosis | 14.0680 | 5.4770 | 8.0739 | 4.7647 | 4.2798 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jütte, L.; Roth, B. Mueller Matrix Microscopy for In Vivo Scar Tissue Diagnostics and Treatment Evaluation. Sensors 2022, 22, 9349. https://doi.org/10.3390/s22239349
Jütte L, Roth B. Mueller Matrix Microscopy for In Vivo Scar Tissue Diagnostics and Treatment Evaluation. Sensors. 2022; 22(23):9349. https://doi.org/10.3390/s22239349
Chicago/Turabian StyleJütte, Lennart, and Bernhard Roth. 2022. "Mueller Matrix Microscopy for In Vivo Scar Tissue Diagnostics and Treatment Evaluation" Sensors 22, no. 23: 9349. https://doi.org/10.3390/s22239349