
Suitability of a Low-Cost Wearable Sensor to Assess Turning in Healthy Adults
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Demographic and Clinical Assessments
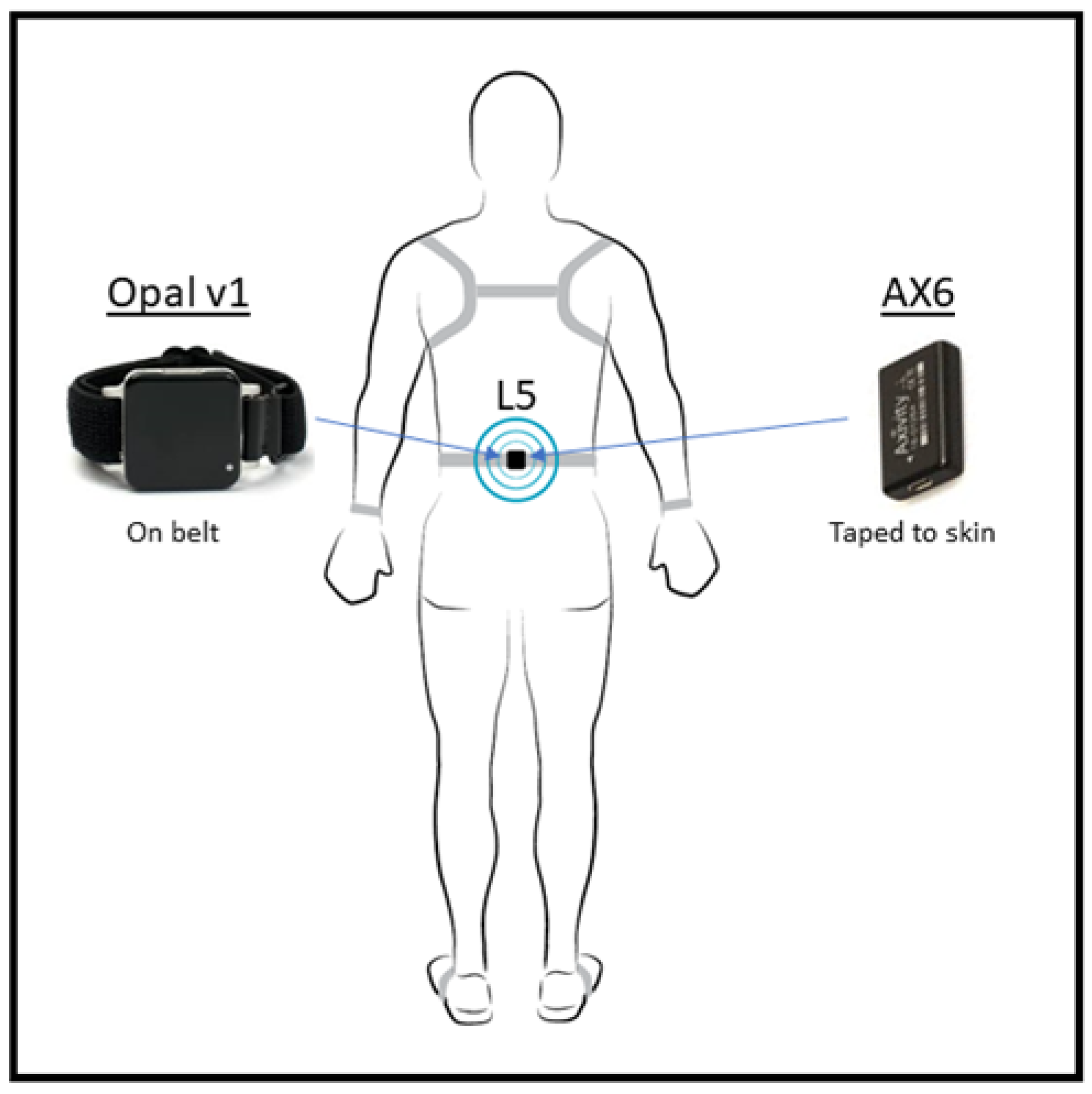
2.3. Equipment
2.4. Gait Assessment
- Task 1: The turns course included six turns per lap (Figure 2), the turns were comprised of two turns at 45°, 90° and 135° [24,25]. Each participant was asked to perform eight laps of the course at a pace comfortable to them (48 turns in total), participants were instructed to follow the tape markers of the course.
- Task 2: The second assessment involved participants walking at a comfortable speed back and forth between two lines set 5m apart. Participants were instructed to perform the 180° turn ‘as smoothly as possible’ at either end.
- Task 3: The final assessment consisted of the participant turning 360° clockwise and then counter-clockwise back and forth for two minutes in a fixed position. Participants were again asked to complete the turns as smoothly as possible.
2.5. Data Processing
2.6. Data Analysis
3. Results
3.1. Participant Demongraphics
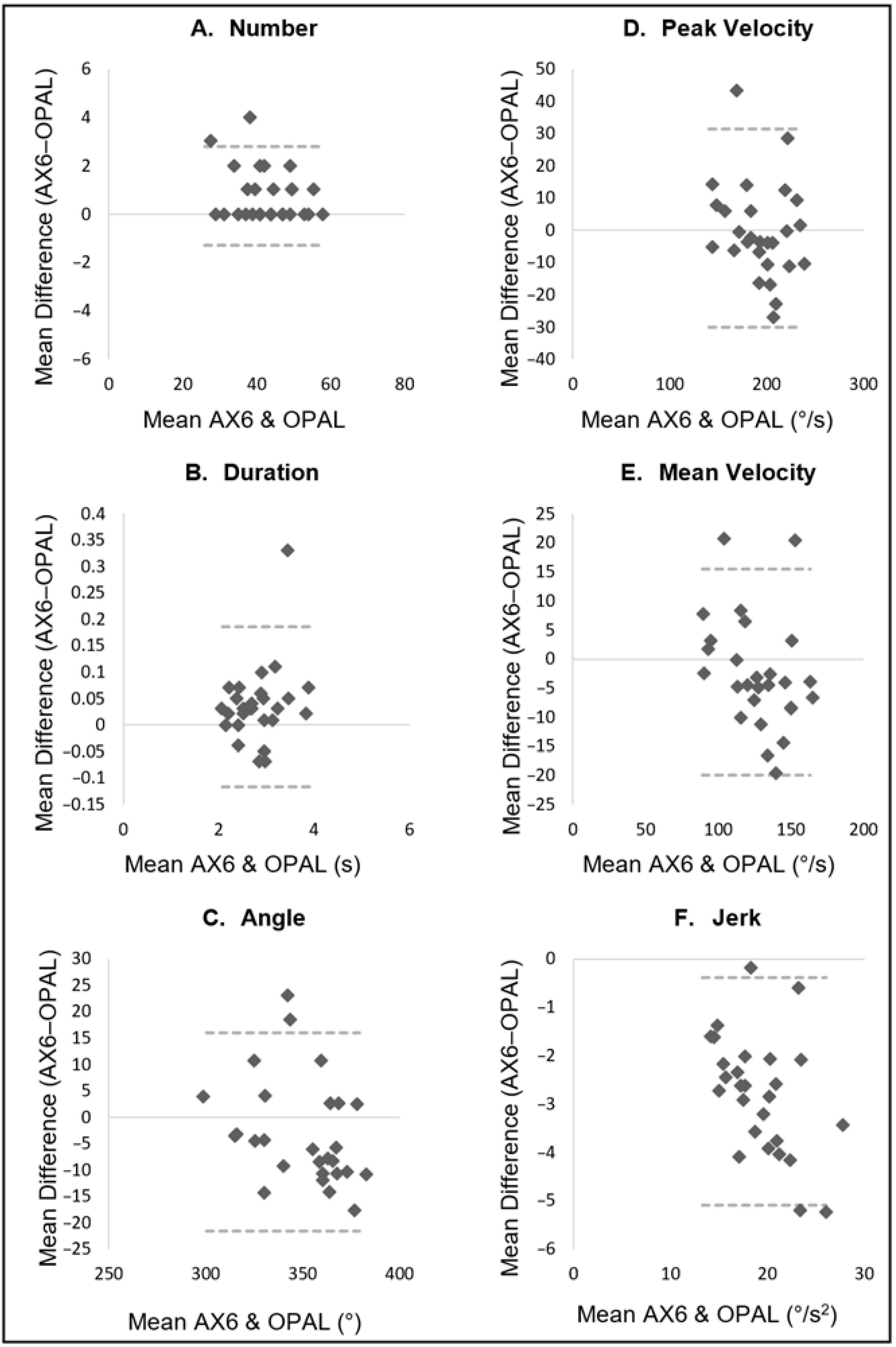
3.2. Turning Validation
3.3. Task 1—Turning Course
3.4. Task 2—Two-Minute Walk
3.5. Task 3—Turning in Place
4. Discussion
4.1. Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Glaister, B.C.; Bernatz, G.C.; Klute, G.K.; Orendurff, M.S. Video task analysis of turning during activities of daily living. Gait Posture 2007, 25, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Stuart, S.; Parrington, L.; Martini, D.N.; Kreter, N.; Chesnutt, J.C.; Fino, P.C.; King, L.A. Analysis of Free-Living Mobility in People with Mild Traumatic Brain Injury and Healthy Controls: Quality over Quantity. J. Neurotrauma 2020, 37, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Bertoli, M.; Della Croce, U.; Cereatti, A.; Mancini, M. Objective measures to investigate turning impairments and freezing of gait in people with Parkinson’s disease. Gait Posture 2019, 74, 187–193. [Google Scholar] [CrossRef]
- Crenna, P.; Carpinella, I.; Rabuffetti, M.; Calabrese, E.; Mazzoleni, P.; Nemni, R.; Ferrarin, M. The association between impaired turning and normal straight walking in Parkinson’s disease. Gait Posture 2007, 26, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Mellone, S.; Mancini, M.; King, L.A.; Horak, F.B.; Chiari, L. The quality of turning in Parkinson’s disease: A compensatory strategy to prevent postural instability? J. Neuroeng. Rehabil. 2016, 13, 39. [Google Scholar] [CrossRef] [Green Version]
- Powell, D.; Stuart, S.; Godfrey, A. Sports related concussion: An emerging era in digital sports technology. NPJ Digit. Med. 2021, 4, 164. [Google Scholar] [CrossRef]
- Stack, E.; Ashburn, A. Dysfunctional turning in Parkinson’s disease. Disabil. Rehabil. 2008, 30, 1222–1229. [Google Scholar] [CrossRef]
- Ganz, D.A.; Bao, Y.; Shekelle, P.G.; Rubenstein, L.Z. Will my patient fall? JAMA 2007, 297, 77–86. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Wallace, D.; Chandler, J.M.; Duncan, P.; Rooney, E.; Fox, M.; Guralnik, J.M. Physical Performance Measures in the Clinical Setting. J. Am. Geriatr. Soc. 2003, 51, 314–322. [Google Scholar] [CrossRef] [Green Version]
- Angelini, L.; Hodgkinson, W.; Smith, C.; Dodd, J.M.; Sharrack, B.; Mazzà, C.; Paling, D. Wearable sensors can reliably quantify gait alterations associated with disability in people with progressive multiple sclerosis in a clinical setting. J. Neurol. 2020, 267, 2897–2909. [Google Scholar] [CrossRef]
- Schaafsma, J.D.; Balash, Y.; Gurevich, T.; Bartels, A.L.; Hausdorff, J.M.; Giladi, N. Characterization of freezing of gait subtypes and the response of each to levodopa in Parkinson’s disease. Eur. J. Neurol. 2003, 10, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robles-García, V.; Corral-Bergantiños, Y.; Espinosa, N.; Jácome, M.A.; García-Sancho, C.; Cudeiro, J.; Arias, P. Spatiotemporal Gait Patterns During Overt and Covert Evaluation in Patients With Parkinson’s Disease and Healthy Subjects: Is There a Hawthorne Effect? J. Appl. Biomech. 2015, 31, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Carse, B.; Meadows, B.; Bowers, R.; Rowe, P. Affordable clinical gait analysis: An assessment of the marker tracking accuracy of a new low-cost optical 3D motion analysis system. Physiotherapy 2013, 99, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Cappozzo, A.; Della Croce, U.; Leardini, A.; Chiari, L. Human movement analysis using stereopho-to-grammetry. Part 1: Theoretical background. Gait Posture 2005, 21, 186–196. [Google Scholar] [PubMed]
- Kobsar, D.; Charlton, J.M.; Tse, C.T.F.; Esculier, J.-F.; Graffos, A.; Krowchuk, N.M.; Thatcher, D.; Hunt, M.A. Validity and reliability of wearable inertial sensors in healthy adult walking: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2020, 17, 62. [Google Scholar] [CrossRef]
- Simon, S.R. Quantification of human motion: Gait analysis—Benefits and limitations to its application to clinical problems. J. Biomech. 2004, 37, 1869–1880. [Google Scholar] [CrossRef]
- Chen, S.; Lach, J.; Lo, B.; Yang, G.-Z. Toward Pervasive Gait Analysis With Wearable Sensors: A Systematic Review. IEEE J. Biomed. Health Inform. 2016, 20, 1521–1537. [Google Scholar] [CrossRef]
- Reid, S.; Held, J.M.; Lawrence, S. Reliability and Validity of the Shaw Gait Assessment Tool for Temporospatial Gait Assessment in People With Hemiparesis. Arch. Phys. Med. Rehabil. 2011, 92, 1060–1065. [Google Scholar] [CrossRef]
- Brodie, M.A.D.; Coppens, M.; Lord, S.R.; Lovell, N.; Gschwind, Y.J.; Redmond, S.J.; Del Rosario, M.; Wang, K.; Sturnieks, D.L.; Persiani, M.; et al. Wearable pendant device monitoring using new wavelet-based methods shows daily life and laboratory gaits are different. Med. Biol. Eng. Comput. 2016, 54, 663–674. [Google Scholar] [CrossRef]
- Tamburini, P.; Storm, F.; Buckley, C.; Bisi, M.C.; Stagni, R.; Mazzà, C. Moving from laboratory to real life conditions: Influence on the assessment of variability and stability of gait. Gait Posture 2018, 59, 248–252. [Google Scholar] [CrossRef]
- Mancini, M.; El-Gohary, M.; Pearson, S.; McNames, J.; Schlueter, H.; Nutt, J.G.; King, L.A.; Horak, F.B. Continuous monitoring of turning in Parkinson’s disease: Rehabilitation potential. NeuroRehabilitation 2015, 37, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, A.; Herman, T.; Giladi, N.; Hausdorff, J.M. Objective Assessment of Fall Risk in Parkinson’s Disease Using a Body-Fixed Sensor Worn for 3 Days. PLoS ONE 2014, 9, e96675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Gohary, M.; Pearson, S.; McNames, J.; Mancini, M.; Horak, F.; Mellone, S.; Chiari, L. Continuous Monitoring of Turning in Patients with Movement Disability. Sensors 2013, 14, 356–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuart, S.; Parrington, L.; Martini, D.; Popa, B.; Fino, P.C.; King, L.A. Validation of a velocity-based algorithm to quantify saccades during walking and turning in mild traumatic brain injury and healthy controls. Physiol. Meas. 2019, 40, 044006. [Google Scholar] [CrossRef]
- Parrington, L.; Jehu, D.A.; Fino, P.C.; Stuart, S.; Wilhelm, J.; Pettigrew, N.; Murchison, C.F.; El-Gohary, M.; Vanderwalker, J.; Pearson, S.; et al. The Sensor Technology and Rehabilitative Timing (START) Protocol: A Randomized Controlled Trial for the Rehabilitation of Mild Traumatic Brain Injury. Phys. Ther. 2020, 100, 687–697. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Godfrey, A.; Del Din, S.; Barry, G.; Mathers, J.C.; Rochester, L. Instrumenting gait with an accelerometer: A system and algorithm examination. Med. Eng. Phys. 2015, 37, 400–407. [Google Scholar] [CrossRef]
- Morris, R.; Stuart, S.; McBarron, G.; Fino, P.C.; Mancini, M.; Curtze, C. Validity of Mobility Lab (version 2) for gait assessment in young adults, older adults and Parkinson’s disease. Physiol. Meas. 2019, 40, 095003. [Google Scholar] [CrossRef]
- Powell, D.; Nouredanesh, M.; Stuart, S.; Godfrey, A. Investigating the AX6 inertial-based wearable for instrumented physical capability assessment of young adults in a low-resource setting. Smart Health 2021, 22, 100220. [Google Scholar] [CrossRef]
- Del Din, S.; Hickey, A.; Hurwitz, N.; Mathers, J.C.; Rochester, L.; Godfrey, A. Measuring gait with an accelerometer-based wearable: Influence of device location, testing protocol and age. Physiol. Meas. 2016, 37, 1785–1797. [Google Scholar] [CrossRef]
- Yang, C.C.; Hsu, Y.L. A review of accelerometry-based wearable motion detectors for physical activity monitoring. Sensors 2010, 10, 7772–7788. [Google Scholar] [CrossRef] [PubMed]
- Rehman, R.Z.U.; Klocke, P.; Hryniv, S.; Galna, B.; Rochester, L.; Del Din, S.; Alcock, L. Turning Detection During Gait: Algorithm Validation and Influence of Sensor Location and Turning Characteristics in the Classification of Parkinson’s Disease. Sensors 2020, 20, 5377. [Google Scholar] [CrossRef] [PubMed]
- Pham, M.H.; Elshehabi, M.; Haertner, L.; Heger, T.; Hobert, M.A.; Faber, G.S.; Salkovic, D.; Ferreira, J.J.; Berg, D.; Sanchez-Ferro, Á.; et al. Algorithm for Turning Detection and Analysis Validated under Home-Like Conditions in Patients with Parkinson’s Disease and Older Adults using a 6 Degree-of-Freedom Inertial Measurement Unit at the Lower Back. Front. Neurol. 2017, 8, 135. [Google Scholar] [CrossRef]
- Mancini, M.; Shah, V.V.; Stuart, S.; Curtze, C.; Horak, F.B.; Safarpour, D.; Nutt, J.G. Measuring freezing of gait during daily-life: An open-source, wearable sensors approach. J. Neuroeng. Rehabil. 2021, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: A systematic review and meta- analysis. BMC Geriatr. 2014, 14, 14. [Google Scholar] [CrossRef] [Green Version]
- Kleiner AF, R.; Pacifici, I.; Vagnini, A.; Camerota, F.; Celletti, C.; Stocchi, F.; De Pandis, M.F.; Galli, M. Timed Up and Go evaluation with wearable devices: Validation in Parkinson’s disease. J. Bodyw. Mov. Ther. 2018, 22, 390–395. [Google Scholar] [CrossRef]
- Powell, D.; Godfrey, A.; Parrington, L.; Campbell, K.R.; King, L.A.; Stuart, S. Free-living Turning Rather Than Gait Differentiates People with Chronic Mild Traumatic Brain Injury from Controls. J. Neuroeng. Rehabil. 2022, 19, 49–56. [Google Scholar] [CrossRef]
- Shah, V.V.; McNames, J.; Mancini, M.; Carlson-Kuhta, P.; Spain, R.I.; Nutt, J.G.; El-Gohary, M.; Curtze, C.; Horak, F.B. Quantity and quality of gait and turning in people with multiple sclerosis, Parkinson’s disease and matched controls during daily living. J. Neurol. 2020, 267, 1188–1196. [Google Scholar] [CrossRef]
- Del Din, S.; Galna, B.; Godfrey, A.; Bekkers EM, J.; Pelosin, E.; Nieuwhof, F.; Mirelman, A.; Hausdorff, J.M.; Rochester, L. Analysis of Free-Living Gait in Older Adults With and Without Parkinson’s Disease and With and Without a History of Falls: Identifying Generic and Disease-Specific Characteristics. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 500–506. [Google Scholar] [CrossRef]
- Mancini, M.; Schlueter, H.; El-Gohary, M.; Mattek, N.; Duncan, C.; Kaye, J.; Horak, F.B. Continuous Monitoring of Turning Mobility and Its Association to Falls and Cognitive Function: A Pilot Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1102–1108. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male (n = 18) | Female (n = 12) | |
|---|---|---|
| Age (years) | 23.6 ± 5.4 | 23.7 ± 4.0 |
| Height (cm) | 175.2 ± 9.5 | 174.8 ± 6.3 |
| Weight (kg) | 77.3 ± 12.5 | 76 ± 12.1 |
| Task | Turn Characteristics | AX6 (n = 30) | OPAL (n = 30) | Agreement | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean Difference | ICC | Lower Bound | Upper Bound | p | LoA (%) | LoA95% | Pearson r | Pearson p | ||
| Turning Course | Number | 43.33 (8.98) | 42.37 (10.27) | −0.97 | 0.873 | 0.751 | 0.937 | <0.285 | 22.2 | 9.526 | 0.881 | <0.001 |
| Duration (s) | 1.55 (0.21) | 1.61 (0.31) | 0.07 | 0.576 | 0.277 | 0.773 | <0.156 | 30.6 | 0.484 | 0.618 | <0.001 | |
| Angle (°) | 110.03 (20.82) | 114.47 (26.00) | 4.44 | 0.722 | 0.493 | 0.857 | <0.177 | 30.7 | 34.427 | 0.740 | <0.001 | |
| Peak Velocity (°/s) | 123.01 (19.78) | 123.00 (21.43) | −0.01 | 0.833 | 0.679 | 0.917 | <0.997 | 19.0 | 23.330 | 0.836 | <0.001 | |
| Mean Velocity (°/s) | 56.38 (6.85) | 55.23 (6.89) | −1.15 | 0.716 | 0.484 | 0.854 | <0.231 | 18.2 | 10.139 | 0.716 | <0.001 | |
| Jerk | 15.79 (3.86) | 18.80 (5.25) | 3.00 | 0.872 | 0.748 | 0.937 | <0.01 | 26.5 | 4.575 | 0.914 | <0.001 | |
| 2MW | Number | 23.03 (3.95) | 21.90 (2.98) | −1.13 | 0.632 | 0.356 | 0.806 | <0.048 | 26.2 | 5.885 | 0.657 | <0.001 |
| Duration (s) | 1.98 (0.30) | 1.98 (0.30) | 0.00 | 0.840 | 0.691 | 0.921 | <0.906 | 16.8 | 0.332 | 0.840 | <0.001 | |
| Angle (°) | 172.10 (11.49) | 172.47 (11.20) | 0.37 | 0.683 | 0.432 | 0.835 | <0.823 | 10.3 | 17.725 | 0.683 | <0.001 | |
| Peak Velocity (°/s) | 178.79 (25.33) | 181.63 (30.03) | 2.84 | 0.842 | 0.694 | 0.921 | <0.329 | 17.0 | 30.638 | 0.854 | <0.001 | |
| Mean Velocity (°/s) | 80.71 (10.69) | 83.67 (11.97) | 2.96 | 0.824 | 0.662 | 0.912 | <0.022 | 16.1 | 13.210 | 0.829 | <0.001 | |
| Jerk | 17.21 (3.23) | 19.84 (3.84) | 2.63 | 0.888 | 0.778 | 0.945 | <0.01 | 17.8 | 3.292 | 0.901 | <0.001 | |
| Turning in place | Number | 42.10 (8.31) | 41.33 (8.51) | −0.77 | 0.992 | 0.984 | 0.996 | <0.01 | 4.9 | 2.038 | 0.993 | <0.001 |
| Duration | 2.91 (0.54) | 2.88 (0.52) | −0.03 | 0.989 | 0.978 | 0.995 | <0.02 | 5.2 | 0.152 | 0.990 | <0.001 | |
| Angle | 349.94 (20.60) | 352.72 (23.51) | 2.78 | 0.906 | 0.811 | 0.954 | <0.124 | 5.4 | 18.833 | 0.913 | <0.001 | |
| Peak Velocity (°/s) | 190.62 (27.41) | 189.84 (30.85) | −0.77 | 0.855 | 0.718 | 0.928 | <0.790 | 16.2 | 30.779 | 0.861 | <0.001 | |
| Mean Velocity (°/s) | 123.57 (21.43) | 125.77 (24.29) | 2.20 | 0.922 | 0.843 | 0.962 | <0.193 | 14.2 | 17.750 | 0.929 | <0.001 | |
| Jerk | 17.84 (3.33) | 20.57 (3.80) | 2.73 | 0.944 | 0.885 | 0.973 | <0.01 | 12.2 | 2.352 | 0.952 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mason, R.; Byerley, J.; Baker, A.; Powell, D.; Pearson, L.T.; Barry, G.; Godfrey, A.; Mancini, M.; Stuart, S.; Morris, R. Suitability of a Low-Cost Wearable Sensor to Assess Turning in Healthy Adults. Sensors 2022, 22, 9322. https://doi.org/10.3390/s22239322
Mason R, Byerley J, Baker A, Powell D, Pearson LT, Barry G, Godfrey A, Mancini M, Stuart S, Morris R. Suitability of a Low-Cost Wearable Sensor to Assess Turning in Healthy Adults. Sensors. 2022; 22(23):9322. https://doi.org/10.3390/s22239322
Chicago/Turabian StyleMason, Rachel, Joe Byerley, Andrea Baker, Dylan Powell, Liam T. Pearson, Gill Barry, Alan Godfrey, Martina Mancini, Samuel Stuart, and Rosie Morris. 2022. "Suitability of a Low-Cost Wearable Sensor to Assess Turning in Healthy Adults" Sensors 22, no. 23: 9322. https://doi.org/10.3390/s22239322