
Deep Learning-Based Computer-Aided Diagnosis (CAD): Applications for Medical Image Datasets


Abstract
:1. Introduction
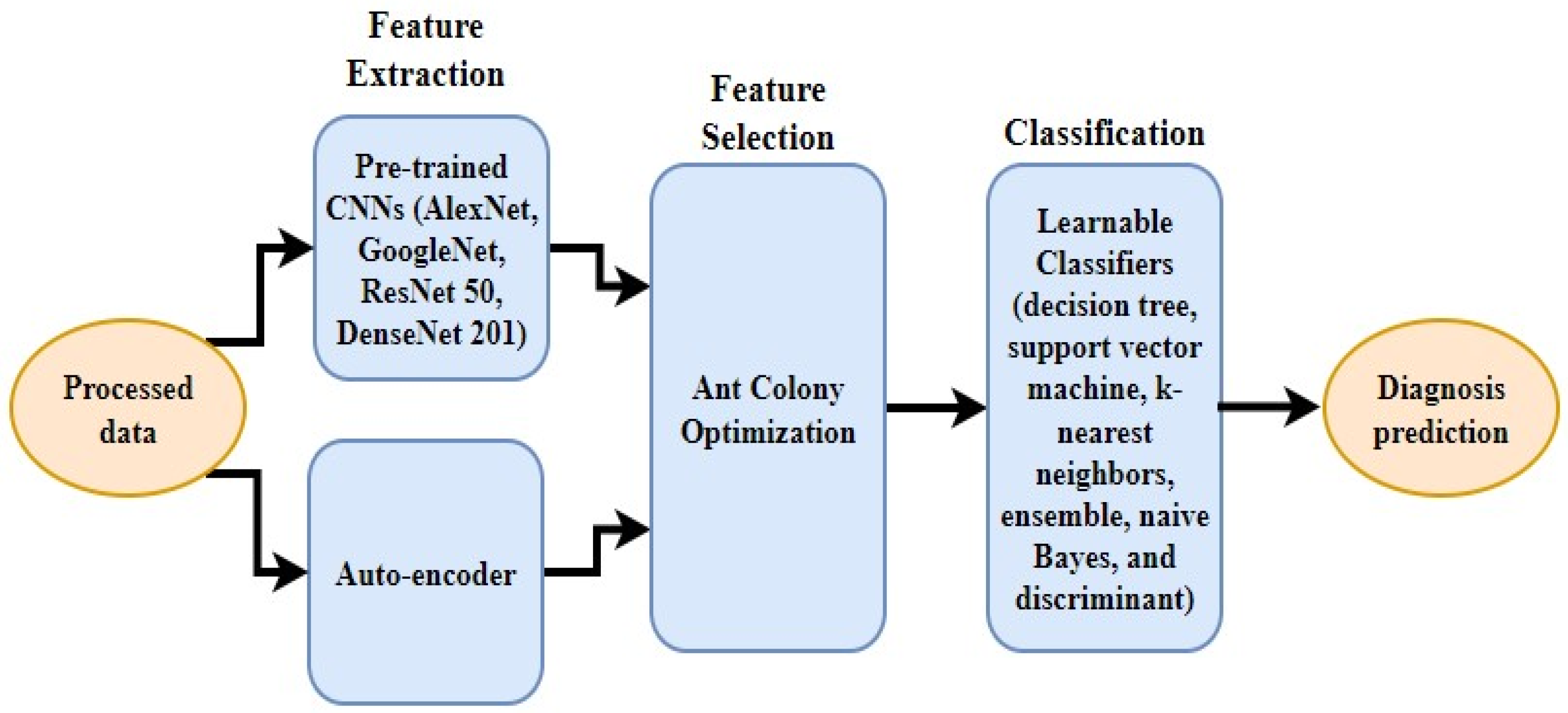
- The extraction of features from the image dataset using auto-encoder and well-known pre-trained CNNs, e.g., ResNet and AlexNet;
- The selection of the most notable features using ACO to enhance accuracy;
- A generic framework is proposed that can work on multiple datasets, such as MRIs and X-rays;
- The evaluation of the proposed classification model against the current baseline diagnostic models.
2. Related Works
2.1. Segmentation and Pre-Processing
2.2. Feature Extraction and Selection
2.3. Classification
3. Material and Methods
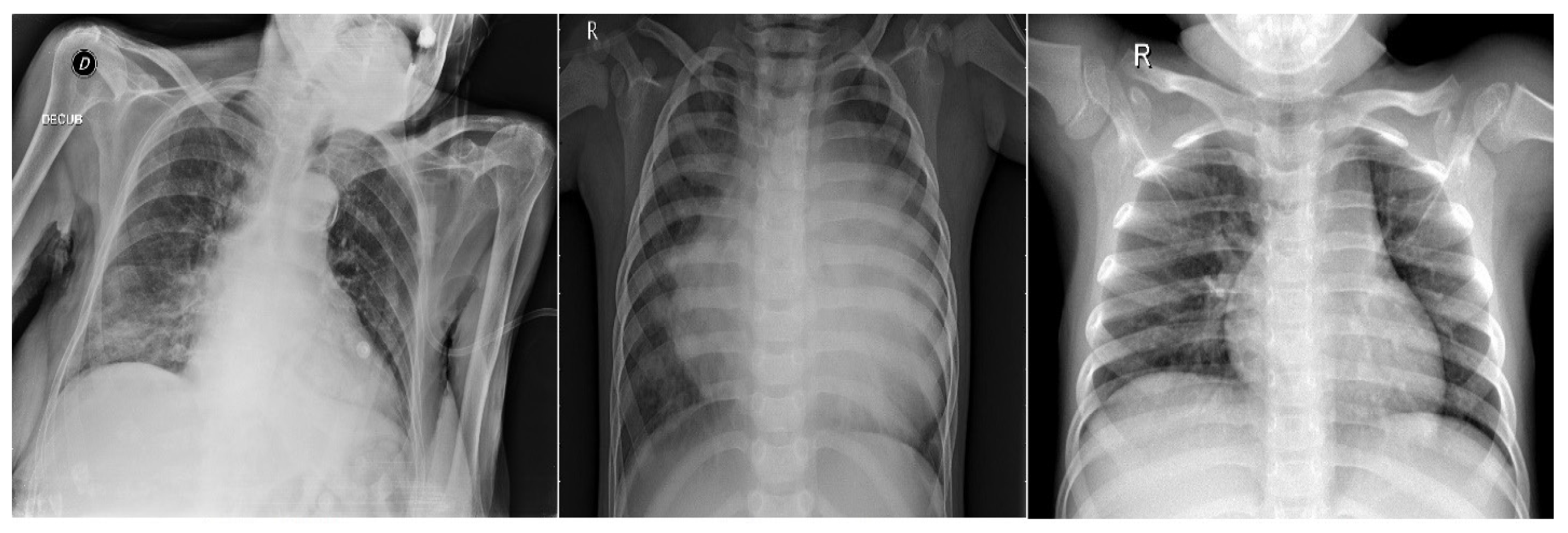
3.1. COVID-19 Dataset
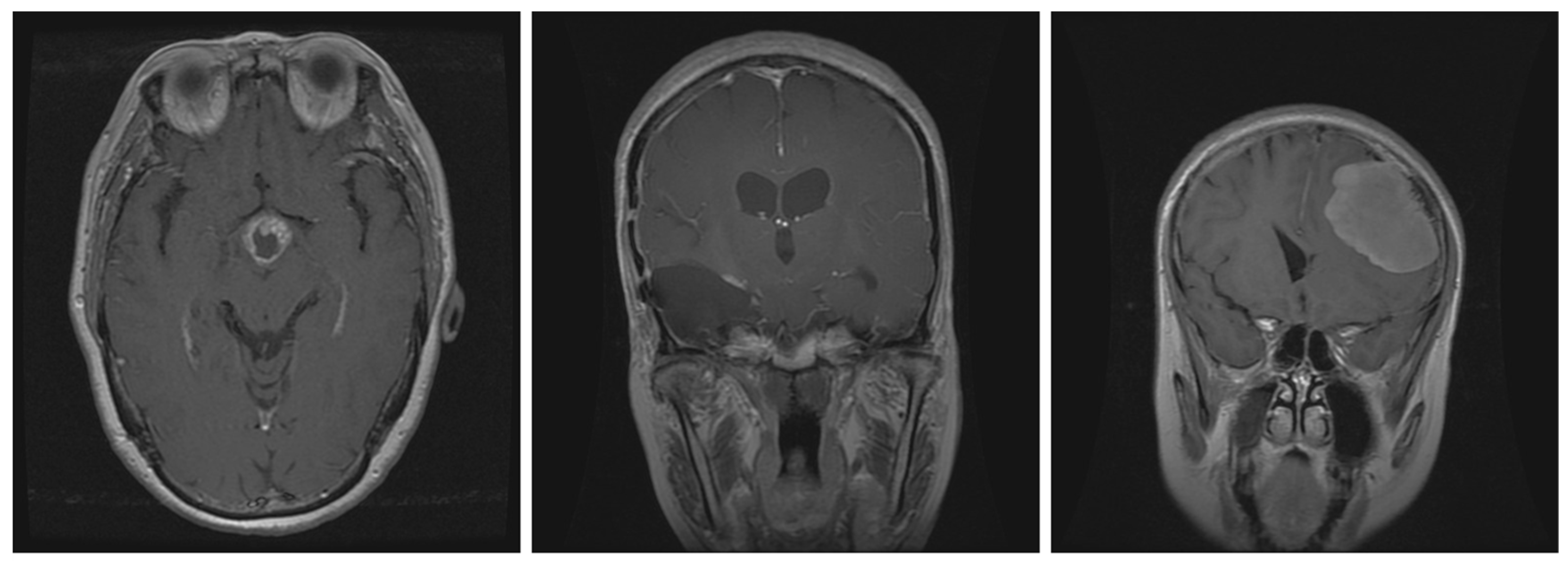
3.2. Brain Tumor Dataset
3.3. Deep Learning Techniques
3.3.1. Convolutional Neural Network
- Alexnet (4096) features.
- Googlenet (1000) features.
- Resnet 50 (2048) features.
- Densenet 201 (1920) features.
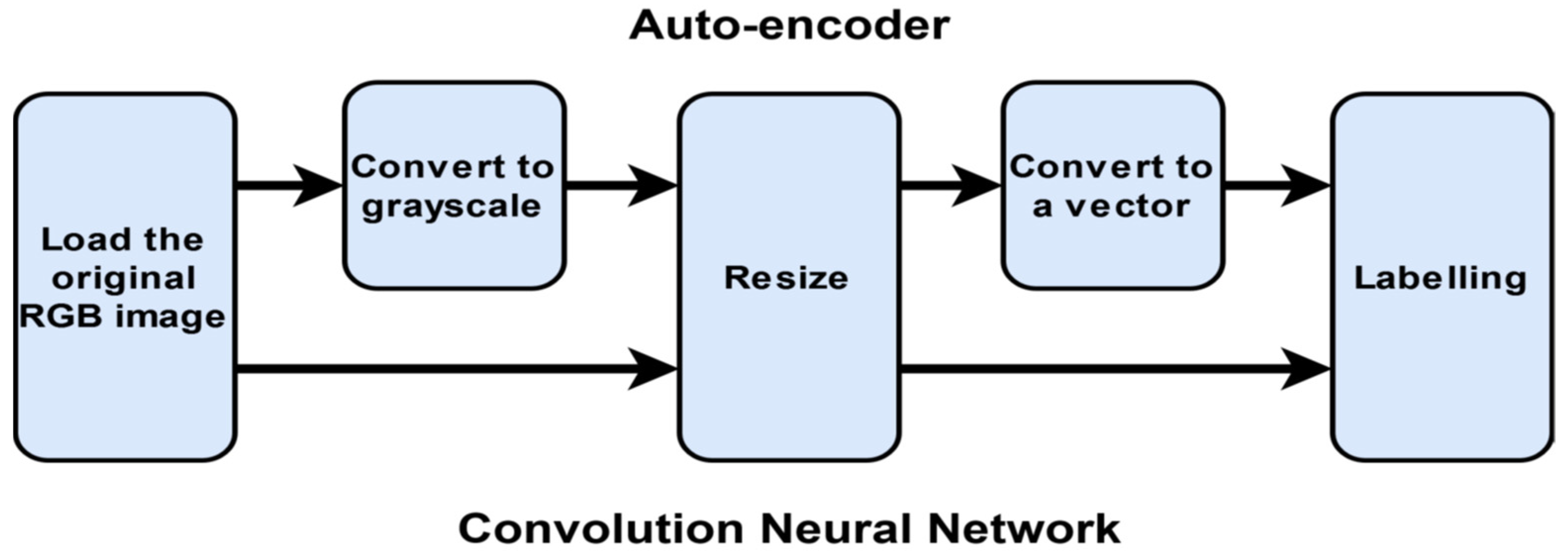
3.3.2. Auto-Encoders
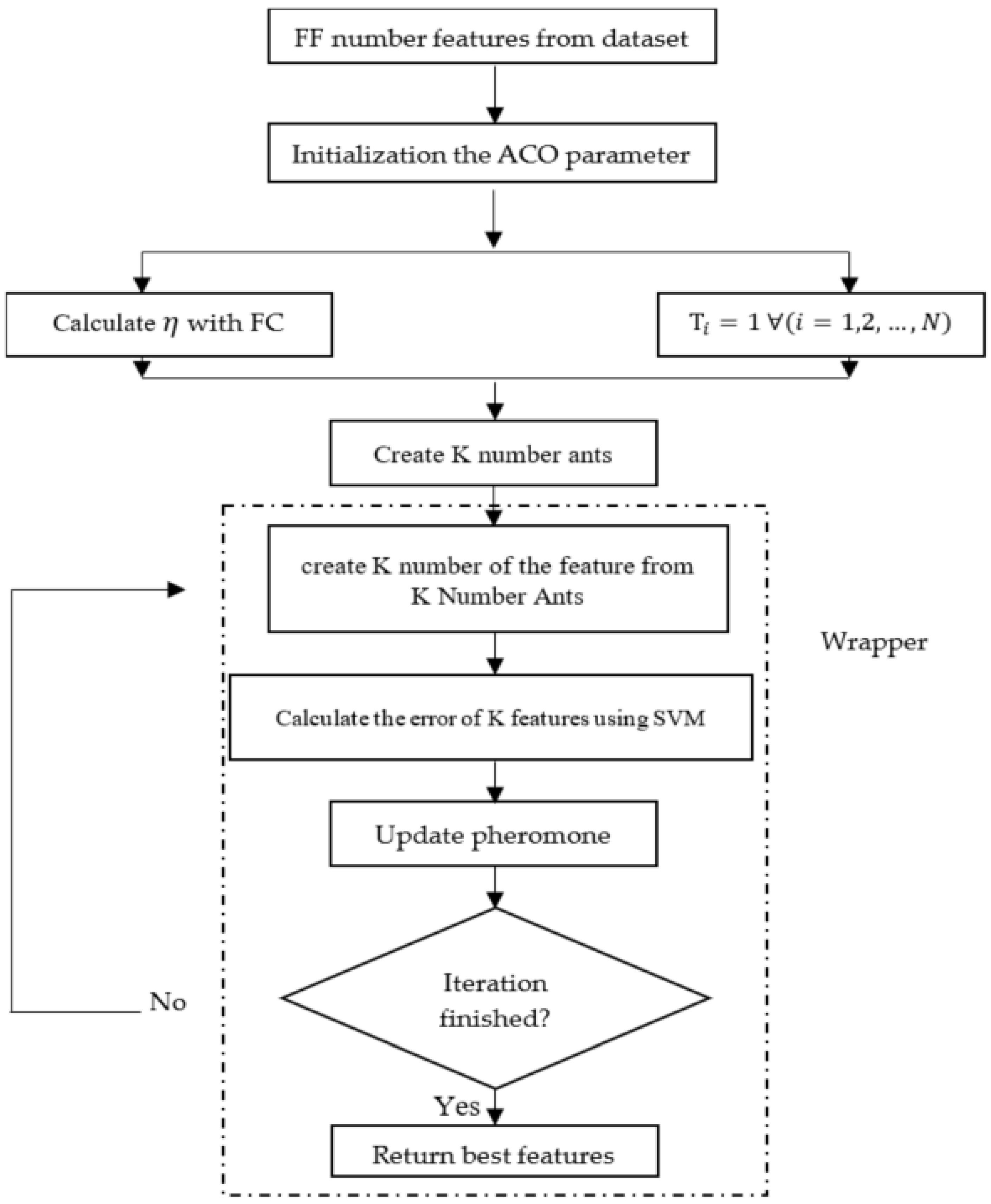
3.4. Ant Colony Optimization Algorithm for Feature Selection
- First, you have to turn the problem into a graph, including nodes and edges.
- See distance nodes () are raised and specified.
- A possible solution is created according to the problem.
- The pheromone update rule is used to determine the effective edges in achieving the best answer.
- The probabilistic transition rule is used to find the next node [52].
3.4.1. Working Method of the Proposed Model
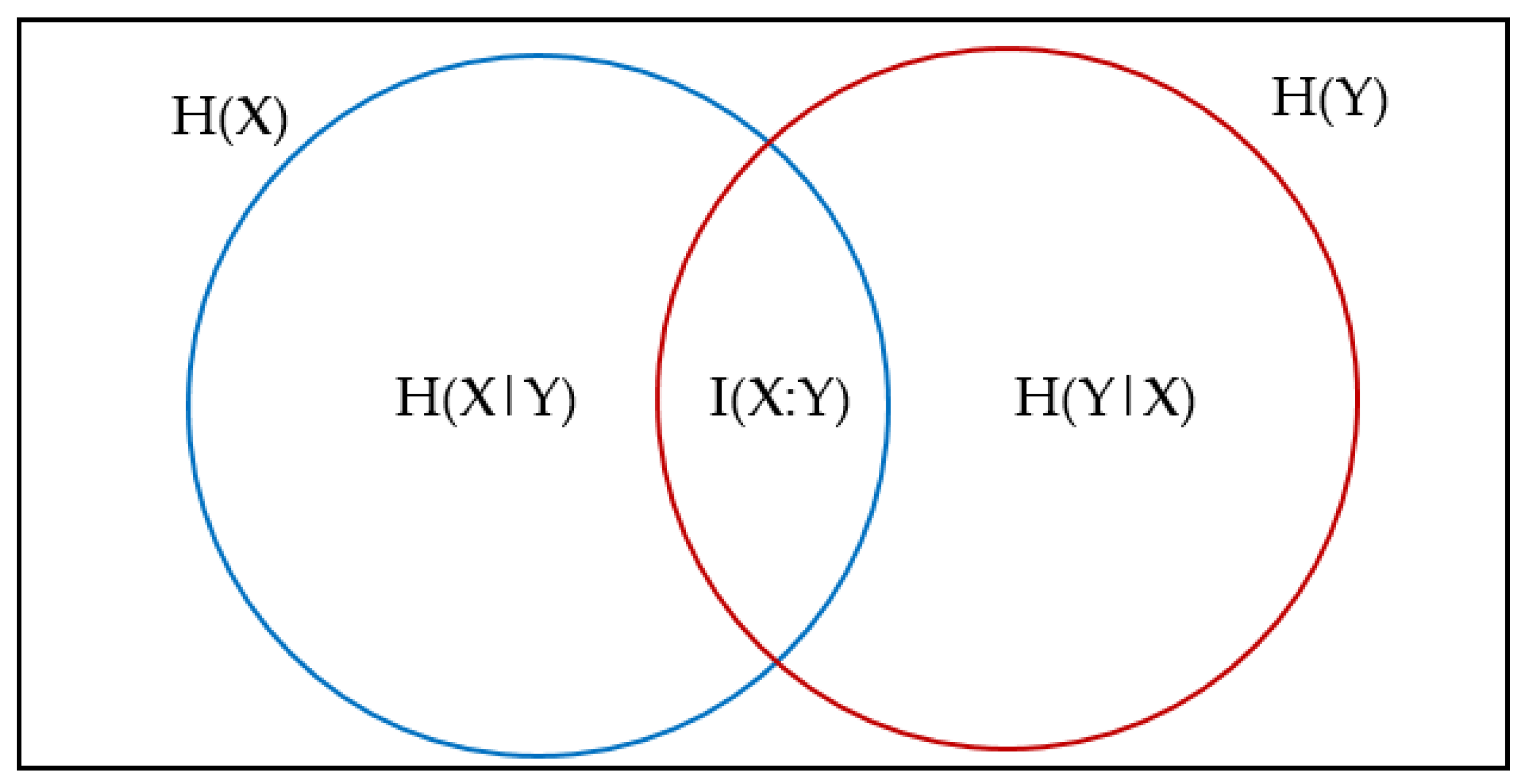
3.4.2. Criteria for Distance and Similarity of Features
3.5. Dataset Pre-Processing
3.6. Overall Architecture of the Proposed Framework
4. Experiments and Results Analysis
4.1. Evaluation Metrics
4.2. Classification Using Learnable Classifiers
4.2.1. Feature Extraction and Feature Selection Using Auto-Encoder and ACO
4.2.2. Feature Extraction-Selection Using Pre-Trained CNNs and ACO
4.3. Performance Comparison with Existing Methods
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Briganti, G.; Le Moine, O. Artificial Intelligence in Medicine: Today and Tomorrow. Front. Med. 2020, 7, 27. [Google Scholar] [CrossRef] [PubMed]
- Lodwick, G.S. Computer-aided diagnosis in radiology: A research plan. Investig. Radiol. 1966, 1, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Giger, M.L.; Chan, H.; Boone, J. Anniversary paper: History and status of CAD and quantitative image analysis: The role of medical physics and AAPM. Med. Phys. 2008, 35, 5799–5820. [Google Scholar] [CrossRef]
- Czajkowska, J.; Borak, M. Computer-Aided Diagnosis Methods for High-Frequency Ultrasound Data Analysis: A Review. Sensors 2022, 22, 8326. [Google Scholar] [CrossRef]
- Meyers, P.H.; Nice, C.M., Jr.; Becker, H.C.; Nettleton, W.J., Jr.; Sweeney, J.W.; Meckstroth, G.R. Automated computer analysis of radiographic images. Radiology 1964, 83, 1029–1034. [Google Scholar] [CrossRef] [PubMed]
- Engle, R.L., Jr. Attempts to use computers as diagnostic aids in medical decision making: A thirty-year experience. Perspect. Biol. Med. 1992, 35, 207–219. [Google Scholar] [CrossRef]
- Doi, K. Computer-aided diagnosis in medical imaging: Historical review, current status and future potential. Comput. Med. Imaging Graph. 2007, 31, 198–211. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.; Hadjiiski, L.M.; Samala, R.K. Computer-aided diagnosis in the era of deep learning. Med. Phys. 2020, 47, e218–e227. [Google Scholar] [CrossRef]
- Li, D.; Fu, Z.; Xu, J. Stacked-autoencoder-based model for COVID-19 diagnosis on CT images. Appl. Intell. 2021, 51, 2805–2817. [Google Scholar] [CrossRef]
- Paganin, F.; Seneterre, E.; Chanez, P.; Daures, J.P.; Bruel, J.M.; Michel, F.B.; Bousquet, J. Computed tomography of the lungs in asthma: Influence of disease severity and etiology. Am. J. Respir. Crit. Care Med. 1996, 153, 110–114. [Google Scholar] [CrossRef]
- Warrick, J.H.; Bhalla, M.; Schabel, S.I.; Silver, R.M. High resolution computed tomography in early scleroderma lung disease. J. Rheumatol. 1991, 18, 1520–1528. [Google Scholar] [PubMed]
- Na’am, J.; Harlan, J.; Nercahyo, G.W.; Arlis, S.; Rani, L.N. Detection of Infiltrate on Infant Chest X-ray. Telkomnika 2017, 15, 1943–1951. [Google Scholar] [CrossRef]
- Paul, J.S.; Plassard, A.J.; Landman, B.A.; Fabbri, D. Deep learning for brain tumor classification. In Proceedings of the Medical Imaging 2017: Biomedical Applications in Molecular, Structural, and Functional Imaging, Orlando, FL, USA, 12–14 February 2017; Volume 10137, p. 1013710. [Google Scholar]
- Black, P.M. Brain tumors. N. Engl. J. Med. 1991, 324, 1555–1564. [Google Scholar] [CrossRef] [PubMed]
- Toğaçar, M.; Cömert, Z.; Ergen, B. Classification of brain MRI using hyper column technique with convolutional neural network and feature selection method. Expert Syst. Appl. 2020, 149, 113274. [Google Scholar] [CrossRef]
- Morais, A.; Egger, J.; Alves, V. Automated computer-aided design of cranial implants using a deep volumetric convolutional denoising autoencoder. In Proceedings of the 2019 World Conference on Information Systems and Technologies, Cairo, Egypt, 24–26 March 2019; pp. 151–160. [Google Scholar]
- Ali, N.A.; Syafeeza, A.R.; Geok, L.J.; Wong, Y.C.; Hamid, N.A.; Jaafar, A.S. Design of Automated Computer-Aided Classification of Brain Tumor Using Deep Learning. In Intelligent and Interactive Computing; Springer: Berlin/Heidelberg, Germany, 2019; pp. 285–291. [Google Scholar]
- Yanase, J.; Triantaphyllou, E. The seven key challenges for the future of computer-aided diagnosis in medicine. Int. J. Med. Inform. 2019, 129, 413–422. [Google Scholar] [CrossRef]
- Sonka, M.; Hlavac, V.; Boyle, R. Image Processing, Analysis, and Machine Vision; Cengage Learning: Boston, MA, USA, 2014; ISBN 1285981448. [Google Scholar]
- Suetens, P. Fundamentals of Medical Imaging; Cambridge University Press: Cambridge, UK, 2017; ISBN 1107159784. [Google Scholar]
- Jeyavathana, R.B.; Balasubramanian, R.; Pandian, A.A. A survey: Analysis on pre-processing and segmentation techniques for medical images. Int. J. Res. Sci. Innov. 2016, 3, 113–120. [Google Scholar]
- Deepak, S.; Ameer, P.M. Brain tumor classification using deep CNN features via transfer learning. Comput. Biol. Med. 2019, 111, 103345. [Google Scholar] [CrossRef]
- Sachdeva, J.; Kumar, V.; Gupta, I.; Khandelwal, N.; Ahuja, C.K. Segmentation, feature extraction, and multiclass brain tumor classification. J. Digit. Imaging 2013, 26, 1141–1150. [Google Scholar] [CrossRef] [Green Version]
- Ismael, M.R.; Abdel-Qader, I. Brain tumor classification via statistical features and back-propagation neural network. In Proceedings of the 2018 IEEE International Conference on Electro/Information Technology (EIT), Rochester, MI, USA, 3–5 May 2018; pp. 252–257. [Google Scholar]
- Qin, W.; Zhao, M.; Mei, S.; Cattani, P.; Guercio, V.; Villecco, F. Realization of Single Image Super-Resolution Reconstruction Based on Wavelet Transform and Coupled Dictionary. In Proceedings of the International Conference “New Technologies, Development and Applications”, Sarajevo, Bosnia and Herzegovina, 23–25 June 2022; pp. 449–456. [Google Scholar]
- Jogin, M.; Madhulika, M.S.; Divya, G.D.; Meghana, R.K.; Apoorva, S. Feature extraction using convolution neural networks (CNN) and deep learning. In Proceedings of the 2018 3rd IEEE International Conference on Recent Trends in Electronics, Information & Communication Technology (RTEICT), Bangalore, India, 18–19 May 2018; pp. 2319–2323. [Google Scholar]
- Bar, Y.; Diamant, I.; Wolf, L.; Lieberman, S.; Konen, E.; Greenspan, H. Chest pathology identification using deep feature selection with non-medical training. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2018, 6, 259–263. [Google Scholar] [CrossRef]
- Ahmed, K.B.; Hall, L.O.; Goldgof, D.B.; Liu, R.; Gatenby, R.A. Fine-tuning convolutional deep features for MRI based brain tumor classification. In Proceedings of the Medical Imaging 2017: Computer-Aided Diagnosis, Orlando, FL, USA, 13–16 February 2017; Volume 10134, p. 101342E. [Google Scholar]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. Chexnet: Radiologist-level pneumonia detection on chest x-rays with deep learning. arXiv 2017, arXiv:1711.05225. [Google Scholar]
- Widhiarso, W.; Yohannes, Y.; Prakarsah, C. Brain tumor classification using gray level co-occurrence matrix and convolutional neural network. IJEIS Indones. J. Electron. Instrum. Syst. 2018, 8, 179–190. [Google Scholar] [CrossRef]
- Sajjad, M.; Khan, S.; Muhammad, K.; Wu, W.; Ullah, A.; Baik, S.W. Multi-grade brain tumor classification using deep CNN with extensive data augmentation. J. Comput. Sci. 2019, 30, 174–182. [Google Scholar] [CrossRef]
- Mei, S.; Liu, M.; Kudreyko, A.; Cattani, P.; Baikov, D.; Villecco, F. Bendlet Transform Based Adaptive Denoising Method for Microsection Images. Entropy 2022, 24, 869. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, A.; Zahoor, M.M.; Nasrullah, R.; Fareed, A.; Cheema, A.A.; Shahrose, A.; Irfan, M.; Alqhatani, A.; Alsulami, A.A.; Zaffar, M.; et al. Computer Aided COVID-19 Diagnosis in Pandemic Era Using CNN in Chest X-ray Images. Life 2022, 12, 1709. [Google Scholar] [CrossRef] [PubMed]
- Mohai, K.; Kálózi-Szabó, C.; Jakab, Z.; Fecht, S.D.; Domonkos, M.; Botzheim, J. Development of an Adaptive Computer-Aided Soft Sensor Diagnosis System for Assessment of Executive Functions. Sensors 2022, 22, 5880. [Google Scholar] [CrossRef]
- Haitao, H.; Cattani, P.; Guercio, V.; Villecco, F. Shearlet Transform and the Application in Image Processing. In Proceedings of the International Conference “New Technologies, Development and Applications”, Sarajevo, Bosnia and Herzegovina, 23–25 June 2022; pp. 464–470. [Google Scholar]
- Gopalakrishnan, K.; Khaitan, S.K.; Choudhary, A.; Agrawal, A. Deep convolutional neural networks with transfer learning for computer vision-based data-driven pavement distress detection. Constr. Build. Mater. 2017, 157, 322–330. [Google Scholar] [CrossRef]
- Wan, S.; Liang, Y.; Zhang, Y. Deep convolutional neural networks for diabetic retinopathy detection by image classification. Comput. Electr. Eng. 2018, 72, 274–282. [Google Scholar] [CrossRef]
- He, T.; Zhang, Z.; Zhang, H.; Zhang, Z.; Xie, J.; Li, M. Bag of tricks for image classification with convolutional neural networks. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 15–20 June 2019; pp. 558–567. [Google Scholar]
- Yadav, S.S.; Jadhav, S.M. Deep convolutional neural network based medical image classification for disease diagnosis. J. Big Data 2019, 6, 113. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Lin, Z.Q.; Wong, A. COVID-Net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci. Rep. 2020, 10, 19549. [Google Scholar] [CrossRef]
- Li, X.; Zhu, D. Covid-xpert: An ai powered population screening of covid-19 cases using chest radiography images. arXiv PPR346252. 2020. Available online: https://europepmc.org/article/ppr/ppr346252 (accessed on 22 October 2022).
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Acharya, U.R. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput. Biol. Med. 2020, 121, 103792. [Google Scholar] [CrossRef] [PubMed]
- Ardakani, A.A.; Kanafi, A.R.; Acharya, U.R.; Khadem, N.; Mohammadi, A. Application of deep learning technique to manage COVID-19 in routine clinical practice using CT images: Results of 10 convolutional neural networks. Comput. Biol. Med. 2020, 121, 103795. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Wei, L.; Niu, P. The novel coronavirus outbreak in Wuhan, China. Glob. Health Res. Policy 2020, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Li, A.C.; Lee, D.T.; Misquitta, K.K.; Uno, K.; Wald, S. COVID-19 detection from chest radiographs using machine learning and convolutional neural networks. medRxiv 2020. [Google Scholar] [CrossRef]
- Cheng, J.; Yang, W.; Huang, M.; Huang, W.; Jiang, J.; Zhou, Y.; Yang, R.; Zhao, J.; Feng, Y.; Feng, Q. Retrieval of brain tumors by adaptive spatial pooling and fisher vector representation. PLoS ONE 2016, 11, e0157112. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, A.; Mahmood, A. Review of deep learning algorithms and architectures. IEEE Access 2019, 7, 53040–53065. [Google Scholar] [CrossRef]
- Dong, G.; Liao, G.; Liu, H.; Kuang, G. A review of the autoencoder and its variants: A comparative perspective from target recognition in synthetic-aperture radar images. IEEE Geosci. Remote Sens. Mag. 2018, 6, 44–68. [Google Scholar] [CrossRef]
- Dorigo, M.; Birattari, M.; Stutzle, T. Ant colony optimization. IEEE Comput. Intell. Mag. 2006, 1, 28–39. [Google Scholar] [CrossRef]
- Dorigo, M.; Socha, K. An introduction to ant colony optimization. In Handbook of Approximation Algorithms and Metaheuristics, 2nd ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 2018; pp. 395–408. ISBN 1351236423. [Google Scholar]
- Dorigo, M.; Blum, C. Ant colony optimization theory: A survey. Theor. Comput. Sci. 2005, 344, 243–278. [Google Scholar] [CrossRef]
- Kanan, H.R.; Faez, K.; Taheri, S.M. Feature selection using ant colony optimization (ACO): A new method and comparative study in the application of face recognition system. In Proceedings of the Industrial Conference on Data Mining, Leipzig, Germany, 14–18 July 2007; pp. 63–76. [Google Scholar]
- Tabakhi, S.; Moradi, P.; Akhlaghian, F. An unsupervised feature selection algorithm based on ant colony optimization. Eng. Appl. Artif. Intell. 2014, 32, 112–123. [Google Scholar] [CrossRef]
- Sivagaminathan, R.K.; Ramakrishnan, S. A hybrid approach for feature subset selection using neural networks and ant colony optimization. Expert Syst. Appl. 2007, 33, 49–60. [Google Scholar] [CrossRef]
- Yu, L.; Liu, H. Efficient feature selection via analysis of relevance and redundancy. J. Mach. Learn. Res. 2004, 5, 1205–1224. [Google Scholar]
- Bennasar, M.; Hicks, Y.; Setchi, R. Feature selection using joint mutual information maximisation. Expert Syst. Appl. 2015, 42, 8520–8532. [Google Scholar] [CrossRef] [Green Version]
- Hoque, N.; Bhattacharyya, D.K.; Kalita, J.K. MIFS-ND: A mutual information-based feature selection method. Expert Syst. Appl. 2014, 41, 6371–6385. [Google Scholar] [CrossRef]
- Kabir, M.; Shahjahan, M.; Murase, K.; Barbosa, H.J.C. Ant colony optimization toward feature selection. In Ant Colony Optimization—Techniques and Applications; IntechOpen: London, UK, 2013; pp. 1–43. [Google Scholar]
- Cheng, J.; Huang, W.; Cao, S.; Yang, R.; Yang, W.; Yun, Z.; Wang, Z.; Feng, Q. Enhanced performance of brain tumor classification via tumor region augmentation and partition. PLoS ONE 2015, 10, e0140381. [Google Scholar] [CrossRef]
- Thejaswini, P.; Bhat, M.B.; Prakash, M.K. Detection and classification of tumour in brain MRI. Int. J. Eng. Manufact.(IJEM) 2019, 9, 11–20. [Google Scholar]
- Afshar, P.; Mohammadi, A.; Plataniotis, K.N. Brain tumor type classification via capsule networks. In Proceedings of the 2018 25th IEEE International Conference on Image Processing (ICIP), Athens, Greece, 7–10 October 2018; pp. 3129–3133. [Google Scholar]
- Belaid, O.N.; Loudini, M. Classification of Brain Tumor by Combination of Pre-Trained VGG16 CNN. J. Inf. Technol. Manag. 2020, 12, 13–25. [Google Scholar]
- Ghassemi, N.; Shoeibi, A.; Rouhani, M. Deep neural network with generative adversarial networks pre-training for brain tumor classification based on MR images. Biomed. Signal Process. Control 2020, 57, 101678. [Google Scholar] [CrossRef]
- Özkaya, U.; Öztürk, Ş.; Barstugan, M. Coronavirus (COVID-19) classification using deep features fusion and ranking technique. In Big Data Analytics and Artificial Intelligence against COVID-19: Innovation Vision and Approach; Springer: Berlin/Heidelberg, Germany, 2020; pp. 281–295. [Google Scholar]
- Mollalo, A.; Rivera, K.M.; Vahedi, B. Artificial neural network modeling of novel coronavirus (COVID-19) incidence rates across the continental United States. Int. J. Environ. Res. Public Health 2020, 17, 4204. [Google Scholar] [CrossRef]
- Sethy, P.K.; Behera, S.K. Detection of coronavirus disease (COVID-19) based on deep features. Preprints 2020. [Google Scholar] [CrossRef] [Green Version]
- Gozes, O.; Frid-Adar, M.; Sagie, N.; Zhang, H.; Ji, W.; Greenspan, H. Coronavirus detection and analysis on chest ct with deep learning. arXiv 2020, arXiv:2004.02640. [Google Scholar]
- Yeşilkanat, C.M. Spatio-temporal estimation of the daily cases of COVID-19 in worldwide using random forest machine learning algorithm. Chaos Solitons Fractals 2020, 140, 110210. [Google Scholar] [CrossRef] [PubMed]
- Khoshbakhtian, F.; Ashraf, A.B.; Khan, S.S. Covidomaly: A deep convolutional autoencoder approach for detecting early cases of covid-19. arXiv 2020, arXiv:2010.02814. [Google Scholar]
- Khozeimeh, F.; Sharifrazi, D.; Izadi, N.H.; Joloudari, J.H.; Shoeibi, A.; Alizadehsani, R.; Gorriz, J.M.; Hussain, S.; Sani, Z.A.; Moosaei, H. CNN AE: Convolution Neural Network combined with Autoencoder approach to detect survival chance of COVID 19 patients. arXiv 2021, arXiv:2104.08954. [Google Scholar]
- Afshar, P.; Heidarian, S.; Naderkhani, F.; Oikonomou, A.; Plataniotis, K.N.; Mohammadi, A. Covid-caps: A capsule network-based framework for identification of covid-19 cases from x-ray images. Pattern Recognit. Lett. 2020, 138, 638–643. [Google Scholar] [CrossRef]
- de Oliveira, S.M.; Bezerra, L.C.T.; Stützle, T.; Dorigo, M.; Wanner, E.F.; de Souza, S.R. A computational study on ant colony optimization for the traveling salesman problem with dynamic demands. Comput. Oper. Res. 2021, 135, 105359. [Google Scholar] [CrossRef]
- Ning, J.; Zhang, Q.; Zhang, C.; Zhang, B. A best-path-updating information-guided ant colony optimization algorithm. Inf. Sci. 2018, 433, 142–162. [Google Scholar] [CrossRef]
- Shyu, S.J.; Yin, P.-Y.; Lin, B.M.T. An ant colony optimization algorithm for the minimum weight vertex cover problem. Ann. Oper. Res. 2004, 131, 283–304. [Google Scholar] [CrossRef]
- Latha, Y.L.M.; Prasad, M.V.N.K. GLCM based texture features for palmprint identification system. In Computational Intelligence in Data Mining-Volume 1; Springer: Berlin/Heidelberg, Germany, 2015; pp. 155–163. [Google Scholar]
- Gárate-Escamila, A.K.; El Hassani, A.H.; Andrès, E. Classification models for heart disease prediction using feature selection and PCA. Informatics Med. Unlocked 2020, 19, 100330. [Google Scholar] [CrossRef]
- Huang, C.-R.; Lee, L.-H. Contrastive approach towards text source classification based on top-bag-of-word similarity. In Proceedings of the 22nd Pacific Asia Conference on Language, Information and Computation, Cebu City, Philippines, 20–22 November 2008; pp. 404–410. [Google Scholar]
- Rui, W.; Xing, K.; Jia, Y. BOWL: Bag of word clusters text representation using word embeddings. In Proceedings of the International Conference on Knowledge Science, Engineering and Management, Passau, Germany, 5–7 October 2016; pp. 3–14. [Google Scholar]
- Ahmed, S.; Frikha, M.; Hussein, T.D.H.; Rahebi, J. Face Recognition System using Histograms of Oriented Gradients and Convolutional Neural Network based on with Particle Swarm Optimization. In Proceedings of the 2021 International Conference on Electrical, Communication, and Computer Engineering (ICECCE), Kuala Lumpur, Malaysia, 12–13 June 2021; pp. 1–5. [Google Scholar]
- Ahmed, S.; Frikha, M.; Hussein, T.D.H.; Rahebi, J. Optimum Feature Selection with Particle Swarm Optimization to Face Recognition System Using Gabor Wavelet Transform and Deep Learning. Biomed Res. Int. 2021, 2021, 6621540. [Google Scholar] [CrossRef]
- Allagwail, S.; Gedik, O.S.; Rahebi, J. Face recognition with symmetrical face training samples based on local binary patterns and the Gabor filter. Symmetry 2019, 11, 157. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Liu, S.; Cao, Y.; Li, X.; Yu, J.; Dai, D.; Ma, X.; Hu, S.; Wu, Z.; Liu, X.; et al. Speech emotion recognition using capsule networks. In Proceedings of the ICASSP 2019-2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, UK, 12–17 May 2019; pp. 6695–6699. [Google Scholar]
- Alashik, K.M.; Yildirim, R. Human Identity Verification From Biometric Dorsal Hand Vein Images Using the DL-GAN Method. IEEE Access 2021, 9, 74194–74208. [Google Scholar] [CrossRef]
- Hussin, S.H.S.; Yildirim, R. StyleGAN-LSRO Method for Person Re-Identification. IEEE Access 2021, 9, 13857–13869. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classifier | Prediction Speed | Memory Usage | Interpretability |
|---|---|---|---|
| Decision Tree (DT) | Fast | Small | Easy |
| Support Vector Machines (SVM) | Medium for linear Slow for others | Medium for linear All others: medium for multiclass, large for binary | Easy for Linear SVM Hard for all other kernel types |
| Kernel Nearest Neighbor (KNN) | Slow for cubic Medium for others | Medium | Hard |
| Ensemble | Fast to medium depending on choice of algorithm | Low to high depending on choice of algorithm | Hard |
| Naïve Bayes | Medium for simple distributions Slow for kernel distributions or high-dimensional data | Small for simple distributions Medium for kernel distributions or high-dimensional data | Easy |
| Discriminant Analysis | Fast | Small for linear, large for quadratic | Easy |
| Parameter | Abbreviation | Mathematic Expression |
|---|---|---|
| Sensitivity, Recall, hit rate, True Positive Rate | (TPR) | |
| Specificity, Selectivity, True Negative Rate | (TNR) | |
| Precision, Positive Predictive Value | (PPV) | |
| Negative Predictive Value | (NPV) | |
| Accuracy | (ACC) | |
| F1 Score | (F1 Score) | |
| Misclassification rate | (MR) | |
| Matthews correlation coefficient (MCC) | (MCC) |
| Method | Dataset | ACC | TPR | TNR | PPV | NPV | F1-Score | MR | MCC |
|---|---|---|---|---|---|---|---|---|---|
| DECISION TREE | COVID-19 | 97.74 | 88.49 | 98.63 | 86.20 | 98.89 | 87.33 | 2.25 | 0.86 |
| Brain Tumor | 92.82 | 88.17 | 94.84 | 88.17 | 94.84 | 88.17 | 7.17 | 0.83 | |
| SVM | COVID-19 | 98.68 | 98.05 | 98.73 | 87.06 | 99.82 | 92.23 | 1.31 | 0.92 |
| Brain Tumor | 96.57 | 93.19 | 98.10 | 95.69 | 96.95 | 94.42 | 3.42 | 0.92 | |
| KNN | COVID-19 | 97.74 | 89.18 | 98.55 | 85.34 | 98.97 | 87.22 | 2.25 | 0.86 |
| Brain Tumor | 99.18 | 97.88 | 99.76 | 99.46 | 99.06 | 98.66 | 0.81 | 0.98 | |
| ENSEMBLE | COVID-19 | 98.21 | 95.14 | 98.48 | 84.48 | 99.57 | 89.49 | 1.78 | 0.89 |
| Brain Tumor | 95.75 | 93.95 | 96.51 | 91.93 | 97.42 | 92.93 | 4.24 | 0.90 | |
| NAIVE BAYES | COVID-19 | 89.28 | 45.45 | 99.42 | 94.82 | 88.73 | 61.45 | 10.71 | 0.61 |
| Brain Tumor | 78.62 | 59.32 | 96.54 | 94.08 | 71.89 | 72.76 | 21.37 | 0.61 | |
| DISCRIMINANT | COVID-19 | 98.44 | 98.00 | 98.48 | 84.48 | 99.82 | 90.74 | 1.55 | 0.90 |
| Brain Tumor | 97.06 | 94.68 | 98.11 | 95.69 | 97.65 | 95.18 | 2.93 | 0.93 |
| Pretrained CNN with ACO (COVID-19 Dataset) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Classifiers | ACC | TPR | TNR | PPV | NPV | F1-SCORE | MR | MCC |
| Pre-trained CNN (AlexNet) + ACO | ||||||||
| DECISION TREE | 96.11 | 77.96 | 97.94 | 79.31 | 97.78 | 78.63 | 3.88 | 0.77 |
| SVM | 98.99 | 98.13 | 99.06 | 90.51 | 99.82 | 94.17 | 1.00 | 0.94 |
| KNN | 98.68 | 98.86 | 98.57 | 85.34 | 99.98 | 92.09 | 1.31 | 0.92 |
| ENSEMBLE | 98.52 | 98.98 | 98.48 | 84.48 | 99.91 | 91.16 | 1.47 | 0.91 |
| NAÏVE BAYES | 94.95 | 65.08 | 99.46 | 94.82 | 94.96 | 77.19 | 5.04 | 0.76 |
| DISCRIMINANT | 99.53 | 99.62 | 99.49 | 94.82 | 99.82 | 97.34 | 0.46 | 0.97 |
| Pre-trained CNN (GoogleNet) + ACO | ||||||||
| DECISION TREE | 97.04 | 84.82 | 98.21 | 81.89 | 98.54 | 83.33 | 2.95 | 0.82 |
| SVM | 98.91 | 98.11 | 98.98 | 89.65 | 99.82 | 93.69 | 1.08 | 0.93 |
| KNN | 98.68 | 99.00 | 98.65 | 86.20 | 99.91 | 92.16 | 1.31 | 0.92 |
| ENSEMBLE | 97.67 | 95.74 | 97.82 | 77.58 | 99.65 | 85.71 | 2.32 | 0.85 |
| NAÏVE BAYES | 98.44 | 91.37 | 99.14 | 91.37 | 99.14 | 91.37 | 1.55 | 0.91 |
| DISCRIMINANT | 98.83 | 98.09 | 98.90 | 88.79 | 99.82 | 93.21 | 1.16 | 0.93 |
| Pre-trained CNN (ResNet 50) + ACO | ||||||||
| DECISION TREE | 97.51 | 91.17 | 98.06 | 80.17 | 99.23 | 85.32 | 2.48 | 0.84 |
| SVM | 99.61 | 99.89 | 99.57 | 95.68 | 99.99 | 97.79 | 0.38 | 0.98 |
| KNN | 98.91 | 99.03 | 98.90 | 88.79 | 99.91 | 93.63 | 1.08 | 0.93 |
| ENSEMBLE | 99.14 | 99.23 | 99.07 | 90.51 | 99.97 | 95.02 | 0.85 | 0.95 |
| NAÏVE BAYES | 99.14 | 92.00 | 99.91 | 99.13 | 99.14 | 95.43 | 0.85 | 0.95 |
| DISCRIMINANT | 99.21 | 99.32 | 98.89 | 99.01 | 99.21 | 96.20 | 0.79 | 0.95 |
| Pre-trained CNN (DenseNet 201) + ACO | ||||||||
| DECISION TREE | 97.59 | 92.92 | 97.98 | 79.31 | 99.40 | 85.58 | 2.40 | 0.85 |
| SVM | 98.99 | 99.04 | 98.98 | 89.65 | 99.91 | 94.11 | 1.00 | 0.94 |
| KNN | 98.75 | 99.37 | 98.65 | 86.20 | 99.90 | 92.59 | 1.24 | 0.92 |
| ENSEMBLE | 98.83 | 99.56 | 98.73 | 87.06 | 99.86 | 93.08 | 1.16 | 0.93 |
| NAÏVE BAYES | 99.14 | 94.11 | 99.65 | 96.55 | 99.40 | 95.31 | 0.85 | 0.95 |
| DISCRIMINANT | 98.99 | 99.57 | 98.88 | 92.34 | 99.80 | 93.12 | 1.01 | 0.94 |
| Pretrained CNN with ACO (Brain Tumor Dataset) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Classifiers | ACC | TPR | TNR | PPV | NPV | F1-SCORE | MR | MCC |
| Pre-trained CNN (AlexNet) + ACO | ||||||||
| DECISION TREE | 91.68 | 86.09 | 94.13 | 86.55 | 93.91 | 86.32 | 8.31 | 0.80 |
| SVM | 98.53 | 96.33 | 99.52 | 98.92 | 98.36 | 97.61 | 1.46 | 0.97 |
| KNN | 98.20 | 96.29 | 99.05 | 97.84 | 98.36 | 97.06 | 1.79 | 0.96 |
| ENSEMBLE | 96.73 | 93.68 | 98.10 | 95.69 | 97.18 | 94.68 | 3.26 | 0.92 |
| NAÏVE BAYES | 89.55 | 74.79 | 99.45 | 98.92 | 85.48 | 85.18 | 10.44 | 0.79 |
| DISCRIMINANT | 98.69 | 95.87 | 99.92 | 99.95 | 98.12 | 97.89 | 1.30 | 0.97 |
| Pre-trained CNN (GoogleNet) + ACO | ||||||||
| DECISION TREE | 87.27 | 81.76 | 89.39 | 74.73 | 92.74 | 78.08 | 12.72 | 0.69 |
| SVM | 95.26 | 94.85 | 95.43 | 89.24 | 97.89 | 91.96 | 4.73 | 0.89 |
| KNN | 94.94 | 90.15 | 97.14 | 93.54 | 95.55 | 91.82 | 5.05 | 0.88 |
| ENSEMBLE | 93.80 | 91.57 | 94.71 | 87.63 | 96.48 | 89.56 | 6.19 | 0.85 |
| NAÏVE BAYES | 91.19 | 82.67 | 95.37 | 89.78 | 91.80 | 86.08 | 8.80 | 0.80 |
| DISCRIMINANT | 96.73 | 93.22 | 98.33 | 96.23 | 96.95 | 94.70 | 3.26 | 0.92 |
| Pre-trained CNN (ResNet 50) + ACO | ||||||||
| DECISION TREE | 88.09 | 79.58 | 91.94 | 81.72 | 90.86 | 80.63 | 11.90 | 0.72 |
| SVM | 97.55 | 98.30 | 97.24 | 93.54 | 99.29 | 95.86 | 2.44 | 0.94 |
| KNN | 97.87 | 95.76 | 98.82 | 97.31 | 98.12 | 96.53 | 2.12 | 0.95 |
| ENSEMBLE | 96.24 | 95.53 | 96.54 | 91.93 | 98.12 | 93.69 | 3.75 | 0.91 |
| NAÏVE BAYES | 91.02 | 79.11 | 97.93 | 95.69 | 88.99 | 86.61 | 8.97 | 0.81 |
| DISCRIMINANT | 96.24 | 94.53 | 96.97 | 93.01 | 97.65 | 93.76 | 3.75 | 0.91 |
| Pre-trained CNN (DenseNet 201) + ACO | ||||||||
| DECISION TREE | 91.51 | 86.41 | 93.70 | 85.48 | 94.14 | 85.94 | 8.48 | 0.80 |
| SVM | 98.20 | 96.29 | 99.05 | 97.84 | 98.36 | 97.06 | 1.79 | 0.96 |
| KNN | 97.71 | 95.26 | 98.81 | 97.31 | 97.89 | 96.27 | 2.28 | 0.95 |
| ENSEMBLE | 97.22 | 94.24 | 98.57 | 96.77 | 97.42 | 95.49 | 2.77 | 0.94 |
| NAÏVE BAYES | 93.96 | 87.81 | 96.87 | 93.01 | 94.37 | 90.33 | 6.03 | 0.86 |
| DISCRIMINANT | 95.22 | 93.84 | 96.05 | 88.54 | 90.41 | 91.45 | 4.78 | 0.89 |
| Method | Acc (%) |
|---|---|
| GLCM + CNN [30] | 82.00 |
| Intensity and texture features + PCA + ANN [23] | 91.00 |
| BOW + SVM [59] | 91.28 |
| 2D Discrete Wavelet transform (DWT) and 2D Gabor filter [24] | 95.66 |
| SVM+ANN [60] | 91.40 |
| Deep CNN+SVM [22] | 98.00 |
| Deep Convolution Neural Network VGG 19 + SoftMax classifier [31] | 94.58 |
| Capsule networks (CapsNets) [61] | 86.56 |
| GLCM + Pre-Trained VGG16 CNN [62] | 96.50 |
| GAN + ConvNet (random split) [63] | 95.60 |
| Auto-encoder + KNN (without ACO) | 97.22 |
| Proposed Method (Auto-encoder + ACO + KNN) | 99.18 |
| Method | Acc (%) |
|---|---|
| CNN with data fusion [64] | 98.27 |
| ANN [65] | 83.98 |
| DNN + SVM [66] | 95.33 |
| DNN [67] | 94.80 |
| Random Forest [68] | 95.90 |
| Stacked-auto-encoder [9] | 94.70 |
| Deep Convolutional Auto-encoder [69] | 76.52 |
| CNN + Auto-encoder [70] | 96.05 |
| Tailored CNN [40] | 92.30 |
| Dense Net [41] | 88.90 |
| Capsule Networks [71] | 95.70 |
| DarkNet-19 based CNN [42] | 87.02 |
| Deep Learning [42] | 98.08 |
| Deep Learning [43] | 86.27 |
| CNN + SVM (without ACO) | 96.45 |
| Proposed Method (CNN + ACO + SVM) | 99.61 |
| Dataset | Combined Methods | ACO | GA | ||||
|---|---|---|---|---|---|---|---|
| Classifiers | Accuracy | Time (h) | Classifiers | Accuracy | Time (h) | ||
| Covid-19 | Auto-encoder | SVM | 98.68% | 0:27:00 | KNN | 97.98% | 1:00:00 |
| CNN (AlexNet) | DISCRIMINANT | 99.53% | 1:17:00 | KNN | 98.60% | 2:07:00 | |
| CNN (GoogleNet) | SVM | 98.91% | 0:21:00 | NAÏVE BAYES | 98.13% | 0:40:00 | |
| CNN (ResNet 50) | SVM | 99.61% | 0:43:00 | KNN | 98.60% | 1:05:00 | |
| CNN (DenseNet 201) | NAÏVE BAYES | 99.14% | 0:39:00 | KNN | 98.75% | 1:04:00 | |
| Brain Tumor | Auto-encoder | KNN | 99.18% | 0:11:00 | ENSEMBLE | 96.24% | 0:16:00 |
| CNN (AlexNet) | DISCRIMINANT | 98.69% | 0:12:00 | ENSEMBLE | 94.61% | 0:30:00 | |
| CNN (GoogleNet) | DISCRIMINANT | 96.73% | 0:05:00 | KNN | 93.96% | 0:09:00 | |
| CNN (ResNet 50) | KNN | 97.87% | 0:11:00 | ENSEMBLE | 97.06% | 0:16:00 | |
| CNN (DenseNet 201) | SVM | 98.20% | 0:09:00 | ENSEMBLE | 96.57% | 0:18:00 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kadhim, Y.A.; Khan, M.U.; Mishra, A. Deep Learning-Based Computer-Aided Diagnosis (CAD): Applications for Medical Image Datasets. Sensors 2022, 22, 8999. https://doi.org/10.3390/s22228999
Kadhim YA, Khan MU, Mishra A. Deep Learning-Based Computer-Aided Diagnosis (CAD): Applications for Medical Image Datasets. Sensors. 2022; 22(22):8999. https://doi.org/10.3390/s22228999
Chicago/Turabian StyleKadhim, Yezi Ali, Muhammad Umer Khan, and Alok Mishra. 2022. "Deep Learning-Based Computer-Aided Diagnosis (CAD): Applications for Medical Image Datasets" Sensors 22, no. 22: 8999. https://doi.org/10.3390/s22228999