


A Flexible Near-Field Biosensor for Multisite Arterial Blood Flow Detection
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sensor Design
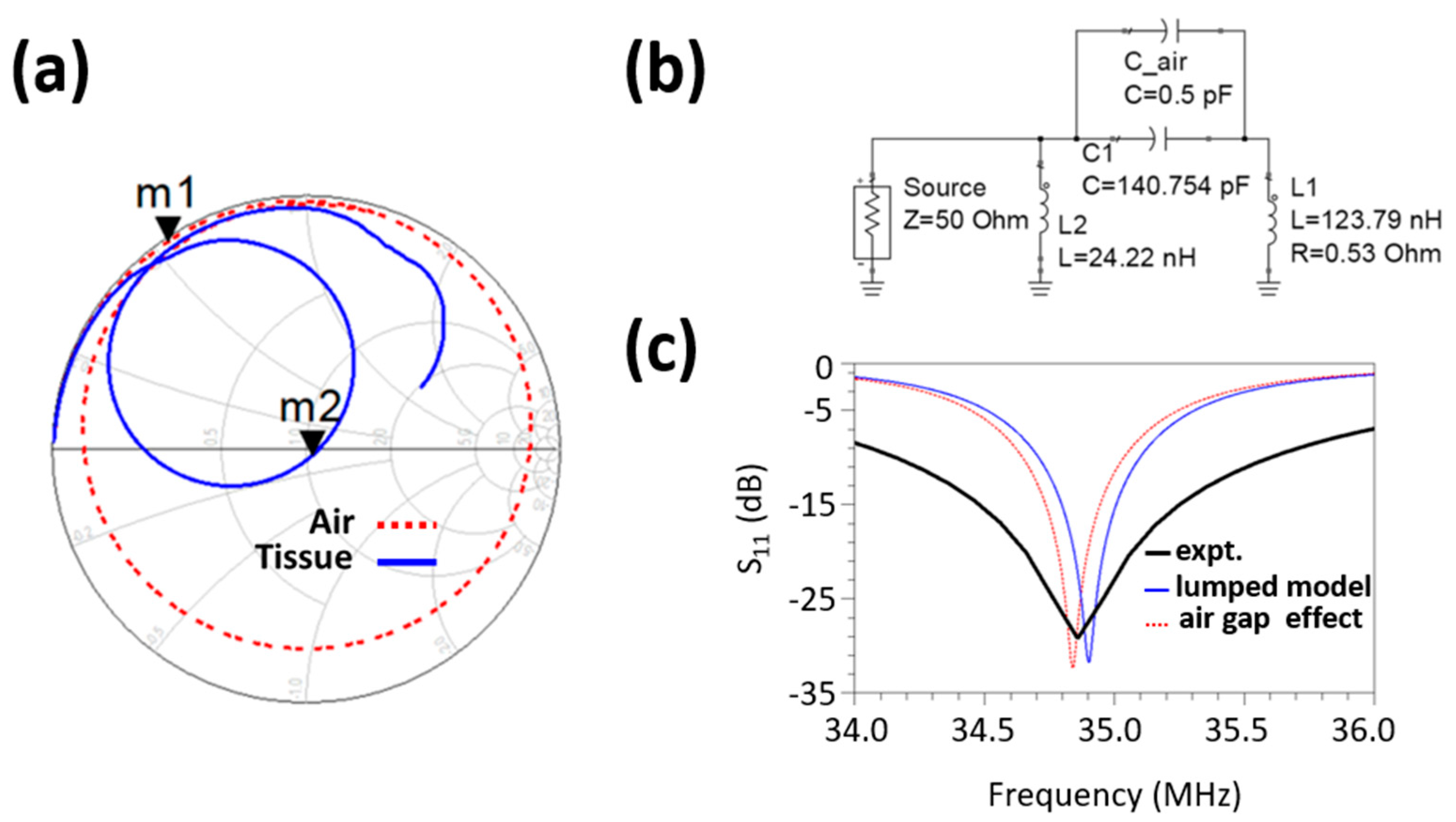
2.2. Computational Characterization
2.3. Readout Hardware
2.4. Methodologies
2.4.1. Experimental Setup and Data Acquisition
- Supraorbital location in the supine position;
- Carotid location in the supine position;
- Apex location in the supine position;
- Radial location in the seated position on a healthy male human subject (subject #1, age: 23 years).
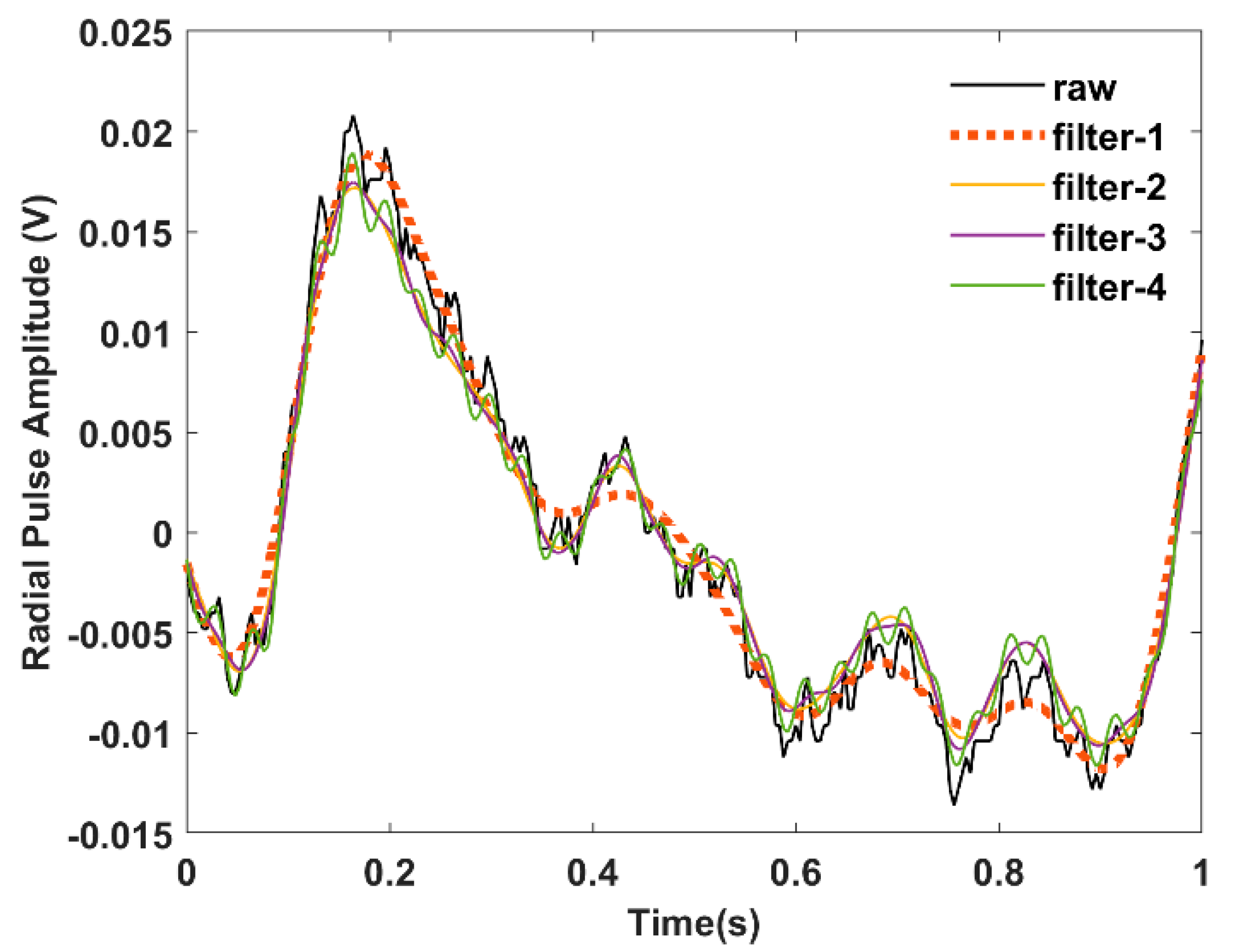
2.4.2. Signal Processing
3. Results
3.1. Radial Blood Flow Detection
3.2. Multisite Blood Flow Detection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- NMohammed; Cluff, K.; Griffith, J.; Loflin, B. A Noninvasive, Electromagnetic, Epidermal Sensing Device for Hemodynamics Monitoring. IEEE Trans. Biomed. Circuits Syst. 2019, 13, 1393–1404. [Google Scholar] [CrossRef] [PubMed]
- Cluff, K.; Patterson, J.; Becker, R.; Jayakumar, B.; Han, K.; Condon, E.; Dudley, K.; Szatkowski, G.; Pipinos, I.I.; Amick, R.Z. Passive Wearable Skin Patch Sensor Measures Limb Hemodynamics Based on Electromagnetic Resonance. IEEE Trans. Biomed. Eng. 2017, 65, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Nemati, E.; Deen, M.J.; Mondal, T. A wireless wearable ECG sensor for long-term applications. IEEE Commun. Mag. 2012, 50, 36–43. [Google Scholar] [CrossRef]
- Deng, Q.; Kammoun, M.; Erturk, A.; Sharma, P. Nanoscale flexoelectric energy harvesting. Int. J. Solids Struct. 2014, 51, 3218–3225. [Google Scholar] [CrossRef] [Green Version]
- NMohammed; Cluff, K.; Griffith, J.; Loflin, B. A Non-invasive Wearable Readout System for Bio-fluid Phenomena Detection. In Proceedings of the 2019 IEEE 16th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Chicago, IL, USA, 19–22 May 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1–4. [Google Scholar]
- Alruwaili, F.; Cluff, K.; Griffith, J.; Farhoud, H. Passive Self Resonant Skin Patch Sensor to Monitor Cardiac Intraventricular Stroke Volume Using Electromagnetic Properties of Blood. IEEE J. Transl. Eng. Health Med. 2018, 6, 1–9. [Google Scholar] [CrossRef]
- Griffith, J.; Cluff, K.; Eckerman, B.; Aldrich, J.; Becker, R.; Moore-Jansen, P.; Patterson, J. Non-Invasive Electromagnetic Skin Patch Sensor to Measure Intracranial Fluid–Volume Shifts. Sensors 2018, 18, 1022. [Google Scholar] [CrossRef] [Green Version]
- Tasnim, F.; Sadraei, A.; Datta, B.; Khan, M.; Choi, K.Y.; Sahasrabudhe, A.; Gálvez, T.A.V.; Wicaksono, I.; Rosello, O.; Nunez-Lopez, C.; et al. Towards personalized medicine: The evolution of imperceptible health-care technologies. Foresight 2018, 20, 589–601. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Li, X.; Hu, H.; Zhang, L.; Huang, Z.; Lin, M.; Zhang, Z.; Yin, Z.; Huang, B.; Gong, H.; et al. Monitoring of the central blood pressure waveform via a conformal ultrasonic device. Nat. Biomed. Eng. 2018, 2, 687. [Google Scholar] [CrossRef]
- Viventi, J.; Kim, D.-H.; Moss, J.D.; Kim, Y.-S.; Blanco, J.A.; Annetta, N.; Hicks, A.; Xiao, J.; Huang, Y.; Callans, D.J.; et al. A Conformal, Bio-Interfaced Class of Silicon Electronics for Mapping Cardiac Electrophysiology. Sci. Transl. Med. 2010, 2, 24ra22. [Google Scholar] [CrossRef] [Green Version]
- Miozzi, C.; Nappi, S.; Amendola, S.; Occhiuzzi, C.; Marrocco, G. A General-Purpose Configurable RFID Epidermal Board With a Two-Way Discrete Impedance Tuning. IEEE Antennas Wirel. Propag. Lett. 2019, 18, 684–687. [Google Scholar] [CrossRef]
- Ha, T.; Tran, J.; Liu, S.; Jang, H.; Jeong, H.; Mitbander, R.; Huh, H.; Qiu, Y.; Duong, J.; Wang, R.L.; et al. A Chest-Laminated Ultrathin and Stretchable E-Tattoo for the Measurement of Electrocardiogram, Seismocardiogram, and Cardiac Time Intervals. Adv. Sci. 2019, 6, 1900290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, Y.-J.; Kim, B.-H.; Yun, G.-H.; Kim, S.-W.; Hong, S.-B.; Yook, J.-G. Flexible Non-Constrained RF Wrist Pulse Detection Sensor Based on Array Resonators. IEEE Trans. Biomed. Circuits Syst. 2015, 10, 300–308. [Google Scholar] [CrossRef] [PubMed]
- An, Y.-J.; Yun, G.-H.; Kim, S.W.; Yook, J.-G. Wrist Pulse Detection System Based on Changes in the Near-Field Reflection Coefficient of a Resonator. IEEE Microw. Wirel. Components Lett. 2014, 24, 719–721. [Google Scholar] [CrossRef]
- An, Y.-J.; Yun, G.-H.; Yook, J.-G. Sensitivity Enhanced Vital Sign Detection Based on Antenna Reflection Coefficient Variation. IEEE Trans. Biomed. Circuits Syst. 2015, 10, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; An, Y.; Yun, G.; Yook, J. RF interferometric wearable wrist pulse detection system. IET Microw. Antennas Propag. 2018, 12, 167–172. [Google Scholar] [CrossRef]
- Kim, B.-H.; Hong, Y.; An, Y.-J.; Kim, S.-G.; Lee, H.-J.; Kim, S.-W.; Hong, S.-B.; Yun, G.-H.; Yook, J.-G. A Proximity Coupling RF Sensor for Wrist Pulse Detection Based on Injection-Locked PLL. IEEE Trans. Microw. Theory Tech. 2016, 64, 1667–1676. [Google Scholar] [CrossRef]
- Kim, S.W.; Choi, S.B.; An, Y.-J.; Kim, B.-H.; Kim, D.W.; Yook, J.-G. Heart Rate Detection During Sleep Using a Flexible RF Resonator and Injection-Locked PLL Sensor. IEEE Trans. Biomed. Eng. 2015, 62, 2568–2575. [Google Scholar] [CrossRef]
- Nopper, R.; Has, R.; Reindl, L. A wireless sensor readout system—Circuit concept, simulation, and accuracy. IEEE Trans. Instrum. Meas. 2011, 60, 2976–3983. [Google Scholar] [CrossRef]
- Tang, M.-C.; Liao, C.-M.; Wang, F.-K.; Horng, T.-S. Noncontact Pulse Transit Time Measurement Using a Single-Frequency Continuous-Wave Radar. In Proceedings of the 2018 IEEE/MTT-S International Microwave Symposium-IMS, Philadelphia, PA, USA, 10–15 June 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 1409–1412. [Google Scholar]
- Teichmann, D.; Foussier, J.; Jia, J.; Leonhardt, S.; Walter, M. Noncontact Monitoring of Cardiorespiratory Activity by Electromagnetic Coupling. IEEE Trans. Biomed. Eng. 2013, 60, 2142–2152. [Google Scholar] [CrossRef]
- Ermak, G.P.; Varavin, A.V.; Vasilev, A.S.; Stumbra, M.; Fateev, A.S.; Zacek, F.; Zajac, J. The phase detectors based on AD8302 for millimeter wave heterodyne interferometer. In Proceedings of the 2012 22nd International Crimean Conference Microwave & Telecommunication Technology, Sevastopol, Ukraine, 10–14 September 2012; IEEE: Piscataway, NJ, USA, 2012; pp. 827–828. [Google Scholar]
- Ganguly, P.; Senior, D.E.; Chakrabarti, A.; Parimi, P.V. Sensitive transmit receive architecture for body wearable RF plethysmography sensor. In Proceedings of the 2016 Asia-Pacific Microwave Conference (APMC), New Delhi, India, 5–9 December 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 1–4. [Google Scholar]
- Kible, V.; de Lima, R.N.; de Brito, K.B.; Bulau, A.; Zimmermann, A. Quadrature Block for UHF Reflection Coefficient Measurements Using a Directional Coupler and Injection Locking. IEEE Trans. Instrum. Meas. 2019, 69, 275–285. [Google Scholar] [CrossRef]
- Woodard, S.E. SansEC sensing technology—A new tool for designing space systems and components. In Proceedings of the 2011 Aerospace Conference, Big Sky, MT, USA, 5–12 March 2011; IEEE: Piscataway, NJ, USA, 2011; pp. 1–11. [Google Scholar]
- Wilson, D.L.; Geselowitz, D.B. Physical Principles of the Displacement Cardiograph Including a New Device Sensitive to Variations in Torso Resistivity. IEEE Trans. Biomed. Eng. 1981, BME-28, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Challis, L. Mechanisms for interaction between RF fields and biological tissue. Bioelectromagnetics 2005, 26, S98–S106. [Google Scholar] [CrossRef] [PubMed]
- Teichmann, D.; de Matteis, D.; Bartelt, T.; Walter, M.; Leonhardt, S. A bendable and wearable cardiorespiratory monitoring device fusing two noncontact sensor principles. IEEE J. Biomed. Health Inform. 2015, 19, 784–793. [Google Scholar] [CrossRef]
- Body Tissue Dielectric Parameters. Available online: https://www.fcc.gov/general/body-tissue-dielectric-parameters (accessed on 28 September 2019).
- Durney, C.H.; Massoudi, H.; Iskander, M.F. Radiofrequency Radiation Dosimetry Handbook; The University of Utah’s Department of Electrical and Computer Engineering: Salt Lake City, UT, USA, 1986. [Google Scholar]
- Miozzi, C.; Saggio, G.; Gruppioni, E.; Marrocco, G. Performance Comparison of Patch and Loop Antennas for the Wireless Power Transfer and Transcutaneous Telemetry in the 860–960 MHz Frequency Band. In Proceedings of the 2019 IEEE 16th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Chicago, IL, USA, 5–12 May 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1–4. [Google Scholar]
- ISCC. IEEE Recommended Practice for Determining the Peak Spatial-Average Specific Absorption Rate (SAR) in the Human Head from Wireless Communications Devices: Measurement Techniques; Institute of Electrical and Electronic Engineers: Piscataway, NJ, USA, 2003. [Google Scholar]
- Kim, J.U.; Lee, Y.J.; Lee, J.; Kim, J.Y. Differences in the properties of the radial artery between Cun, Guan, Chi, and nearby segments using ultrasonographic imaging: A pilot study on arterial depth, diameter, and blood flow. Evid.-Based Complement. Altern. Med. 2015, 2015, 381634. [Google Scholar]
- Laurent, S.; Girerd, X.; Mourad, J.J.; Lacolley, P.; Beck, L.; Boutouyrie, P.; Mignot, J.P.; Safar, M. Elastic modulus of the radial artery wall material is not increased in patients with essential hypertension. Arter. Thromb. A J. Vasc. Biol. 1994, 14, 1223–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elsamnah, F.; Bilgaiyan, A.; Affiq, M.; Shim, C.-H.; Ishidai, H.; Hattori, R. Comparative Design Study for Power Reduction in Organic Optoelectronic Pulse Meter Sensor. Biosensors 2019, 9, 48. [Google Scholar] [CrossRef] [Green Version]
- Tyan, C.-C.; Liu, S.-H.; Chen, J.-Y.; Chen, J.-J.; Liang, W.-M. A Novel Noninvasive Measurement Technique for Analyzing the Pressure Pulse Waveform of the Radial Artery. IEEE Trans. Biomed. Eng. 2007, 55, 288–297. [Google Scholar] [CrossRef]
- Politi, M.T.; Ghigo, A.; Fernández, J.M.; Khelifa, I.; Gaudric, J.; Fullana, J.M.; Lagrée, P.-Y. The dicrotic notch analyzed by a numerical model. Comput. Biol. Med. 2016, 72, 54–64. [Google Scholar] [CrossRef]
- Becker, R. RF Resonant Skin Patch Sensor for Peripheral Limb Hemodynamics; Wichita State University: Wichita, KS, USA, 2019. [Google Scholar]
- Chen, J.; Liu, H.; Wang, W.; Nabulsi, N.; Zhao, W.; Kim, J.Y.; Kwon, M.; Ryou, J. High Durable, Biocompatible, and Flexible Piezoelectric Pulse Sensor Using Single-Crystalline III-N Thin Film. Adv. Funct. Mater. 2019, 1903162. [Google Scholar] [CrossRef]
- Chen, L.Y.; Tee, C.K.; Chortos, A.; Schwartz, G.; Tse, V.; Lipomi, D.J.; Wong, H.-S.P.; McConnell, M.; Bao, Z. Continuous wireless pressure monitoring and mapping with ultra-small passive sensors for health monitoring and critical care. Nat. Commun. 2014, 5, 5028. [Google Scholar] [CrossRef] [Green Version]
- Loflin, B.; Cluff, K.; Griffith, J.; Mohammed, N. Identification of shoulder joint clearance in space suit using electromagnetic resonant spiral proximity sensor for injury prevention. Acta Astronaut. 2020, 170, 46–54. [Google Scholar] [CrossRef]
- Schmidt, D.; Mahapatro, A.; Loflin, B.; Cluff, K. Evaluation of Polyvinylidene Fluoride (PVDF) integrated sensor for physiological temperature detection. Mater. Technol. 2022, 37, 1725–1733. [Google Scholar] [CrossRef]
- Elgendi, M.; Liang, Y.; Ward, R. Toward Generating More Diagnostic Features from Photoplethysmogram Waveforms. Diseases 2018, 6, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, J.; Ito, S. Pulse Pressure Amplification, Arterial Stiffness, and Peripheral Wave Reflection Determine Pulsatile Flow Waveform of the Femoral Artery. Hypertension 2010, 56, 926–933. [Google Scholar] [CrossRef] [Green Version]
- O’Rourke, M.F.; Pauca, A.; Jiang, X.J. Pulse wave analysis. Br. J. Clin. Pharmacol. 2001, 51, 507–522. [Google Scholar] [CrossRef]
- Scissons, R. Characterizing Triphasic, Biphasic, and Monophasic Doppler Waveforms: Should a Simple Task Be So Difficult? J. Diagn. Med. Sonogr. 2008, 24, 269–276. [Google Scholar] [CrossRef]
- Etemadi, M.; Inan, O.T.; Heller, J.A.; Hersek, S.; Klein, L.; Roy, S. A wearable patch to enable long-term monitoring of environmental, activity and hemodynamics variables. IEEE Trans. Biomed. Circuits Syst. 2015, 10, 280–288. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Allen, J.; Khalid, S.G.; Chen, F.; Zheng, D. Filtering-induced time shifts in photoplethysmography pulse features measured at different body sites: The importance of filter definition and standardization. Physiol. Meas. 2021, 42, 074001. [Google Scholar] [CrossRef]
- Hartmann, V.; Liu, H.; Chen, F.; Hong, W.; Hughes, S.; Zheng, D. Toward Accurate Extraction of Respiratory Frequency From the Photoplethysmogram: Effect of Measurement Site. Front. Physiol. 2019, 10, 732. [Google Scholar] [CrossRef]











Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohammed, N.; Cluff, K.; Sutton, M.; Villafana-Ibarra, B.; Loflin, B.E.; Griffith, J.L.; Becker, R.; Bhandari, S.; Alruwaili, F.; Desai, J. A Flexible Near-Field Biosensor for Multisite Arterial Blood Flow Detection. Sensors 2022, 22, 8389. https://doi.org/10.3390/s22218389
Mohammed N, Cluff K, Sutton M, Villafana-Ibarra B, Loflin BE, Griffith JL, Becker R, Bhandari S, Alruwaili F, Desai J. A Flexible Near-Field Biosensor for Multisite Arterial Blood Flow Detection. Sensors. 2022; 22(21):8389. https://doi.org/10.3390/s22218389
Chicago/Turabian StyleMohammed, Noor, Kim Cluff, Mark Sutton, Bernardo Villafana-Ibarra, Benjamin E. Loflin, Jacob L. Griffith, Ryan Becker, Subash Bhandari, Fayez Alruwaili, and Jaydip Desai. 2022. "A Flexible Near-Field Biosensor for Multisite Arterial Blood Flow Detection" Sensors 22, no. 21: 8389. https://doi.org/10.3390/s22218389