
Accuracy of Ground Reaction Force and Muscle Activation Prediction in a Child-Adapted Musculoskeletal Model


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurement Procedure and Equipment
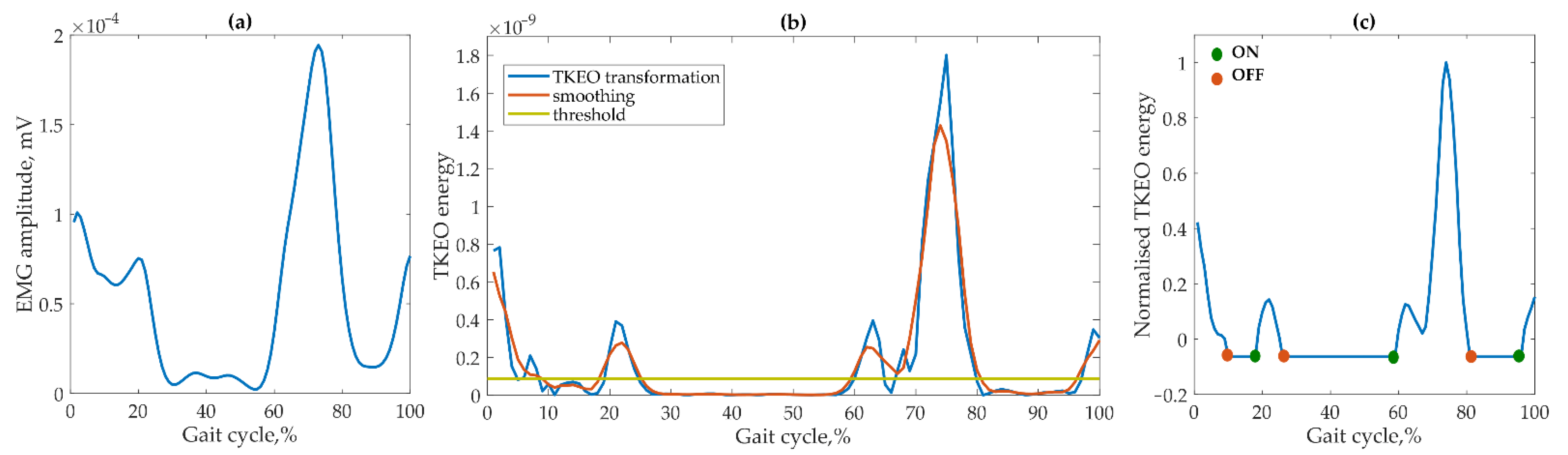
2.3. Data Processing
2.4. Model Description and Output
2.5. Model Accuracy Evaluation
- (1)
- the root-mean-square error (RMSE);
- (2)
- the Pearson correlation coefficient r;
- (3)
- (4)
- the coincidence of muscle activity (only for a comparison of muscle activations).
3. Results
3.1. Accuracy Assessment of Muscular Activation
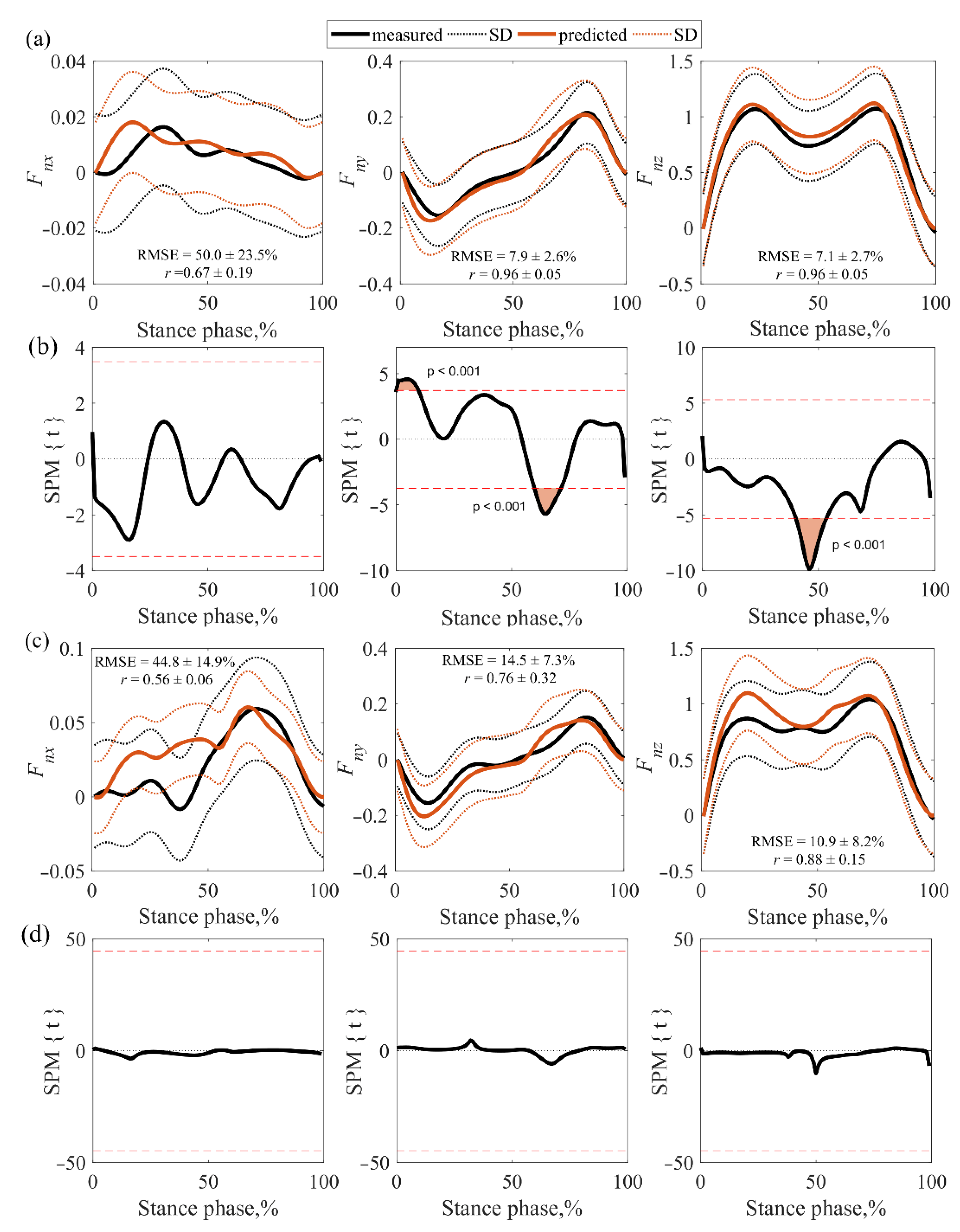
3.2. Accuracy Assessment of GRFs
4. Discussion
- MS model activation start delay [33];
- The time delay introduced by a low-pass Butterworth digital filter selected for EMG data [34];
- A large number of the MS model outputs, because a particular muscle is divided into several fibres, and during the measurements the EMG signal is more related to the activity in the largest parts of the muscle closest to the electrodes [37].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects | Body Side | Mismatch of Muscle Activations (%) | ||||
|---|---|---|---|---|---|---|
| BF | RF | SE | LG | MG | ||
| HCH | Right (n = 376) | 21.5 ± 17.2 | 17.0 ± 20.1 | 24.6 ± 18.7 | 24.4 ± 15.4 | 31.9 ± 18.4 |
| Left (n = 373) | 30.0 ± 22.4 | 20.2 ± 21.1 | 27.1 ± 18.0 | 29.3 ± 20.1 | 29.0 ± 17.2 | |
| Both (n = 749) | 25.8 ± 20.1 | 18.6 ± 20.2 | 25.9 ± 18.1 | 26.8 ± 17.8 | 30.4 ± 17.6 | |
| CPh1 | Right n = 41) | 39.0 | 19.0 | 36.0 | 12.0 | 50.0 |
| Left (n = 41) | 44.0 | 26.0 | 46.0 | 36.0 | 41.0 | |
| Both (n = 82) | 41.5 ± 3.5 | 22.5 ± 4.9 | 41.0 ± 7.1 | 24.0 ± 16.9 | 45.5 ± 6.4 | |
| CPd1 | Right (n = 32) | 35.0 | 25.0 | 38.0 | 14.0 | 21.0 |
| Left (n = 32) | 56.0 | 24.0 | 41.0 | 28.0 | 23.0 | |
| Both (n = 64) | 45.5 ± 14.8 | 24.5 ± 0.7 | 39.5 ± 2.1 | 21.0 ± 9.9 | 22.0 ± 1.4 | |
| CPd2 | Right (n = 2) | 0 | 0 | 0 | 0 | 0 |
| Left (n = 1) | 0 | 0 | 0 | 0 | 0 | |
| Both (n = 3) | 0 | 0 | 0 | 0 | 0 | |
| CPd3 | Right (n = 13) | 1.0 | 11.0 | 0 | 35.0 | 37.0 |
| Left (n = 13) | 4.0 | 4.0 | 0 | 17.0 | 11.0 | |
| Both (n = 26) | 2.5 ± 2.1 | 7.5 ± 4.9 | 0 | 26.0 ± 12.7 | 24.0 ± 18.4 | |
| Subjects | Body Side | Muscular Activity Coincidence (%) | ||||
|---|---|---|---|---|---|---|
| BF | RF | SE | LG | MG | ||
| HCH | Right (n = 376) | 61.5 ± 23.1 | 58.1 ± 23.4 | 60.9 ± 23.6 | 62.4 ± 22.8 | 64.9 ± 24.1 |
| Left (n = 373) | 62.1 ± 24.2 | 59.9 ± 23.2 | 64.7 ± 21.9 | 67.5 ± 21.8 | 75.6 ± 18.3 | |
| Both (n = 749) | 61.8 ± 24.6 | 59.0 ± 23.3 | 62.8 ± 22.7 | 64.9 ± 22.3 | 70.3 ± 21.2 | |
| CPh1 | Right (n = 41) | 61.5 ± 27.9 | 54.6 ± 25.3 | 57.6 ± 35.7 | 47.3 ± 27.8 | 64.3 ± 29.1 |
| Left (n = 41) | 57.5 ± 25.3 | 62.8 ± 29.6 | 53.5 ± 23.9 | 63.1 ± 24.2 | 75.8 ± 20.6 | |
| Both (n = 82) | 59.5 ± 26.6 | 58.7 ± 27.5 | 55.6 ± 29.8 | 55.2 ± 26.0 | 70.1 ± 24.9 | |
| CPd1 | Right (n = 32) | 72.4 ± 21.9 | 48.4 ± 30.4 | 61.1 ± 26.2 | 69.3 ± 20.2 | 72.7 ± 18.8 |
| Left (n = 32) | 65.3 ± 27.2 | 60.2 ± 20.8 | 63.1 ± 29.5 | 54.5 ± 27.3 | 61.6 ± 22.8 | |
| Both (n = 64) | 68.9 ± 24.6 | 54.3 ± 25.6 | 62.1 ± 27.9 | 61.9 ± 23.8 | 67.2 ± 20.8 | |
| CPd2 | Right (n = 2) | 92.9 ± 10.1 | 75.5 ± 14.5 | 91.4 ± 8.9 | 96.7 ± 2.3 | 38.1 ± 0.9 |
| Left (n = 1) | 68.5 | 95.8 | 66.0 | 84.5 | 96.5 | |
| Both (n = 3) | 84.7 ± 15.8 | 82.3 ± 15.6 | 82.9 ± 15.9 | 92.7 ± 7.3 | 57.6 ± 33.7 | |
| CPd3 | Right (n = 13) | 59.9 ± 26.1 | 40.5 ± 29.3 | 67.8 ± 16.6 | 51.1 ± 38.1 | 62.3 ± 29.9 |
| Left (n = 13) | 58.2 ± 24.3 | 32.6 ± 28.1 | 35.8 ± 27.8 | 75.5 ± 18.5 | 70.1 ± 16.4 | |
| Both (n = 26) | 59.1 ± 25.2 | 36.6 ± 28.7 | 51.8 ± 22.2 | 63.3 ± 28.3 | 66.2 ± 23.2 | |
References
- Black, M.M.; Walker, S.P.; Fernald, L.C.H.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early Childhood Development Coming of Age: Science through the Life Course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef] [Green Version]
- Rastegarpanah, A.; Scone, T.; Saadat, M.; Rastegarpanah, M.; Taylor, S.; Sadeghein, N. Targeting Effect on Gait Parameters in Healthy Individuals and Post-stroke Hemiparetic Individuals. J. Rehabil. Assist. Technol. Eng. 2018, 5, 2055668318766710. [Google Scholar] [CrossRef] [PubMed]
- Senden, R.; Grimm, B.; Heyligers, I.C.; Savelberg, H.H.C.M.; Meijer, K. Acceleration-Based Gait Test for Healthy Subjects: Reliability and Reference Data. Gait Posture 2009, 30, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, E.J.; Gutierrez-Farewik, E.M. Computation of Ground Reaction Force Using Zero Moment Point. J. Biomech. 2015, 48, 3776–3781. [Google Scholar] [CrossRef] [Green Version]
- Fluit, R.; Andersen, M.S.; Kolk, S.; Verdonschot, N.; Koopman, H.F.J.M. Prediction of Ground Reaction Forces and Moments during Various Activities of Daily Living. J. Biomech. 2014, 47, 2321–2329. [Google Scholar] [CrossRef]
- Oh, S.E.; Choi, A.; Mun, J.H. Prediction of Ground Reaction Forces during Gait Based on Kinematics and a Neural Network Model. J. Biomech. 2013, 46, 2372–2380. [Google Scholar] [CrossRef]
- Recinos, E.; Abella, J.; Riyaz, S.; Demircan, E. Real-Time Vertical Ground Reaction Force Estimation in a Unified Simulation Framework Using Inertial Measurement Unit Sensors. Robotics 2020, 9, 88. [Google Scholar] [CrossRef]
- Arnold, E.M.; Ward, S.R.; Lieber, R.L.; Delp, S.L. A Model of the Lower Limb for Analysis of Human Movement. Ann. Biomed. Eng. 2010, 38, 269–279. [Google Scholar] [CrossRef] [Green Version]
- Durandau, G.; Farina, D.; Sartori, M. Robust Real-Time Musculoskeletal Modeling Driven by Electromyograms. IEEE Trans. Biomed. Eng. 2018, 65, 556–564. [Google Scholar] [CrossRef] [Green Version]
- Burkhart, K.A.; Bruno, A.G.; Bouxsein, M.L.; Bean, J.F.; Anderson, D. Estimating Apparent Maximum Muscle Stress of Trunk Extensor Muscles in Older Adults Using Subject-Specific Musculoskeletal Models. J. Orthop. Res. 2018, 36, 498–505. [Google Scholar] [CrossRef]
- Scheys, L.; Jonkers, I.; Schutyser, F.; Pans, S.; Spaepen, A.; Suetens, P. Image Based Methods to Generate Subject-Specific Musculoskeletal Models for Gait Analysis. Int. Congr. Ser. 2005, 1281, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Teran, J.; Sifakis, E.; Blemker, S.; Ng-Thow-Hing, V.; Lau, C.; Fedkiw, R. Creating and Simulating Skeletal Muscle from the Visible Human Data Set. IEEE Trans. Vis. Comput. Graph. 2005, 11, 317–328. [Google Scholar] [CrossRef]
- Wesseling, M.; Bosmans, L.; Van Dijck, C.; Sloten, J.V.; Wirix-Speetjens, R.; Jonkers, I. Non-rigid Deformation to Include Subject-Specific Detail in Musculoskeletal Models of CP Children with Proximal Femoral Deformity and Its Effect on Muscle and Contact Forces during Gait. Comput. Methods Biomech. Biomed. Eng. 2019, 22, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Hainisch, R.; Kranzl, A.; Lin, Y.-C.; Pandy, M.G.; Gfoehler, M. A Generic Musculoskeletal Model of the Juvenile Lower Limb for Biomechanical Analyses of Gait. Comput. Methods Biomech. Biomed. Eng. 2020, 24, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Sicilia, A. A Musculoskeletal Multibody Algorithm Based on a Novel Rheonomic Constraints Definition Applied to the Lower Limb. J. Biomech. Eng. 2022, 144, 081010. [Google Scholar] [CrossRef]
- Koller, W.; Baca, A.; Kainz, H. Impact of Scaling Errors of the Thigh and Shank Segments on Musculoskeletal Simulation Results. Gait Posture 2021, 87, 65–74. [Google Scholar] [CrossRef]
- Paternostro-Sluga, T.; Grim-Stieger, M.; Posch, M.; Schuhfried, O.; Vacariu, G.; Mittermaier, C.; Bittner, C.; Fialka-Moser, V. Reliability and Validity of the Medical Research Council (MRC) Scale and a Modified Scale for Testing Muscle Strength in Patients with Radial Palsy. J. Rehabil. Med. 2008, 40, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Dufek, J.S.; Currie, R.L.; Gouws, P.-L.; Candela, L.; Gutierrez, A.P.; Mercer, J.A.; Putney, L.G. Effects of Overweight and Obesity on Walking Characteristics in Adolescents. Hum. Mov. Sci. 2012, 31, 897–906. [Google Scholar] [CrossRef]
- DeWolf, A.H.; Sylos-Labini, F.; Cappellini, G.; Lacquaniti, F.; Ivanenko, Y. Emergence of Different Gaits in Infancy: Relationship Between Developing Neural Circuitries and Changing Biomechanics. Front. Bioeng. Biotechnol. 2020, 8, 473. [Google Scholar] [CrossRef]
- Palisano, R.J.; Rosenbaum, P.; Bartlett, D.; Livingston, M.H. Content Validity of the Expanded and Revised Gross Motor Function Classification System. Dev. Med. Child Neurol. 2008, 50, 744–750. [Google Scholar] [CrossRef]
- Davis, R.B.; Õunpuu, S.; Tyburski, D.; Gage, J.R. A Gait Analysis Data Collection and Reduction Technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Solnik, S.; Rider, P.; Steinweg, K.; DeVita, P.; Hortobágyi, T. Teager–Kaiser Energy Operator Signal Conditioning Improves EMG Onset Detection. Eur. J. Appl. Physiol. 2010, 110, 489–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özgünen, K.T.; Çelik, U.; Kurdak, S.S. Determination of an Optimal Threshold Value for Muscle Activity Detection in EMG Analysis. J. Sport Sci. Med. 2010, 9, 620–628. [Google Scholar]
- Roewer, B.D.; Ford, K.R.; Myer, G.D.; Hewett, T.E. The ‘Impact’ of Force Filtering Cut-off Frequency on the Peak Knee Abduction Moment during Landing: Artefact or ‘Artifiction’? Br. J. Sport Med. 2014, 48, 464–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Den Bogert, A.J.; De Koning, J.J. On Optimal Filtering for Inverse Dynamics Analysis. 1996. Available online: http://www.kin.ucalgary.ca/isb/data/invdyn (accessed on 8 June 2021).
- White, R.; Agouris, I.; Selbie, R.D.; Kirkpatrick, M. The Variability of Force Platform Data in Normal and Cerebral Palsy Gait. Clin. Biomech. 1999, 14, 185–192. [Google Scholar] [CrossRef]
- Rasmussen, J.; Zee, M.D.; Damsgaard, M.; Christensen, S.T.; Marek, C.; Siebertz, K. A General Method for Scaling Musculo-Skeletal Models. 2005. Available online: http://www.ramsis.de (accessed on 9 June 2021).
- Pataky, T.C. Generalized N-Dimensional Biomechanical Field Analysis Using Statistical Parametric Mapping. J. Biomech. 2010, 43, 1976–1982. [Google Scholar] [CrossRef]
- Friston, K.J.; Holmes, A.P.; Worsley, K.J.; Poline, J.-P.; Frith, C.D.; Frackowiak, R.S.J. Statistical Parametric Maps in Functional Imaging: A General Linear Approach. Hum. Brain Mapp. 1994, 2, 189–210. [Google Scholar] [CrossRef]
- Halawi, L.; Clarke, A.; George, K. Evaluating Predictive Performance. In Harnessing the Power of Analytics; Springer: Cham, Switzerland, 2022; pp. 51–59. [Google Scholar] [CrossRef]
- Taylor, R. Interpretation of the Correlation Coefficient: A Basic Review. J. Diagn. Med. Sonogr. 1990, 6, 35–39. [Google Scholar] [CrossRef]
- Lilliefors, H.W. On the Kolmogorov-Smirnov Test for Normality with Mean and Variance Unknown. J. Am. Stat. Assoc. 1967, 62, 399–402. [Google Scholar] [CrossRef]
- Mörl, F.; Siebert, T.; Schmitt, S.; Blickhan, R.; Günther, M. Electro-Mechanical Delay in Hill-Type Muscle Models. J. Mech. Med. Biol. 2012, 12, 1250085. [Google Scholar] [CrossRef]
- Manal, K.; Rose, W. A General Solution for the Time Delay Introduced by a Low-Pass Butterworth Digital Filter: An Application to Musculoskeletal Modeling. J. Biomech. 2007, 40, 678–681. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Zemany, L.; Peng, C.-K.; Goldberger, A.L. Maturation of Gait Dynamics: Stride-To-Stride Variability and Its Temporal Organization in Children. J. Appl. Physiol. 1999, 86, 1040–1047. [Google Scholar] [CrossRef] [Green Version]
- Agostini, V.; Nascimbeni, A.; Gaffuri, A.; Imazio, P.; Benedetti, M.G.; Knaflitz, M. Normative EMG Activation Patterns of School-Age Children During Gait. Gait Posture 2010, 32, 285–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damsgaard, M.; Rasmussen, J.; Christensen, S.T.; Surma, E.; de Zee, M. Analysis of Musculoskeletal Systems in the AnyBody Modeling System. Simul. Model. Pract. Theory 2006, 14, 1100–1111. [Google Scholar] [CrossRef]
- Rajagopal, A.; Dembia, C.L.; DeMers, M.S.; Delp, D.D.; Hicks, J.L.; Delp, S.L. Full-Body Musculoskeletal Model for Muscle-Driven Simulation of Human Gait. IEEE Trans. Biomed. Eng. 2016, 63, 2068–2079. [Google Scholar] [CrossRef]
- Ding, Z.; Azmi, N.L.; Bull, A.M.J. Validation and Use of a Musculoskeletal Gait Model to Study the Role of Functional Electrical Stimulation. IEEE Trans. Biomed. Eng. 2019, 66, 892–897. [Google Scholar] [CrossRef]
- Ding, Z.; Tsang, C.K.; Nolte, D.; Kedgley, A.E.; Bull, A.M.J. Improving Musculoskeletal Model Scaling Using an Anatomical Atlas: The Importance of Gender and Anthropometric Similarity to Quantify Joint Reaction Forces. IEEE Trans. Biomed. Eng. 2019, 66, 3444–3456. [Google Scholar] [CrossRef]








| Age (year) | Height (m) | BMI (kg/m2) | |
|---|---|---|---|
| Male (n = 6) | 9.0 ± 1.6 | 1.340 ± 0.109 | 15.9 ± 1.8 |
| Female (n = 11) | 7.6 ± 2.0 | 1.299 ± 0.108 | 16.6 ± 2.4 |
| All | 7.9 ± 2.0 | 1.314 ± 0.107 | 16.4 ± 2.2 |
| Marking | CP Form |
GMFCS Score | Affected Side | Gender | Age (year) | Height (m) | BMI (kg/m2) |
|---|---|---|---|---|---|---|---|
| CPh1 (n = 1) | H | 1 | right | F | 7.0 | 1.320 | 17.9 |
| CPd1 (n = 1) | D | 1 | both | F | 8.0 | 1.370 | 16.4 |
| CPd2 (n = 1) | D | 2 | both | M | 7.0 | 1.270 | 13.6 |
| CPd3 (n = 1) | D | 3 | both | M | 6.0 | 1.180 | 15.8 |
| All | - | 1.6 ± 0.9 | - | - | 7.0 ± 0.82 | 1.285 ± 0.08 | 15.4 ± 1.8 |
| Subjects | Body Side and Stride Number | RMSE (%) | ||||
|---|---|---|---|---|---|---|
| BF | RF | SE | LG | MG | ||
| HCH | Right (n = 376) | 21.4 ± 9.3 | 22.0 ± 6.4 | 26.1 ± 9.2 | 22.4 ± 2.3 | 25.4 ± 5.4 |
| Left (n = 373) | 26.0 ± 9.4 | 20.5 ± 7.9 | 27.1 ± 6.8 | 21.1 ± 6.2 | 25.5 ± 7.8 | |
| CPh1 | Right n = 41) | 23.0 ± 7.6 | 18.4 ± 7.6 | 22.2 ± 6.8 | 22.8 ± 6.3 | 24.7 ± 6.1 |
| Left (n = 41) | 29.1 ± 9.1 | 18.3 ± 6.4 | 29.3 ± 6.2 | 20.2 ± 5.0 | 22.8 ± 5.7 | |
| CPd1 | Right (n = 32) | 30.7 ± 4.2 | 20.2 ± 6.5 | 32.1 ± 7.3 | 21.8 ± 12.0 | 14.8 ± 4.5 |
| Left (n = 32) | 30.8 ± 6.4 | 16.9 ± 13.5 | 24.9 ± 4.5 | 14.5 ± 8.9 | 16.5 ± 9.5 | |
| CPd2 | Right (n = 2) | 21.4 ± 5.5 | 13.8 ± 7.1 | 14.5 ± 10.1 | 25.4 ± 6.7 | 27.9 ± 8.5 |
| Left (n = 1) | 18.1 | 10.4 | 22.7 | 21.9 | 28.1 | |
| CPd3 | Right (n = 13) | 18.9 ± 7.3 | 32.8 ± 7.1 | 18.4 ± 9.2 | 34.3 ± 8.4 | 35.2 ± 9.4 |
| Left (n = 13) | 18.7 ± 5.9 | 32.6 ± 9.7 | 14.7 ± 8.9 | 35.3 ± 8.7 | 33.5 ± 9.0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daunoraviciene, K.; Ziziene, J. Accuracy of Ground Reaction Force and Muscle Activation Prediction in a Child-Adapted Musculoskeletal Model. Sensors 2022, 22, 7825. https://doi.org/10.3390/s22207825
Daunoraviciene K, Ziziene J. Accuracy of Ground Reaction Force and Muscle Activation Prediction in a Child-Adapted Musculoskeletal Model. Sensors. 2022; 22(20):7825. https://doi.org/10.3390/s22207825
Chicago/Turabian StyleDaunoraviciene, Kristina, and Jurgita Ziziene. 2022. "Accuracy of Ground Reaction Force and Muscle Activation Prediction in a Child-Adapted Musculoskeletal Model" Sensors 22, no. 20: 7825. https://doi.org/10.3390/s22207825