
How Long Should GPS Recording Lengths Be to Capture the Community Mobility of An Older Clinical Population? A Parkinson’s Example

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
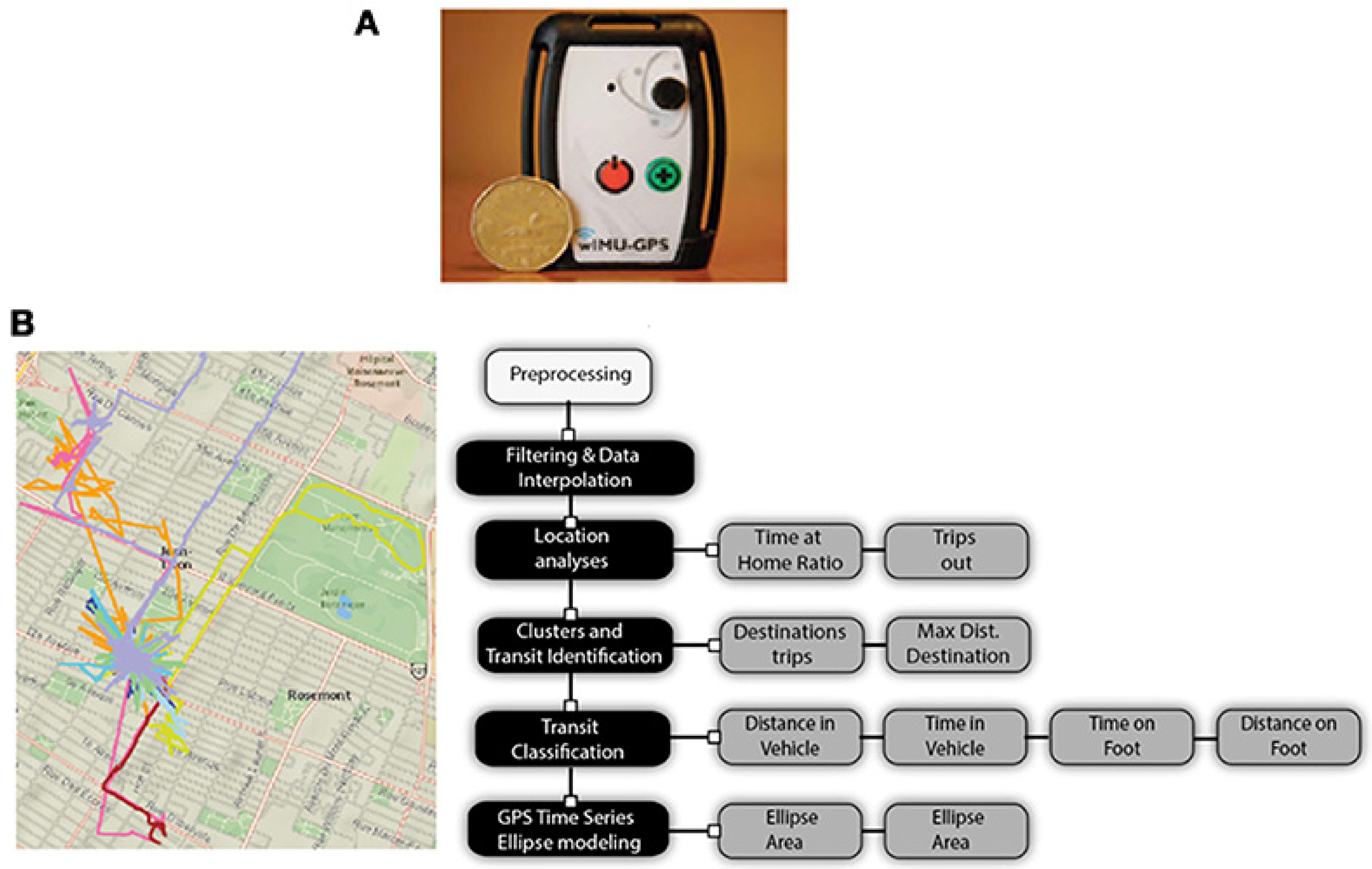
2.1. Equipment
2.2. Outcomes of Interest
2.3. Comparison Methods
2.4. Criterion and Comparison Group Selection
2.5. Criterion Group
2.6. Comparison Groups
2.7. Analysis
2.8. Subgroup Comparisons
3. Results
3.1. Demographics
3.2. Number of Days Collected
3.3. Daily and Day-to-Day Variations
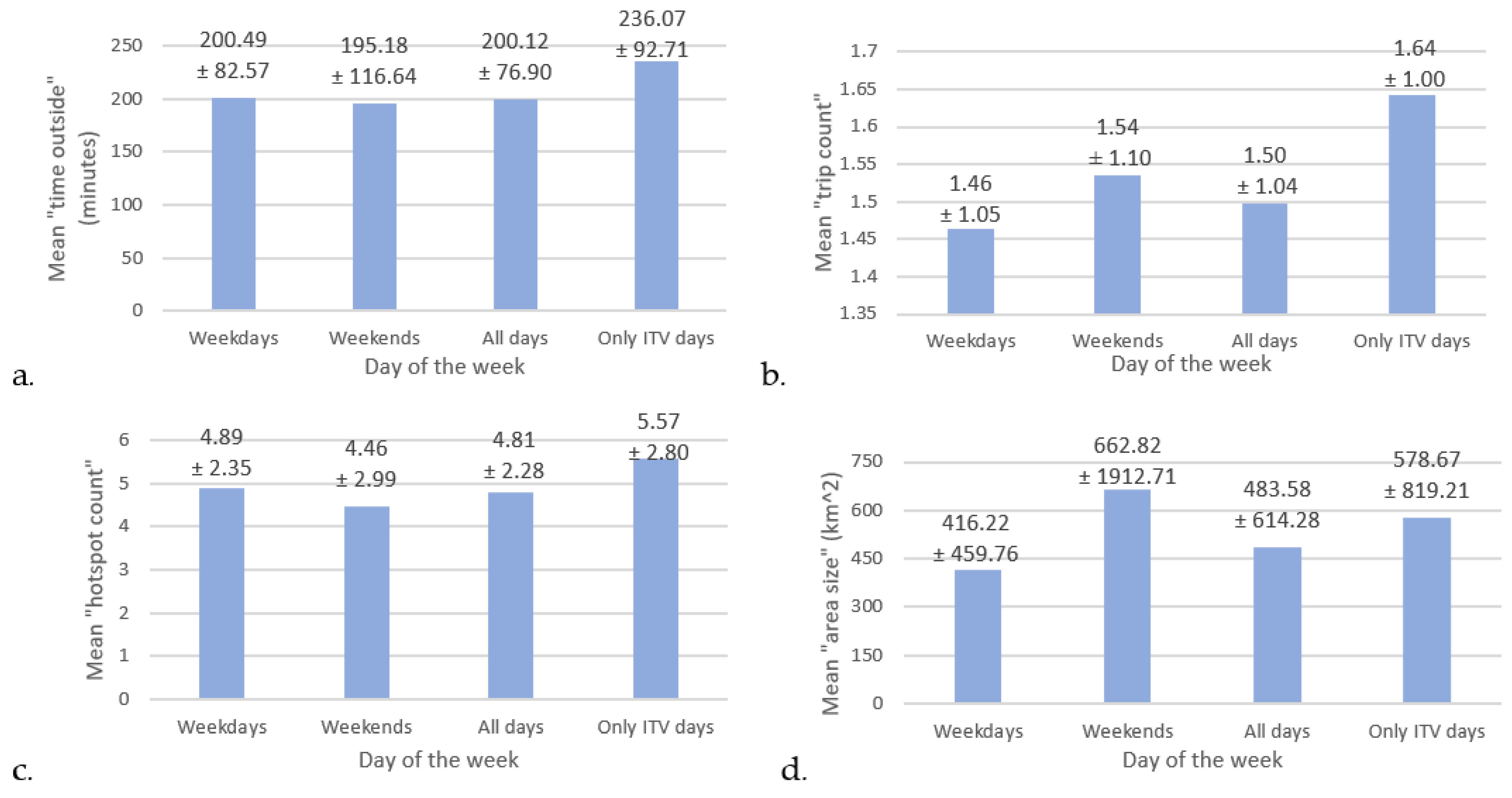
3.4. Weekday to Weekend Variations
3.5. Mean Community Mobility Outcomes
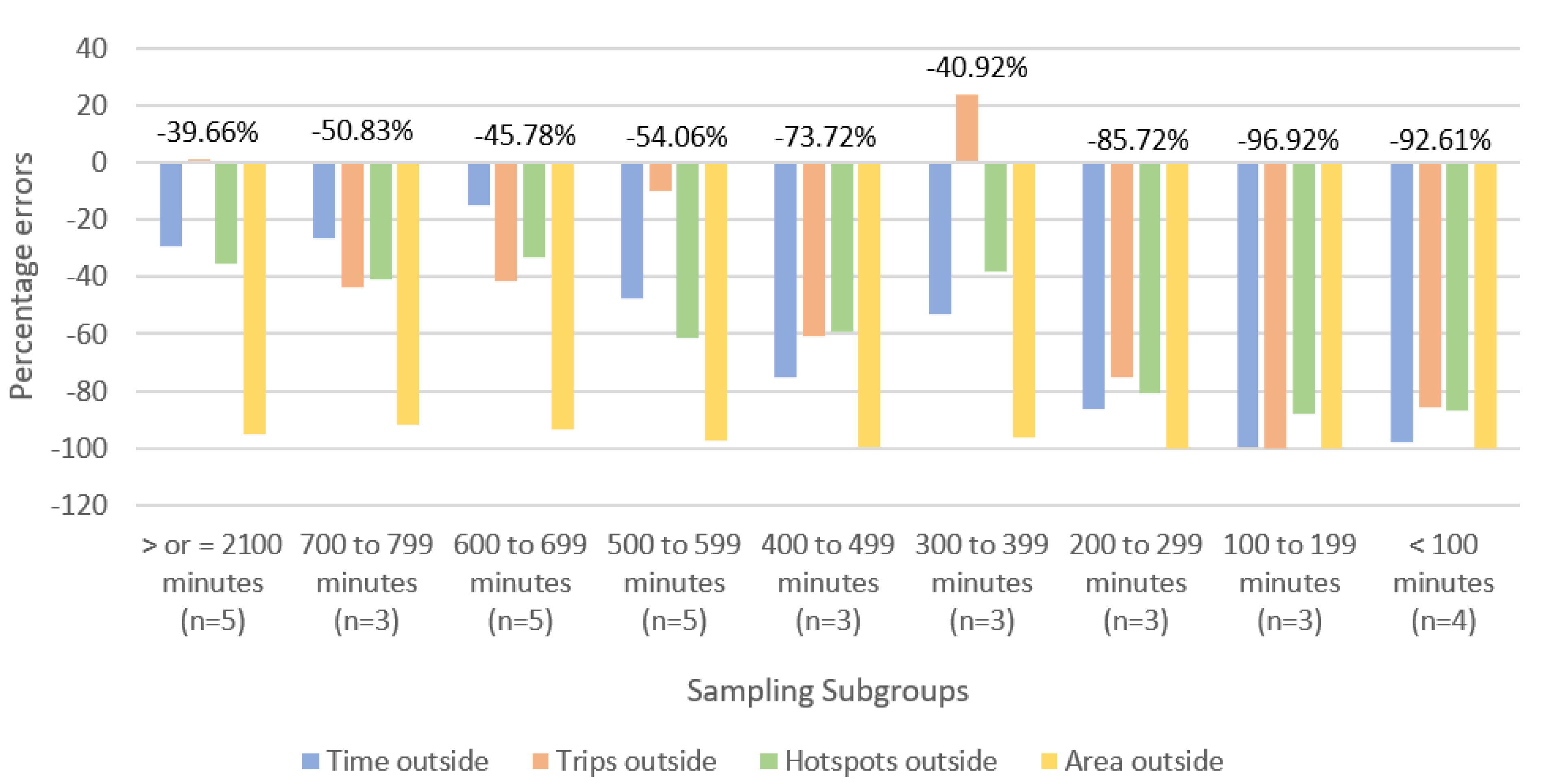
3.6. Comparing Sampling to Criterion: Absolute Comparison
3.6.1. Overall CM Outcomes
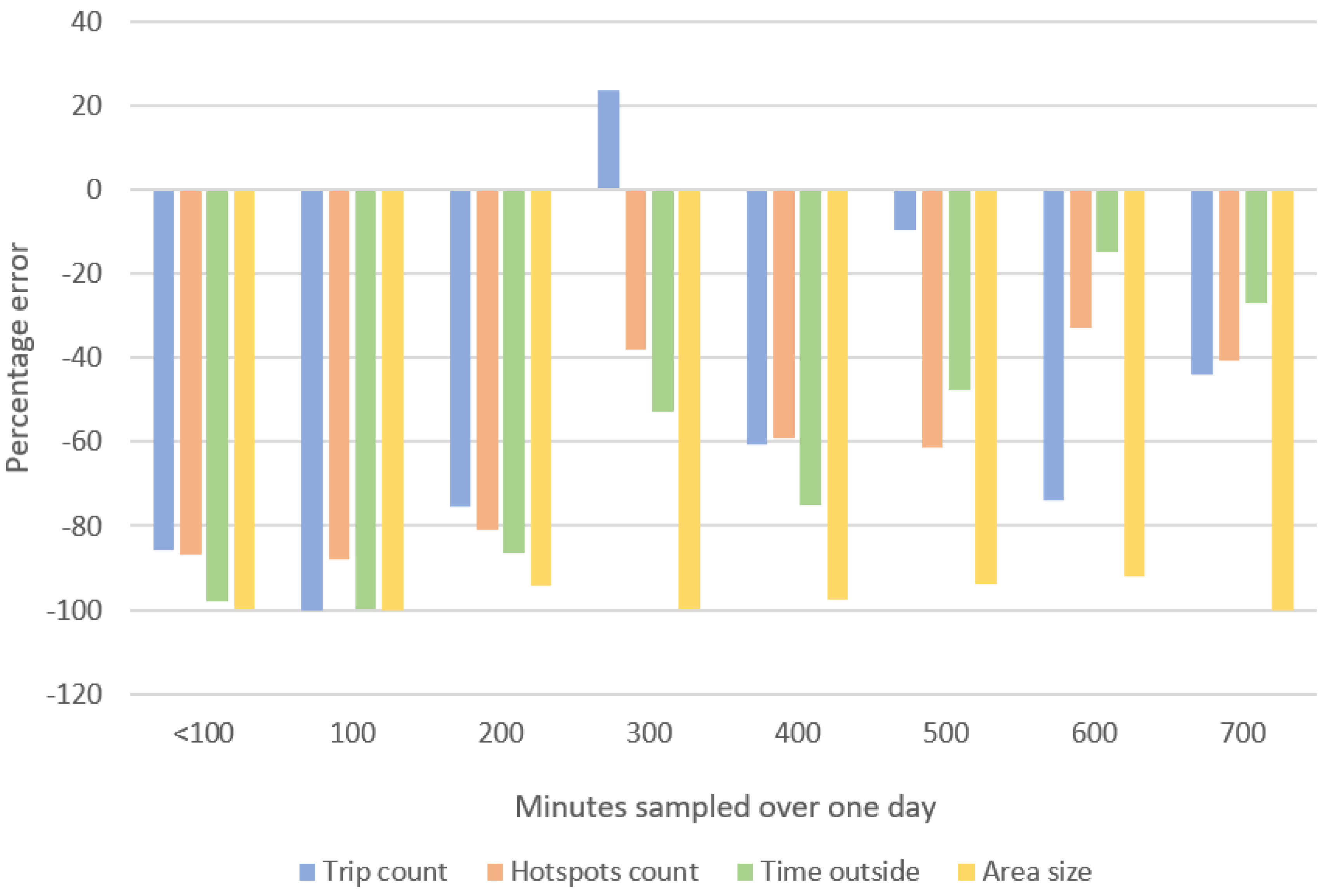
3.6.2. Specific CM Outcomes
4. Discussion
4.1. Sampling Rate by Outcome
4.2. Variability in Mobility
4.3. Recommended Recording Length
4.4. Limitations
Sampling Subgroup and Sample Size
4.5. Strengths
4.5.1. Criterion and ITV
4.5.2. Two Weeks of Sampling
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- La Grow, S.; Yeung, P.; Towers, A.; Alpass, F.; Stephens, C. The impact of mobility on quality of life among older persons. J. Aging Health 2013, 25, 723–736. [Google Scholar] [CrossRef]
- Occupational Therapy Association. Occupational Therapy Framework: Domain & Process 3rd Edition. Am. J. Occup. Ther. 2014, 68, S1–S48. [Google Scholar]
- Brusilovskiy, E.; Klein, L.A.; Townley, G.; Snethen, G.; McCormick, B.; Hiremath, S.V.; Salzer, M.S. Examining the relationship between community mobility and participation using GPS and self-report data. Soc. Sci. Med. 2020, 265, 113539. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Bherer, L.; Studenski, S.; Gopaul, K.; Oteng-Amoako, A.; Woolmore-Goodwin, S.; Stoole, P.; Wells, J.; Doherty, T.J.; Zecevic, A.A.; et al. Mobility and Cognition in Seniors. Report from the 2008 Institute of Aging (CIHR) Mobility and Cognition Workshop. Can. Geriatr. J. 2015, 18, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Albert, S.M.; Bear-Lehman, J.; Anderson, S.J. Declines in Mobility and Changes in Performance in the Instrumental Activities of Daily Living Among Mildly Disabled Community-Dwelling Older Adults. J. Gerontol. Ser. A 2014, 70, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Sheppard, K.D.; Sawyer, P.; Ritchie, C.S.; Allman, R.M.; Brown, C.J. Life-Space Mobility Predicts Nursing Home Admission Over 6 Years. J. Aging Health 2013, 25, 907–920. [Google Scholar] [CrossRef] [PubMed]
- Mackey, D.C.; Cauley, J.; Barrett-Connor, E.; Schousboe, J.T.; Cawthon, P.M.; Cummings, S.R. The Osteoporotic Fractures in Men Research Group Life-Space Mobility and Mortality in Older Men: A Prospective Cohort Study. J. Am. Geriatr. Soc. 2014, 62, 1288–1296. [Google Scholar] [CrossRef]
- Kelly, P.; Krenn, P.; Titze, S.; Stopher, P.; Foster, C. Quantifying the Difference Between Self-Reported and Global Positioning Systems-Measured Journey Durations: A Systematic Review. Transp. Rev. 2013, 33, 443–459. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, J.A.; Winters, M.; Clarke, P.; McKay, H. Generating GPS activity spaces that shed light upon the mobility habits of older adults: A descriptive analysis. Int. J. Health Geogr. 2014, 13, 51. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, J.A.; Winters, M.; Ashe, M.C.; Clarke, P.J.; McKay, H.A. Destinations That Older Adults Experience Within Their GPS Activity Spaces. Environ. Behav. 2015, 48, 55–77. [Google Scholar] [CrossRef]
- Zhu, L.; Duval, C.; Boissy, P.; Montero-Odasso, M.; Zou, G.; Jog, M.; Speechley, M. Comparing GPS-Based Community Mobility Measures with Self-report Assessments in Older Adults with Parkinson’s Disease. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2020, 75, 2361–2370. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, W.; Aminian, K. Mobility assessment in older people: New possibilities and challenges. Eur. J. Ageing 2007, 4, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hache, G.; Lemaire, E.; Baddour, N. Development of a Wearable Mobility Monitoring System. Master’s Thesis, University of Ottawa, Ottawa, ON, Canada, 2010. [Google Scholar]
- De Bruin, E.D.; Hartmann, A.; Uebelhart, D.; Murer, K.; Zijlstra, W. Wearable systems for monitoring mobility-related activities in older people: A systematic review. Clin. Rehabil. 2008, 22, 878–895. [Google Scholar] [CrossRef]
- Boissy, P.; Blamoutier, M.; Brière, S.; Duval, C. Quantification of free-living community mobility in healthy older adults using wearable sensors. Front. Public Health 2018, 6, 216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bricka, S.; Bhat, C.R. Comparative Analysis of Global Positioning System–Based and Travel Survey–Based Data. Transp. Res. Rec. J. Transp. Res. Board 2006, 1972, 9–20. [Google Scholar] [CrossRef]
- Bricka, S.G.; Sen, S.; Paleti, R.; Bhat, C.R. An analysis of the factors influencing differences in survey-reported and GPS-recorded trips. Transp. Res. Part C Emerg. Technol. 2012, 21, 67–88. [Google Scholar] [CrossRef] [Green Version]
- Wolf, J.; Oliveira, M.; Thompson, M. Impact of Underreporting on Mileage and Travel Time Estimates: Results from Global Positioning System-Enhanced Household Travel Survey. Transp. Res. Rec. J. Transp. Res. Board 2003, 1854, 189–198. [Google Scholar] [CrossRef]
- Houston, D.; Luong, T.T.; Boarnet, M.G. Tracking daily travel; Assessing discrepancies between GPS-derived and self-reported travel patterns. Transp. Res. Part C Emerg. Technol. 2014, 48, 97–108. [Google Scholar] [CrossRef]
- Duncan, M.J.; Mummery, W.K. GIS or GPS? A Comparison of Two Methods For Assessing Route Taken During Active Transport. Am. J. Prev. Med. 2007, 33, 51–53. [Google Scholar] [CrossRef]
- Tung, J.Y.; Rose, R.V.; Gammada, E.; Lam, I.; Roy, E.A.; Black, S.E.; Poupart, P. Measuring Life Space in Older Adults with Mild-to-Moderate Alzheimer’s Disease Using Mobile Phone GPS. Gerontology 2014, 60, 154–162. [Google Scholar] [CrossRef]
- Kerr, J.; Marshall, S.; Godbole, S.; Neukam, S.; Crist, K.; Wasilenko, K.; Golshan, S.; Buchner, D. The Relationship between Outdoor Activity and Health in Older Adults Using GPS. Int. J. Environ. Res. Public Health 2012, 9, 4615–4625. [Google Scholar] [CrossRef] [Green Version]
- Krenn, P.J.; Titze, S.; Oja, P.; Jones, A.; Ogilvie, D. Use of Global Positioning Systems to Study Physical Activity and the Environment: A Systematic Review. Am. J. Prev. Med. 2011, 41, 508–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zenk, S.N.; Matthews, S.A.; Kraft, A.N.; Jones, K.K. How many days of global positioning system (GPS) monitoring do you need to measure activity space environments in health research? Health Place 2018, 51, 52–60. [Google Scholar] [CrossRef]
- Confuorto, P.; Di Martire, D.; Centolanza, G.; Iglesias, R.; Mallorqui, J.J.; Novellino, A.; Plank, S.; Ramondini, M.; Thuro, K.; Calcaterra, D. Post-failure evolution analysis of a rainfall-triggered landslide by multi-temporal interferometry SAR approaches integrated with geotechnical analysis. Remote Sens. Environ. 2017, 188, 51–72. [Google Scholar] [CrossRef]
- Shen, L.; Stopher, P.R. Review of GPS Travel Survey and GPS Data-Processing Methods. Transp. Rev. 2014, 34, 316–334. [Google Scholar] [CrossRef]
- Wu, J.; Jiang, C.; Jaimes, G.; Bartell, S.; Dang, A.; Baker, D.; Delfino, R.J. Travel patterns during pregnancy: Comparison between Global Positioning System (GPS) tracking and questionnaire data. Environ. Health 2013, 12, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webber, S.C.; Porter, M.M. Monitoring mobility in older adults using global positioning system (GPS) watches and accelerometers: A feasibility study. J. Aging Phys. Act. 2009, 17, 455–467. [Google Scholar] [CrossRef]
- Gell, N.M.; Rosenberg, D.E.; Carlson, J.; Kerr, J.; Belza, B. Built environment attributes related to GPS measured active trips in mid-life and older adults with mobility disabilities. Disabil. Health J. 2014, 8, 290–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boissy, P.; Brière, S.; Hamel, M.; Jog, M.; Speechley, M.; Karelis, A.; Frank, J.; Vincent, C.; Edwards, R.; Duval, C. Wireless inertial measurement unit with GPS (WIMU-GPS) Wearable monitoring platform for ecological assessment of lifespace and mobility in aging and disease. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 5815–5819. [Google Scholar] [CrossRef]
- Schenk, A.K.; Witbrodt, B.C.; Hoarty, C.A.; Carlson, R.H., Jr.; Goulding, E.H.; Potter, J.F.; Bonasera, S.J. Cellular Telephones Measure Activity and Lifespace in Community-Dwelling Adults: Proof of Principle. J. Am. Geriatr. Soc. 2011, 59, 345–352. [Google Scholar] [CrossRef]
- Patla, A.E.; Shumway-Cook, A. Dimensions of Mobility: Defining the Complexity and Difficulty Associated with Community Mobility. J. Aging Phys. Act. 1999, 7, 7–19. [Google Scholar] [CrossRef]
- Webber, M.S.C.; Porter, M.M.; Menec, V.H. Mobility in Older Adults: A Comprehensive Framework. Gerontologist 2010, 50, 443–450. [Google Scholar] [CrossRef] [Green Version]
- Davis, M.G.; Fox, K.R.; Hillsdon, M.; Coulson, J.C.; Sharp, D.J.; Stathi, A.; Thompson, J.L. Getting out and about in older adults: The nature of daily trips and their association with objectively assessed physical activity. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 116. [Google Scholar] [CrossRef] [Green Version]
- Clarke, P.; Hirsch, J.A.; Melendez, R.; Winters, M.; Gould, J.S.; Ashe, M.; Furst, S.; McKay, H. Snow and Rain Modify Neighbourhood Walkability for Older Adults. Can. J. Aging 2017, 36, 159–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prescott, M.; Miller, W.C.; Routhier, F.; Ben Mortenson, W. Factors affecting the activity spaces of people who use mobility devices to get around the community. Health Place 2020, 64, 102375. [Google Scholar] [CrossRef] [PubMed]
- Hino, K.; Lee, J.S.; Asami, Y. Interaction effect of neighborhood walkability and season on adults’ step count. J. Transp. Health 2021, 20, 101027. [Google Scholar] [CrossRef]
- Satariano, W.A.; Kealey, M.; Hubbard, A.; Kurtovich, M.E.; Ivey, S.L.; Bayles, C.M.; Hunter, M.R.H.; Prohaska, T.R. Mobility Disability in Older Adults: At the Intersection of People and Places. Gerontologist 2014, 56, 525–534. [Google Scholar] [CrossRef] [Green Version]
- Zenk, S.N.; Schulz, A.J.; Odoms-Young, A.M.; Wilbur, J.; Matthews, S.; Gamboa, C.; Wegrzyn, L.R.; Hobson, S.; Stokes, C. Feasibility of Using Global Positioning Systems (GPS) With Diverse Urban Adults: Before and After Data on Perceived Acceptability, Barriers, and Ease of Use. J. Phys. Act. Health 2012, 9, 924–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Measuring Day-to-Day Variability in Travel Behavior Using GPS Data. U.S. Department of Transportation Federal Highway Administration Website. Updated on 13 July 2016. Available online: https://www.fhwa.dot.gov/ohim/gps/travel_char.htm (accessed on 1 September 2016).
- Hendrickson, C.C.; Mann, W.C. Changes over time in community mobility of elders with disabilities. Phys. Occup. Ther. Geriatr. 2005, 23, 75–89. [Google Scholar] [CrossRef]
- Fristedt, S.; Dahl, A.K.; Wretstrand, A.; Björklund, A.; Falkmer, T. Changes in Community Mobility in Older Men and Women. A 13-Year Prospective Study. PLoS ONE 2014, 9, e87827. [Google Scholar] [CrossRef] [Green Version]
- Tiainen, K.; Raitanen, J.; Vaara, E.; Hervonen, A.; Jylhä, M. Longitudinal changes in mobility among nonagenarians: The Vitality 90+ Study. BMC Geriatr. 2015, 15, 124. [Google Scholar] [CrossRef] [Green Version]
- Hart, T.L.; Ainsworth, B.E.; Tudor-Locke, C. Objective and Subjective Measures of Sedentary Behavior and Physical Activity. Med. Sci. Sports Exerc. 2011, 43, 449–456. [Google Scholar] [CrossRef]
- Trost, S.G.; Pate, R.R.; Freedson, P.S.; Sallis, J.F.; Taylor, W.C. Using objective physical activity measures with youth: How many days of monitoring are needed? Med. Sci. Sport Exerc. 2000, 32, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Bouça-Machado, R.; Maetzler, W.; Ferreira, J.J. What is Functional Mobility Applied to Parkinson’s Disease? J. Park. Dis. 2018, 8, 121–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, C.; Lindström, B.; Forsgren, L.; Johansson, G.M. Balance and mobility in patients with newly diagnosed Parkinson’s disease—A five-year follow-up of a cohort in northern Sweden. Disabil. Rehabil. 2018, 42, 770–778. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criterion Participants (n = 14) | All Participants (n = 56) | |
|---|---|---|
| Demographics covariates | Mean ± s.d.; n (range or %) | |
| Age (years) | 69.2 ± 6.5 (57–79) | 67.1 ± 6.3 (55–79) |
| Sex | ||
| Male | 8 (57.1%) | 39 (69.6%) |
| Female | 6 (42.9%) | 17 (30.4%) |
| Marital status | ||
| Unmarried/widowed/ | 6 (42.9%) | |
| separated | 8 (57.1%) | 7 (12.5%) |
| Married/common law | 49 (84.4%) | |
| Employment status | Fully retired = 12 (85.7%) | Fully retired = 47 (83.9%) |
| Partial or full employment = 2 (14.3%) | Partial or full employment = 9 (16.1%) | |
| Residential setting | Urban = 5 (35.7%) | Urban = 12 (21.4%) |
| Suburban = 1 (7.1%) | Suburban = 15 (26.8%) | |
| Rural, in town = 5 (35.7%) | Rural, in town = 19 (33.9%) | |
| Rural, outside of town = 3 (21.4%) | Rural, outside of town = 10 (17.9%) | |
| Living situation | Alone = 5 (35.7%) | Alone = 8 (14.3%) |
| With family/friends = 9 (64.3%) | With family/friends = 48 (85.7%) | |
| Driving status | Drives = 14 (100%) | Drives = 51 (91.1%) |
| Does not drive = 0 (0%) | Does not drive = 5 (8.9%) | |
| MoCA | 26.6 ± 2.5 (23–30) | 25.3 ± 3.0 (18–30) |
| Time since PD diagnosis (years) | 5.4 ± 4.0 (<1–14) | 6.4 ± 5.6 (<1–30) |
| Impact of PD on overall quality of life (PDQ-39 scores; 0 = no impact, 100 = total impairment) | 13.9 ± 15.8 (2.1–64.7) | 20.8 ± 12.4 (1.8–51.4) |
| CM Outcomes | All Non-ITV Days | ITV Days | ||
|---|---|---|---|---|
| Mobility Outcomes | Mean | Coefficient of Variation (s.d./mean∗100) | Mean | Coefficient of Variation of the ITV (s.d./mean∗100) |
| Time outside in minutes (range) | 119.95 ± 135.34 (0.7–465.02) | 112.83% | 244.9 ± 169.95 (0.03–712.47) | 69.40% |
| Trip count (range) | 1.19 ± 1.49 (0 to 8) | 83.31% | 1.68 ± 1.40 (0–7) | 83.33% |
| Hotspot count (range) | 3.19 ± 2.93 (0 to 16) | 78.30% | 5.75 ± 4.50 (1–27) | 78.26% |
| Area size in km2 (range) | 182.68 ± 732.12 (0 to 4241.77) | 400.77% | 671.63 ± 1758.4 (0–10,250) | 261.81% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, L.; Boissy, P.; Duval, C.; Zou, G.; Jog, M.; Montero-Odasso, M.; Speechley, M. How Long Should GPS Recording Lengths Be to Capture the Community Mobility of An Older Clinical Population? A Parkinson’s Example. Sensors 2022, 22, 563. https://doi.org/10.3390/s22020563
Zhu L, Boissy P, Duval C, Zou G, Jog M, Montero-Odasso M, Speechley M. How Long Should GPS Recording Lengths Be to Capture the Community Mobility of An Older Clinical Population? A Parkinson’s Example. Sensors. 2022; 22(2):563. https://doi.org/10.3390/s22020563
Chicago/Turabian StyleZhu, Lynn, Patrick Boissy, Christian Duval, Guangyong Zou, Mandar Jog, Manuel Montero-Odasso, and Mark Speechley. 2022. "How Long Should GPS Recording Lengths Be to Capture the Community Mobility of An Older Clinical Population? A Parkinson’s Example" Sensors 22, no. 2: 563. https://doi.org/10.3390/s22020563