
Hybrid Detection of Breast Abnormalities Based on Contrast Agents: Introducing a Proof of Concept from a Physics Perspective

Abstract
:1. Introduction
2. Materials and Methods
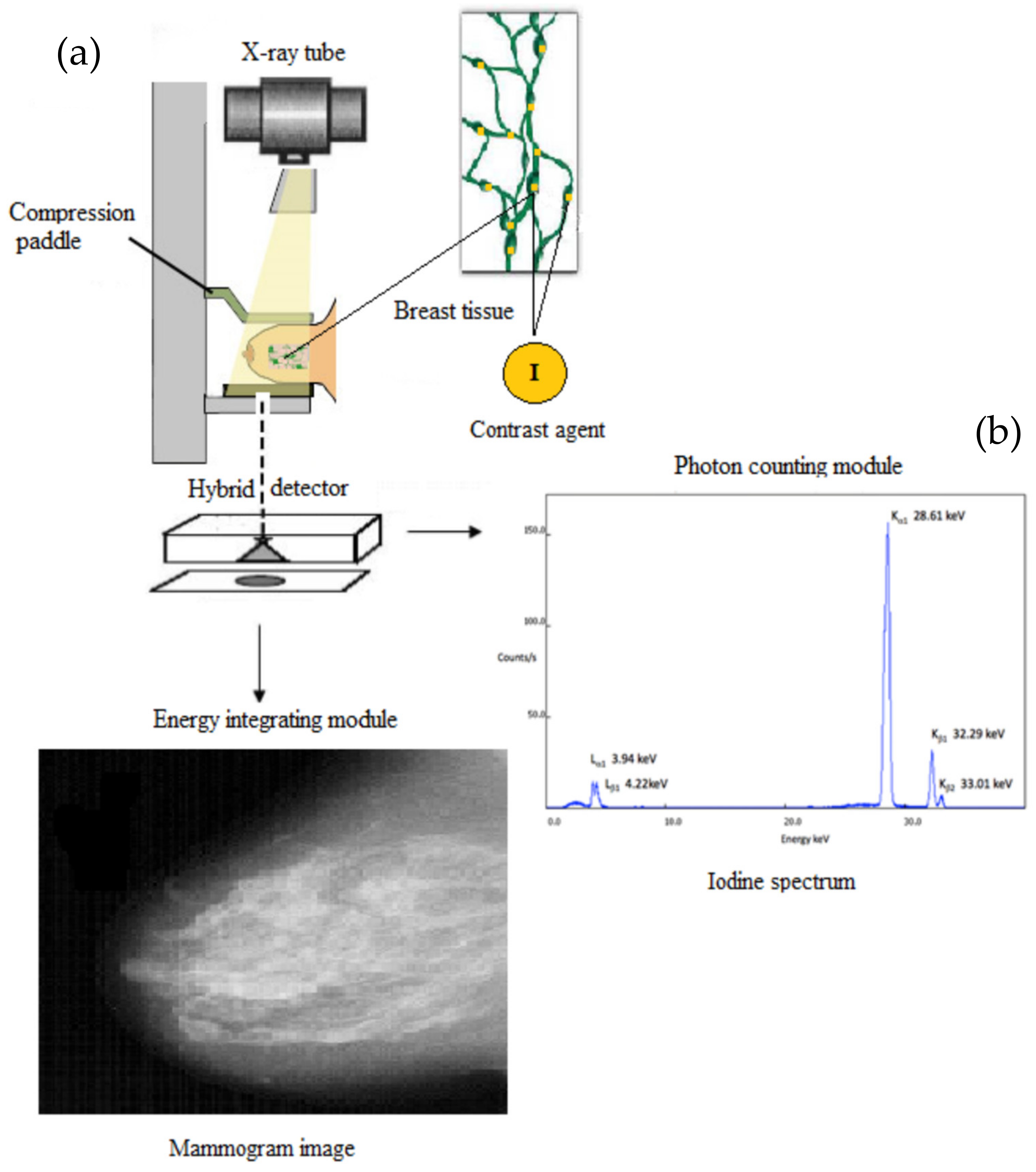
2.1. The Hybrid Detective Imaging System
2.2. The Role of the Contrast Agent as “Fingerprint” Tissue Abnormality
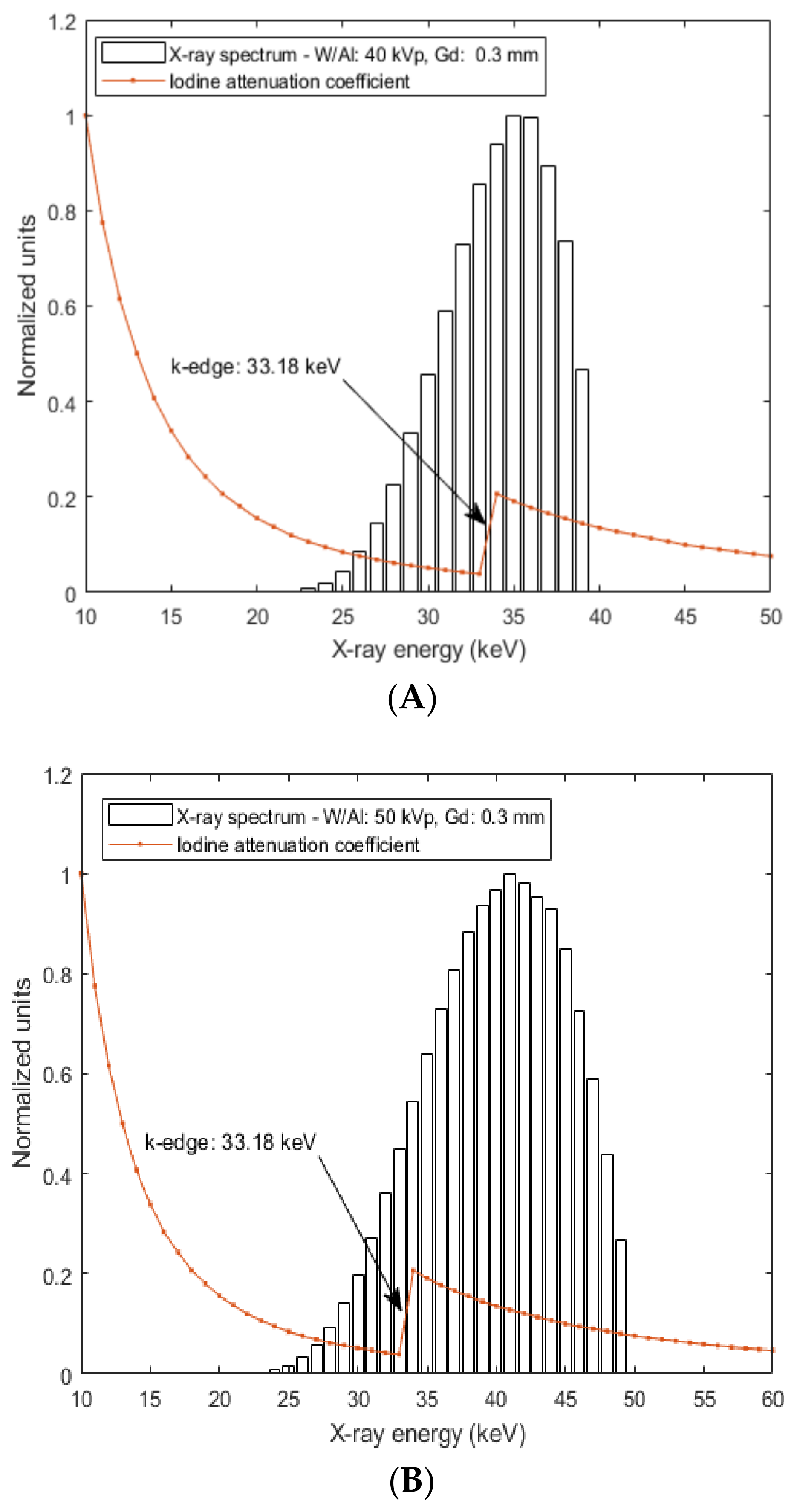
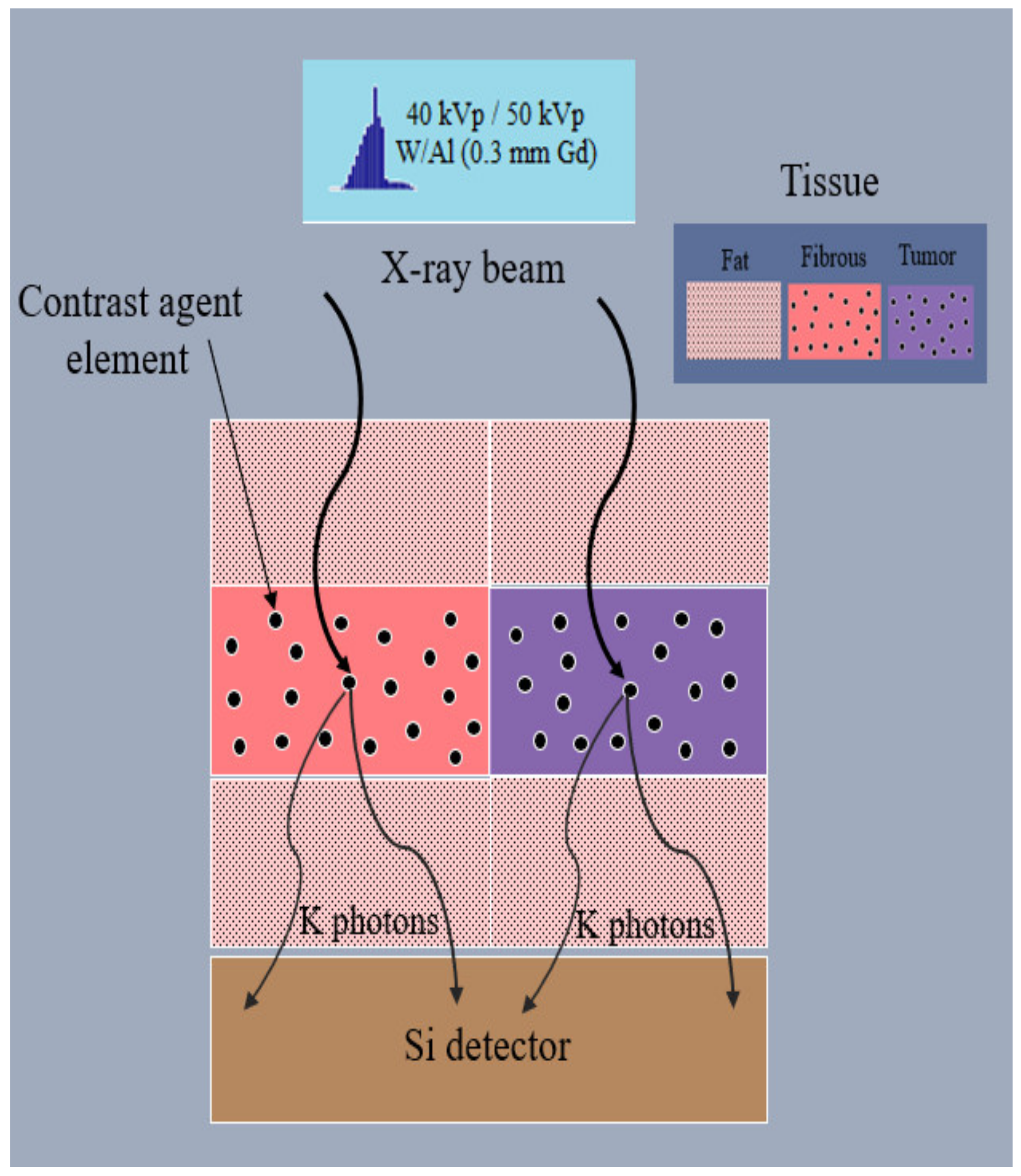
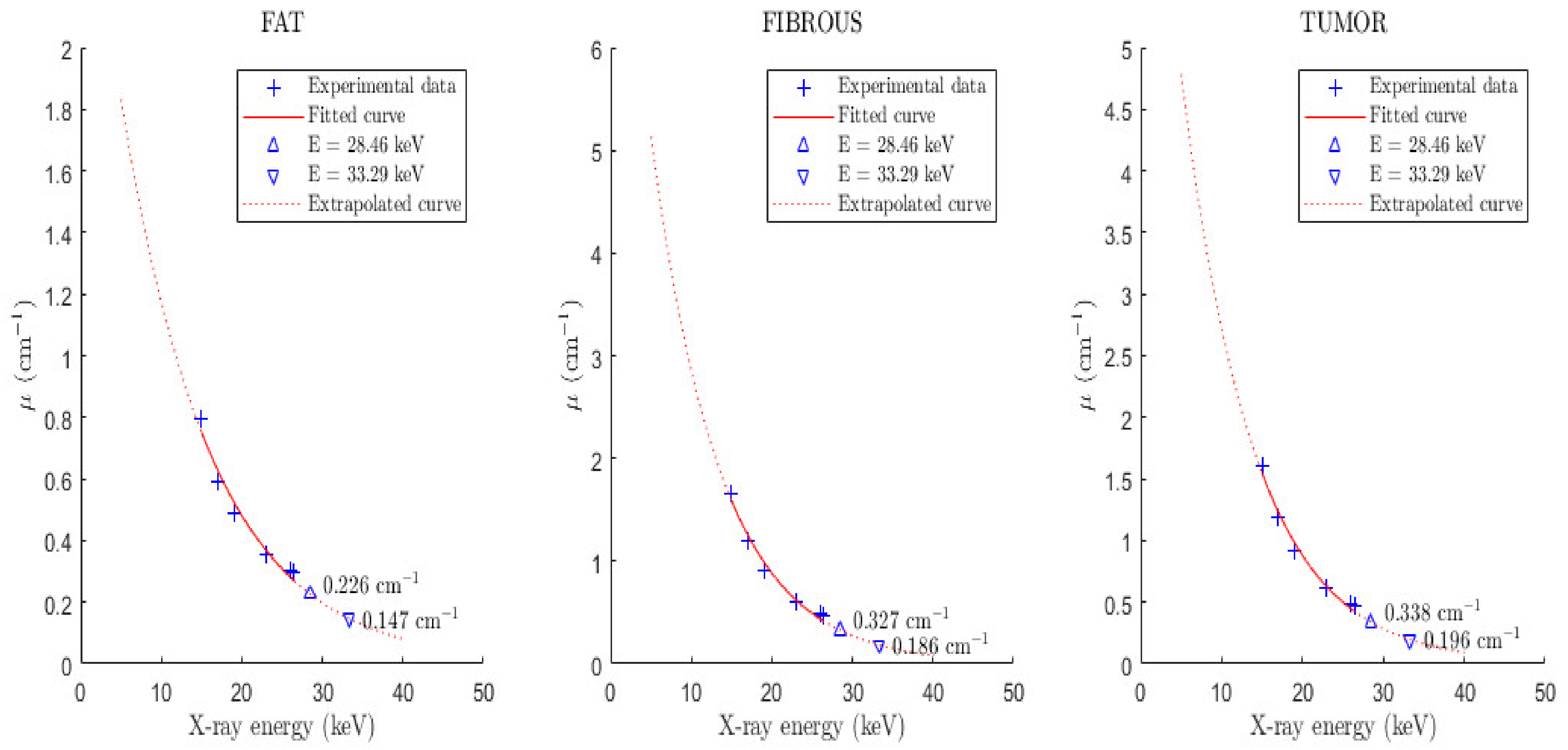
2.3. Monte Carlo Modeling of K-X-rays Emitted by the Contrast Agent
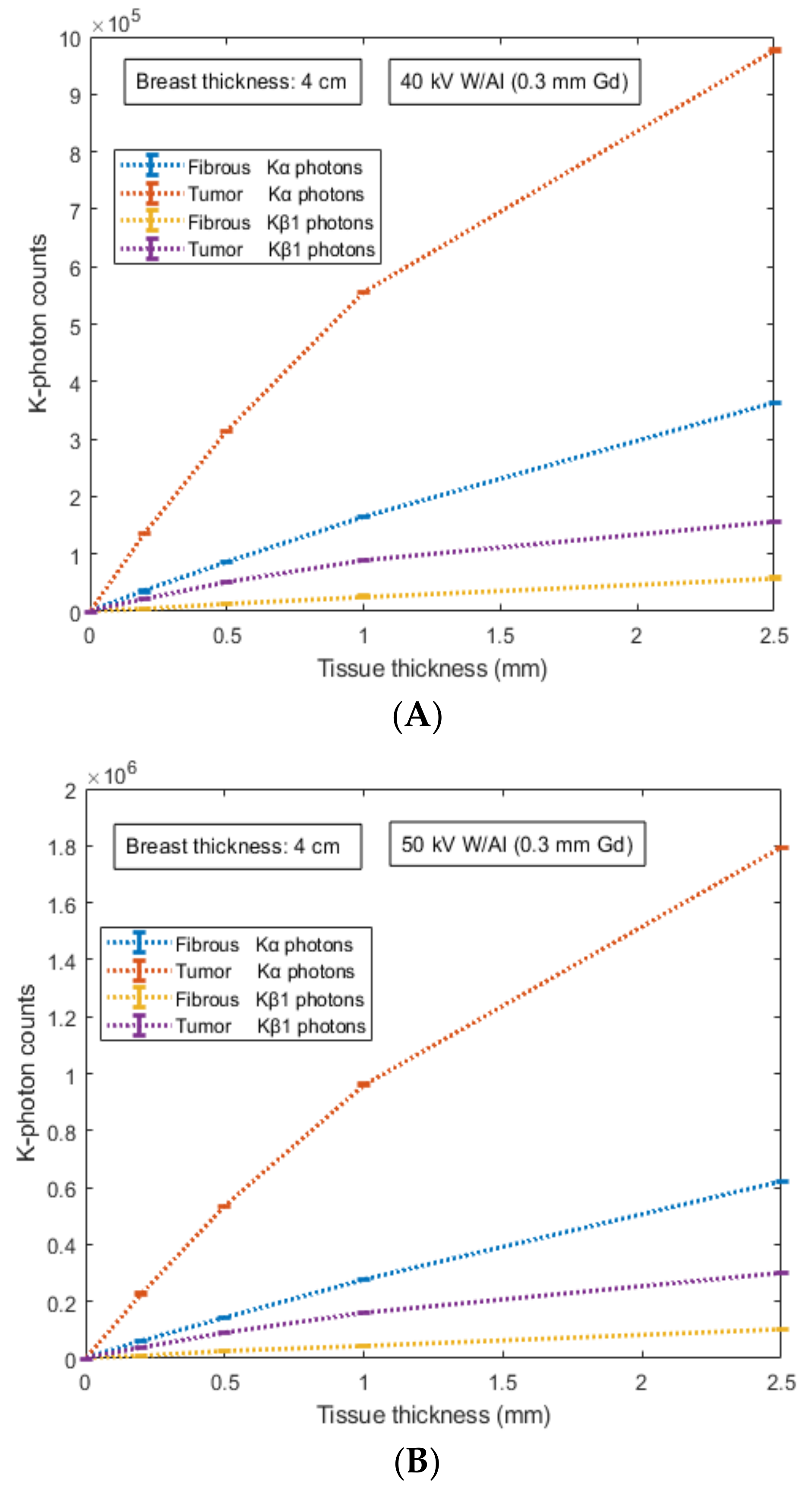
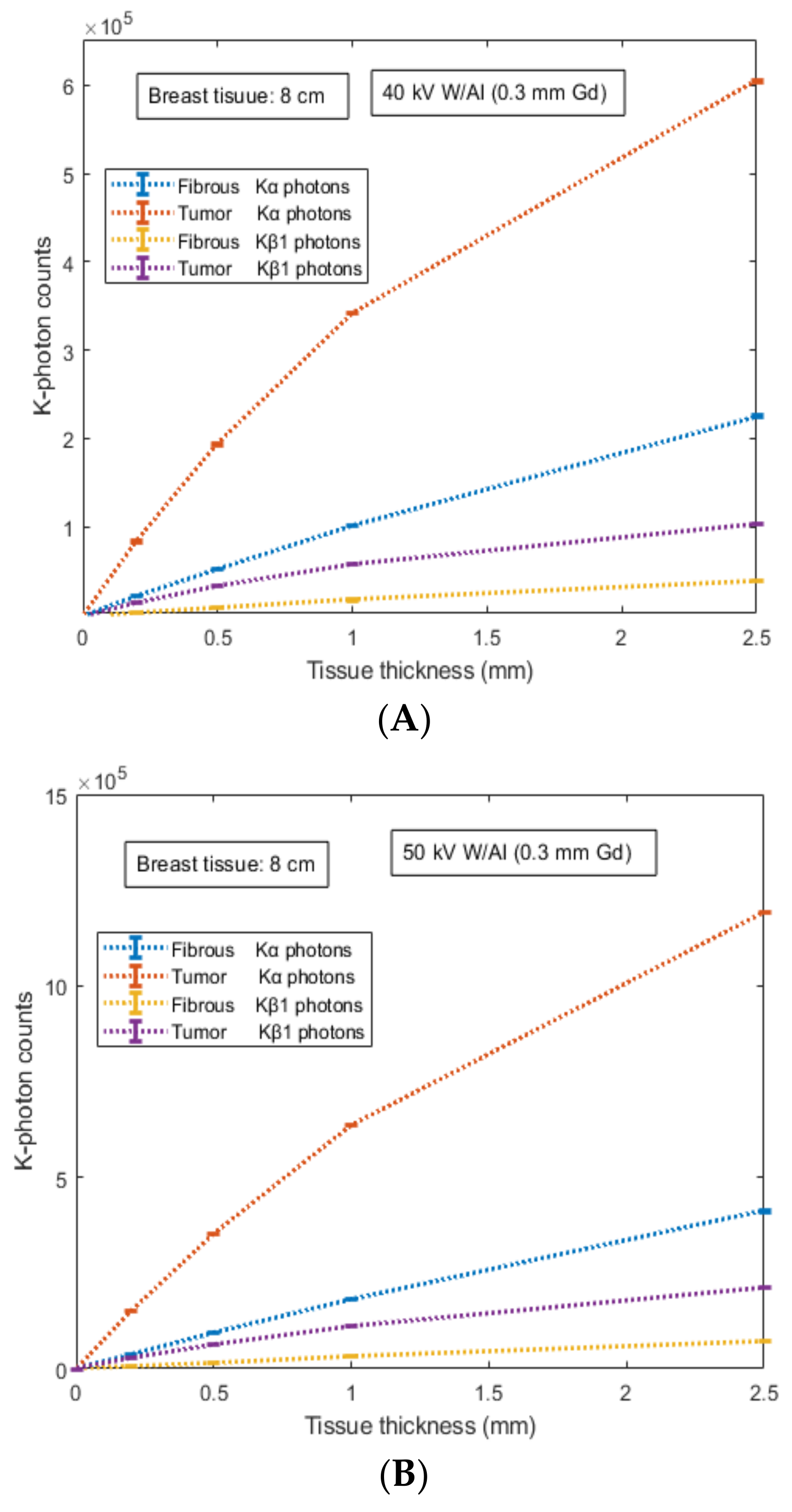
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fass, L. Imaging and cancer: A review. Mol. Oncol. 2008, 2, 115–152. [Google Scholar] [CrossRef] [PubMed]
- Dance, D.R.; Christofides, S.; Maidment, A.D.A.; McLean, I.D.; Ng, K.H. Diagnostic Radiology Physics; International Atomic Energy Agency (IAEA): Vienna, Austria, 2014. [Google Scholar]
- Cherry, S. Multimodality imaging: Beyond PET/CT and SPECT/CT. Semin. Nucl. Med. 2009, 39, 348–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huellner, M.W.; Appenzeller, P.; Kuhn, F.P.; Husmann, L.; Pietsch, C.M.; Burger, I.A.; Porto, M.; Delso, G.; Schulthess, G.K.; Veit-Haibach, P. Whole-body nonenhanced PET/MR versus PET/CT in the staging and restaging of cancers: Preliminary observations. Radiology 2014, 273, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.; Siegel, R.; Jemal, A. Global Cancer Facts & Figures 2018, 4th ed.; American Cancer Society: Atlanta, GA, USA, 2018. [Google Scholar]
- Chen, Y.-C.; Prabhu, K.S.; Das, A.; Mastro, A.M. Dietary selenium supplementation modifies breast tumor growth and metastasis. Int. J. Cancer. 2013, 133, 2054–2064. [Google Scholar] [CrossRef] [PubMed]
- The Swedish Organized Service Screening Evaluation Group. Reduction in breast cancer mortality from organized service screening with mammography: 1. Further confirmation with extended data. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Thurfjell, E.L.; Lindgren, J.A. Breast cancer survival rates with mammographic screening: Similar favorable survival rates for women younger and those older than 50 years. Radiology 1996, 201, 421–426. [Google Scholar] [CrossRef]
- Durduran, T.; Choe, R.; Baker, W.B.; Yodh, A.G. Diffuse optics for tissue monitoring and tomography. Rep. Prog. Phys. 2010, 73, 076701. [Google Scholar] [CrossRef] [Green Version]
- Gibson, A.P.; Hebden, J.C.; Arridge, S.R. Recent advances in diffuse optical imaging. Phys. Med. Biol. 2005, 50, R1–R43. [Google Scholar] [CrossRef]
- Kerlikowske, K.; Barclay, J.; Grady, D.; Sickles, E.A.; Ernster, V. Comparison of risk factors for ductal carcinoma in situ and invasive breast cancer. J. Natl. Cancer Inst. 1997, 89, 76–82. [Google Scholar] [CrossRef] [Green Version]
- Lucassen, A.; Watson, E.; Eccles, D. Advice about mammography for a young woman with a family history of breast cancer. Br. Med. J. 2004, 322, 1040–1042. [Google Scholar] [CrossRef]
- Carney, P.A.; Miglioretti, D.L.; Yankaskas, B.C.; Kerlikowske, K.; Rosenberg, R.; Rutter, C.M.; Geller, B.M.; Abraham, L.A.; Taplin, S.H.; Dignan, M.; et al. Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography. Ann. Intern. Med. 2003, 138, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Boyd, N.F.; Guo, H.; Martin, L.J.; Sun, L.; Stone, J.; Fishell, E.; Jong, R.A.; Hislop, G.; Chiarelli, A.; Minkin, S.; et al. Mammographic density and the risk and detection of breast cancer. N. Engl. J. Med. 2007, 356, 227–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warner, E.; Plewes, D.B.; Shumak, R.S.; Catzavelos, G.C.; Di Prospero, L.S.; Yaffe, M.J.; Goel, V.; Ramsay, E.; Chart, P.L.; Cole, D.E.; et al. Comparison of breast magnetic resonance imaging, mammography and ultrasound for surveillance of women at high risk for hereditary breast cancer. J. Clin. Oncol. 2001, 19, 3524–3531. [Google Scholar] [CrossRef] [PubMed]
- Lobbes, M.B.I.; Smidt, M.L.; Houwers, J.; Tjan-Heijnen, V.C.; Wildberger, J.E. Contrast enhanced mammography: Techniques, current results, and potential indications. Clin. Radiol. 2013, 68, 935–944. [Google Scholar] [CrossRef]
- Punnoose, J.; Xu, J.; Sisniega, A.; Zbijewski, W.; Siewerdsen, J.H. Technical Note: SPEKTR 3.0—A computational tool for x-ray spectrum modeling and analysis. Med. Phys. 2016, 43, 4711–4717. [Google Scholar] [CrossRef]
- Nowotny, R. XMuDat: Photon Attenuation Data on PC; IAEA-NDS-195; International Atomic Energy Agency: Vienna, Austria, 1998; Available online: https://www-nds.iaea.org/publications/iaea-nds/iaea-nds-0195.htm (accessed on 31 August 2022).
- Jochelson, M.S.; Dershaw, D.D.; Sung, J.S.; Heerdt, A.S.; Thornton, C.; Moskowitz, C.S.; Ferrara, J.; Morris, E.A. Bilateral contrast-enhanced dual-energy digital mammography: Feasibility and comparison with conventional digital mammography and MR imaging in women with known breast carcinoma. Radiology 2013, 266, 743–751. [Google Scholar] [CrossRef] [Green Version]
- Wilson, C.B.J.H.; Lammertsma, A.A.; McKenzie, C.G.; Sikora, K.; Jones, T. Measurements of blood flow and exchanging water space in breast tumors using positron emission tomography: A rapid and noninvasive dynamic method. Cancer Res. 1992, 52, 1592–1597. [Google Scholar]
- Cullen, D.E.; Hubbell, J.H.; Kissel, L. EPDL97 the Evaluated Data Library, ’97 version, Report UCRL-50400; LLNLL: Livermore, CA, USA, 1997. [Google Scholar]
- Hubbell, J.H.; Trehan, P.N.; Singh, N.; Chand, B.; Mehta, D.; Garg, M.L.; Garg, R.R.; Singh, S.; Puri, S. A Review, Bibliography, and Tabulation of K, L, and Higher Atomic Shell X-ray Fluorescence Yields. J. Phys. Chem. Ref. Data 1994, 23, 339–364. [Google Scholar] [CrossRef]
- Chen, R.C.; Longo, R.; Rigon, L.; Zanconati, F.; De Pellegrin, A.; Arfelli, F.; Dreossi, D.; Menk, R.-H.; Vallazza, E.; Xiao, T.Q.; et al. Measurement of the linear attenuation coefficients of breast tissues by synchrotron radiation computed tomography. Phy. Med. Biol. 2010, 55, 4993–5005. [Google Scholar] [CrossRef]
- Blanchota, G.; Chmeissania, M.; Diazb, A.; Diazb, F.; Fernandezc, J.; Garciab, E.; Garciaa, J.; Kainbergerd, F.; Lozanoe, M.; Maiorinoa, M.; et al. Dear-Mama: A photon counting X-ray imaging project for medical applications. Nucl. Instr. Meth. A 2006, 569, 136–139. [Google Scholar] [CrossRef]
- Bor, D.; Tukel, S.; Olgar, T.; Aydin, E. Variations in breast doses for an automatic mammography unit. Diagn. Interv. Radiol. 2008, 14, 122–126. [Google Scholar] [PubMed]
- IAEA-TECDOC-1447; Optimization of the Radiological Protection of Patients: Image Quality and Dose in Mammography (Coordinated Research in Europe). IAEA: Vienna, Austria, May 2005.
- Abbene, L.; La Manna, A.; Fauci, F.; Gerardi, G.; Stumbo, S.; Raso, G. X-ray spectroscopy and dosimetry with a portable CdTe device. Nucl. Instr. Meth. A 2007, 571, 373–377. [Google Scholar] [CrossRef]
- Liaparinos, P.; Bliznakova, K. Monte Carlo performance on the x-ray converter thickness in digital mammography using software breast models. Med. Phys. 2012, 39, 6638–6651. [Google Scholar] [CrossRef] [PubMed]
- Hoheisel, M. Review of medical imaging with emphasis on X-ray detectors. Nucl. Instr. Meth. A 2006, 563, 215–224. [Google Scholar] [CrossRef]
- Liaparinos, P. LIGHTAWE—Case studies of LIGHT spreAd in poWder materials: A montE carlo simulation tool for research and educational purposes. Appl. Phys. B 2019, 125, 151. [Google Scholar] [CrossRef]
- Liaparinos, P.F. Optical diffusion performance of nanophosphor-based materials for use in medical imaging. J. Biomed. Opt. 2012, 17, 126013. [Google Scholar] [CrossRef]
- Dainty, J.C.; Shaw, R. Image Science; Academic: New York, NY, USA, 1974. [Google Scholar] [CrossRef]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef]
- Procza, S.; Avilab, C.; Feya, J.; Roqueb, G.; Schuetza, M.; Hamannc, E. X-ray and gamma imaging with Medipix and Timepix detectors in medical research. Radiat. Meas. 2019, 127, 106104. [Google Scholar] [CrossRef]
- Quarati, F.; O’Shea, V.; Smith, K. Image quality of medipix2 assemblies with silicon detectors of two different thicknesses. Nucl. Instr. Meth. A 2005, 546, 42–45. [Google Scholar] [CrossRef]
- Leng, S.; Bruesewitz, M.; Tao, S.; Rajendran, K.; Halaweish, A.F.; Campeau, N.G.; Fletcher, J.G.; McCollough, C.H. Photon-counting Detector CT: System Design and Clinical Applications of an Emerging Technology. Radiographics 2019, 39, 729–743. [Google Scholar] [CrossRef]
- Wang, X.; Meier, D.; Taguchi, K.; Wagenaar, D.J.; Patt, B.E.; Frey, E.C. Material separation in X-ray CT with energy resolved photon-counting detectors. Med. Phys. 2011, 38, 1534–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, V.A.; Davidson, W.D.; Melone, J.J.; O’Shea, V.; Smith, K.M.; Donohue, L.; Lea, L.; Robb, K.; Nenonen, S.; Sipila, H. Three-dimensional medipix—A new generation of X-ray detectors. IEEE Trans. Nucl. Sci. 2005, 52, 1873–1876. [Google Scholar] [CrossRef]
- Hainfeld, J.F.; Ridwan, S.M.; Stanishevskiy, Y.; Smilowitz, N.R.; Davis, J.; Smilowitz, H.M. Small, long blood half-life iodine nanoparticle for vascular and tumor imaging. Sci. Rep. 2018, 8, 13803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, R.S.; Samei, E.; Lo, J.Y.; Baker, J.A. Can Compression Be Reduced for Breast Tomosynthesis? Monte Carlo Study on Mass and Microcalcification Conspicuity in Tomosynthesis. Radiology 2009, 251, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Poulos, A.; McLean, D.; Rickard, M.; Heard, R. Breast compression in mammography: How much is enough? Australas. Radiol. 2003, 47, 121–126. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Contrast Agent-Iodine (I) | |
|---|---|
| K-edge (keV) | 33.18 |
| Fluorescent yield ωKα | 0.841 a |
| X-ray energy (keV) Κα | 28.46 |
| Fluorescent yield ωKβ | 0.900 b |
| X-ray energy (keV) Κβ1 | 33.29 |
| Probability of KL relaxation ξKL | 0.820 c |
| Κα Produced | Κα Emitted | Κβ1 Produced | Κβ1 Emitted | |
|---|---|---|---|---|
| Tissue thickness (mm) | 40 kV W/Al (0.3 mm Gd) | |||
| ESAK 10 mGy: 154,325,927 ± 2361 X-ray photons | ||||
| Fibrous tissue | ||||
| 0.20 | 919,530 ± 1113 | 180,213 ± 91 | 216,270 ± 585 | 46,657 ± 134 |
| 0.50 | 2,259,247 ± 303 | 439,864 ± 318 | 531,387 ± 314 | 113,560 ± 243 |
| 1.00 | 4,390,417 ± 1123 | 845,360 ± 1441 | 1,031,301 ± 689 | 218,528 ± 210 |
| 2.50 | 10,069,414 ± 6029 | 1,871,363 ± 662 | 2,364,725 ± 577 | 485,761 ± 558 |
| Tumor tissue | ||||
| 0.20 | 3,554,987 ± 1547 | 696,311 ± 525 | 834,560 ± 1110 | 179,404 ± 303 |
| 0.50 | 8,288,675 ± 1295 | 1,613,178 ± 176 | 1,946,062 ± 160 | 416,505 ± 316 |
| 1.00 | 14,825,168 ± 5152 | 2,847,935 ± 487 | 3,480,900 ± 1381 | 735,349 ± 988 |
| 2.50 | 27,282,049 ± 8256 | 5,018,295 ± 1782 | 6,411,497 ± 3725 | 1,304,219 ± 1618 |
| 50 kV W/Al (0.3 mm Gd) | ||||
| ESAK 10 mGy: 208,131,504 ± 11,054 X-ray photons | ||||
| Fibrous tissue | ||||
| 0.20 | 1,528,085 ± 950 | 299,099 ± 672 | 359,320 ± 227 | 77,464 ± 362 |
| 0.50 | 3,769,500 ± 1747 | 733,758 ± 1030 | 886,339 ± 886 | 189,812 ± 236 |
| 1.00 | 7,359,554 ± 3712 | 1,414,941 ± 742 | 1,729,163 ± 243 | 366,219 ± 397 |
| 2.50 | 17,167,289 ± 2508 | 3,193,661 ± 1358 | 4,030,857 ± 878 | 829,263 ± 962 |
| Tumor tissue | ||||
| 0.20 | 5,946,659 ± 302 | 1,164,779 ± 1396 | 1,397,721 ± 558 | 300,511 ± 824 |
| 0.50 | 14,048,481 ± 3716 | 2,734,730 ± 1064 | 3,298,319 ± 1223 | 704,555 ± 647 |
| 1.00 | 25,675,571 ± 3529 | 4,940,486 ± 3296 | 6,028,654 ± 1281 | 1,275,854 ± 751 |
| 2.50 | 49,935,784 ± 3291 | 9,208,489 ± 3261 | 11,721,499 ± 2947 | 2,390,102 ± 1366 |
| Κα Produced | Κα Emitted | Κβ1 Produced | Κβ1 Emitted | |
|---|---|---|---|---|
| Tissue thickness (mm) | 40 kV W/Al (0.3 mm Gd) | |||
| ESAK 15 mGy: 231,489,318 ± 1873 X-ray photons | ||||
| Fibrous tissue | ||||
| 0.20 | 1,086,583 ± 693 | 111,018 ± 172 | 255,284 ± 856 | 30,692 ± 133 |
| 0.50 | 2,668,106 ± 128 | 271,053 ± 131 | 626,624 ± 804 | 74,837 ± 277 |
| 1.00 | 5,182,404 ± 1631 | 521,206 ± 614 | 1,216,283 ± 1555 | 144,092 ± 164 |
| 2.50 | 11,883,820 ± 1862 | 1,158,467 ± 891 | 2,792,623 ± 849 | 322,277 ± 618 |
| Tumor tissue | ||||
| 0.20 | 4,195,170 ± 458 | 429,199 ± 132 | 985,172 ± 553 | 118,587 ± 355 |
| 0.50 | 9,782,535 ± 3045 | 995,528 ± 776 | 2,297,811 ± 1913 | 274,695 ± 243 |
| 1.00 | 17,496,435 ± 4343 | 1,758,550 ± 2252 | 4,112,562 ± 474 | 486,680 ± 484 |
| 2.50 | 32,188,347 ± 913 | 3,107,396 ± 1886 | 7,563,711 ± 3166 | 864,557 ± 604 |
| 50 kV W/Al (Gd filtration) | ||||
| ESAK 15 mGy: 312,198,595 ± 11,587 X-ray photons | ||||
| Fibrous tissue | ||||
| 0.20 | 1,927,864 ± 480 | 196,690 ± 354 | 452,256 ± 791 | 54,170 ± 116 |
| 0.50 | 4,753,395 ± 2088 | 482,327 ± 408 | 1,115,946 ± 404 | 133,064 ± 253 |
| 1.00 | 9,279,887 ± 1131 | 932,832 ± 612 | 2,180,559 ± 511 | 258,119 ± 317 |
| 2.50 | 21,657,692 ± 2070 | 2,112,970 ± 1711 | 5,086,165 ± 1837 | 586,491 ± 1310 |
| Tumor tissue | ||||
| 0.20 | 7,494,827 ± 1304 | 765,266 ± 340 | 1,761,087 ± 1369 | 211,620 ± 758 |
| 0.50 | 17,722,602 ± 6765 | 1,801,619 ± 619 | 4,165,397 ± 1660 | 497,862 ± 461 |
| 1.00 | 32,418,446 ± 9013 | 3,261,592 ± 1376 | 7,612,154 ± 2321 | 901,771 ± 1504 |
| 2.50 | 63,219,666 ± 6066 | 6,123,979 ± 417 | 14,856,997 ± 3051 | 1,704,321 ± 1617 |
| Ratio of Κα Counted | Ratio of Κβ1 Counted | Ratio of Κα Counted | Ratio of Κβ1 Counted | |
|---|---|---|---|---|
| 40 kV W/Al (0.3 mm Gd) | ||||
| Tissue thickness(mm) | Fat tissue: 4 cm | Fat tissue: 8 cm | ||
| 0.20 | 3.87 | 3.88 | 3.86 | 3.86 |
| 0.50 | 3.67 | 3.68 | 3.66 | 3.66 |
| 1.00 | 3.37 | 3.35 | 3.38 | 3.38 |
| 2.50 | 2.68 | 2.68 | 2.68 | 2.68 |
| 50 kV W/Al (0.3mm Gd) | ||||
| Fat tissue: 4 cm | Fat tissue: 8 cm | |||
| 0.20 | 3.88 | 3.85 | 3.88 | 3.87 |
| 0.50 | 3.72 | 3.72 | 3.74 | 3.75 |
| 1.00 | 3.49 | 3.48 | 3.50 | 3.48 |
| 2.50 | 2.89 | 2.89 | 2.90 | 2.90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liaparinos, P. Hybrid Detection of Breast Abnormalities Based on Contrast Agents: Introducing a Proof of Concept from a Physics Perspective. Sensors 2022, 22, 7514. https://doi.org/10.3390/s22197514
Liaparinos P. Hybrid Detection of Breast Abnormalities Based on Contrast Agents: Introducing a Proof of Concept from a Physics Perspective. Sensors. 2022; 22(19):7514. https://doi.org/10.3390/s22197514
Chicago/Turabian StyleLiaparinos, Panagiotis. 2022. "Hybrid Detection of Breast Abnormalities Based on Contrast Agents: Introducing a Proof of Concept from a Physics Perspective" Sensors 22, no. 19: 7514. https://doi.org/10.3390/s22197514