

Kidney Cancer Prediction Empowered with Blockchain Security Using Transfer Learning
 ,
,  , ,
, ,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Literature Review
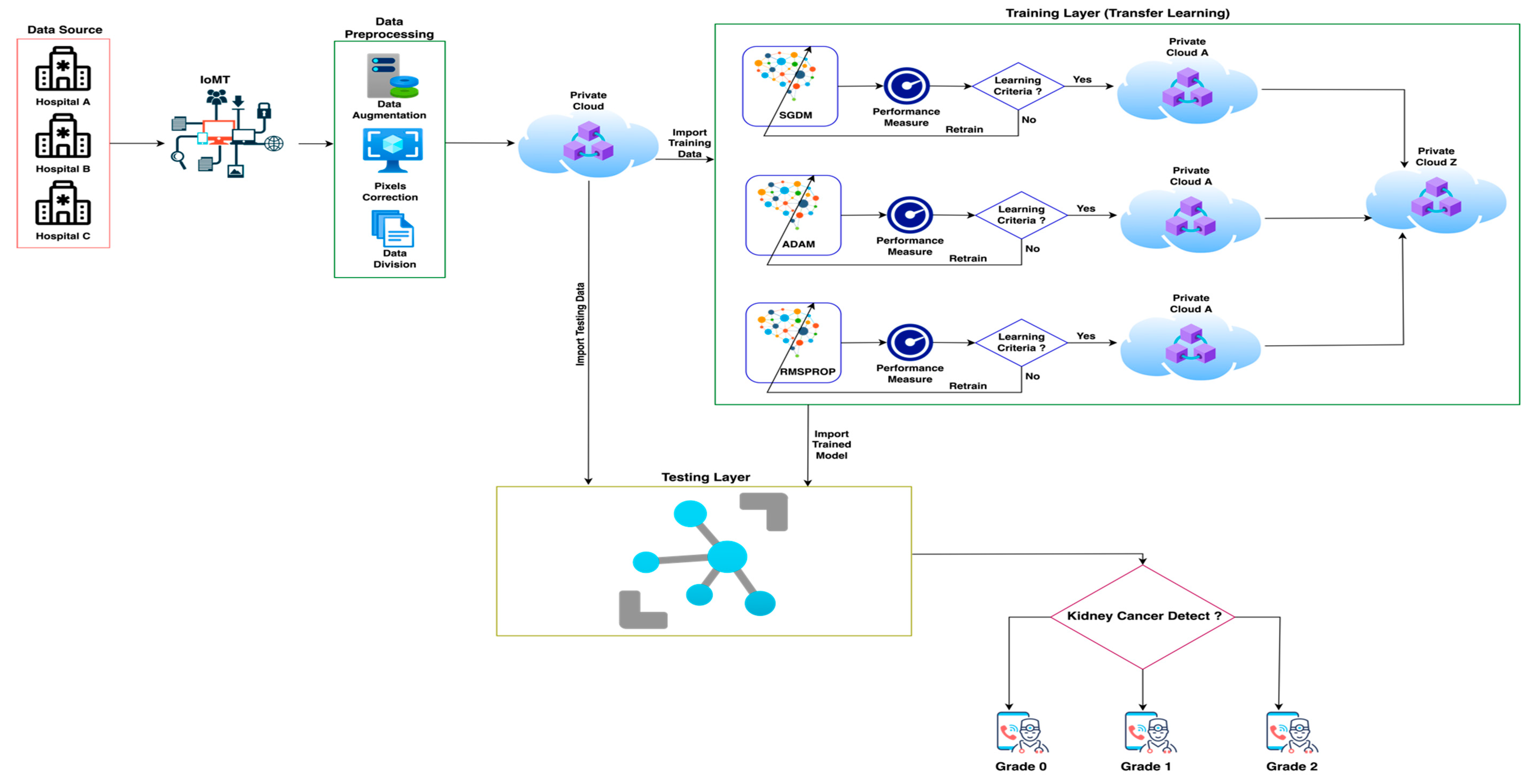
- IoMT-based proposed framework.
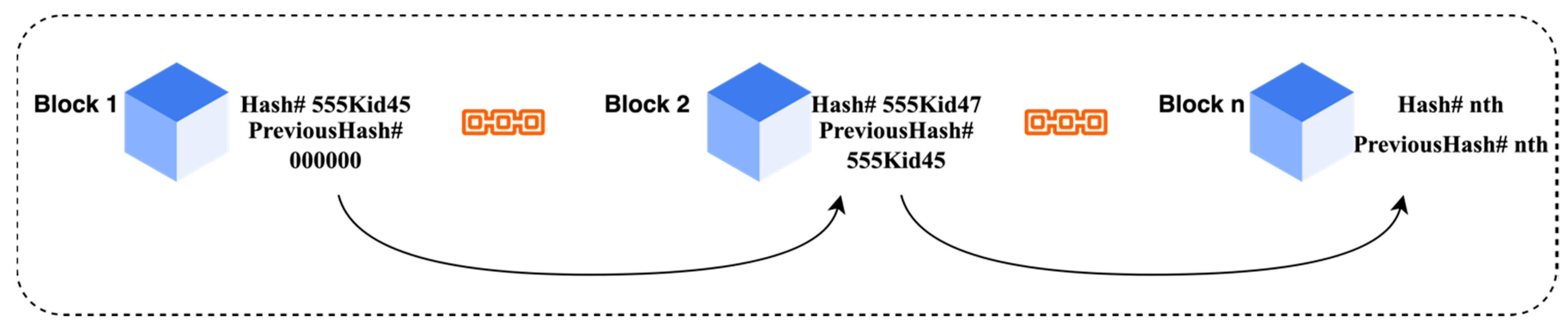
- The proposed model used blockchain technology for patients’ data security.
- The proposed model used various deep learning techniques empowered with transfer learning with the help of various parameters to predict kidney cancer.
- Numerous statistical matrixes were used to check the performance and reliability of the proposed framework.
3. Materials and Methods
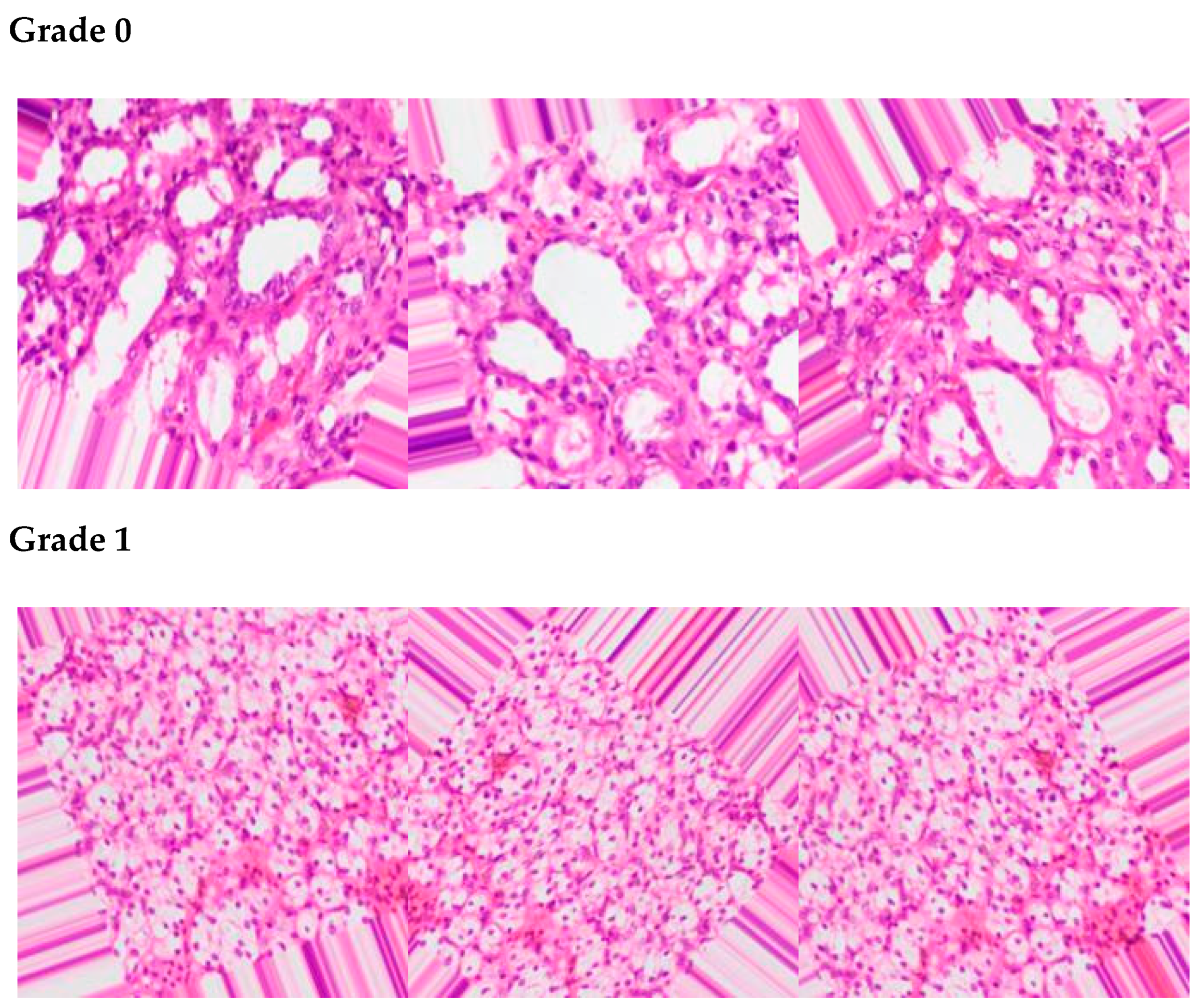
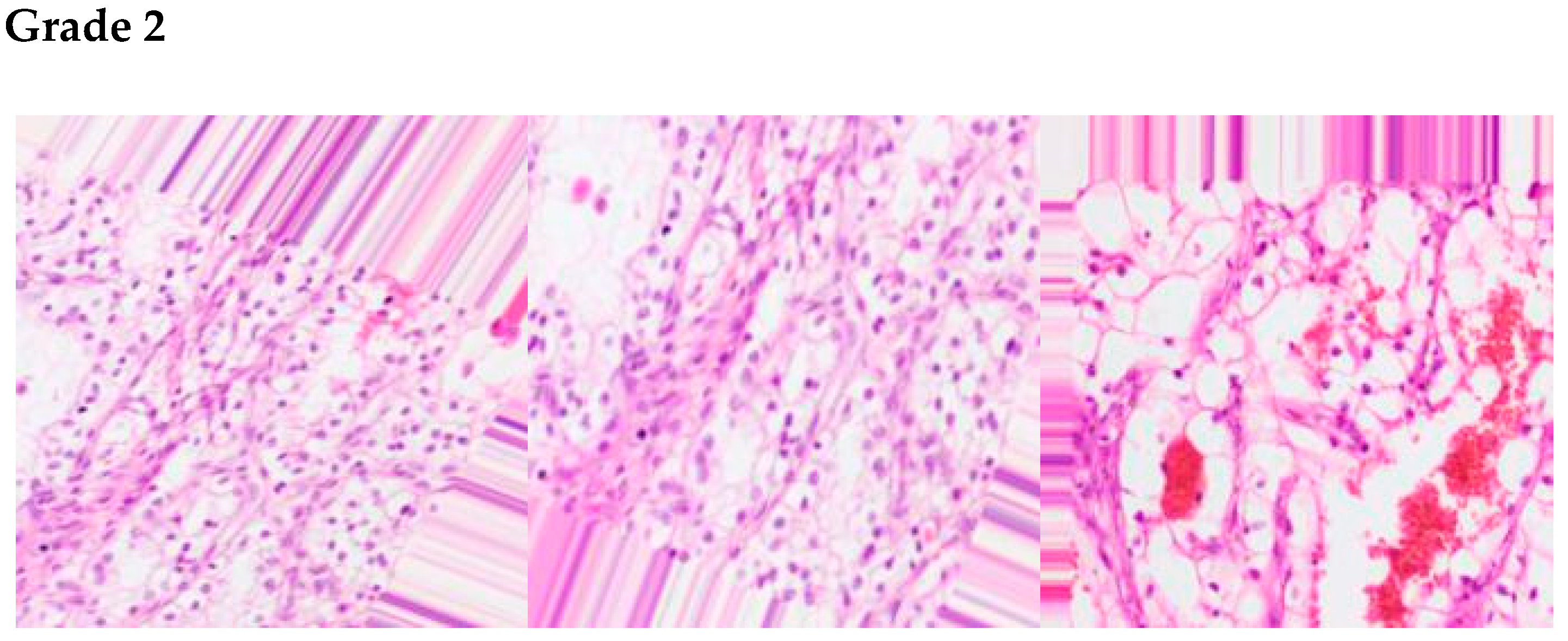
4. Data Set
5. Simulation and Results
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Zhan, C.; Wang, Z.; Xu, C.; Huang, X.; Su, J.; Chen, B.; Wang, M.; Qi, Z.; Bai, P. Development and Validation of a Prognostic Gene Signature in Clear Cell Renal Cell Carcinoma. Front. Mol. Biosci. 2021, 8, 609865. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Gong, Y.; Ning, X.; Peng, D.; Liu, L.; He, S.; Gong, K.; Zhang, C.; Li, X.; Zhou, L. Downregulation of CLDN7 due to promoter hypermethylation is associated with human clear cell renal cell carcinoma progression and poor prognosis. J. Exp. Clin. Cancer Res. 2018, 37, 276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motzer, R.J.; Bander, N.H.; Nanus, D.M. Renal-cell carcinoma. N. Engl. J. Med. 1996, 335, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Yang, Y. Identification of Mast Cell-Based Molecular Subtypes and a Predictive Signature in Clear Cell Renal Cell Carcinoma. Front. Mol. Biosci. 2021, 8, 719982. [Google Scholar] [CrossRef] [PubMed]
- Karakiewicz, P.I.; Briganti, A.; Chun, F.K.-H.; Trinh, Q.-D.; Perrotte, P.; Ficarra, V.; Cindolo, L.; De La Taille, A.; Tostain, J.; Mulders, P.F.; et al. Multi-Institutional Validation of a New Renal Cancer–Specific Survival Nomogram. J. Clin. Oncol. 2007, 25, 1316–1322. [Google Scholar] [CrossRef]
- Pantuck, A.J.; Zisman, A.; SBelldegrun, A. The changing natural history of renal cell carcinoma. J. Urol. 2001, 166, 1611–1623. [Google Scholar] [CrossRef]
- Wood, C.G. Multimodal Approaches in the Management of Locally Advanced and Metastatic Renal Cell Carcinoma: Combining Surgery and Systemic Therapies to Improve Patient Outcome. Clin. Cancer Res. 2007, 13, 697s–702s. [Google Scholar] [CrossRef] [Green Version]
- Muselaers, C.H.; Boerman, O.C.; Oosterwijk, E.; Langenhuijsen, J.F.; Oyen, W.J.; Mulders, P.F. Indium-111–labeled Girentuximab ImmunoSPECT as a Diagnostic Tool in Clear Cell Renal Cell Carcinoma. Eur. Urol. 2013, 63, 1101–1106. [Google Scholar] [CrossRef]
- Li, F.; Yang, M.; Li, Y.; Zhang, M.; Wang, W.; Yuan, D.; Tang, D. An improved clear cell renal cell carcinoma stage prediction model based on gene sets. BMC Bioinform. 2020, 21, 232. [Google Scholar] [CrossRef]
- Lazichand, I.; Bakris, G.L. Prediction, and management of hyperkalemia across the spectrum of chronic kidney disease. Seminars Nephrol. 2014, 34, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Changand, A.; Kramer, H. Should eGFR and albuminuria be added to the Framingham Risk Score chronic kidney disease and cardiovascular disease risk prediction. Nephron Clin. Pract. 2011, 119, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.D.; Yang, W.; Anderson, A.H.; Feldman, H.I.; Demirjian, S.; Hamano, T.; He, J.; Lash, J.; Lustigova, E.; Rosas, S.E.; et al. Urine neutrophil gelatinase–associated lipocalin levels do not improve risk prediction of progressive chronic kidney disease. Kidney Int. 2013, 83, 909–914. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.M.; Zhuang, H.; Ibrahim, A.; Rehman, O.; Huang, M.; Wu, A. A Machine Learning Approach for the Classification of Kidney Cancer Subtypes Using miRNA Genome Data. Appl. Sci. 2018, 8, 2422. [Google Scholar] [CrossRef] [Green Version]
- Sheehan, S.; Mawe, S.; Cianciolo, R.E.; Korstanje, R.; Mahoney, J.M. Detection and Classification of Novel Renal Histologic Phenotypes Using Deep Neural Networks. Am. J. Pathol. 2019, 189, 1786–1796. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Fei, H.; Liang, X.; Ji, D.; Cheng, M. A hybrid neural network model for predicting kidney disease in hypertension patients based on electronic health records. BMC Med. Informatics Decis. Mak. 2019, 19, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Kallenberger, S.M.; Schmidt, C. Forecasting the development of acute kidney injury using a recurrent neural network. Cardiovasc. Res. 2019, 115, e155–e157. [Google Scholar] [CrossRef] [PubMed]
- Suberi, A.A.M.; Zakaria, W.N.W.; Tomari, R. Dendritic Cell Recognition in Computer Aided System for Cancer Immunotherapy. Procedia Comput. Sci. 2017, 105, 177–182. [Google Scholar] [CrossRef]
- Sudharani, K.; Sarma, T.; Prasad, K.S. Advanced Morphological Technique for Automatic Brain Tumor Detection and Evaluation of Statistical Parameters. Procedia Technol. 2016, 24, 1374–1387. [Google Scholar] [CrossRef]
- Tabibu, S.; Vinod, P.K.; Jawahar, C.V. Pan-Renal Cell Carcinoma classification and survival prediction from histopathology images using deep learning. Sci. Rep. 2019, 9, 10509. [Google Scholar] [CrossRef]
- Santini, G.; Moreau, N.; Rubeaux, M. Kidney tumor segmentation using an ensembling multi-stage deep learning approach. A contribution to the KiTS19 challenge. arXiv 2019, arXiv:1909.00735. [Google Scholar]
- Sobhaninia, Z.; Rezaei, S.; Karimi, N.; Emami, A.; Samavi, S. Brain Tumor Segmentation by Cascaded Deep Neural Networks Using Multiple Image Scales. In Proceedings of the 2020 28th Iranian Conference on Electrical Engineering (ICEE), Tabriz, Iran, 4–6 August 2020. [Google Scholar]
- Song, T.; Zhang, Q.W.; Duan, S.F.; Bian, Y.; Hao, Q.; Xing, P.-Y.; Wang, T.-G.; Chen, L.-G.; Ma, G.; Lu, J.-P. MRI-based radionics approach for differentiation of hypovascular non-functional pancreatic neuroendocrine tumors and solid pseudopapillary neoplasms of the pancreas. BMC Med. Imaging 2021, 21, 36. [Google Scholar] [CrossRef]
- Shibata, T.; Teramoto, A.; Yamada, H.; Ohmiya, N.; Saito, K.; Fujita, H. Automated Detection and Segmentation of Early Gastric Cancer from Endoscopic Images Using Mask R-CNN. Appl. Sci. 2020, 10, 3842. [Google Scholar] [CrossRef]
- Sokoutil, M.; Sokouti, M.; Sokouti, B. Computer-aided diagnosis of thyroid cancer using image processing techniques. Int. J. Comput. Sci. Netw. Secur. 2018, 18, 329–339. [Google Scholar]
- Han, S.; Hwang, S.I.; Lee, H.J. The Classification of Renal Cancer in 3-Phase CT Images Using a Deep Learning Method. J. Digit. Imaging 2019, 32, 638–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skalski, A. Kidney tumor segmentation and detection on computed tomography data. In Proceedings of the 2016 IEEE International Conference on Imaging Systems and Techniques (IST), Chania, Greece, 4–6 October 2016; pp. 238–242. [Google Scholar]
- Rahman, A.-U.; Alqahtani, A.; Aldhafferi, N.; Nasir, M.U.; Khan, M.F.; Khan, M.A.; Mosavi, A. Histopathologic Oral Cancer Prediction Using Oral Squamous Cell Carcinoma Biopsy Empowered with Transfer Learning. Sensors 2022, 22, 3833. [Google Scholar] [CrossRef] [PubMed]
- Taleb, N.; Mehmood, S.; Zubair, M.; Naseer, I.; Mago, B.; Nasir, M.U. Ovary Cancer Diagnosing Empowered with Machine Learning. In Proceedings of the 2022 International Conference on Business Analytics for Technology and Security (ICBATS), Dubai, United Arab Emirates, 16–17 February 2022; pp. 1–6. [Google Scholar]
- Ghazal, T.M.; Hamadi, H.A.; Nasir, M.U.; Rahman, A.U.; Gollapalli, M.; Zubair, M.; Khan, M.A.; Yeun, C.Y. Supervised Machine Learning Empowered Multifactorial Genetic Inheritance Disorder Prediction. Comput. Intell. Neurosci. 2022, 2022, 1051388. [Google Scholar] [CrossRef]
- Nasir, M.U.; Khan, M.A.; Zubair, M.; Ghazal, T.M.; Said, R.A.; Al Hamadi, H. Single and Mitochondrial Gene Inheritance Disorder Prediction Using Machine Learning. Comput. Mater. Contin. 2022, 73, 953–963. [Google Scholar] [CrossRef]
- Nasir, M.U.; Ghazal, T.M.; Khan, M.A.; Zubair, M.; Rahman, A.-U.; Ahmed, R.; Al Hamadi, H.; Yeun, C.Y. Breast Cancer Prediction Empowered with Fine-Tuning. Comput. Intell. Neurosci. 2022, 2022, 5918686. [Google Scholar] [CrossRef]
- Rahman, A.U.; Nasir, M.U.; Gollapalli, M.; Alsaif, S.A.; Almadhor, A.S.; Mehmood, S.; Khan, M.A.; Mosavi, A. IoMT-Based Mitochondrial and Multifactorial Genetic Inheritance Disorder Prediction Using Machine Learning. Comput. Intell. Neurosci. 2022, 2022, 2650742. [Google Scholar] [CrossRef]
- Rahman, A.-U.; Nasir, M.U.; Gollapalli, M.; Zubair, M.; Saleem, M.A.; Mehmood, S.; Khan, M.A.; Mosavi, A. Advance Genome Disorder Prediction Model Empowered with Deep Learning. IEEE Access 2022, 10, 70317–70328. [Google Scholar] [CrossRef]
- Kaggle, Kidney Cancer. Available online: https://www.kaggle.com/datasets/atreyamajumdar/kidney-cancer (accessed on 1 May 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Model | Data | IoMT | Blockchain Security | Accuracy | Limitations |
|---|---|---|---|---|---|---|
| Ibrahim et al. [14] | LSTM | miRNA (Feature) | NO | NO | 95% | More validation for clinical studies, handcrafted features |
| Sheehan et al. [15] | DNN | CT Scan (Image) | NO | NO | 81% | Features issues, imbalance of data |
| Ren et al. [16] | HNN | Clinical (Feature) | NO | NO | 89.7% | Handcrafted feature |
| Kallenberger et al. [17] | RNN | Clinical (Feature) | NO | NO | 87% | Handcrafted feature |
| Vinod et al. [20] | CNN | RCC (Image) | NO | NO | 92.61% | Imbalance data issues |
| Moreau et al. [21] | CNN | Kits19 (Feature) | NO | NO | 89% | Handcrafted features, different stages for more local features |
| Lee et al. [26] | DNN | RCC (Image) | NO | NO | 85% | Performance matrixes should be improved, imbalance data |
| Shalski [27] | Vascular Tree | CT Scan (Image) | NO | NO | 92.1% | Feature selection and data segmentation, imbalance of data |
| Steps | Code |
|---|---|
| 1 | Data Source (h1, h2, h3, ………, hn) |
| 2 | IoMT (Data Source) |
| 3 | Data Preprocessing (Augmentation, Pixels Correction, Data Division) |
| 4 | Store Preprocessed Data  Private Cloud (Blockchain Secured) Private Cloud (Blockchain Secured) |
| 5 | Transfer Learning |
| 6 | Import Test Data Private Cloud Import Trained Model Private Cloud Z |
| 7 | Apply Texting (Predict Kidney Cancer) |
| 8 | Apply Statistical Matrix |
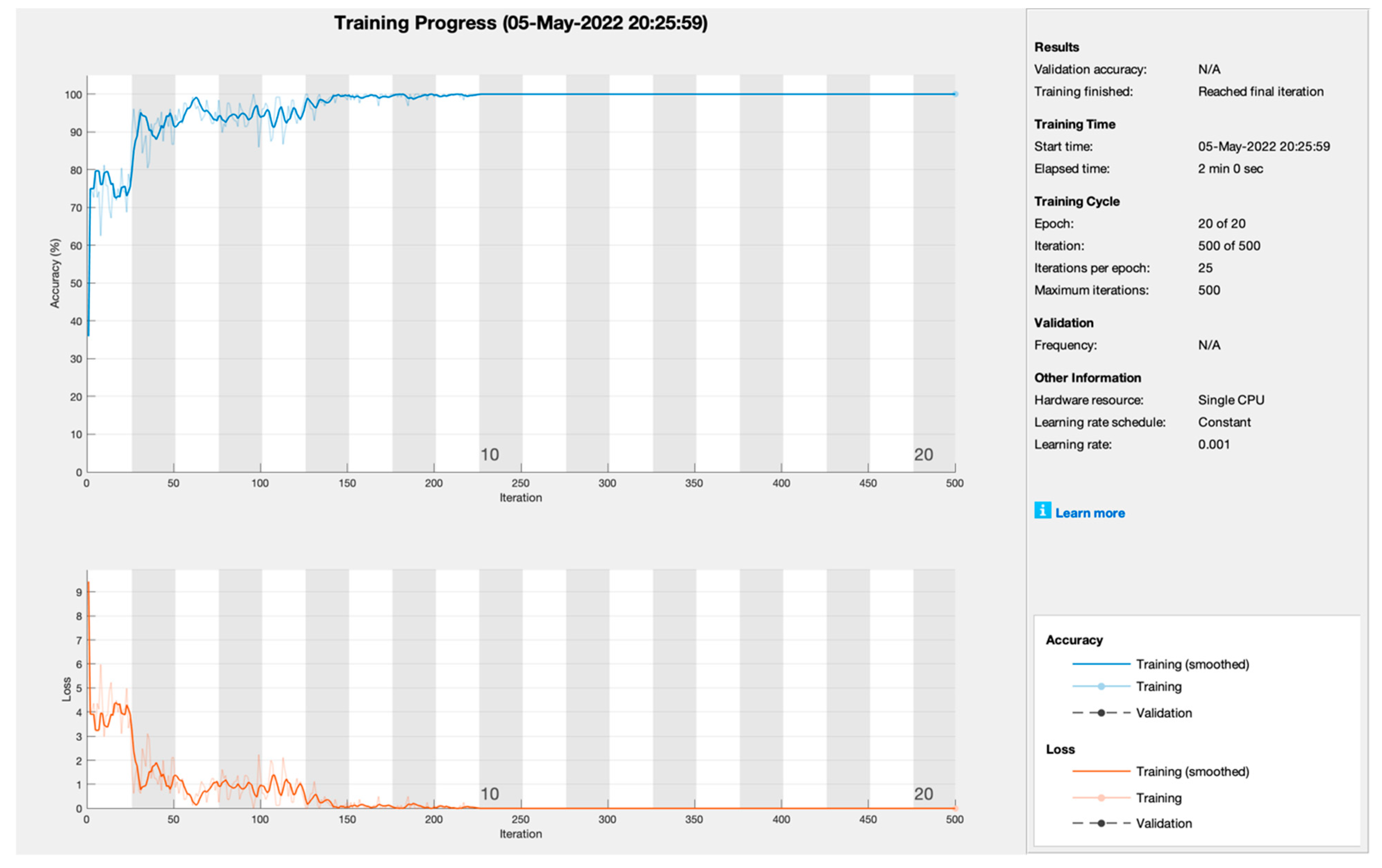
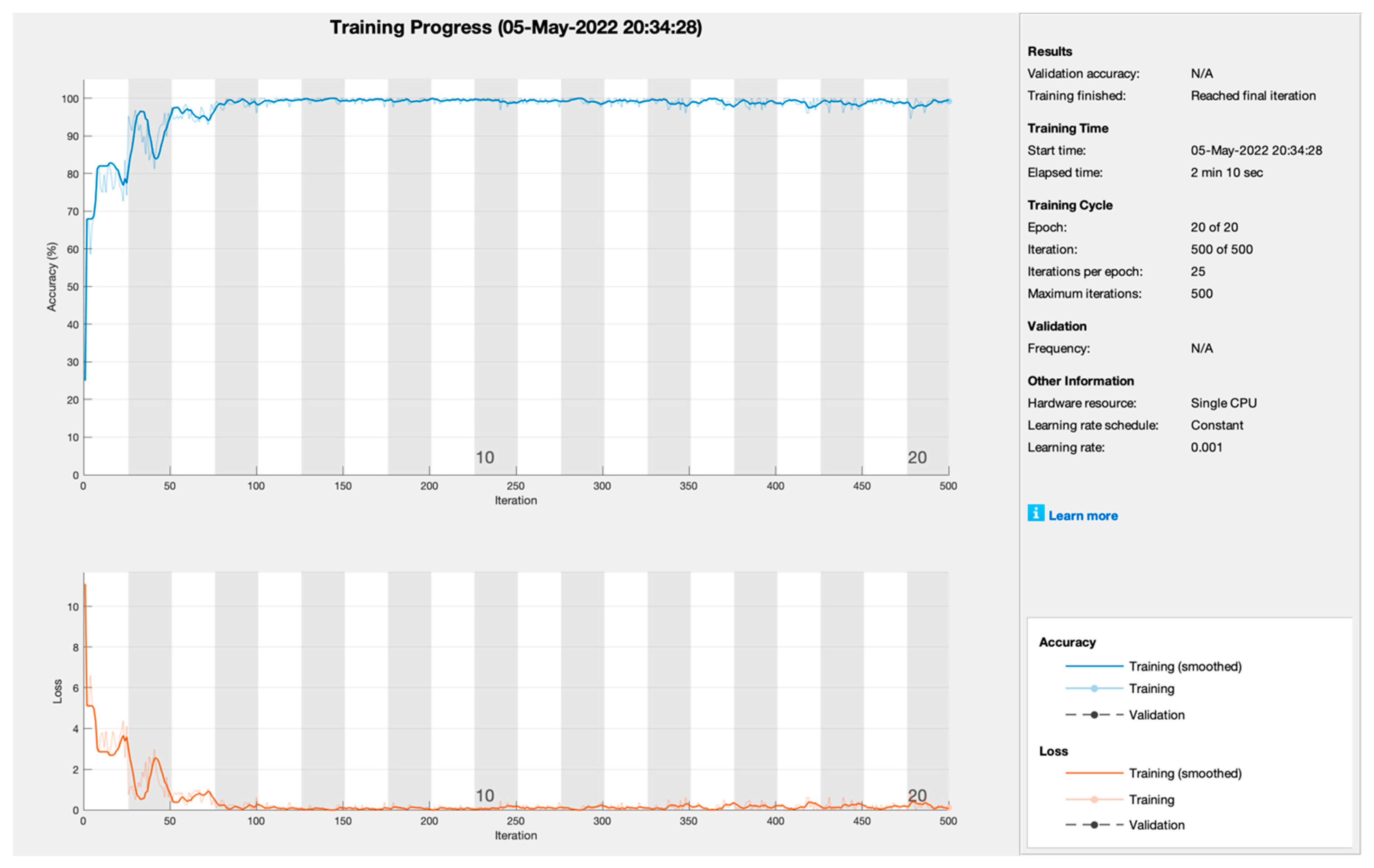
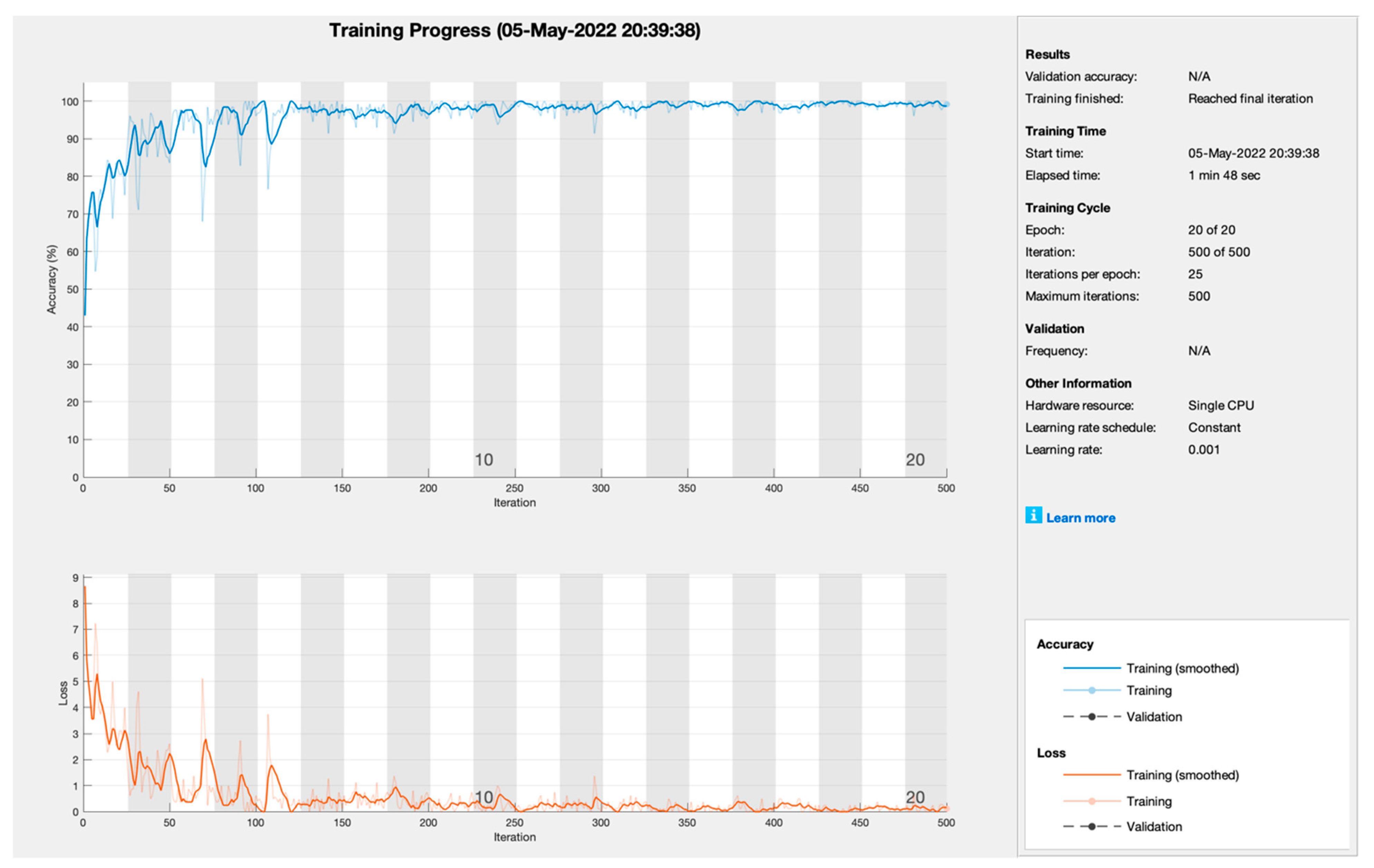
| AlexNet | |||||
|---|---|---|---|---|---|
| Model | Iterations | Learning Rate | Epoch | CA (%) | MCR (%) |
| SGDM | 500 | 0.001 | 20 | 99.8 | 0.2 |
| ADAM | 99.00 | 1.00 | |||
| RMSPROP | 98.98 | 1.02 | |||
| Total Samples (18) | Grade 0 | Grade 1 | Grade 2 |
|---|---|---|---|
| Grade 0 | 6 | 0 | 0 |
| Grade 1 | 0 | 6 | 0 |
| Grade 2 | 0 | 1 | 5 |
| Total Samples (18) | Grade 0 | Grade 1 | Grade 2 |
|---|---|---|---|
| Grade 0 | 6 | 0 | 0 |
| Grade 1 | 0 | 6 | 0 |
| Grade 2 | 0 | 2 | 4 |
| Total Samples (18) | Grade 0 | Grade 1 | Grade 2 |
|---|---|---|---|
| Grade 0 | 6 | 0 | 0 |
| Grade 1 | 1 | 5 | 0 |
| Grade 2 | 0 | 1 | 5 |
| Total Samples (990) | Grade 0 | Grade 1 | Grade 2 |
|---|---|---|---|
| Grade 0 | 330 | 1 | 0 |
| Grade 1 | 0 | 322 | 0 |
| Grade 2 | 0 | 7 | 330 |
| Total Samples (990) | Grade 0 | Grade 1 | Grade 2 |
|---|---|---|---|
| Grade 0 | 330 | 0 | 1 |
| Grade 1 | 0 | 321 | 1 |
| Grade 2 | 8 | 7 | 322 |
| Total Samples (990) | Grade 0 | Grade 1 | Grade 2 |
|---|---|---|---|
| Grade 0 | 327 | 2 | 2 |
| Grade 1 | 0 | 319 | 3 |
| Grade 2 | 10 | 3 | 324 |
| SGDM (%) | |||||||||
| CA | CMR | Sen | Spec | F1 | PPV | NPV | FPR | FNR | LPR |
| 99.20 | 0.80 | 100.00 | 99.85 | 99.85 | 99.70 | 100.00 | 0.15 | 0.00 | 660.00 |
| LNR | FMI | ||||||||
| 0.00 | 99.85 | ||||||||
| ADAM (%) | |||||||||
| CA | CMR | Sen | Spec | F1 | PPV | NPV | FPR | FNR | LPR |
| 98.30 | 1.70 | 99.69 | 98.95 | 98.77 | 97.87 | 99.85 | 1.05 | 0.31 | 95.13 |
| LNR | FMI | ||||||||
| 0.00 | 98.77 | ||||||||
| RMSPROP (%) | |||||||||
| CA | CMR | Sen | Spec | F1 | PPV | NPV | FPR | FNR | LPR |
| 98.18 | 1.82 | 96.14 | 99.23 | 97.30 | 98.48 | 98.03 | 0.77 | 3.86 | 125.56 |
| LNR | FMI | ||||||||
| 0.04 | 97.30 | ||||||||
| Study | Model | Dataset | IoMT | Blockchain Security | Accuracy |
|---|---|---|---|---|---|
| Ibrahim et al. [14] | LSTM | miRNA (Feature) | NO | NO | 95% |
| Sheehan et al. [15] | DNN | CT Scan (Image) | NO | NO | 81% |
| Ren et al. [16] | HNN | Clinical (Feature) | NO | NO | 89.7% |
| Kallenberger et al. [17] | RNN | Clinical (Feature) | NO | NO | 87% |
| Vinod et al. [20] | CNN | RCC (Image) | NO | NO | 92.61% |
| Moreau et al. [21] | CNN | Kits19 (Feature) | NO | NO | 89% |
| Lee et al. [26] | DNN | RCC (Image) | NO | NO | 85% |
| Shalski [27] | Vascular Tree | CT Scan (Image) | NO | NO | 92.1% |
| Benchmark [35] | ResNet Custom | Biopsy (Image) | No | No | 79% |
| Benchmark [35] | VGG Net | Biopsy (Image) | No | No | 20% |
| The Proposed Model (Augmented Test Data) | Transfer Learning (SGDM, ADAM, RMSPROP) | Biopsy (Image) | Yes | Yes | 99.2% |
| The Proposed Model (NonAugmented Test Data) | Transfer Learning (SGDM, ADAM, RMSPROP) | Biopsy (Image) | Yes | Yes | 93.75% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasir, M.U.; Zubair, M.; Ghazal, T.M.; Khan, M.F.; Ahmad, M.; Rahman, A.-u.; Hamadi, H.A.; Khan, M.A.; Mansoor, W. Kidney Cancer Prediction Empowered with Blockchain Security Using Transfer Learning. Sensors 2022, 22, 7483. https://doi.org/10.3390/s22197483
Nasir MU, Zubair M, Ghazal TM, Khan MF, Ahmad M, Rahman A-u, Hamadi HA, Khan MA, Mansoor W. Kidney Cancer Prediction Empowered with Blockchain Security Using Transfer Learning. Sensors. 2022; 22(19):7483. https://doi.org/10.3390/s22197483
Chicago/Turabian StyleNasir, Muhammad Umar, Muhammad Zubair, Taher M. Ghazal, Muhammad Farhan Khan, Munir Ahmad, Atta-ur Rahman, Hussam Al Hamadi, Muhammad Adnan Khan, and Wathiq Mansoor. 2022. "Kidney Cancer Prediction Empowered with Blockchain Security Using Transfer Learning" Sensors 22, no. 19: 7483. https://doi.org/10.3390/s22197483