
Optical Identification of Parenteral Nutrition Solutions Exploiting Refractive Index Sensing



Abstract
:1. Introduction
2. Material and Methods
2.1. Solutions for Artificial Parenteral Nutrition
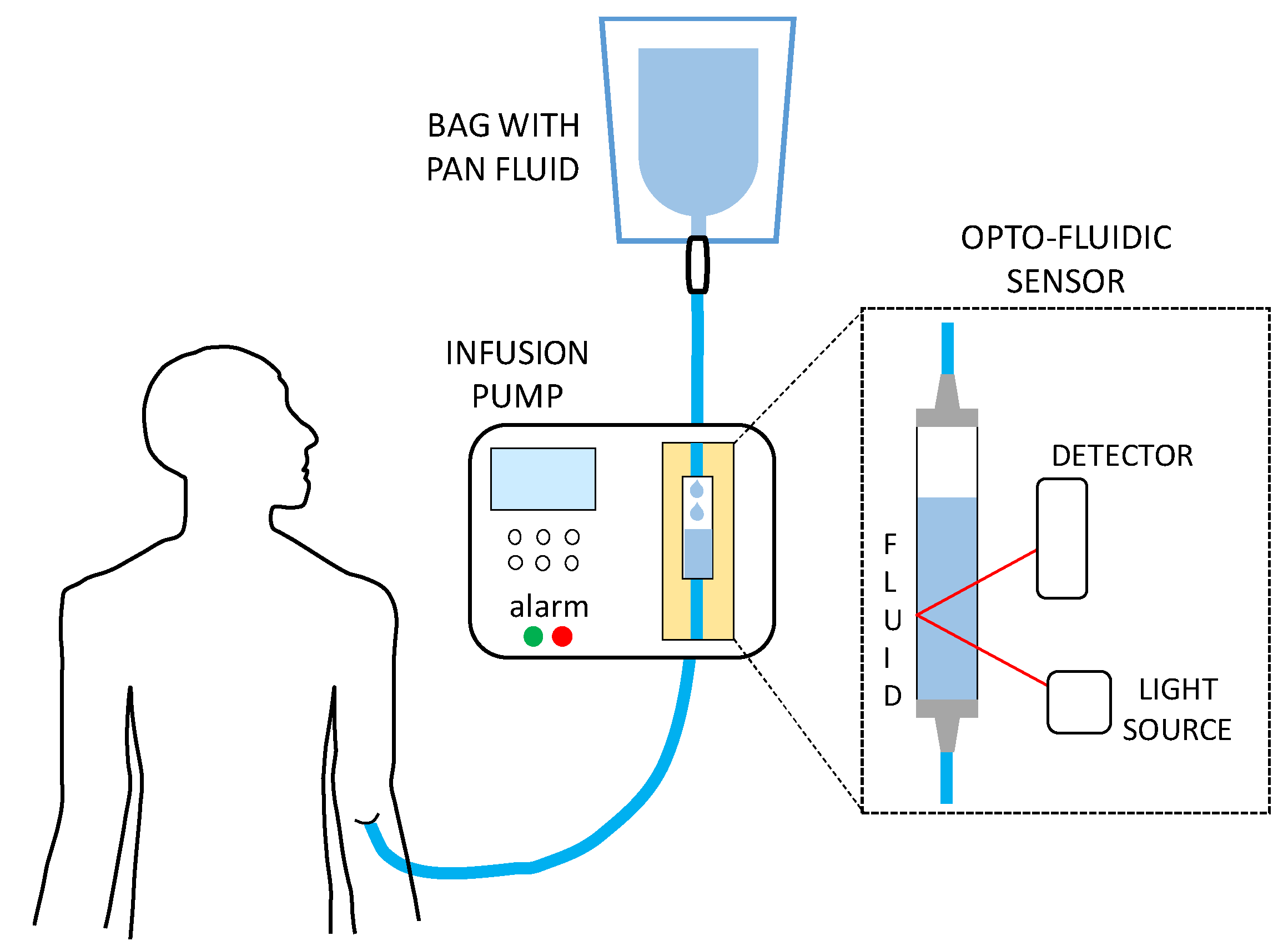
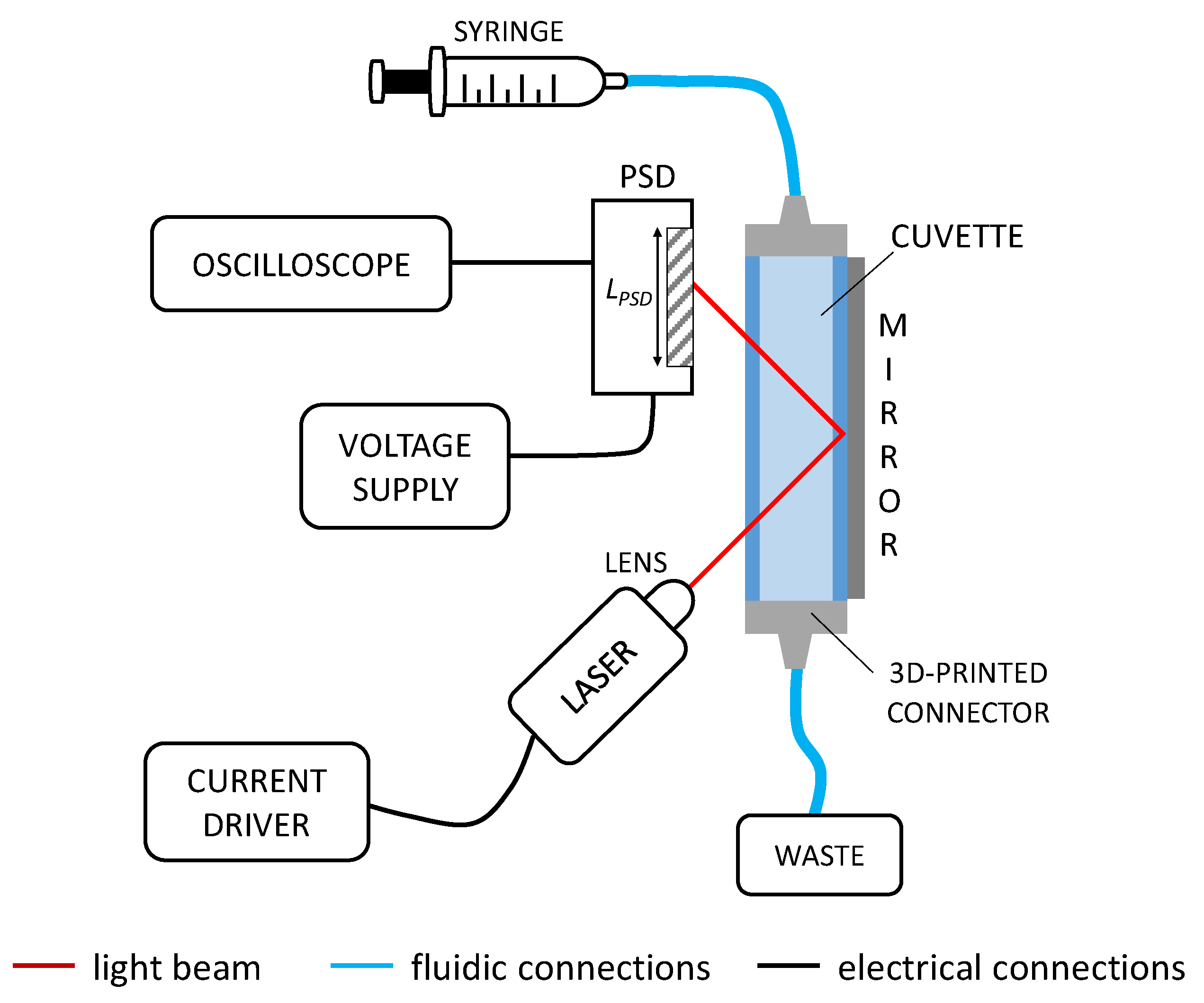
2.2. Optofluidic Configuration
2.3. Principle of Operation of the Sensor
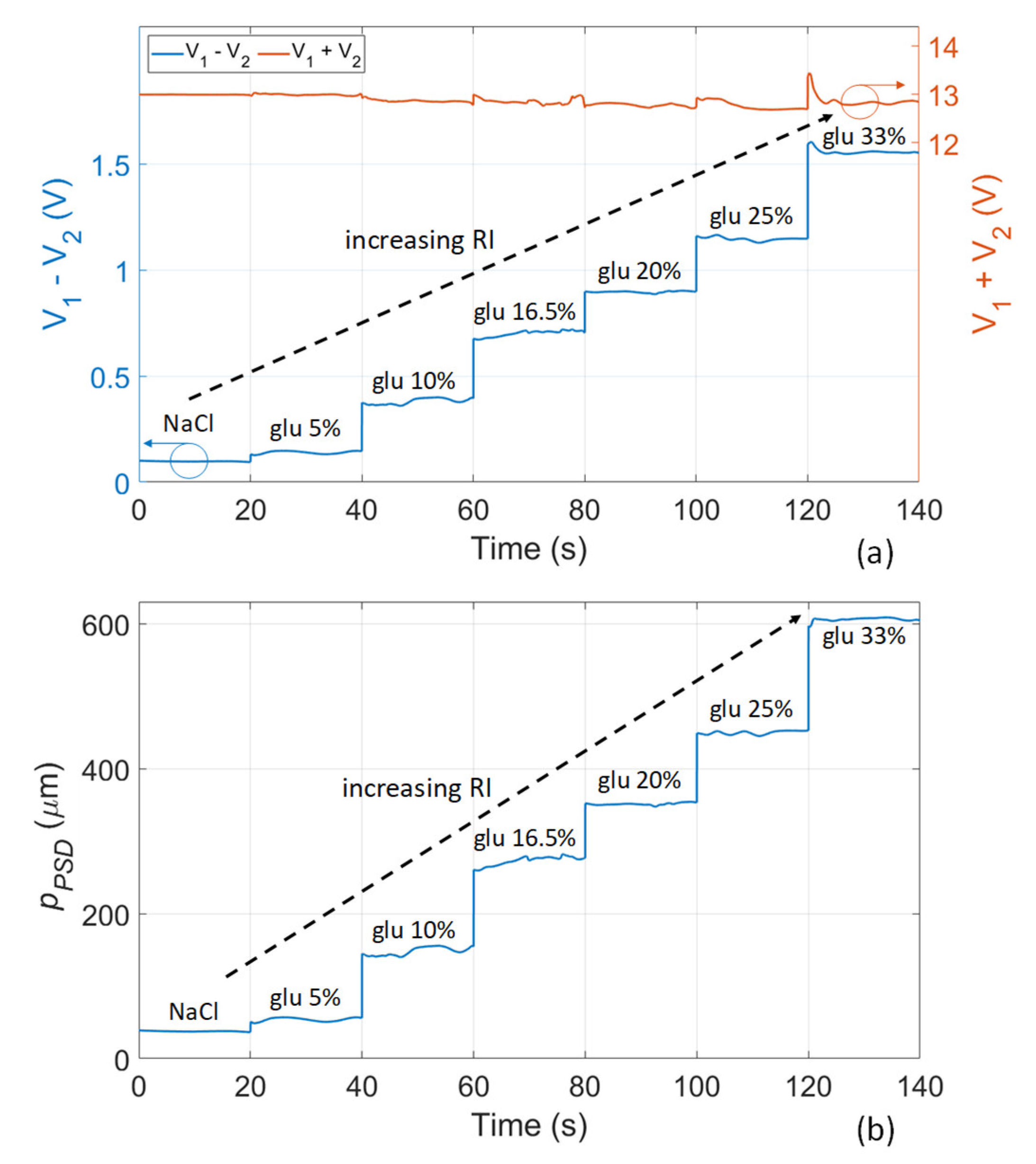
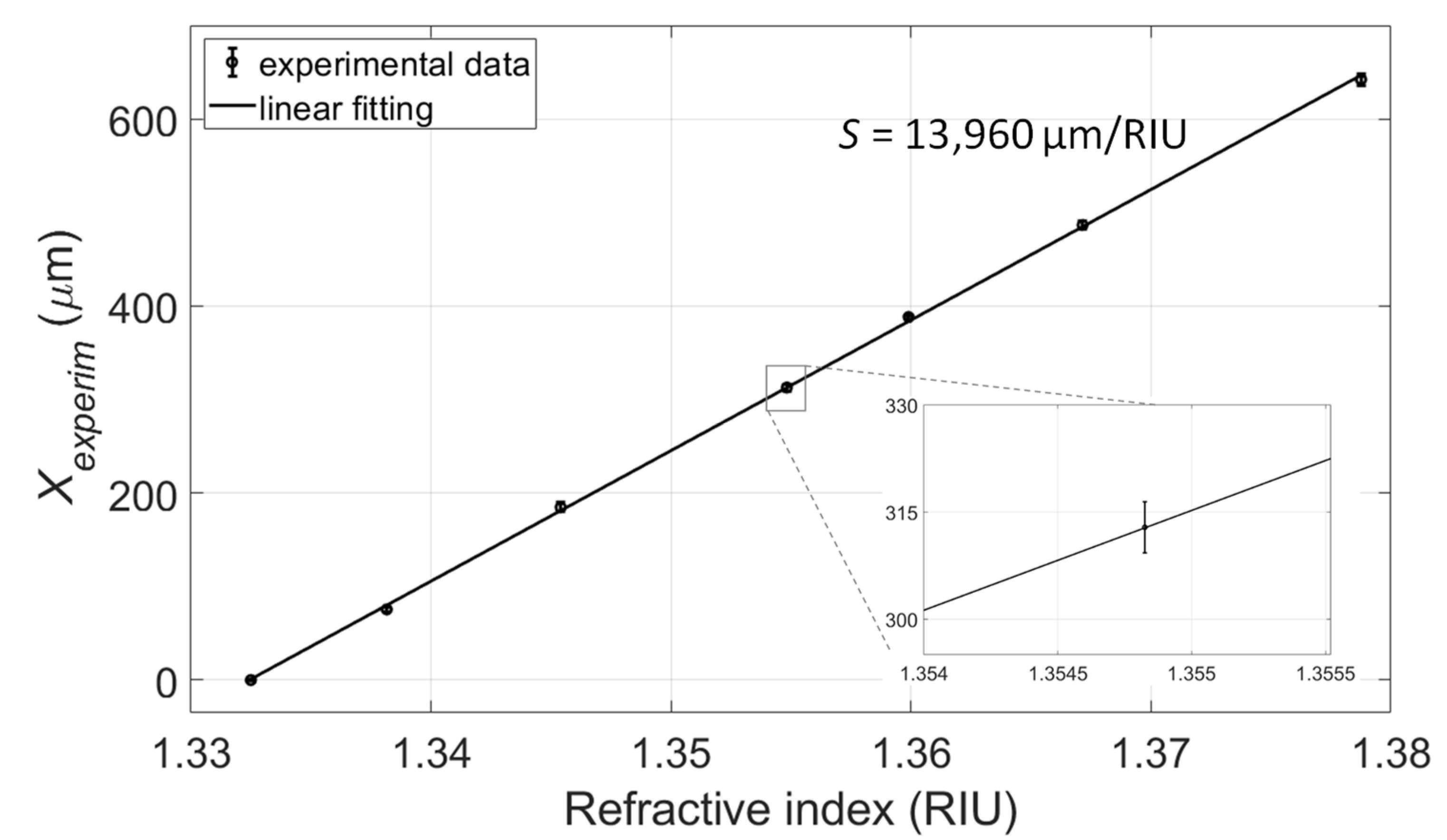
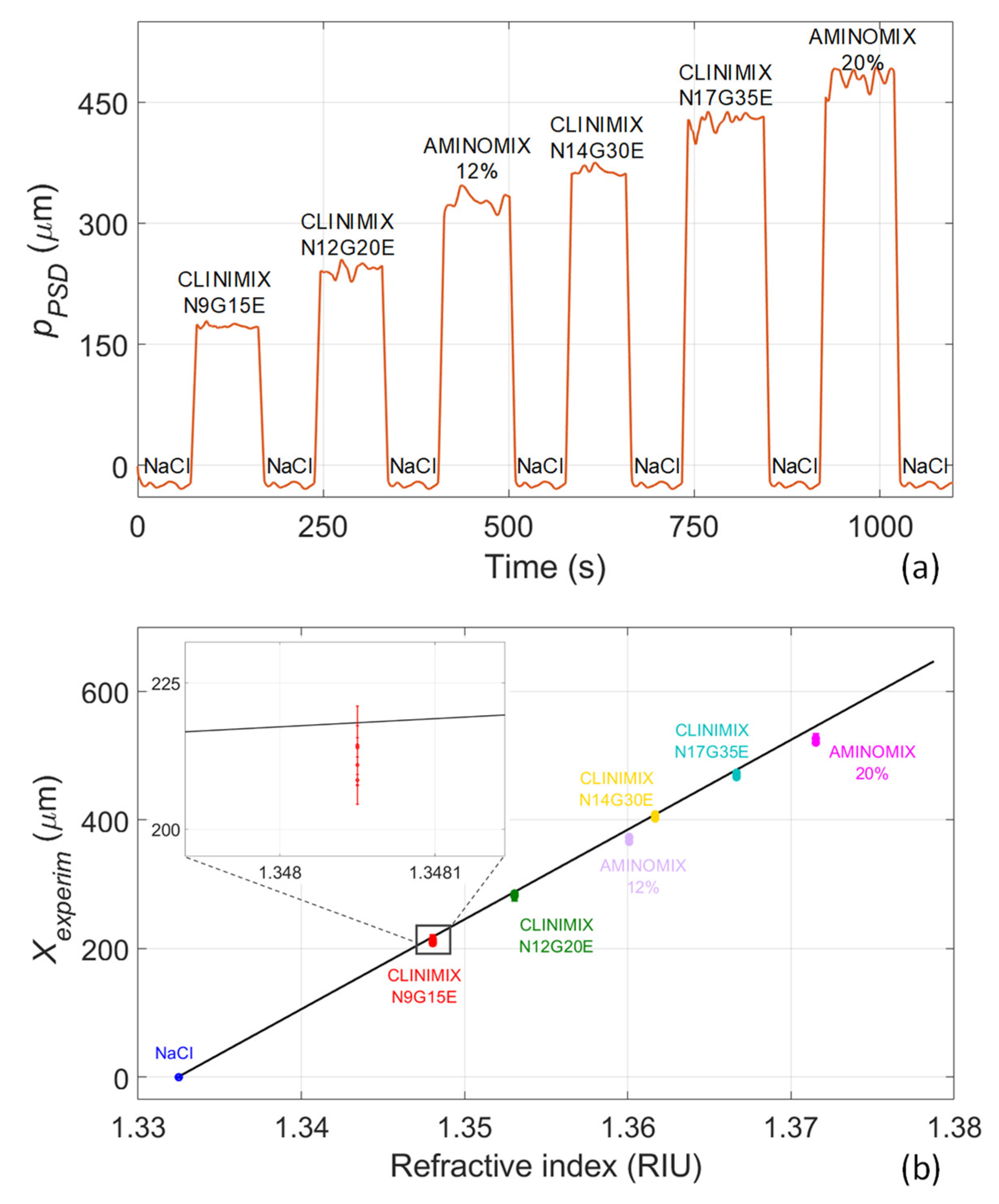
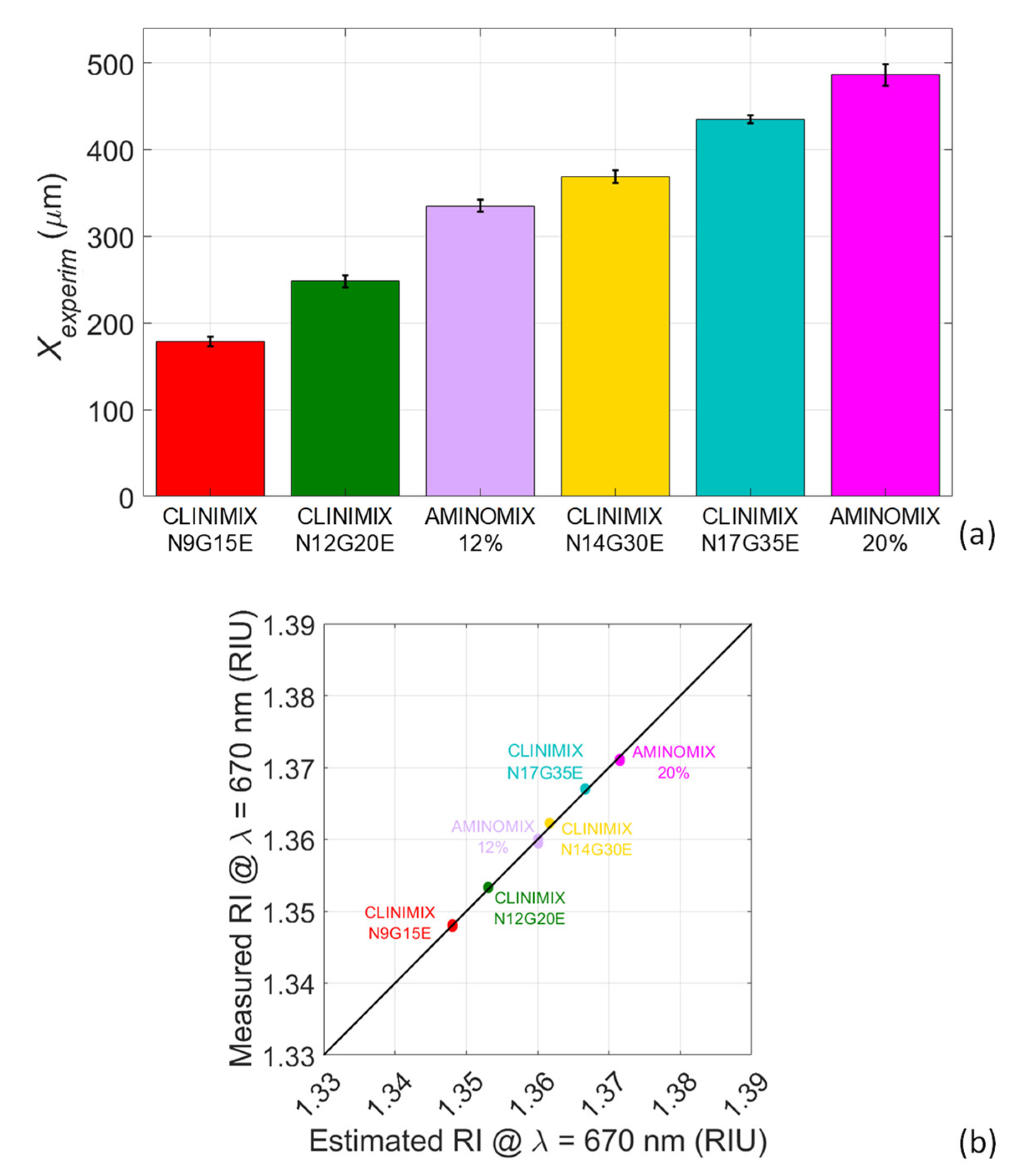
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, S.C.; Escher, J.; Hébuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. ESPEN practical guideline: Clinical Nutrition in inflammatory bowel disease. Clin. Nutr. 2020, 39, 632–653. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef]
- Ferrara, F.; De Rosa, F.; Vitiello, A. The Central Role of Clinical Nutrition in COVID-19 Patients During and After Hospitalization in Intensive Care Unit. SN Compr. Clin. Med. 2020, 2, 1064–1068. [Google Scholar] [CrossRef] [PubMed]
- Brugliera, L.; Spina, A.; Castellazzi, P.; Cimino, P.; Arcuri, P.; Negro, A.; Houdayer, E.; Alemanno, F.; Giordani, A.; Mortini, P.; et al. Nutritional management of COVID-19 patients in a rehabilitation unit. Eur. J. Clin. Nutr. 2020, 74, 860–863. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.; Sexton, E. Managing children and adolescents on parenteral nutrition: Challenges for the nutritional support team. Proc. Nutr. Soc. 2006, 65, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Mihatsch, W.A.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Desci, T.; Domellöf, M.; Embleton, N.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition. Clin. Nutr. 2018, 37, 2303–2305. [Google Scholar] [CrossRef] [PubMed]
- Akbar, Z.; Saeed, H.; Saleem, Z.; Andleeb, S. Dosing errors in total parenteral nutrition prescriptions at a specialized cancer care hospital of Lahore: The role of clinical pharmacist. Oncol. Pharm. Pract. 2021, 27, 531–540. [Google Scholar] [CrossRef]
- Sacks, G.S.; Rough, S.; Kudsk, K.A. Frequency and Severity of Harm of Medication Errors Related to the Parenteral Nutrition Process in a Large University Teaching Hospital. Pharmacotherapy 2009, 29, 966–974. [Google Scholar] [CrossRef]
- Mistry, P.; Smith, R.H.; Fox, A. Patient Safety Incidents Related to the Use of Parenteral Nutrition in All Patient Groups: A Systematic Scoping Review. Drug Saf. 2022, 45, 1–8. [Google Scholar] [CrossRef]
- Brown, E.W.; McClellan, N.H.; Minard, G.; Maish, G.O.; Dickerson, R.N. Avoiding Patient Harm With Parenteral Nutrition During Electrolyte Shortages. Hosp. Pharm. 2018, 53, 403–407. [Google Scholar] [CrossRef]
- Cohen, M.R.; Smetzer, J.L. Another Tragic Parenteral Nutrition Compounding Error: Change in Anzemet Indication: Teva’s Lansoprazole Orally Disentegrating Tablet Clogs Tubes: Lawyers Weigh in on Consistent Use of Smart Pump Libraries. Hosp. Pharm. 2011, 46, 470–476. [Google Scholar] [CrossRef]
- Grissinger, M. Mismatched prescribing and pharmacy templates for parenteral nutrition lead to data-entry errors. Pharm. Ther. 2015, 40, 349–350. [Google Scholar] [PubMed]
- Grissinger, M. A fatal zinc overdose in a Neonate: Confusion of micrograms with milligrams. Pharm. Ther. 2011, 36, 393–409. [Google Scholar]
- Ruktanonchai, D.; Lowe, M.; Norton, S.A.; Garret, T.; Soghier, L.; Weiss, E.; Hatfield, J.; Lapinski, J.; Abrams, S.; Barfield, W.; et al. Zinc deficiency-associated dermatitis in infants during a nationwide shortage of injectable zinc—Washington, DC, and Houston, Texas, 2012–2013. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 35–37. [Google Scholar]
- Raphael, B.P.; Murphy, M.; Gura, K.M.; Litman, H.; Dalton, M.K.; Finkelstein, J.A.; Lightdale, J.R. Discrepancies Between Prescribed and Actual Pediatric Home Parenteral Nutrition Solutions. Nutr. Clin. Pract. 2016, 31, 654–658. [Google Scholar] [CrossRef]
- Cohen, M.R.; Smetzer, J.L. Important Change with Heparin Labels; Benadryl Dispensed Instead of Vitamins for Home Parenteral Nutrition; Potassium and Sodium Acetate Injection Mix-Ups; Don’t Truncate, Stem, or Shorten Drug Names. Hosp. Pharm. 2013, 48, 267–269. [Google Scholar] [CrossRef]
- Li, Q.; Kirkendall, E.S.; Hall, E.S.; Ni, Y.; Lingren, T.; Kaiser, M.; Lingren, N.; Zhai, H.; Solti, I.; Melton, K. Automated detection of medication administration errors in neonatal intensive care. J. Biomed. Inform. 2015, 57, 124–133. [Google Scholar] [CrossRef]
- MacKay, M.; Anderson, C.; Boehme, S.; Cash, J.; Zobell, J. Frequency and Severity of Parenteral Nutrition Medication Errors at a Large Children’s Hospital After Implementation of Electronic Ordering and Compounding. Nutr. Clin. Pract. 2016, 31, 195–206. [Google Scholar] [CrossRef]
- Jaywant, S.A.; Singh, H.; Arif, K.M. Sensors and Instruments for Brix Measurement: A Review. Sensors 2022, 22, 2290. [Google Scholar] [CrossRef]
- Singh, S. Refractive Index Measurement and its Applications. Phys. Scr. 2002, 65, 167–180. [Google Scholar] [CrossRef]
- Ye, F.; Tian, C.; Ma, C.; Zhang, Z.F. Fiber optic sensors based on circular and elliptical polymer optical fiber for measuring refractive index of liquids. Opt. Fiber Technol. 2022, 68, 102812. [Google Scholar] [CrossRef]
- Pereira, D.; Bierlich, J.; Kobelke, J.; Pereira, V.; Ferreira, M.S. Optical Fiber Sensor for Monitoring the Evaporation of Ethanol–Water Mixtures. Sensors 2022, 22, 5498. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Liu, Z.; Zhang, Y.; Liu, S. Side-Polished D-Type Fiber SPR Sensor for RI Sensing with Temperature Compensation. IEEE Sens. J. 2021, 21, 16621–16628. [Google Scholar] [CrossRef]
- Khanikar, T.; De, M.; Singh, V.K. A review on infiltrated or liquid core fiber optic SPR sensors. Photonics Nanostruct. Fundam. Appl. 2021, 46, 100945. [Google Scholar] [CrossRef]
- Minato, H.; Kakul, Y.; Nishimoto, A.; Nanjo, M. Remote Refractive Index Difference Meter for Salinity Sensor. IEEE Trans. Instrum. Meas. 1989, 38, 608–612. [Google Scholar] [CrossRef]
- Nemoto, S. Measurement of the refractive index of liquid using laser beam displacement. Appl. Opt. 1992, 31, 6690. [Google Scholar] [CrossRef]
- Docchio, F.; Corini, S.; Perini, M.; Kasana, R.S. A Simple and Reliable System for Measuring the Refractive Index of Liquids Using a Position-Sensitive Detector. IEEE Trans. Instrum. Meas. 1995, 44, 68–70. [Google Scholar] [CrossRef]
- Yeh, Y.L.; Wang, C.C.; Jang, M.J.; Chen, C.H.; Tzeng, S.M.; Lin, Y.P.; Chen, K.S. Real-Time Measurement of Glucose Concentration Using Position Sensing Detector. In Proceedings of the 3rd IEEE International Conference on Nano/Micro Engineered and Molecular Systems, NEMS, Sanya, China, 6–9 January 2008; pp. 561–565. [Google Scholar]
- Seow, Y.C.; Lim, S.P.; Khoo, B.C.; Lee, H.P. An optofluidic refractive index sensor based on partial refraction. Sens. Actuators B Chem. 2010, 147, 607–611. [Google Scholar] [CrossRef]
- Malinin, A.V.; Zanishevskaja, A.A.; Tuchin, V.V.; Skibina, Y.S.; Silokhin, I.Y. Photonic crystal fibers for food quality analysis. In Biophotonics: Photonic Solutions for Better Health Care III; Popp, J., Drexler, W., Tuchin, V.V., Matthews, D.L., Eds.; SPIE: Bellingham, DC, USA, 2012; Volume 8427, p. 842746. [Google Scholar]
- Zhao, H.; Brown, P.H.; Schuck, P. On the distribution of protein refractive index increments. Biophys. J. 2011, 100, 2309–2317. [Google Scholar] [CrossRef]
- Tan, C.Y.; Huang, Y.X. Dependence of Refractive Index on Concentration and Temperature in Electrolyte Solution, Polar Solution, Nonpolar Solution, and Protein Solution. J. Chem. Eng. Data 2015, 60, 2827–2833. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PAN Fluid | nPAN fluid (RIU) Estimated at 670 nm |
|---|---|
| CLINIMIX N9G15E | 1.3481 |
| CLINIMIX N12G20E | 1.3531 |
| AMINOMIX 20% | 1.3601 |
| CLINIMIX N14G30E | 1.3617 |
| CLINIMIX N17G35E | 1.3667 |
| AMINOMIX 20% | 1.3716 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bello, V.; Bodo, E.; Merlo, S. Optical Identification of Parenteral Nutrition Solutions Exploiting Refractive Index Sensing. Sensors 2022, 22, 6815. https://doi.org/10.3390/s22186815
Bello V, Bodo E, Merlo S. Optical Identification of Parenteral Nutrition Solutions Exploiting Refractive Index Sensing. Sensors. 2022; 22(18):6815. https://doi.org/10.3390/s22186815
Chicago/Turabian StyleBello, Valentina, Elisabetta Bodo, and Sabina Merlo. 2022. "Optical Identification of Parenteral Nutrition Solutions Exploiting Refractive Index Sensing" Sensors 22, no. 18: 6815. https://doi.org/10.3390/s22186815