
A New Phased-Array Magnetic Resonance Imaging Receive-Only Coil for HBO2 Studies


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
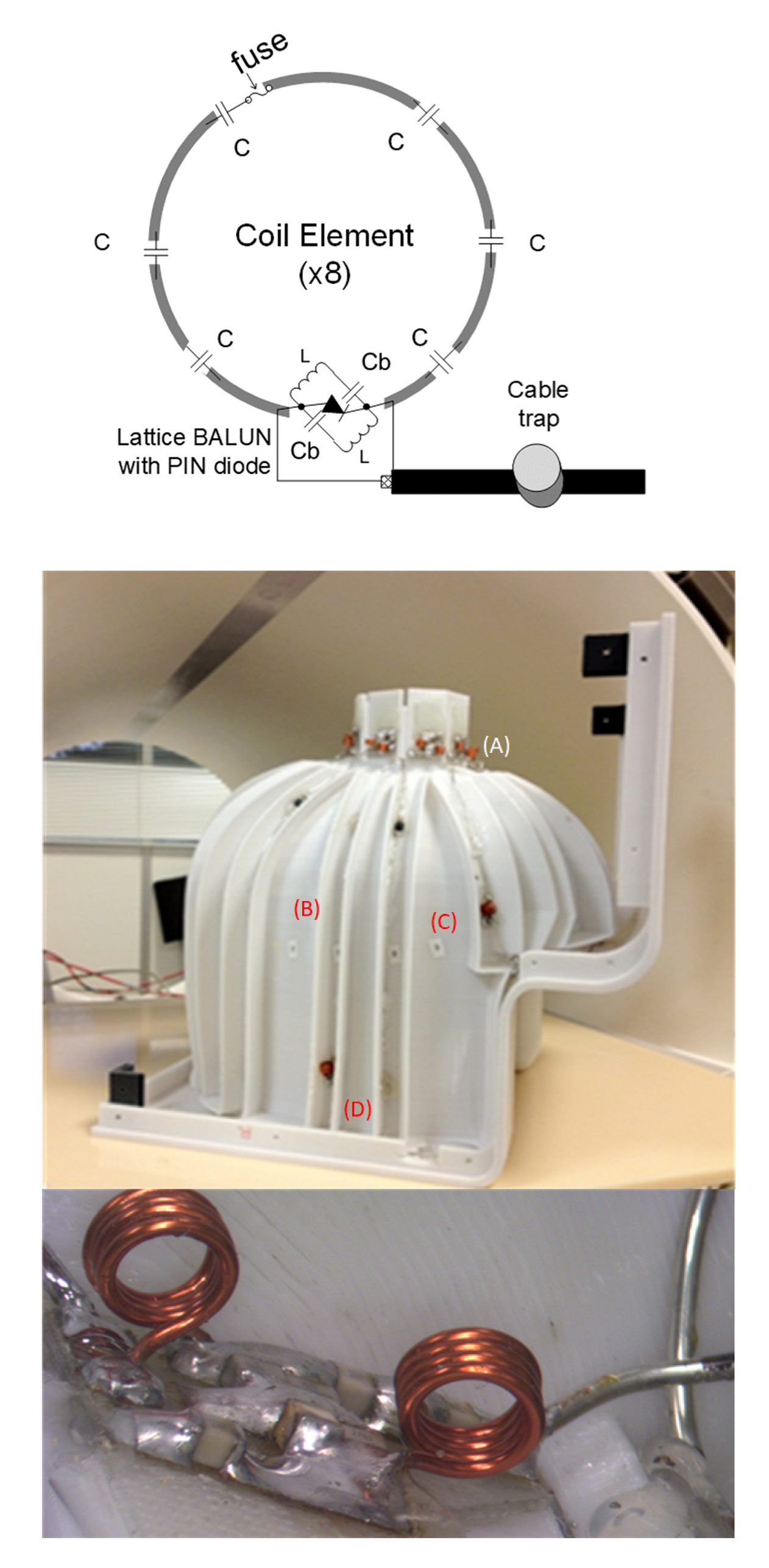
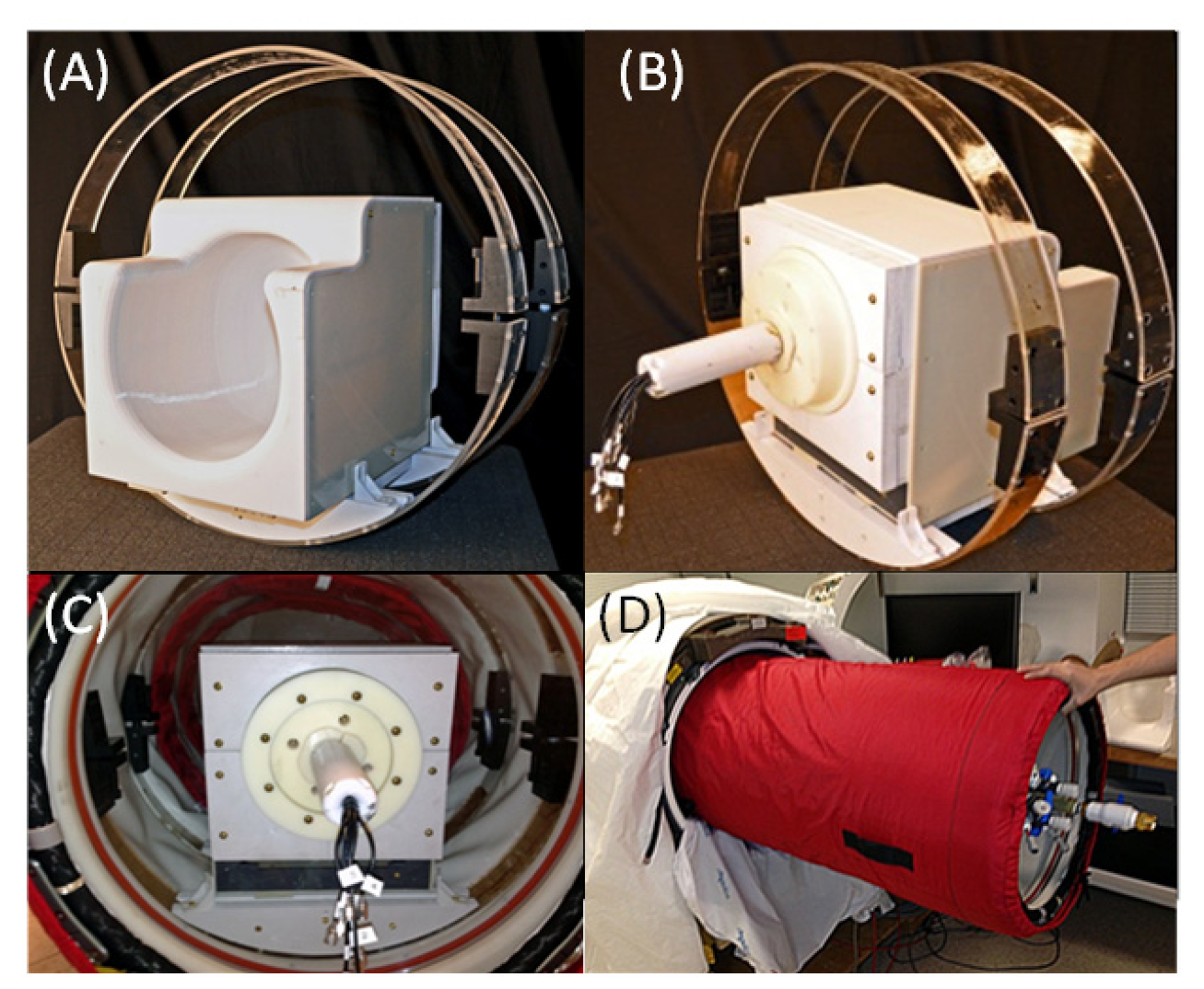
2.1. Eight-Channel Phased-Array Head Coil and the Preamplifier Interface Board
2.2. RF Safety Testing
- Cover protection. The cover protection test checks if the cover protects the subject from touching any electrical parts of the coil.
- Fuses and/or passive circuits The fuses test checks if fuses were present in the coil.
- Availability of the SAR parameters. The SAR test parameters were included in the coil files located on the scanner.
- Detuning during the transmitting phase. The detuning during the transmitting phase checks whether the active detuning of the receive coil during transmitting is sufficient to prevent the high-voltage RF power from leaking into the receive coil.
- Heating and performance test. The heating and performance test checks the heating on the surface of the RF receive coil due to RF or gradient coil switching by running the default Siemens pulse sequences, namely grad-free pulse or fidseq. The grad-free pulse sequence parameters were selected with the number of averages = 100, TR = 2.5 s, and five measurements running for 5 min. The fidseq sequence parameters were selected to create an applied B1 field of the Body coil with 30 μT and a duty cycle of 5% over 15 min. The change in surface temperature ∆T before and after every measurement must be ≤4 °C.
2.3. MRI Imaging
2.3.1. Phantom Imaging
2.3.2. Human Imaging
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathieu, D. Handbook on Hyperbaric Medicine; Springer: Dordrecht, The Netherlands, 2006; p. xix. 812p. [Google Scholar]
- Moon, R.E.; Mitchell, S.J. Hyperbaric oxygen for decompression sickness. Undersea Hyperb. Med. 2021, 48, 195–203. Available online: https://www.ncbi.nlm.nih.gov/pubmed/33975411 (accessed on 21 June 2022). [CrossRef] [PubMed]
- Fujita, M.; Todani, M.; Kaneda, K.; Suzuki, S.; Wakai, S.; Kikuta, S.; Sasaki, S.; Hattori, N.; Yagishita, K.; Kuwata, K.; et al. Use of Hyperbaric Oxygen Therapy for Preventing Delayed Neurological Sequelae in Patients with Carbon Monoxide Poisoning: A Multicenter, Prospective, Observational Study in Japan. PLoS ONE 2021, 16, e0253602. [Google Scholar] [CrossRef] [PubMed]
- Tomoye, E.O.; Moon, R.E. Hyperbaric oxygen for intracranial abscess. Undersea Hyperb. Med. 2021, 48, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Ostrowski, R.P.; Stepien, K.; Pucko, E.; Matyja, E. The efficacy of hyperbaric oxygen in hemorrhagic stroke: Experimental and clinical implications. Arch. Med. Sci. 2017, 13, 1217–1223. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wu, J.; Xiao, N.; Li, B. Hyperbaric Oxygen Therapy Is Beneficial for the Improvement of Clinical Symptoms of Cerebral Palsy: A Systematic Review and Meta-Analysis. Complement. Med. Res. 2022, 29, 158–171. [Google Scholar] [CrossRef]
- Bennett, M.H. Evidence brief: Hyperbaric oxygen therapy (HBOT) for traumatic brain injury and/or post-traumatic stress disorder. Diving Hyperb. Med. 2018, 48, 115. [Google Scholar] [CrossRef] [PubMed]
- Kirkland, P.J.; Mathew, D.; Modi, P.; Cooper, J.S. Nitrogen Narcosis in Diving; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Wingelaar, T.T.; van Ooij, P.-J.A.M.; Brinkman, P.; van Hulst, R.A. Pulmonary Oxygen Toxicity in Navy Divers: A Crossover Study Using Exhaled Breath Analysis After a One-Hour Air or Oxygen Dive at Nine Meters of Sea Water. Front. Physiol. 2019, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Belliveau, J.W.; Kennedy, D.N., Jr.; McKinstry, R.C.; Buchbinder, B.R.; Weisskoff, R.M.; Cohen, M.S.; Vevea, J.M.; Brady, T.J.; Rosen, B.R. Functional mapping of the human visual cortex by magnetic resonance imaging. Science 1991, 254, 716–719. Available online: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=1948051 (accessed on 3 December 2020). [CrossRef] [PubMed]
- Heyboer, M., III. Hyperbaric Oxygen Therapy Side Effects—Where Do We Stand? J. Am. Coll. Clin. Wound Spec. 2016, 8, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Altintop, I.; Akcin, M.E.; Tatli, M.; Ilbasmis, M.S. Factors that influence the decision for hyperbaric oxygen therapy (HBOT) in cases of carbon monoxide poisoning: A retrospective study. Ann. Burn. Fire Disasters 2018, 31, 168–173. Available online: https://www.ncbi.nlm.nih.gov/pubmed/30863246 (accessed on 28 October 2020).
- Chavez, S.; Storey, P.; Graham, S.J. Robust correction of spike noise: Application to diffusion tensor imaging. Magn. Reason. Med. 2009, 62, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Foo, T.F.; Grigsby, N.S.; Mitchell, J.D.; Slayman, B.E. SNORE: Spike noise removal and detection. IEEE Trans. Med. Imaging 1994, 13, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Haacke, E.M.; Lenz, G.W.; Nelson, A.D. Pseudo-gating: Elimination of periodic motion artifacts in magnetic resonance imaging without gating. Magn. Reason. Med. 1987, 4, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Yi-Hsuan, K.; MacFall, J.R. Correction of MR k-space data corrupted by spike noise. IEEE Trans. Med. Imaging 2000, 19, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.; Gustafson, C.; Ray, R.; Hendrick, R. MRI: Principles and Artifacts; Hendrick, R.E., Russ, P.D., Simon, J.H., Eds.; Raven: Nashville, TN, USA, 1993; pp. 270–271. [Google Scholar]
- Wald, L.; Wiggins, G.; Potthast, A.; Wiggins, C.; Triantafyllou, C. Design Considerations and Coil Comparisons for 7 T Brain Imaging. Appl. Magn. Reason. 2005, 29, 19. [Google Scholar] [CrossRef]
- Roemer, P.B.; Edelstein, W.A.; Hayes, C.E.; Souza, S.P.; Mueller, O.M. The NMR phased array. Magn. Reason. Med. 1990, 16, 192–225. Available online: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=2266841 (accessed on 3 December 2020). [CrossRef]
- Seeber, D.A.; Jevtic, J.; Menon, A. Floating shield current suppression trap. Concepts Magn. Reason. Part B Magn. Reason. Eng. 2004, 21B, 26–31. [Google Scholar] [CrossRef]
- Noordegraaf, J.; Hull, H. C-shield parylene allows major weight saving for EM shielding of microelectronics. In Proceedings of the First IEEE International Symposium on Polymeric Electronics Packaging, PEP ′97 (Cat. No.97TH8268), Norrkoping, Sweden, 30 October 1997; pp. 189–196. [Google Scholar] [CrossRef]
- Fortin, J.B.; Lu, T.M. Chemical Vapor Deposition Polymerization: The Growth and Properties of Parylene Thin Films; Kluwer Academic Publishers: Boston, MA, USA, 2004; p. xvi. 102p. [Google Scholar]
- Winchester, M.R.; Payling, R. Radio-frequency glow discharge spectrometry: A critical review. Spectrochim. Acta Part B At. Spectrosc. 2004, 59, 607–666. [Google Scholar] [CrossRef]
- Asfani, D.A.; Negara, I.M.Y.; Fahmi, D.; Wiryatama, R.; Haq, M.W.A.; Wahyudi, M. Analysis of low voltage arcing characteristic on direct short circuit through arcing thermal synchronization sensing and short circuit current. In Proceedings of the 2017 International Seminar on Intelligent Technology and Its Applications (ISITIA), Surabaya, Indonesia, 28–29 August 2017; pp. 165–168. [Google Scholar] [CrossRef]
- Kellman, P.; McVeigh, E.R. Image reconstruction in SNR units: A general method for SNR measurement. Magn. Reason. Med. 2005, 54, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B. FreeSurfer. Neuroimage 2012, 62, 774–781. [Google Scholar] [CrossRef]
- FDA. Testing and Labeling Medical Devices for Safety in the Magnetic Resonance (MR) Environment; Center for Devices and Radiological Health, Ed.; FDA: Washington, DC, USA, 2021.
- Davids, M.; Guerin, B.; Klein, V.; Wald, L.L. Optimization of MRI Gradient Coils With Explicit Peripheral Nerve Stimulation Constraints. IEEE Trans. Med. Imaging 2021, 40, 129–142. [Google Scholar] [CrossRef]
- Davids, M.; Guérin, B.; Endt, A.V.; Schad, L.R.; Wald, L.L. Prediction of peripheral nerve stimulation thresholds of MRI gradient coils using coupled electromagnetic and neurodynamic simulations. Magn. Reason. Med. 2019, 81, 686–701. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.R.; Katznelson, E. The modular gradient coil: An holistic approach to power efficient and high performance whole-body MRI without peripheral nerve stimulation. MAGMA 1999, 9, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Ham, C.L.; Engels, J.M.; van de Wiel, G.T.; Machielsen, A. Peripheral nerve stimulation during MRI: Effects of high gradient amplitudes and switching rates. J. Magn. Reason. Imaging 1997, 7, 933–937. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.P.; Diamant, A.M. Theoretical evaluation of peripheral nerve stimulation during MRI with an implanted spinal fusion stimulator. Magn. Reason. Imaging 1997, 15, 1145–1156. [Google Scholar] [CrossRef]
- Reilly, J.P. Applied Bioelectricity: From Electrical Stimulation to Electropathology; Springer: Berlin/Heidelberg, Germany, 1998; 632p. [Google Scholar]
- Chronik, B.A.; Ramachandran, M. Simple anatomical measurements do not correlate significantly to individual peripheral nerve stimulation thresholds as measured in MRI gradient coils. J. Magn. Reason. Imaging 2003, 17, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.K.; Bassen, H.; Osepchuk, J.; Balzano, Q.; Petersen, R.; Meltz, M.; Cleveland, R.; Lin, J.C.; Heynick, L. Radio frequency electromagnetic exposure: Tutorial review on experimental dosimetry. Bioelectromagnetics 1996, 17, 195–208. [Google Scholar] [CrossRef]
- Reilly, P.J. Maximum pulsed electromagnetic field limits based on peripheral nerve stimulation: Application to IEEE/ANSI C95.1 electromagnetic field standards. IEEE Trans. Biomed. Eng. 1998, 45, 137–141. [Google Scholar] [CrossRef]
- Kanal, E.; Shellock, F.G. Burns associated with clinical MR examinations. Radiology 1990, 175, 585. [Google Scholar] [CrossRef]
- Kanal, E.; Shellock, F.G.; Talagala, L. Safety considerations in MR imaging. Radiology 1990, 176, 593–606. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.B.; Charles, C.; Boswell, R.W. Breakdown behavior in radio-frequency argon discharges. Phys. Plasmas 2003, 10, 875–881. [Google Scholar] [CrossRef]
- Davis, T.L.; Kwong, K.K.; Weisskoff, R.M.; Rosen, B.R. Calibrated functional MRI: Mapping the dynamics of oxidative metabolism. Proc. Natl. Acad. Sci. USA 1998, 95, 1834–1839. [Google Scholar] [CrossRef] [PubMed]
- Hoge, R.D.; Atkinson, J.; Gill, B.; Crelier, G.R.; Marrett, S.; Pike, G.B. Investigation of BOLD signal dependence on cerebral blood flow and oxygen consumption: The deoxyhemoglobin dilution model. Magn. Reason. Med. 1999, 42, 849–863. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mareyam, A.; Shank, E.; Wald, L.L.; Qin, M.K.; Bonmassar, G. A New Phased-Array Magnetic Resonance Imaging Receive-Only Coil for HBO2 Studies. Sensors 2022, 22, 6076. https://doi.org/10.3390/s22166076
Mareyam A, Shank E, Wald LL, Qin MK, Bonmassar G. A New Phased-Array Magnetic Resonance Imaging Receive-Only Coil for HBO2 Studies. Sensors. 2022; 22(16):6076. https://doi.org/10.3390/s22166076
Chicago/Turabian StyleMareyam, Azma, Erik Shank, Lawrence L. Wald, Michael K. Qin, and Giorgio Bonmassar. 2022. "A New Phased-Array Magnetic Resonance Imaging Receive-Only Coil for HBO2 Studies" Sensors 22, no. 16: 6076. https://doi.org/10.3390/s22166076