
Non-Contact Breathing Monitoring Using Sleep Breathing Detection Algorithm (SBDA) Based on UWB Radar Sensors

 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
- This paper discusses the implementation of a variance feature with wavelet decomposition for signal clutter removal using an interval dependent threshold method.
- Periodic motion detection was detected by monitoring the periodicity of the signal via applying a sine curve fitting algorithm to match the output signal through a calculated R-square value.
- Ensemble Empirical Mode Decomposition (EEMD) with a Fast Fourier Transform (FFT) was implemented for extracting BR.
2. Related Work
3. Method
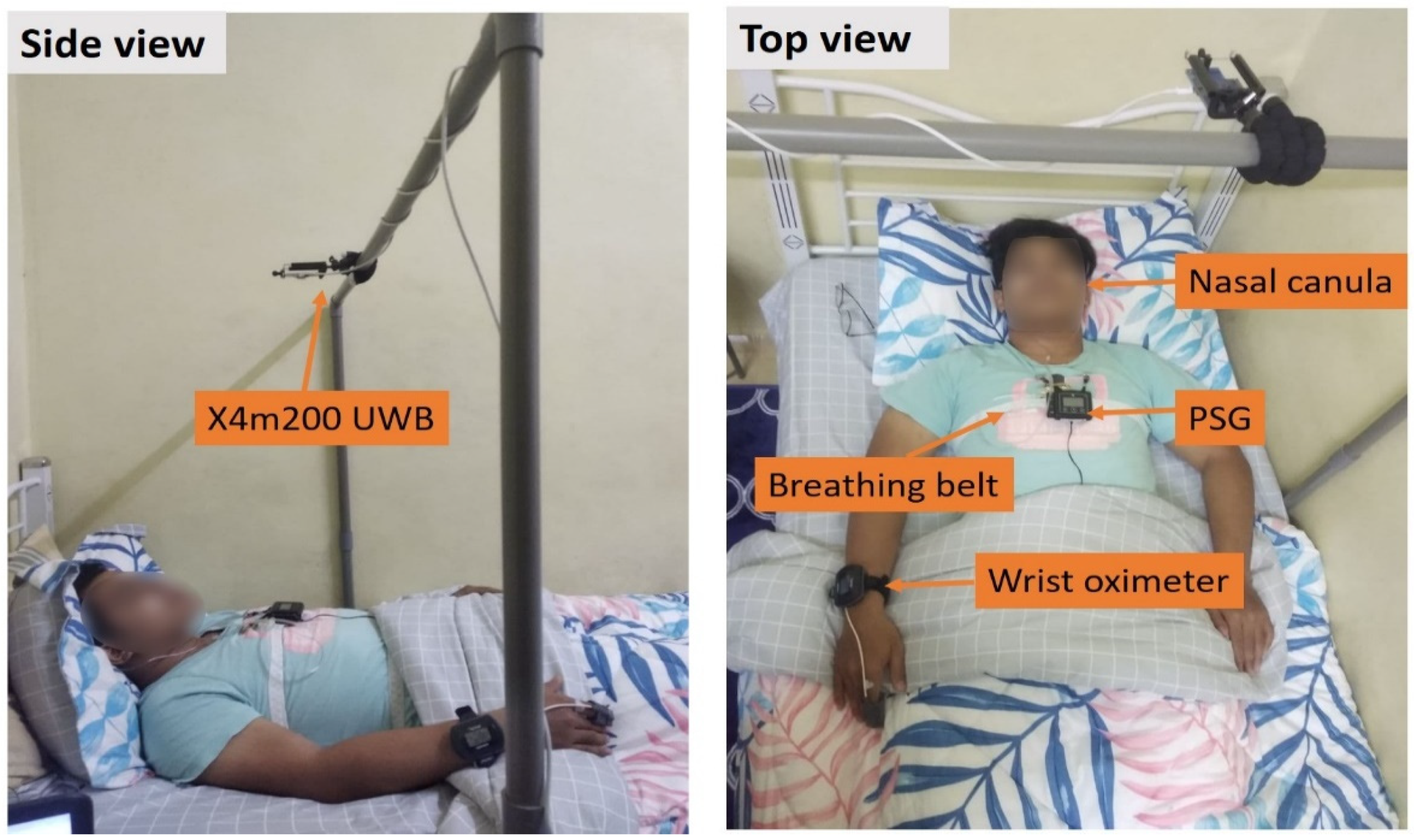
3.1. Data Collection
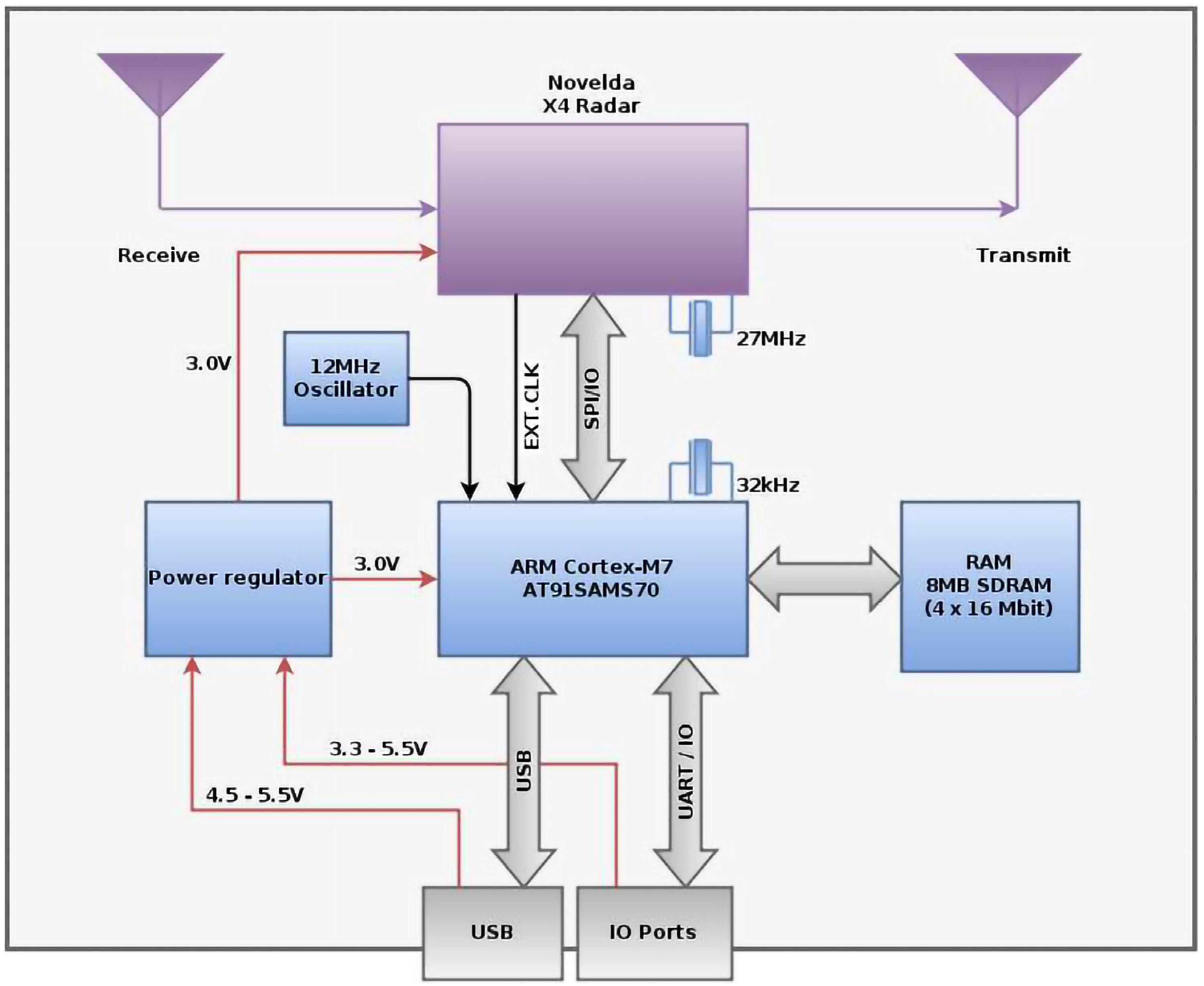
3.2. UWB Radar Working Principle
3.3. Sleep Breathing Detection Algorithm (SBDA)
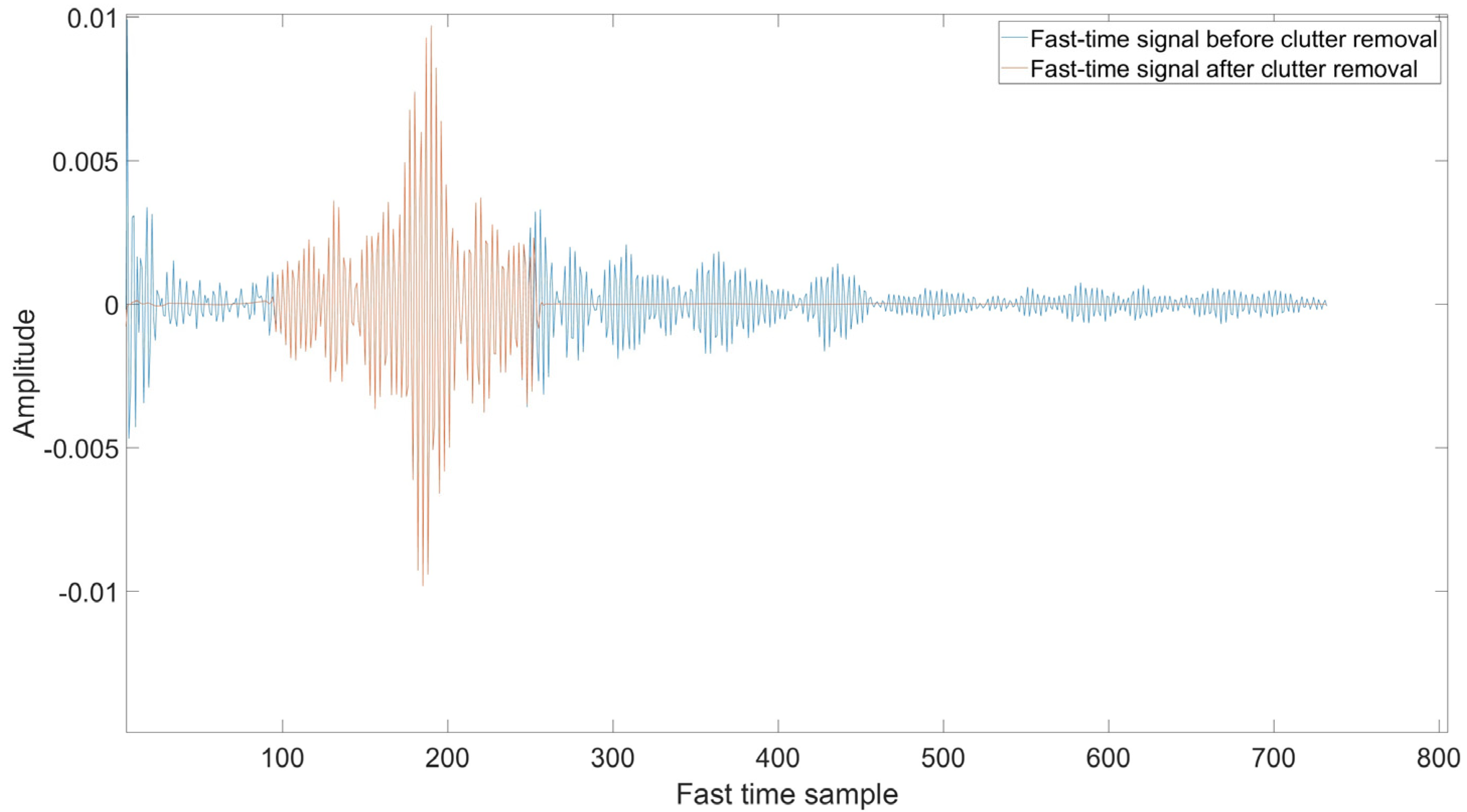
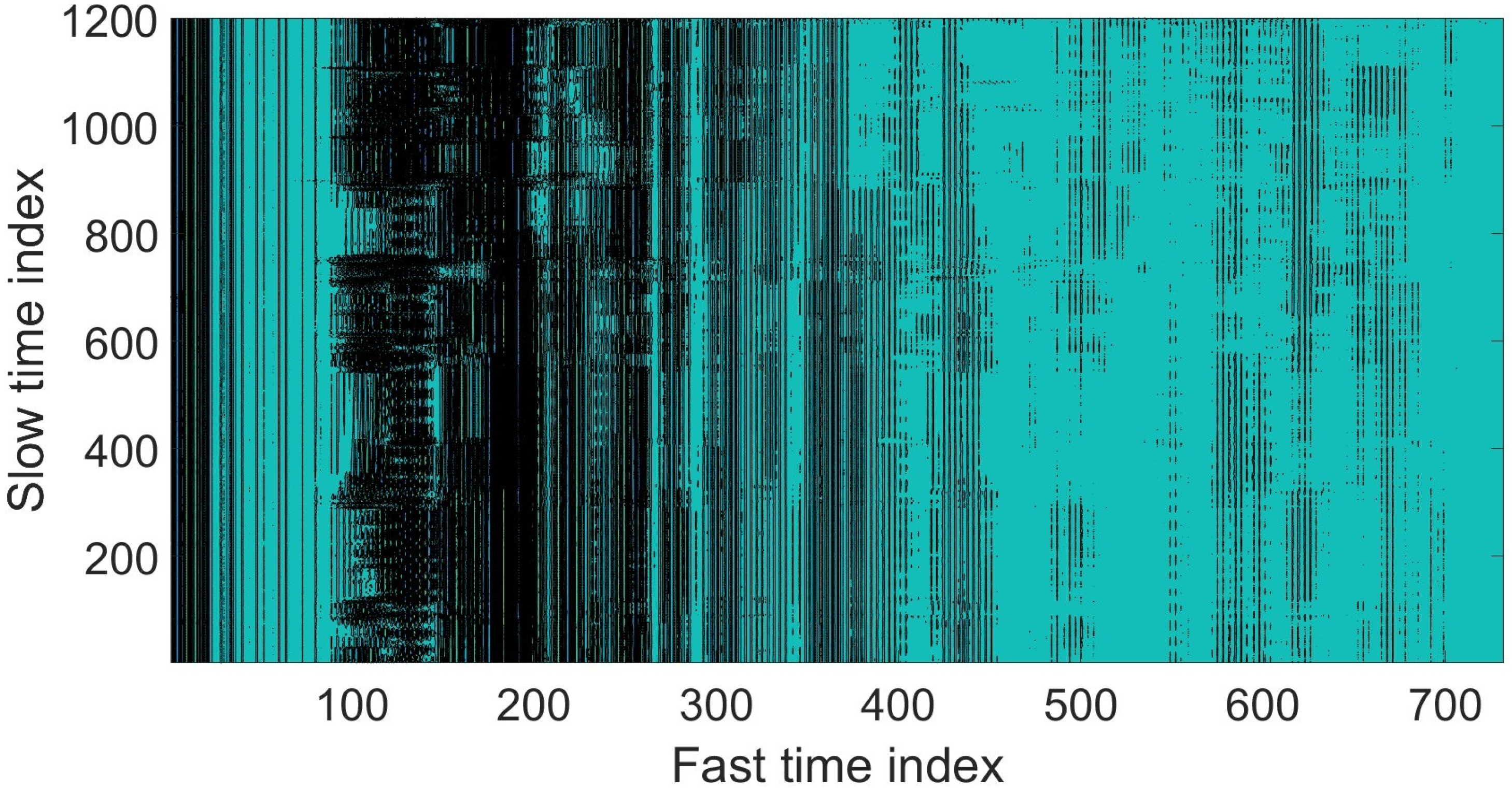
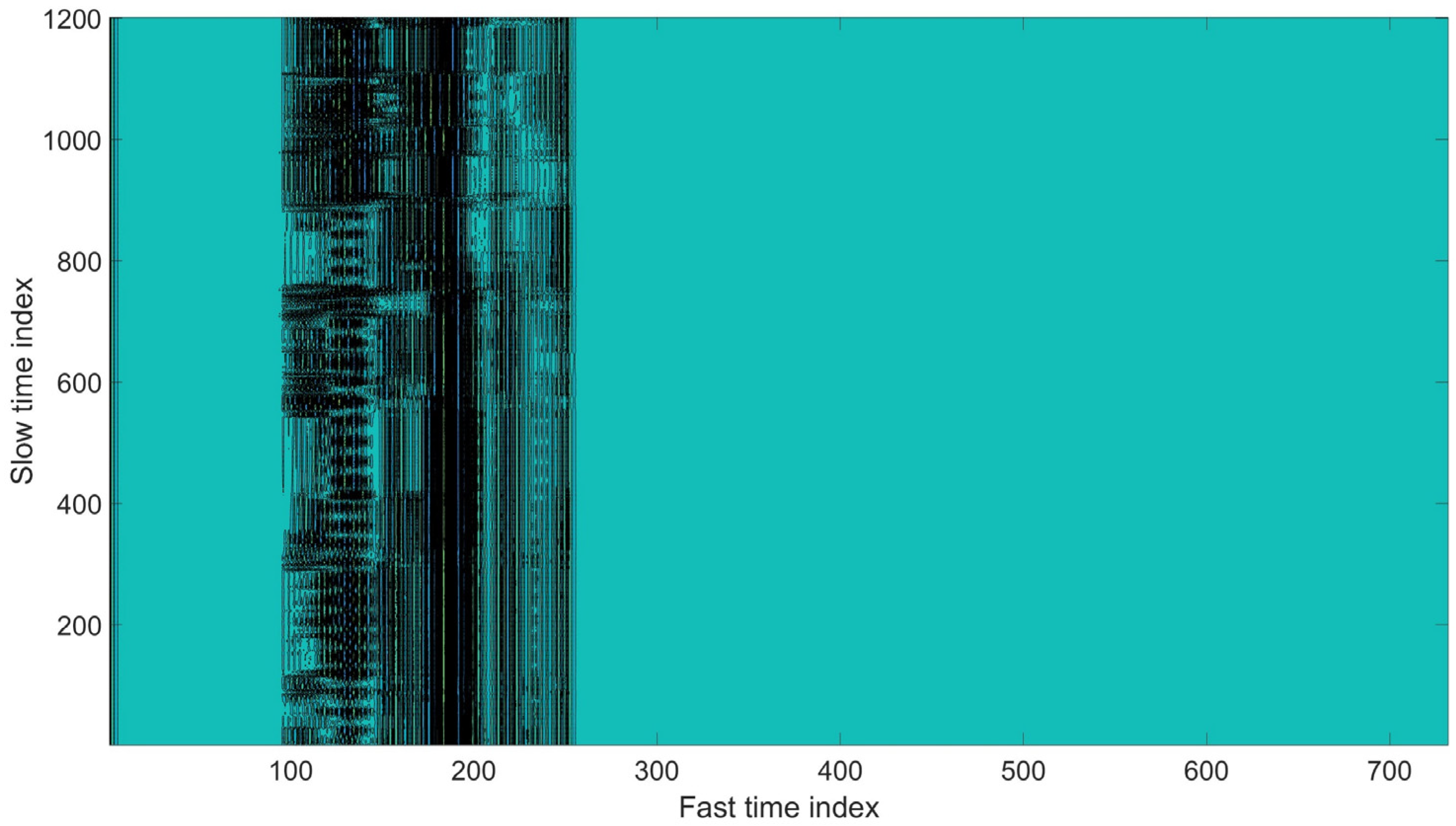
3.3.1. Clutter Suppression
- A decompose the signal in order to satisfy the signal-to-noise ratio in the signal.
- Select threshold detail coefficients. This paper adopts a dependent threshold method due to the behavior of the signal. The threshold was selected based on the width of the variance curve signal. A soft threshold was applied to the detail coefficients.
- Reconstruction. To reconstruct the signal, Inverse Wavelet Transform (IWT) was used to obtain a de-noised signal.
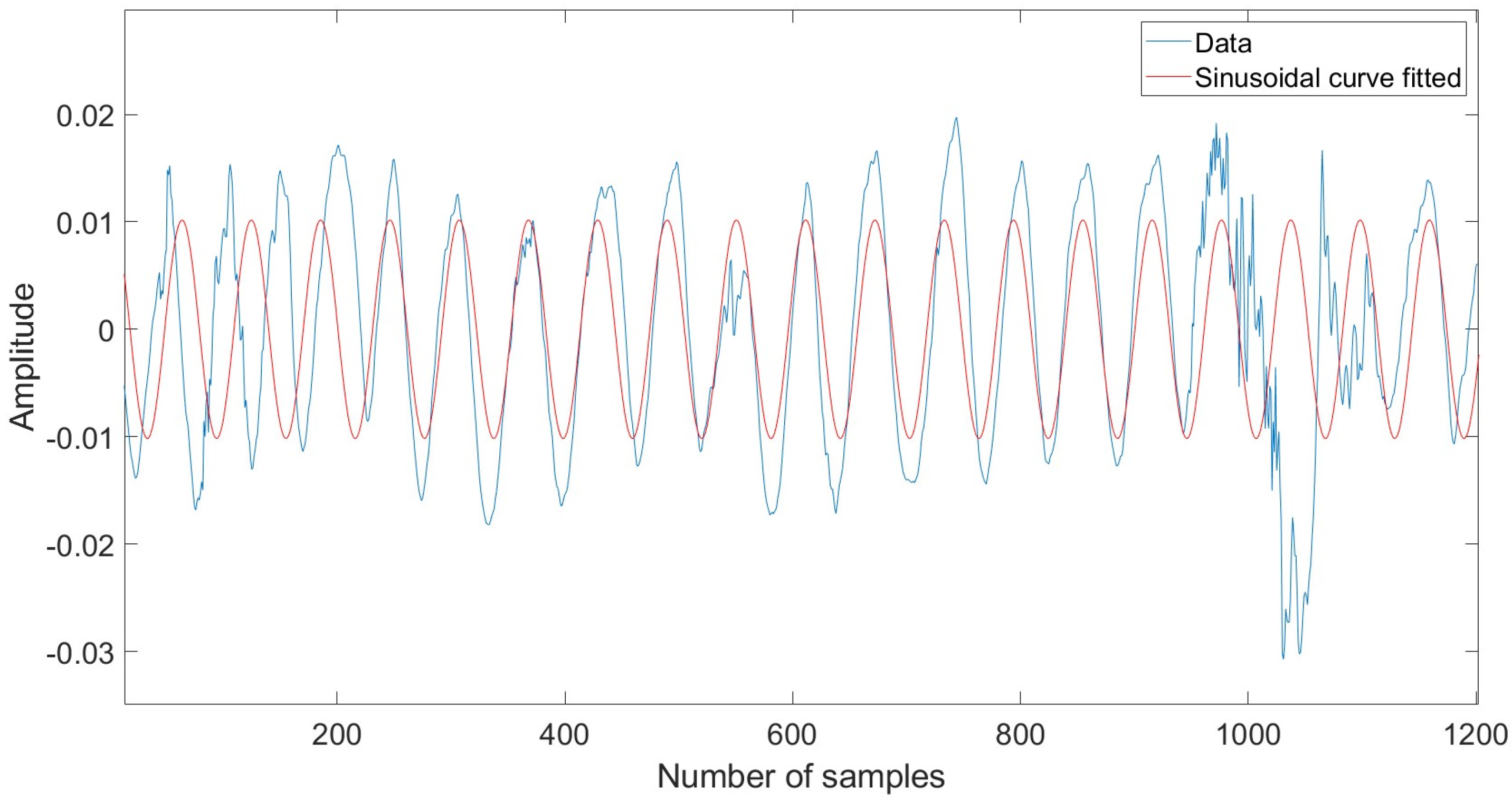
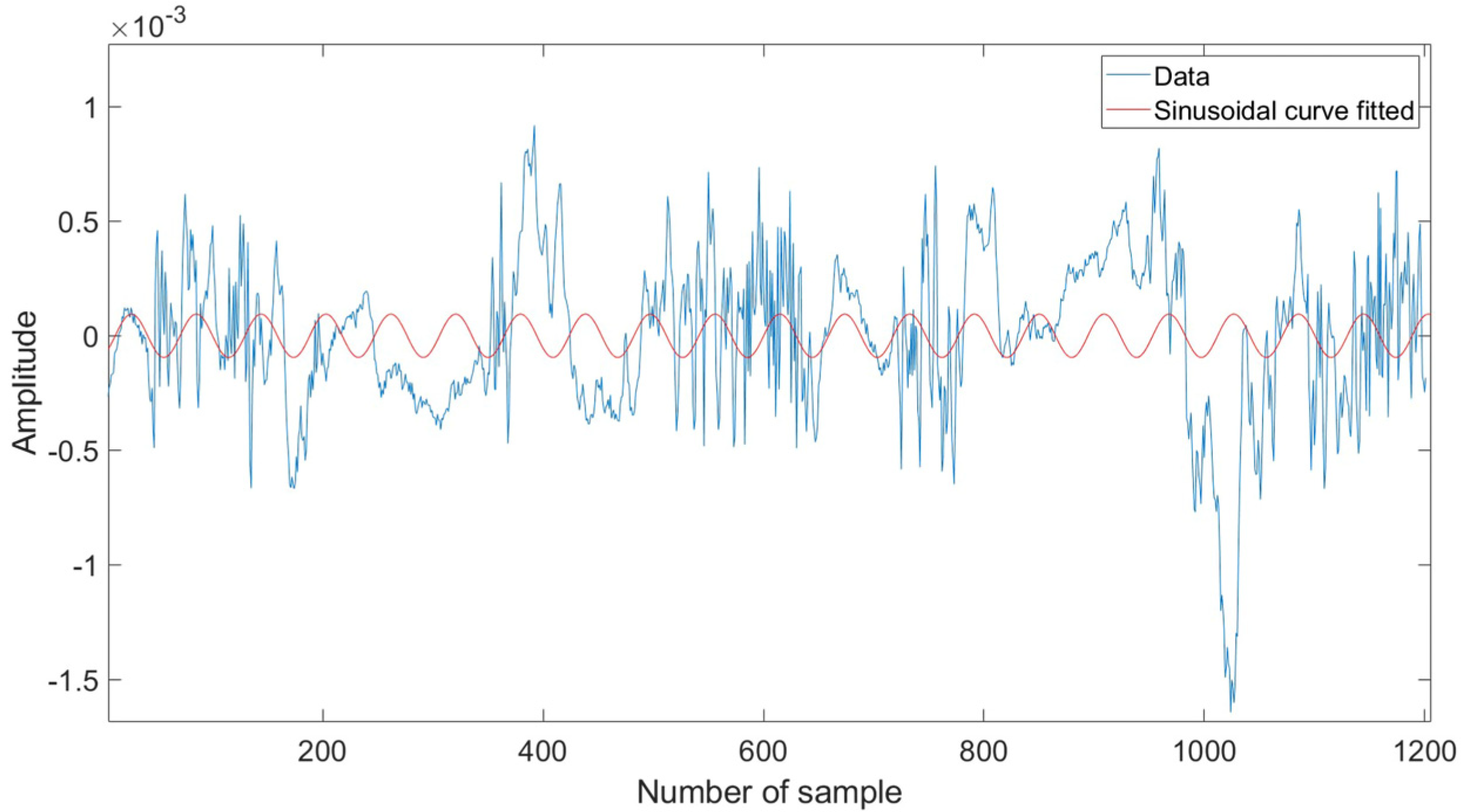
3.3.2. Periodic Motion Detection
- The general sine curve fitting algorithm procedure in this paper involves three steps as detailed below.
- Apply the sine curve fit in Equation (6) which gives amplitude, frequency, and phase constant for the best fit to the raw signals.
- Determine the R-square value for each signal using Equation (7).
- Find the signals with an R-square value above a threshold value.
3.3.3. Ensemble Empirical Mode Decomposition Approach
- 1.
- Add Gaussian white noise to the input signal .where () are different realizations of Gaussian white noise and indicates the signal with Gaussian white noise.
- 2.
- Applied EMD algorithm to the signal for obtaining the component.
- 3.
- Add other white noise to the observation signal again and repeat step 1 and 2 until times.
- 4.
- Perform average operation on component which has times trials for obtaining new component.
- 5.
- Final EEMD can be written as
3.3.4. ’s Selection and Signal Reconstruction Methods
4. Result
4.1. Clutter Removal
4.2. Respiration Signal Extraction
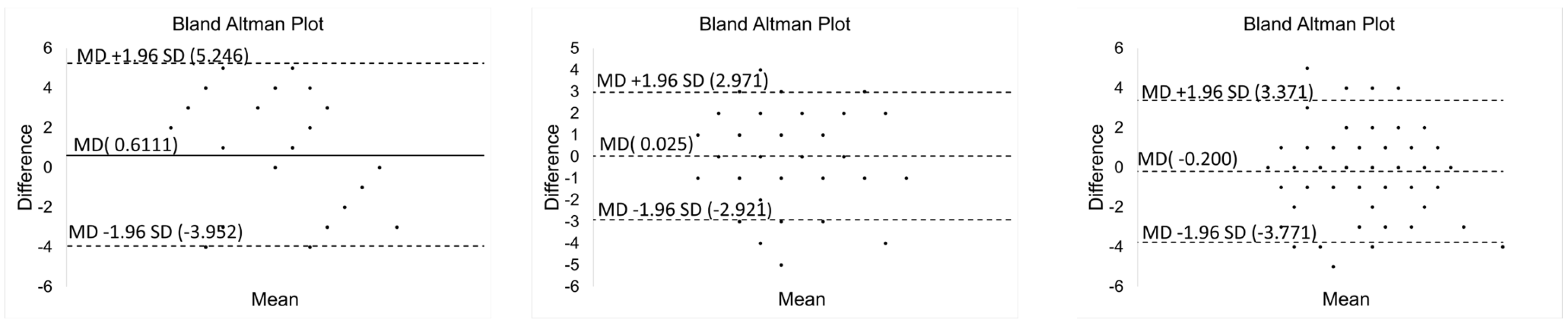
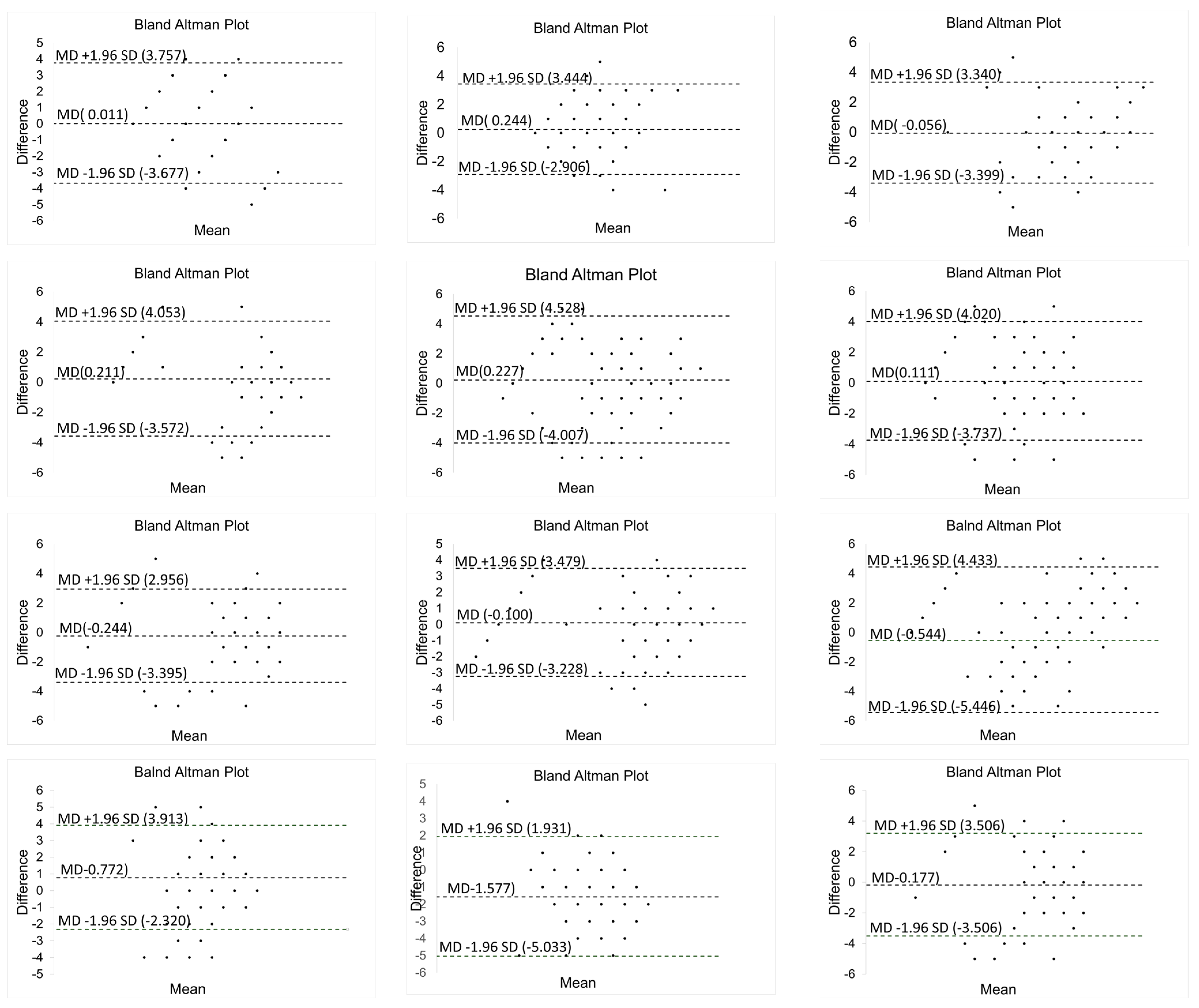
4.3. Agreement of Proposed Method with PSG Device
4.4. Comparison with Other Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosenberg, A.L.; Watts, C. Patients readmitted to ICUs: A systematic review of risk factors and outcomes. Chest 2000, 118, 492–502. [Google Scholar] [CrossRef] [PubMed]
- Goldhill, D.R.; McNarry, A.F.; Mandersloot, G.; McGinley, A. A physiologically-based early warning score for ward patients: The association between score and outcome. Anaesthesia 2005, 60, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Yuan, G.; Drost, N.; McIvor, R. Respiratory Rate and Breathing Pattern. McMaster Univ. Med. J. 2013, 10, 23–25. [Google Scholar]
- Fleming, S.; Thompson, M.; Stevens, R.; Heneghan, C.; Plüddemann, A.; MacOnochie, I.; Tarassenko, L.; Mant, D. Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: A systematic review of observational studies. Lancet 2011, 377, 1011–1018. [Google Scholar] [CrossRef] [Green Version]
- White, D.P. Pathogenesis of obstructive and central sleep apnea. Am. J. Respir. Crit. Care Med. 2005, 172, 1363–1370. [Google Scholar] [CrossRef] [Green Version]
- Latten, G.H.P.; Spek, M.; Muris, J.W.M.; Cals, J.W.L.; Stassen, P.M. Accuracy and interobserver-agreement of respiratory rate measurements by healthcare professionals, and its effect on the outcomes of clinical prediction/diagnostic rules. PLoS ONE 2019, 14, e0223155. [Google Scholar] [CrossRef] [Green Version]
- Mukkamala, S.G.; Gennings, C.; Wenzel, R.P. R = 20: Bias in the reporting of respiratory rates. Am. J. Emerg. Med. 2008, 26, 237–239. [Google Scholar] [CrossRef]
- Sun, Z.; Sessler, D.I.; Dalton, J.E.; Devereaux, P.; Shahinyan, A.; Naylor, A.J.; Hutcherson, M.T.; Finnegan, P.S.; Tandon, V.; Darvish-Kazem, S.; et al. Postoperative Hypoxemia Is Common and Persistent: A Prospective Blinded Observational Study. Anesth. Analg. 2015, 121, 709. [Google Scholar] [CrossRef] [Green Version]
- Subbe, C.P.; Kinsella, S. Continuous monitoring of respiratory rate in emergency admissions: Evaluation of the respirasenseTM sensor in acute care compared to the industry standard and gold standard. Sensors 2018, 18, 2700. [Google Scholar] [CrossRef] [Green Version]
- Verkruysse, W.; Svaasand, L.O.; Nelson, J.S. Remote plethysmographic imaging using ambient light. Opt. Express 2008, 16, 21434–21445. [Google Scholar] [CrossRef] [Green Version]
- Nam, Y.; Reyes, B.A.; Chon, K.H. Estimation of Respiratory Rates Using the Built-in Microphone of a Smartphone or Headset. IEEE J. Biomed. Health Inform. 2016, 20, 1493–1501. [Google Scholar] [CrossRef] [PubMed]
- Ge, L.; Zhang, J.; Wei, J. Single-Frequency Ultrasound-Based Respiration Rate Estimation with Smartphones. Comput. Math. Methods Med. 2018, 2018, 3675974. [Google Scholar] [CrossRef] [Green Version]
- Li, S.H.; Lin, B.S.; Tsai, C.H.; Yang, C.T.; Lin, B.S. Design of wearable breathing sound monitoring system for real-time wheeze detection. Sensors 2017, 17, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baboli, M.; Singh, A.; Soll, B.; Boric-Lubecke, O.; Lubecke, V.M. Wireless Sleep Apnea Detection Using Continuous Wave Quadrature Doppler Radar. IEEE Sens. J. 2020, 20, 538–545. [Google Scholar] [CrossRef]
- Cardillo, E.; Caddemi, A. Feasibility Study to Preserve the Health of an Industry 4.0 Worker: A Radar System for Monitoring the Sitting-Time. In Proceedings of the 2019 II Workshop on Metrology for Industry 4.0 and IoT (MetroInd4.0&IoT), Naples, Italy, 4–6 June 2019; pp. 254–258. [Google Scholar] [CrossRef]
- Fernandes, J.R.; Wentzloff, D. Recent advances in IR-UWB transceivers: An overview. In Proceedings of the 2010 IEEE International Symposium on Circuits and Systems, Paris, France, 30 May–2 June 2010; pp. 3284–3287. [Google Scholar] [CrossRef]
- Choi, J.W.; Yim, D.H.; Cho, S.H. People Counting Based on an IR-UWB Radar Sensor. IEEE Sens. J. 2017, 17, 5717–5727. [Google Scholar] [CrossRef]
- Leem, S.K.; Khan, F.; Cho, S.H. Vital sign monitoring and mobile phone usage detection using IR-UWB radar for intended use in car crash prevention. Sensors 2017, 17, 1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghaffar, A.; Khan, F.; Cho, S.H. Hand Pointing Gestures Based Digital Menu Board Implementation Using IR-UWB Transceivers. IEEE Access 2019, 7, 58148–58157. [Google Scholar] [CrossRef]
- Kang, S.; Kim, D.K.; Lee, Y.; Lim, Y.H.; Park, H.K.; Cho, S.H.; Cho, S.H. Non-contact diagnosis of obstructive sleep apnea using impulse-radio ultra-wideband radar. Sci. Rep. 2020, 10, 6–12. [Google Scholar] [CrossRef]
- Wang, D.; Yoo, S.; Cho, S.H. Experimental comparison of ir-uwb radar and fmcw radar for vital signs. Sensors 2020, 20, 6695. [Google Scholar] [CrossRef]
- Alarifi, A.; Al-Salman, A.; Alsaleh, M.; Alnafessah, A.; Al-Hadhrami, S.; Al-Ammar, M.A.; Al-Khalifa, H.S. Ultra wideband indoor positioning technologies: Analysis and recent advances. Sensors 2016, 16, 707. [Google Scholar] [CrossRef]
- Aiello, R.; Batra, A. Ultra Wideband Systems: Technologies and Applications; Elsevier: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Sachdev, P.S. Neuropsychiatric dimensions of movement disorders in sleep. Psychiatr. Times 2006, 23, 41–43. [Google Scholar]
- Khan, F.; Ghaffar, A.; Khan, N.; Cho, S.H. An overview of signal processing techniques for remote health monitoring using impulse radio UWB transceiver. Sensors 2020, 20, 2479. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Bocca, M.; Jain, V.; Mohapatra, P. Contactless breathing rate monitoring in vehicle using UWB radar. In Proceedings of the 7th International Workshop on Real-World Embedded Wireless Systems and Networks, Shenzhen, China, 4 November 2018; pp. 13–18. [Google Scholar] [CrossRef]
- Eren, C.; Karamzadeh, S.; Kartal, M. The artifacts of human physical motions on vital signs monitoring. In Proceedings of the 2019 Scientific Meeting on Electrical-Electronics & Biomedical Engineering and Computer Science (EBBT), Istanbul, Turkey, 24–26 April 2019; pp. 1–5. [Google Scholar]
- Lazaro, A.; Girbau, D.; Villarino, R. Analysis of vital signs monitoring using an IR-UWB radar. Prog. Electromagn. Res. 2010, 100, 265–284. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Z.; Yang, D.; Zhao, R.; Liang, B. Vital sign signal extraction method based on permutation entropy and EMD algorithm for ultra-wideband radar. In Proceedings of the 2019 3rd International Conference on Electronic Information Technology and Computer Engineering (EITCE), Xiamen, China, 18–20 October 2019; pp. 1268–1273. [Google Scholar] [CrossRef]
- Khan, F.; Cho, S.H. A detailed algorithm for vital sign monitoring of a stationary/non-stationary human through IR-UWB radar. Sensors 2017, 17, 290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazaro, A.; Girbau, D.; Villarino, R. Techniques for clutter suppression in the presence of body movements during the detection of respiratory activity through UWB radars. Sensors 2014, 14, 2595–2618. [Google Scholar] [CrossRef] [PubMed]
- Adib, F.; Mao, H.; Kabelac, Z.; Katabi, D.; Miller, R.C. Smart homes that monitor breathing and heart rate. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems, Seoul, Korea, 18–23 April 2015; pp. 837–846. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, X.; Ding, Y.; Wang, Y.; Zhou, J.; Zhang, L. Contactless simultaneous breathing and heart rate detections in physical activity using ir-uwb radars. Sensors 2021, 21, 5503. [Google Scholar] [CrossRef]
- Chung, F.; Abdullah, H.R.; Liao, P. STOP-bang questionnaire a practical approach to screen for obstructive sleep apnea. Chest 2016, 149, 631–638. [Google Scholar] [CrossRef] [Green Version]
- Chiu, H.Y.; Chen, P.Y.; Chuang, L.P.; Chen, N.H.; Tu, Y.K.; Hsieh, Y.J.; Wang, Y.C.; Guilleminault, C. Diagnostic accuracy of the Berlin questionnaire, STOP-BANG, STOP, and Epworth sleepiness scale in detecting obstructive sleep apnea: A bivariate meta-analysis. Sleep Med. Rev. 2017, 36, 57–70. [Google Scholar] [CrossRef]
- Saeed, U.; Shah, S.Y.; Alotaibi, A.A.; Althobaiti, T.; Ramzan, N. Portable UWB RADAR Sensing System for Transforming Subtle Chest Movement into Actionable Micro-Doppler Signatures to Extract Respiratory Rate Exploiting ResNet Algorithm. IEEE Sens. J. 2021, 21, 23518–23526. [Google Scholar] [CrossRef]
- Tan, L.; Jiang, J. Subband and Wavelet-Based Coding. In Digital Signal Processing; McGraw-Hill: New York, NY, USA, 2019; pp. 591–648. ISBN 9780128150719. [Google Scholar] [CrossRef]
- Mallat, S.G. A theory for multiresolution signal decomposition: The wavelet representation. IEEE Trans. Pattern Anal. Mach. Intell. 1989, 11, 674–693. [Google Scholar] [CrossRef] [Green Version]
- Daubechies, I. The Wavelet Transform, Time-Frequency Localization and Signal Analysis. IEEE Trans. Inf. Theory 1990, 36, 961–1005. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Huang, N.E. Ensemble empirical mode decomposition: A noise-assisted data analysis method. Adv. Adapt. Data Anal. 2009, 1, 1–41. [Google Scholar] [CrossRef]
- Lin, S.H.N.; Lin, G.H.; Tsai, P.J.; Hsu, A.L.; Lo, M.T.; Yang, A.C.; Lin, C.P.; Wu, C.W. Sensitivity enhancement of task-evoked fMRI using ensemble empirical mode decomposition. J. Neurosci. Methods 2016, 258, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, L.; Zeng, Z.; Liu, F. Simulation and signal processing of UWB radar for human detection in complex environment. In Proceedings of the 2012 14th International Conference on Ground Penetrating Radar (GPR), Shanghai, China, 4–8 June 2012. [Google Scholar]
- Flandrin, P.; Rilling, G.; Gonçalvés, P. Empirical mode decomposition as a filter bank. IEEE Signal Process. Lett. 2004, 11, 112–114. [Google Scholar] [CrossRef] [Green Version]
- Huang, N.E.; Shen, Z.; Long, S.R.; Wu, M.C.; Snin, H.H.; Zheng, Q.; Yen, N.C.; Tung, C.C.; Liu, H.H. The empirical mode decomposition and the Hubert spectrum for nonlinear and non-stationary time series analysis. Proc. R. Soc. Lond. Ser. A Math. Phys. Eng. Sci. 1998, 454, 903–995. [Google Scholar] [CrossRef]
- Shen, H.; Xu, C.; Yang, Y.; Sun, L.; Cai, Z.; Bai, L.; Clancy, E.; Huang, X. Respiration and Heartbeat Rates Measurement Based on Autocorrelation Using IR-UWB Radar. IEEE Trans. Circuits Syst. II Express Briefs 2018, 65, 1470–1474. [Google Scholar] [CrossRef]
- Pittella, E.; Zanaj, B.; Pisa, S.; Cavagnaro, M. Measurement of Breath Frequency by Body-Worn UWB Radars: A Comparison among Different Signal Processing Techniques. IEEE Sens. J. 2017, 17, 1772–1780. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects | Age | Weight (kg) | Height (cm) | Neck Circumference (inch) | Gender | Epworth Score | STOPBANG Score | AHI | Rating |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 27 | 65 | 163 | 12.5 | Female | 9 | 1 | 4 | Normal |
| 2 | 26 | 57 | 163 | 12.0 | Female | 7 | 1 | 3.7 | Normal |
| 3 | 28 | 53 | 151 | 13.5 | Female | 6 | 0 | 2.8 | Normal |
| 4 | 28 | 40 | 158 | 12.5 | Female | 9 | 1 | 0.8 | Normal |
| 5 | 23 | 50 | 170 | 12.0 | Female | 8 | 1 | 0.4 | Normal |
| 6 | 42 | 100 | 162 | 16.5 | Female | 5 | 2 | 12 | Abnormal |
| 7 | 36 | 54 | 159 | 14.5 | Female | 6 | 0 | 1.3 | Normal |
| 8 | 24 | 76 | 150 | 15.0 | Female | 6 | 1 | 2.6 | Normal |
| 9 | 41 | 68 | 163 | 13.0 | Female | 13 | 1 | 5.4 | Abnormal |
| 10 | 42 | 101 | 169 | 17.0 | Male | 3 | 6 | 23.2 | Abnormal |
| 11 | 21 | 75 | 175 | 15.3 | Male | 8 | 2 | 0.8 | Normal |
| 12 | 42 | 108 | 168 | 15.0 | Male | 19 | 4 | 24.5 | Abnormal |
| 13 | 27 | 48 | 167 | 13.0 | Male | 9 | 2 | 5.5 | Abnormal |
| 14 | 38 | 81 | 178 | 15.2 | Male | 4 | 3 | 18.1 | Abnormal |
| 15 | 25 | 67 | 165 | 14.0 | Male | 8 | 3 | 2.7 | Normal |
| Subject | 3 | 4 | 5 | 6 | 7 | 10 |
|---|---|---|---|---|---|---|
| 1 | - | 0.0241 | 0.6642 | 0.5175 | 0.4550 | - |
| 2 | - | 0.1725 | 0.7565 | 0.6546 | 0.4040 | - |
| 3 | - | 0.0495 | 0.6554 | 0.5013 | 0.6563 | - |
| 4 | - | 0.2752 | 0.6701 | 0.5753 | 0.0051 | - |
| 5 | - | 0.1694 | 0.7490 | 0.5828 | 0.2768 | - |
| 6 | - | 0.3934 | 0.8145 | 0.6163 | 0.6916 | - |
| 7 | - | 0.5834 | 0.6768 | 0.5548 | 0.2016 | - |
| 8 | - | 0.0545 | 0.7918 | 0.5246 | 0.3457 | - |
| 9 | - | 0.2868 | 0.6443 | 0.6721 | 0.1725 | - |
| 10 | - | 0.5909 | 0.7223 | 0.5038 | 0.0341 | - |
| 11 | - | 0.0836 | 0.7718 | 0.6402 | 0.0020 | - |
| 12 | - | 0.0728 | 0.6104 | 0.5225 | 0.1039 | - |
| 13 | - | 0.2947 | 0.6174 | 0.6390 | 0.2253 | - |
| 14 | - | 0.1167 | 0.6145 | 0.5879 | 0.1146 | - |
| 15 | - | 0.2936 | 0.6250 | 0.5956 | 0.4659 | - |
| Percentage Error | |||
|---|---|---|---|
| Subject | Autocorrelation + FFT (%) [45] | Mean Subtraction + FFT (%) [46] | SBDA (%) |
| 1 | 14.20 | 20.38 | 8.02 |
| 2 | 11.22 | 15.75 | 6.69 |
| 3 | 9.53 | 11.50 | 7.56 |
| 4 | 8.02 | 8.39 | 7.66 |
| 5 | 12.57 | 16.65 | 8.49 |
| 6 | 10.65 | 14.04 | 7.25 |
| 7 | 11.73 | 18.65 | 4.81 |
| 8 | 16.77 | 26.47 | 7.08 |
| 9 | 7.11 | 8.20 | 6.02 |
| 10 | 9.91 | 15.77 | 4.05 |
| 11 | 9.56 | 13.24 | 5.88 |
| 12 | 9.98 | 14.96 | 5.01 |
| 13 | 9.81 | 14.89 | 4.73 |
| 14 | 9.64 | 14.83 | 4.45 |
| 15 | 9.46 | 14.76 | 4.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Husaini, M.; Kamarudin, L.M.; Zakaria, A.; Kamarudin, I.K.; Ibrahim, M.A.; Nishizaki, H.; Toyoura, M.; Mao, X. Non-Contact Breathing Monitoring Using Sleep Breathing Detection Algorithm (SBDA) Based on UWB Radar Sensors. Sensors 2022, 22, 5249. https://doi.org/10.3390/s22145249
Husaini M, Kamarudin LM, Zakaria A, Kamarudin IK, Ibrahim MA, Nishizaki H, Toyoura M, Mao X. Non-Contact Breathing Monitoring Using Sleep Breathing Detection Algorithm (SBDA) Based on UWB Radar Sensors. Sensors. 2022; 22(14):5249. https://doi.org/10.3390/s22145249
Chicago/Turabian StyleHusaini, Muhammad, Latifah Munirah Kamarudin, Ammar Zakaria, Intan Kartika Kamarudin, Muhammad Amin Ibrahim, Hiromitsu Nishizaki, Masahiro Toyoura, and Xiaoyang Mao. 2022. "Non-Contact Breathing Monitoring Using Sleep Breathing Detection Algorithm (SBDA) Based on UWB Radar Sensors" Sensors 22, no. 14: 5249. https://doi.org/10.3390/s22145249