
A New Immersive Virtual Reality Station for Cardiopulmonary Resuscitation Objective Structured Clinical Exam Evaluation

 , ,
, ,
Abstract
:1. Introduction
- Learning. The student follows a guided procedure to practice a specific skill.
- Training. The student receives real-time feedback and audio-visual stimulus to test the concentration.
- Assessment. The student faces a CPR test without any guide and receives real-time feedback from the physical mannequin.
2. Materials and Methods
2.1. CPR-OSCE VR: Design and Implementation
2.1.1. General Architecture
2.1.2. Services-Based Singleton Pattern
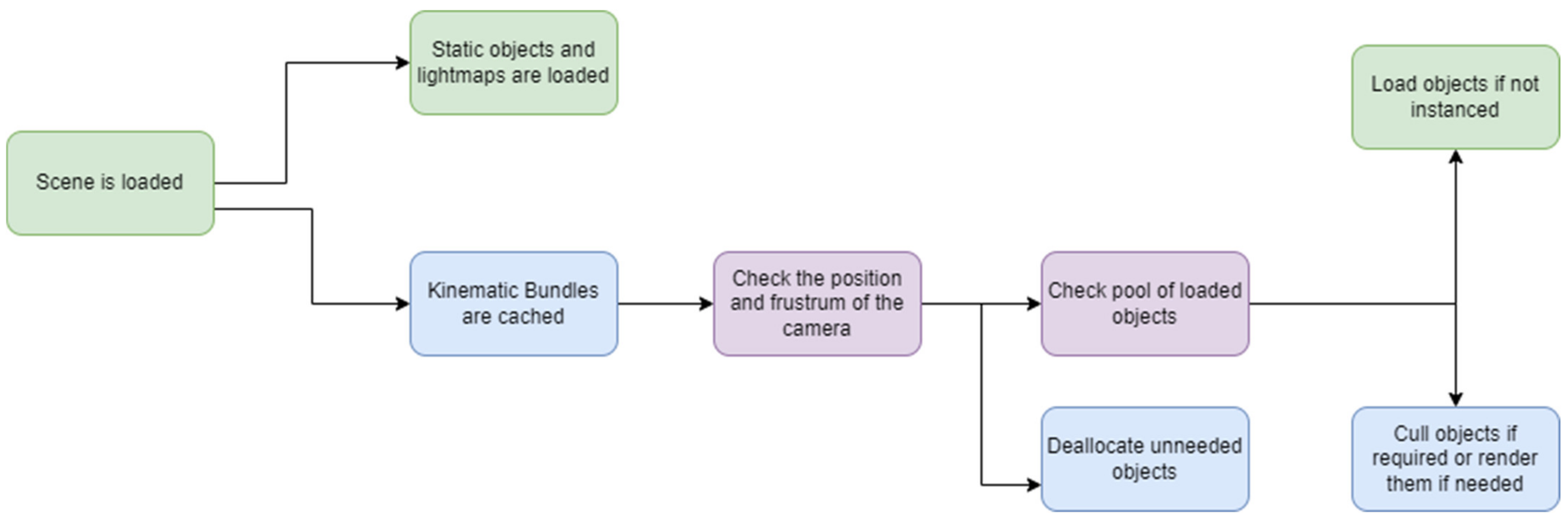
2.1.3. Scene Management and Asset Bundles
2.1.4. Rendering Optimizations
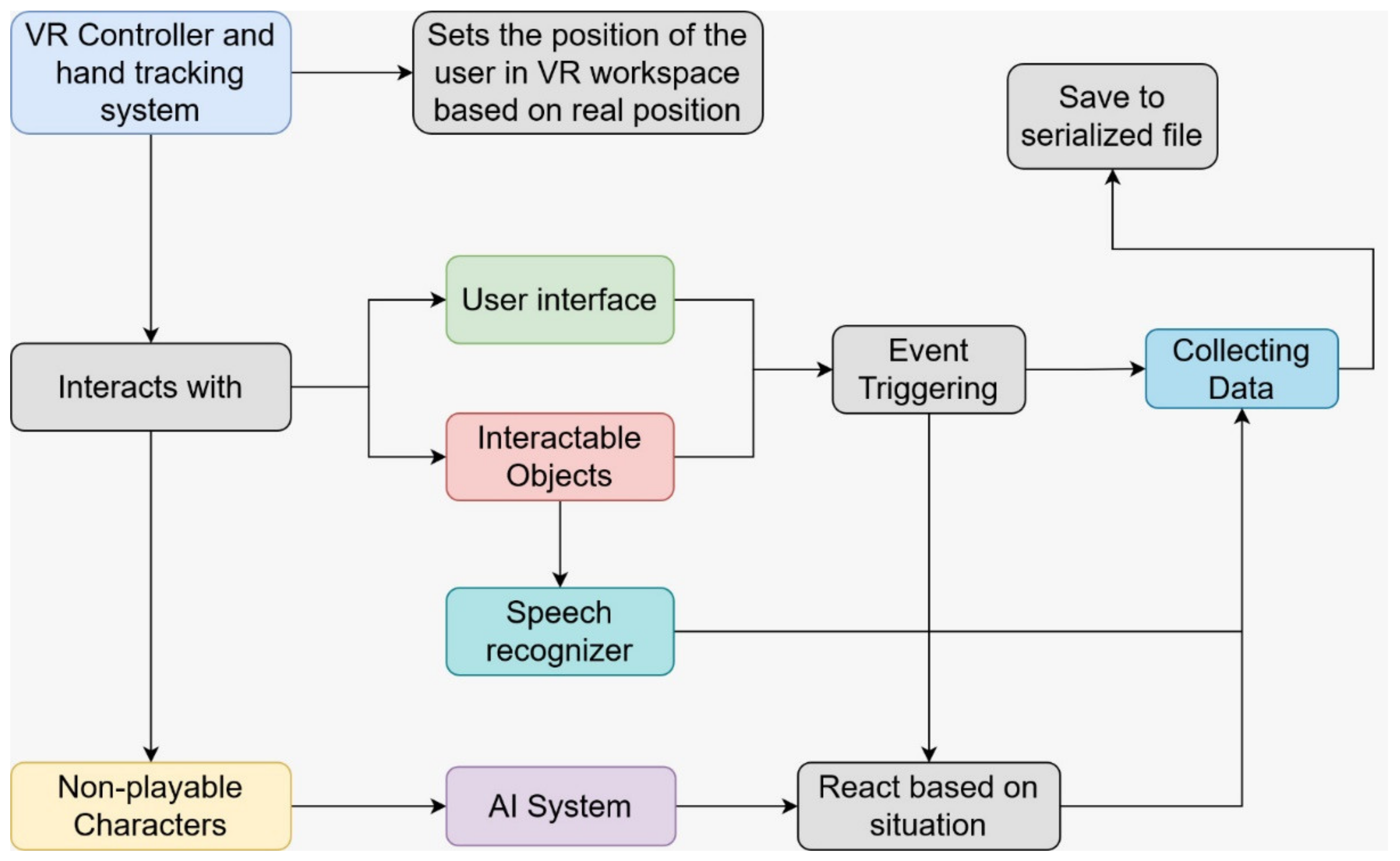
2.1.5. Control
2.1.6. Speech Recognition
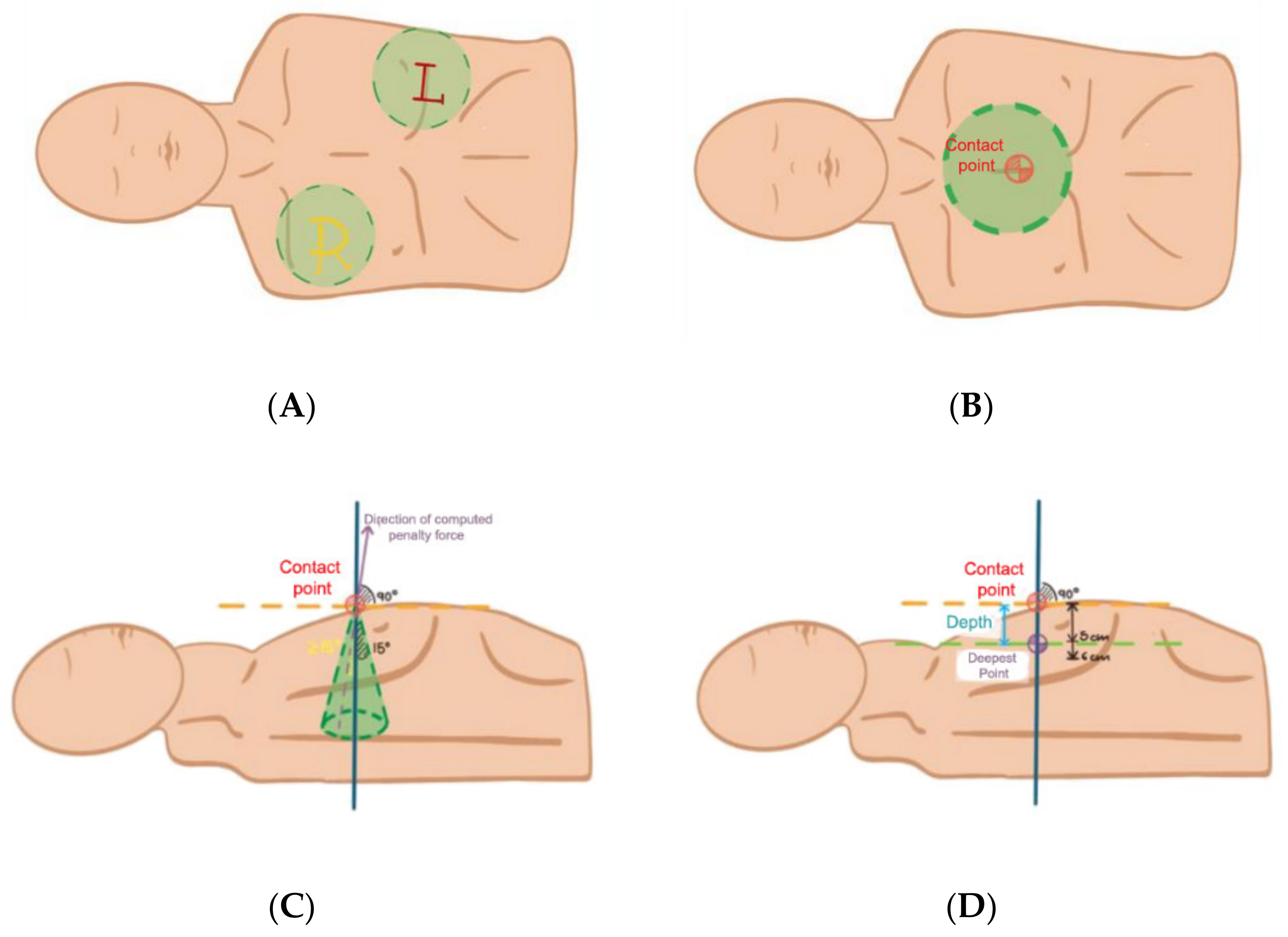
2.1.7. Performance Metrics
2.1.8. Video Streaming
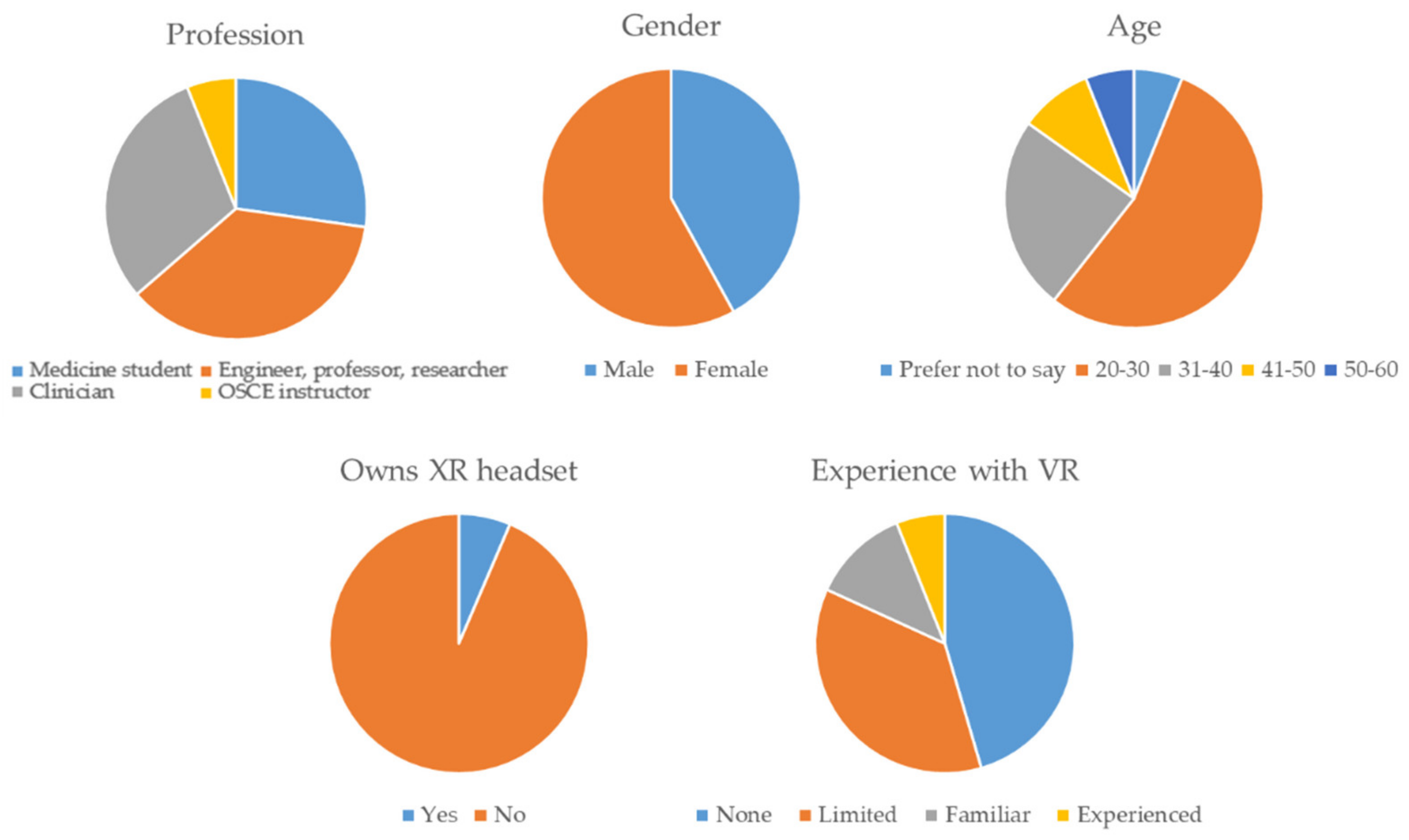
2.2. Validation
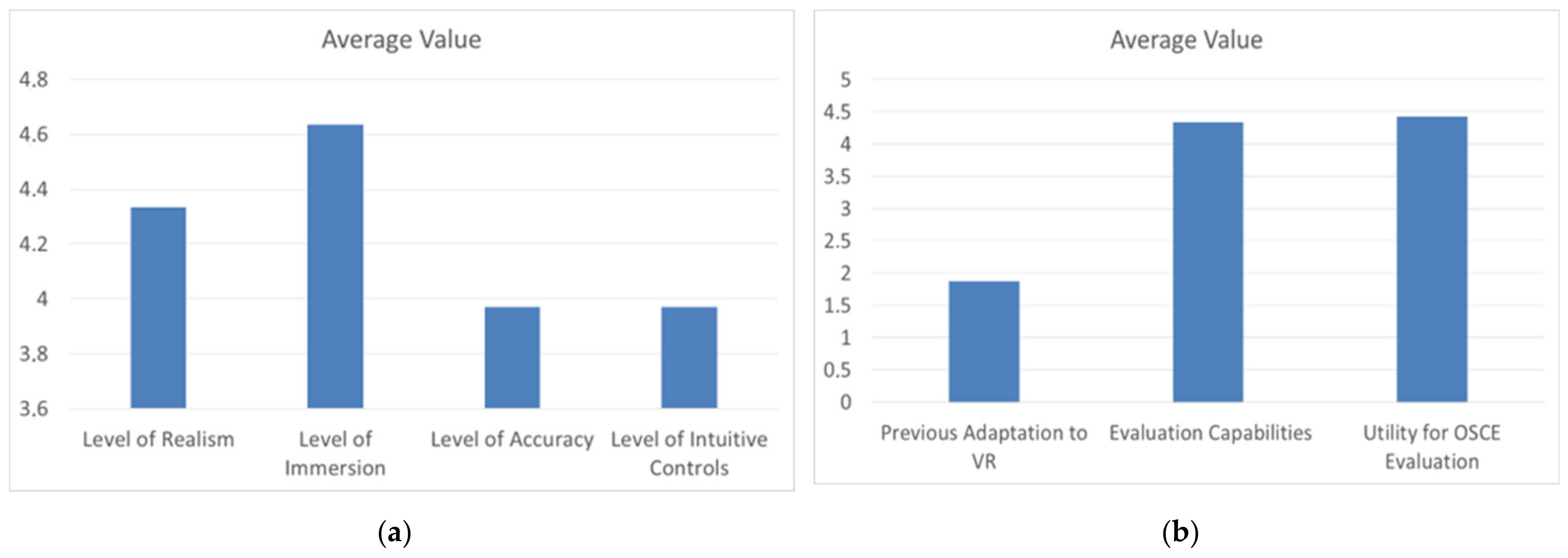
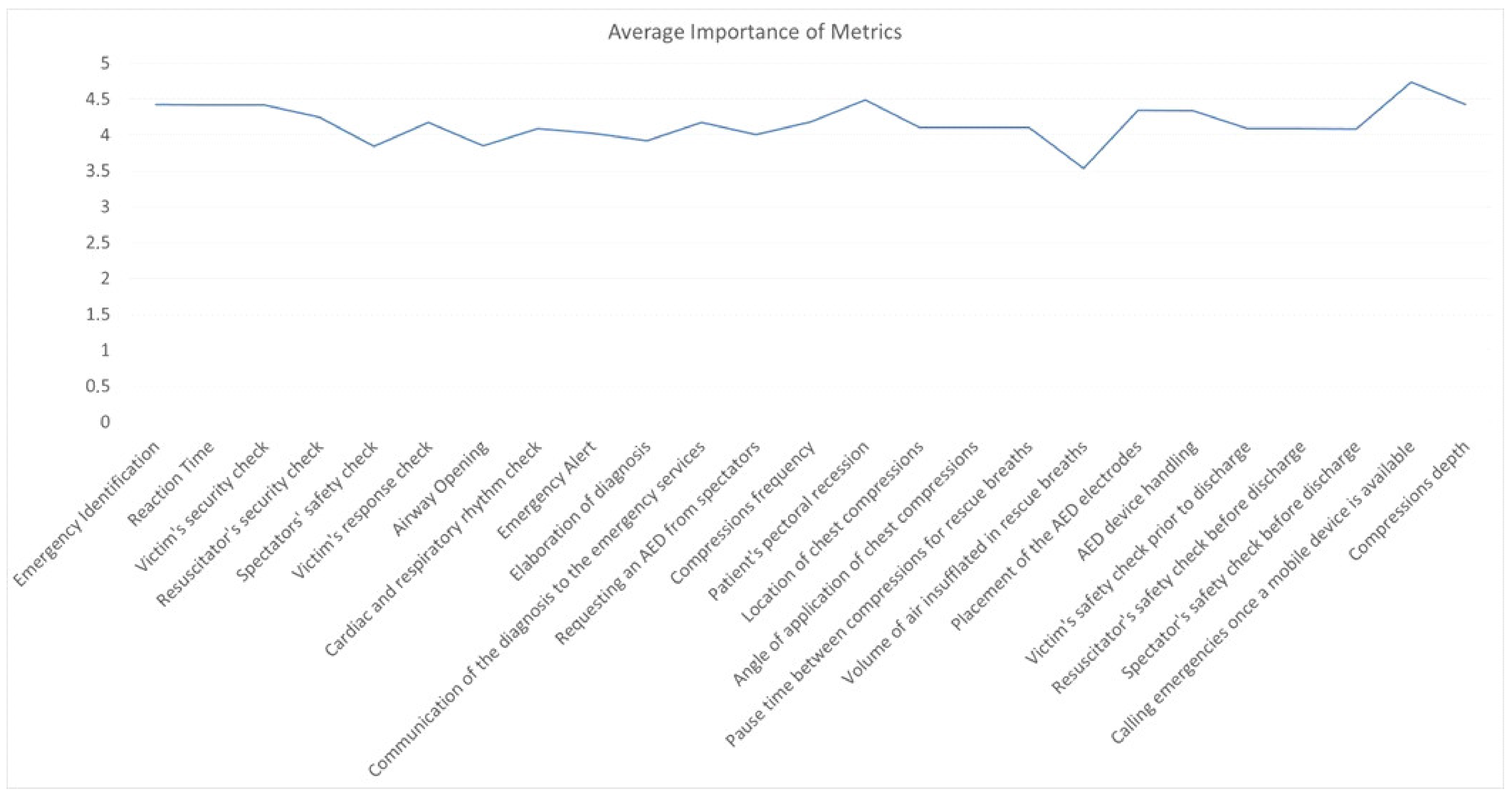
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zayyan, M. Objective Structured Clinical Examination: The Assessment of Choice. Oman Med. J. 2011, 26, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Harden, R.M.; Gleeson, F.A. Assessment of Clinical Competence Using an Objective Structured Clinical Examination (OSCE). Med. Educ. 1979, 13, 41–54. [Google Scholar] [CrossRef] [PubMed]
- López-Messa, J.B.; Martín-Hernández, H.; Pérez-Vela, J.L.; Molina-Latorre, R.; Herrero-Ansola, P. Novedades En Métodos Formativos En Resucitación. Med. Intensiva 2011, 35, 433–441. [Google Scholar] [CrossRef] [PubMed]
- American Heart Association. Frequently Asked Questions: AHA Requirement on Use of Feedback Devices in Adult CPR Training. Available online: http://ahainstructornetwork.americanheart.org (accessed on 24 May 2022).
- Gruenerbl, A.; Javaheri, H.; Monger, E.; Gobbi, M.; Lukowicz, P. Training CPR with a Wearable Real Time Feedback System. In Proceedings of the International Symposium on Wearable Computers (ISWC), Singapore, 8–12 October 2018; pp. 44–47. [Google Scholar]
- Lu, T.C.; Chen, Y.; Ho, T.W.; Chang, Y.T.; Lee, Y.T.; Wang, Y.S.; Chen, Y.P.; Fu, C.M.; Chiang, W.C.; Ma, M.H.M.; et al. A Novel Depth Estimation Algorithm of Chest Compression for Feedback of High-Quality Cardiopulmonary Resuscitation Based on a Smartwatch. J. Biomed. Inform. 2018, 87, 60–65. [Google Scholar] [CrossRef]
- Wanner, G.K.; Osborne, A.; Greene, C.H. Brief Compression-Only Cardiopulmonary Resuscitation Training Video and Simulation with Homemade Mannequin Improves CPR Skills. BMC Emerg. Med. 2016, 16, 45. [Google Scholar] [CrossRef] [Green Version]
- Ohle, R.; Moskalyk, M.; Boissonneault, E.; Bilgasem, A.; Tissot, E.; McIsaac, S. Is a Homemade Cardiopulmonary Resuscitation (CPR) Trainer Non-Inferior to a Commercially Available CPR Mannequin in Teaching High-Quality CPR? A Non-Inferiority Randomized Control Trial. Resusc. Plus 2021, 6, 100134. [Google Scholar] [CrossRef]
- Truszewski, Z.; Szarpak, L.; Kurowski, A.; Evrin, T.; Zasko, P.; Bogdanski, L.; Czyzewski, L. Randomized Trial of the Chest Compressions Effectiveness Comparing 3 Feedback CPR Devices and Standard Basic Life Support by Nurses. Am. J. Emerg. Med. 2016, 34, 381–385. [Google Scholar] [CrossRef]
- Perkins, G.D.; Handley, A.J.; Koster, R.W.; Castrén, M.; Smyth, M.A.; Olasveengen, T.; Monsieurs, K.G.; Raffay, V.; Gräsner, J.T.; Wenzel, V.; et al. European Resuscitation Council Guidelines for Resuscitation 2015. Section 2. Adult Basic Life Support and Automated External Defibrillation. Resuscitation 2015, 95, 81–99. [Google Scholar] [CrossRef] [Green Version]
- Neumar, R.W.; Shuster, M.; Callaway, C.W.; Gent, L.M.; Atkins, D.L.; Bhanji, F.; Brooks, S.C.; De Caen, A.R.; Donnino, M.W.; Ferrer, J.M.E.; et al. Part 1: Executive Summary: 2020 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S337–S357. [Google Scholar] [CrossRef]
- Plagisou, L.; Tsironi, M.; Zyga, S.; Moisoglou, I.; Maniadakis, N.; Prezerakos, P. Assessment of Nursing Staff’s Theoretical Knowledge of Cardiovascular Resuscitation in an NHS Public Hospital. Hell. J. Cardiol. 2015, 56, 149–153. [Google Scholar]
- Cook, D.A.; Brydges, R.; Zendejas, B.; Hamstra, S.J.; Hatala, R. Mastery Learning for Health Professionals Using Technology-Enhanced Simulation: A Systematic Review and Meta-Analysis. Acad. Med. 2013, 88, 1178–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semeraro, F.; Ristagno, G.; Giulini, G.; Gnudi, T.; Kayal, J.S.; Monesi, A.; Tucci, R.; Scapigliati, A. Virtual Reality Cardiopulmonary Resuscitation (CPR): Comparison with a Standard CPR Training Mannequin. Resuscitation 2019, 135, 234–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morie, J.F. Virtual Reality, Immersion, and the Unforgettable Experience. In Proceedings of the Stereoscopic Displays and Virtual Reality Systems XIII, San Jose, CA, USA, 16–19 January 2006; p. 60551X. [Google Scholar]
- Nolan, J.; Soar, J.; Eikeland, H. The Chain of Survival. Resuscitation 2006, 71, 270–271. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, M.E.; Brennan, E.E.; Goldberger, Z.D.; Swor, R.A.; Terry, M.; Bobrow, B.J.; Gazmuri, R.J.; Travers, A.H.; Rea, T. Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S414–S435. [Google Scholar] [CrossRef] [Green Version]
- ISAR, C. A Glance into Virtual Reality Development Using Unity. Inform. Econ. 2018, 22, 14–22. [Google Scholar] [CrossRef]
- Pensieri, C.; Pennacchini, M. Overview: Virtual Reality in Medicine. J. Virtual Worlds Res. 2014, 7, 353–401. [Google Scholar] [CrossRef] [Green Version]
- Semeraro, F.; Frisoli, A.; Bergamasco, M.; Cerchiari, E.L. Mini VREM Project (Mini Virtual Reality Enhanced Mannequin). Resuscitation 2010, 81, S106. [Google Scholar] [CrossRef]
- Loconsole, C.; Frisoli, A.; Semeraro, F.; Stroppa, F.; Mastronicola, N.; Filippeschi, A.; Marchetti, L. RELIVE: A Markerless Assistant for CPR Training. IEEE Trans. Hum.-Mach. Syst. 2016, 46, 755–760. [Google Scholar] [CrossRef]
- Wattanasoontorn, V.; Magdics, M.; Boada, I.; Sbert, M. A Kinect-Based System for Cardiopulmonary Resuscitation Simulation: A Pilot Study. In Serious Games Development and Applications. SGDA 2013. Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2013; Volume 8101, pp. 51–63. [Google Scholar] [CrossRef]
- Bench, S.; Winter, C.; Francis, G. Use of a Virtual Reality Device for Basic Life Support Training. Simul. Healthc. J. Soc. Simul. Healthc. 2019, 14, 287–292. [Google Scholar] [CrossRef]
- Varun Durai, S.I.; Arjunan, R.; Manivannan, M. Affordable Hi-Fidelity VR Based CPR Simulator with Haptics Feedback. In Proceedings of the HAVE 2017—IEEE International Symposium on Haptic, Audio-Visual Environments and Games, Abu Dhabi, United Arab Emirates, 22–23 October 2017; pp. 1–5. [Google Scholar]
- Cerezo, C.; Segura, F.; Melendreras, R.; García-Collado, Á.J.; Nieto, S.; Jiguera, L.; Pardo, S.; García, S.; Linares, E.; Pardo Ríos, M. La Realidad Virtual Como Método de Enseñanza de La Reanimación Cardiopulmonar: Un Estudio Aleatorizado. Emerg. Rev. Soc. Esp. Med. Urgenc. Emerg. 2019, 31, 43–46. [Google Scholar]
- Nas, J.; Thannhauser, J.; Vart, P.; Van Geuns, R.J.; Muijsers, H.E.C.; Mol, J.Q.; Aarts, G.W.A.; Konijnenberg, L.S.F.; Gommans, D.H.F.; Ahoud-Schoenmakers, S.G.A.M.; et al. Effect of Face-to-Face vs Virtual Reality Training on Cardiopulmonary Resuscitation Quality: A Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Everson, T.; Joordens, M.; Forbes, H.; Horan, B. Virtual Reality and Haptic Cardiopulmonary Resuscitation Training Approaches: A Review. IEEE Syst. J. 2022, 16, 1391–1399. [Google Scholar] [CrossRef]
- Almousa, O.; Prates, J.; Yeslam, N.; Gregor, D.M.; Zhang, J.; Phan, V.; Nielsen, M.; Smith, R.; Qayumi, K. Virtual Reality Simulation Technology for Cardiopulmonary Resuscitation Training: An Innovative Hybrid System With Haptic Feedback. Simul. Gaming 2019, 50, 6–22. [Google Scholar] [CrossRef]
- Leary, M.; McGovern, S.K.; Chaudhary, Z.; Patel, J.; Abella, B.S.; Blewer, A.L. Comparing Bystander Response to a Sudden Cardiac Arrest Using a Virtual Reality CPR Training Mobile App versus a Standard CPR Training Mobile App. Resuscitation 2019, 139, 167–173. [Google Scholar] [CrossRef]
- Blender. Available online: https://www.blender.org/about/ (accessed on 24 May 2022).
- Gatrell, M.; Counsell, S. Design Patterns and Fault-Proneness a Study of Commercial C# Software. In Proceedings of the 2011 Fifth International Conference on Research Challenges in Information Science, Gosier, France, 19–21 May 2011. [Google Scholar] [CrossRef]
- Unity-Scripting API. Object.DontDestroyOnLoad. Available online: https://docs.unity3d.com/ScriptReference/Object.DontDestroyOnLoad.html (accessed on 24 May 2022).
- Unity-Manual. AssetBundles. Available online: https://docs.unity3d.com/Manual/AssetBundlesIntro.html (accessed on 24 May 2022).
- Kwon, S.J.; Kim, S.H.; Kim, H.J.; Kim, J.S. LZ4m: A Fast Compression Algorithm for in-Memory Data. In Proceedings of the 2017 IEEE International Conference on Consumer Electronics (ICCE 2017), Las Vegas, NV, USA, 8–10 January 2017; pp. 420–423. [Google Scholar] [CrossRef]
- Unity-Manual. ScriptableObject. Available online: https://docs.unity3d.com/Manual/class-ScriptableObject.html (accessed on 24 May 2022).
- Three Types of Visibility Culling Techniques: 1) View-Frustum Culling|Download Scientific Diagram. Available online: https://www.researchgate.net/figure/Three-types-of-visibility-culling-techniques-1-View-Frustum-Culling-2-back-face_fig1_2440562 (accessed on 24 May 2022).
- Saredakis, D.; Szpak, A.; Birckhead, B.; Keage, H.A.D.; Rizzo, A.; Loetscher, T. Factors Associated With Virtual Reality Sickness in Head-Mounted Displays: A Systematic Review and Meta-Analysis. Front. Hum. Neurosci. 2020, 14, 96. [Google Scholar] [CrossRef] [Green Version]
- AMD FidelityFX-Super Resolution 2.0-GPUOpen. Available online: https://gpuopen.com/fidelityfx-superresolution-2/ (accessed on 24 May 2022).
- Peri, C.; Xiong, Y. Image Guided Depth Super-Resolution for Spacewarp in XR Applications. In Proceedings of the 2021 IEEE International Conference on Consumer Electronics (ICCE), Las Vegas, NV, USA, 10–12 January 2021. [Google Scholar] [CrossRef]
- Bearded Ninja Games Virtual Reality Interaction Framework for Unity Engine 2021. Available online: http://beardedninjagames.com/vr-framework/ (accessed on 24 May 2022).
- Verschaar, M.; Lobo, D.; Otaduy, M.A. Soft Hand Simulation for Smooth and Robust Natural Interaction. In Proceedings of the 25th IEEE Conference on Virtual Reality and 3D User Interfaces (VR 2018–Proceedings), Tuebingen/Reutlingen, Germany, 18–22 March 2018; pp. 183–190. [Google Scholar]
- Zhang, H.; Ye, Y.; Shiratori, T.; Komura, T. ManipNet: Neural Manipulation Synthesis with a Hand-Object Spatial Representation. ACM Trans. Graph. 2021, 40, 1–14. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metrics | Units | Evaluated Skill |
|---|---|---|
| Emergency identification | Yes/No | Clinical judgement, diagnosis management |
| Reaction time | Time in seconds | Clinical judgement, diagnosis management |
| Checking patient, bystander and rescuer safety | Yes/No | Ethical, legal aspects and professionalism |
| Checking the patient’s response | Yes/No | Physical exploration |
| Opening of the breathing airway | Yes/No | Technical and procedural skills |
| Checking heart and breathing rates | Yes/No | Physical exploration |
| Diagnostic communication to emergency services | Yes/No | Communication skills |
| Calling to emergency services | Yes/No | Communication skills |
| Diagnosis elaboration | Right/Wrong | Anamnesis, triage |
| Request for an automated external defibrillator (AED) | Yes/No | Communication skills |
| Time to carry out the preliminary checks | Time in seconds | Technical and procedural skills |
| Frequency of CPR compressions | Number | Technical and procedural skills |
| Depth of CPR compressions | cm | Technical and procedural skills |
| Pectoral recoil of the patient | Complete/Incomplete | Technical and procedural skills |
| Location of CPR compressions | Right/Wrong | Technical and procedural skills |
| Angle of application of CPR compressions | Right/Wrong | Technical and procedural skills |
| Pause time between compressions for rescue breaths | Time in seconds | Technical and procedural skills |
| Volume of air insufflated in rescue breaths | Liters | Technical and procedural skills |
| Placement of the AED electrodes | Right/Wrong | Technical and procedural skills |
| Handling the AED device | Right/Wrong | Technical and procedural skills |
| Checking the patient’s, bystanders’ and rescuer’s safety prior to electroshock | Yes/No | Ethical, legal aspects and professionalism |
| Simulators | RELIVE | LISSA | CODE-BLUE | VR-UCAM | LIFE SAVER | VR-Hybrid | VR-CPR | CPR Mobile | CPR-VR | FPS CPR VR |
|---|---|---|---|---|---|---|---|---|---|---|
| Type of simulation | Mini-VREM | Mini-VREM | VR | VR | VR | VR | VR | VR | VR | VR |
| Immersive | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Emergency scenario | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Multiple scenarios | No | Yes | No | No | Yes | No | No | No | No | No |
| Mannequin usage | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | No |
| Learning Mode | No | Yes | Yes | No | Yes | Yes | No | No | Yes | Yes |
| Training Mode | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Evaluation Mode | No | No | No | No | No | Yes | No | Yes | No | No |
| Simultaneous users | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Feedback | I | I | I | I | I | I + E | I | E | I | I + E |
| Haptic Device | M | M | C | M | M | M | M | C | M + C | C |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Matesanz, M.; Guzmán-García, C.; Oropesa, I.; Rubio-Bolivar, J.; Quintana-Díaz, M.; Sánchez-González, P. A New Immersive Virtual Reality Station for Cardiopulmonary Resuscitation Objective Structured Clinical Exam Evaluation. Sensors 2022, 22, 4913. https://doi.org/10.3390/s22134913
Rodríguez-Matesanz M, Guzmán-García C, Oropesa I, Rubio-Bolivar J, Quintana-Díaz M, Sánchez-González P. A New Immersive Virtual Reality Station for Cardiopulmonary Resuscitation Objective Structured Clinical Exam Evaluation. Sensors. 2022; 22(13):4913. https://doi.org/10.3390/s22134913
Chicago/Turabian StyleRodríguez-Matesanz, Manuel, Carmen Guzmán-García, Ignacio Oropesa, Javier Rubio-Bolivar, Manuel Quintana-Díaz, and Patricia Sánchez-González. 2022. "A New Immersive Virtual Reality Station for Cardiopulmonary Resuscitation Objective Structured Clinical Exam Evaluation" Sensors 22, no. 13: 4913. https://doi.org/10.3390/s22134913