
Accuracy Assessment of Percutaneous Pedicle Screw Placement Using Cone Beam Computed Tomography with Metal Artifact Reduction

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Surgical Procedure
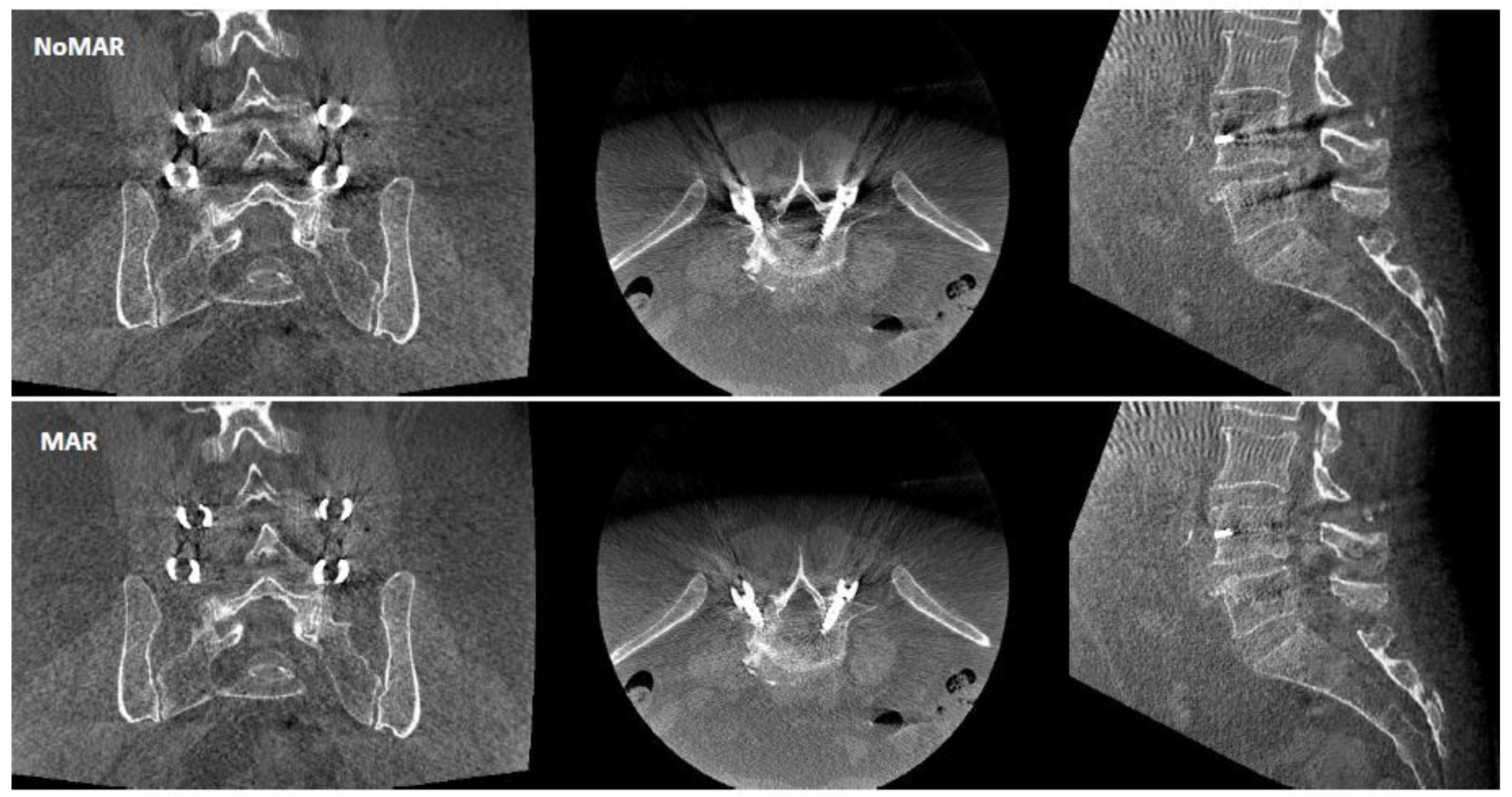
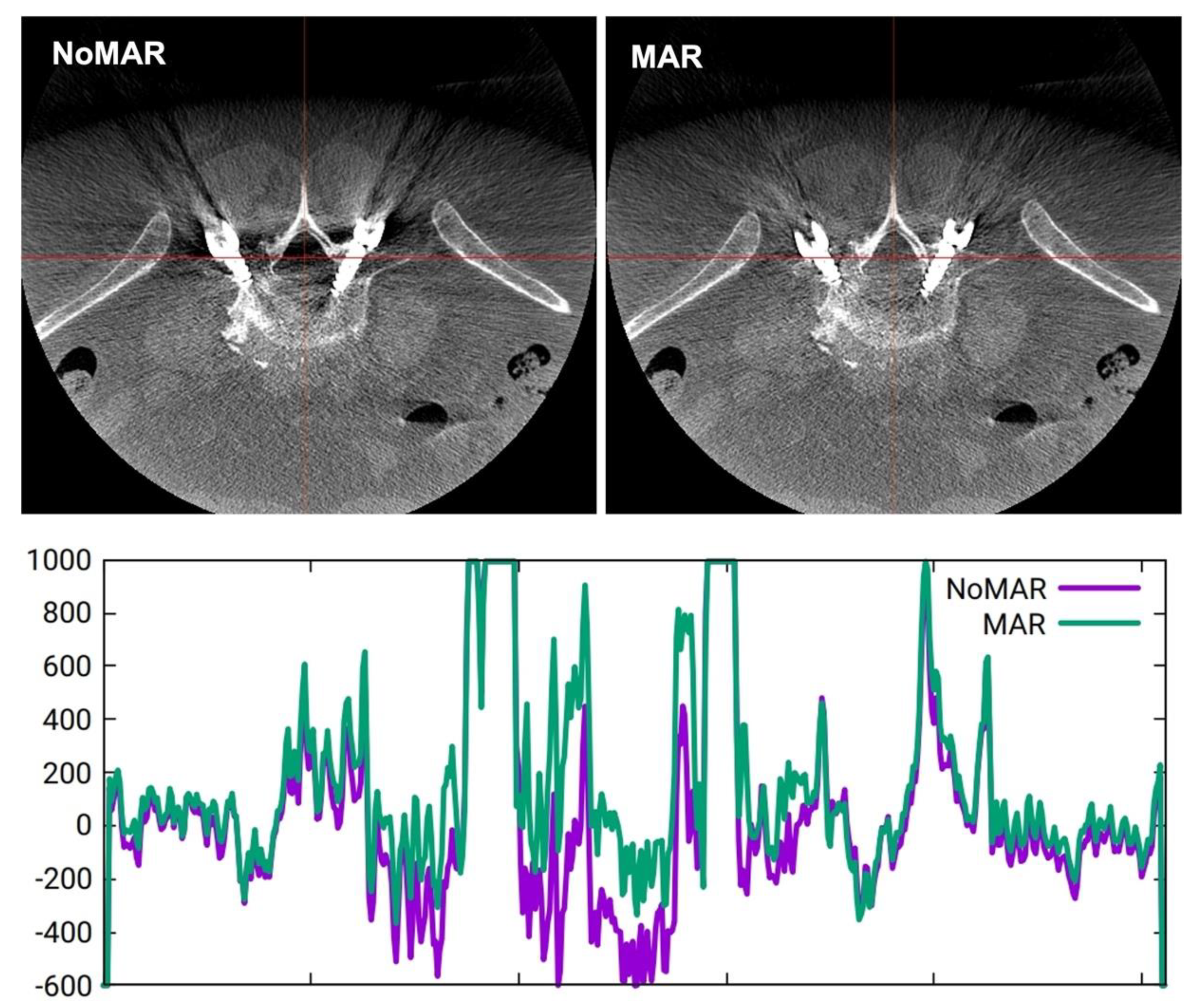
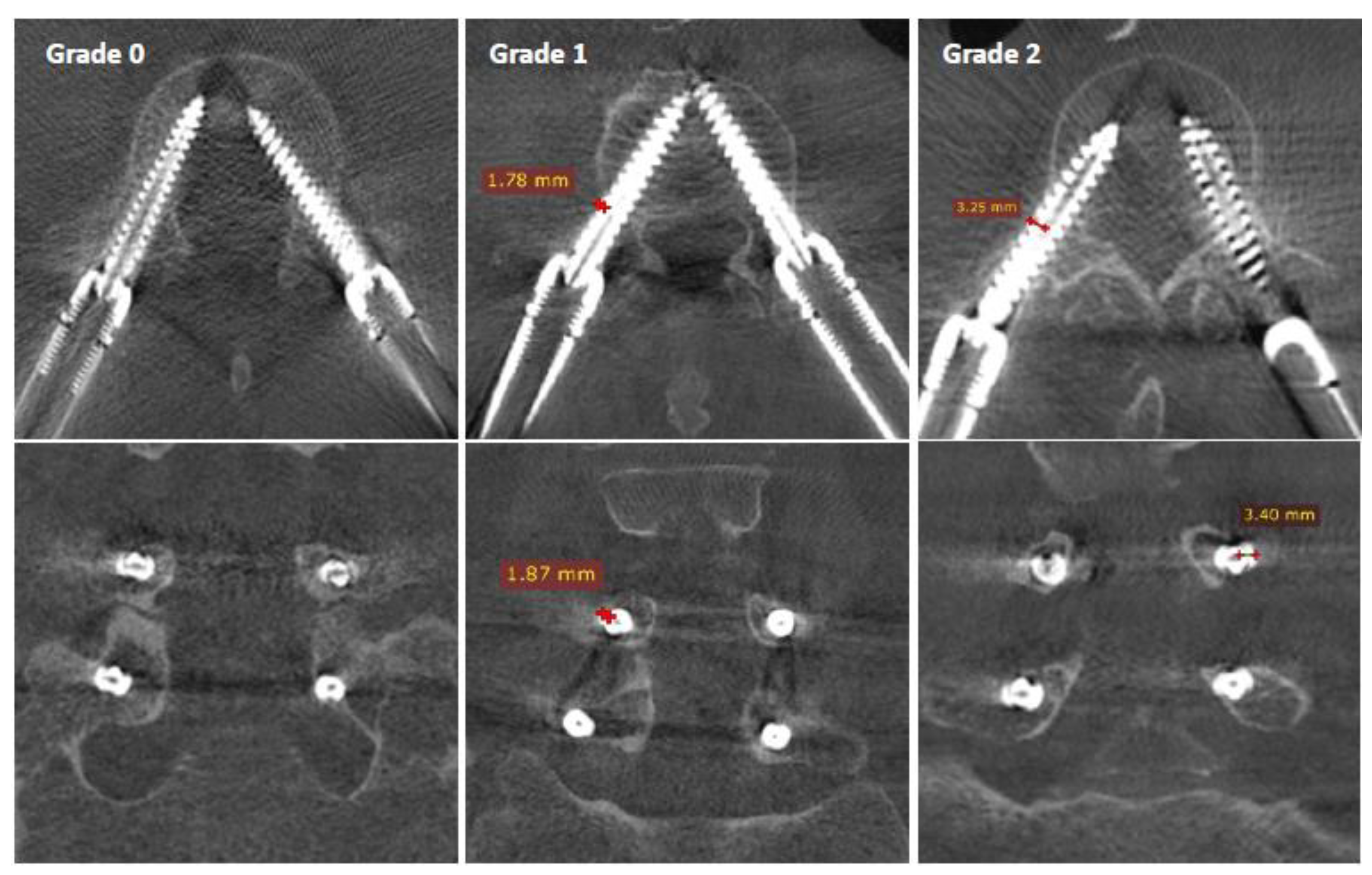
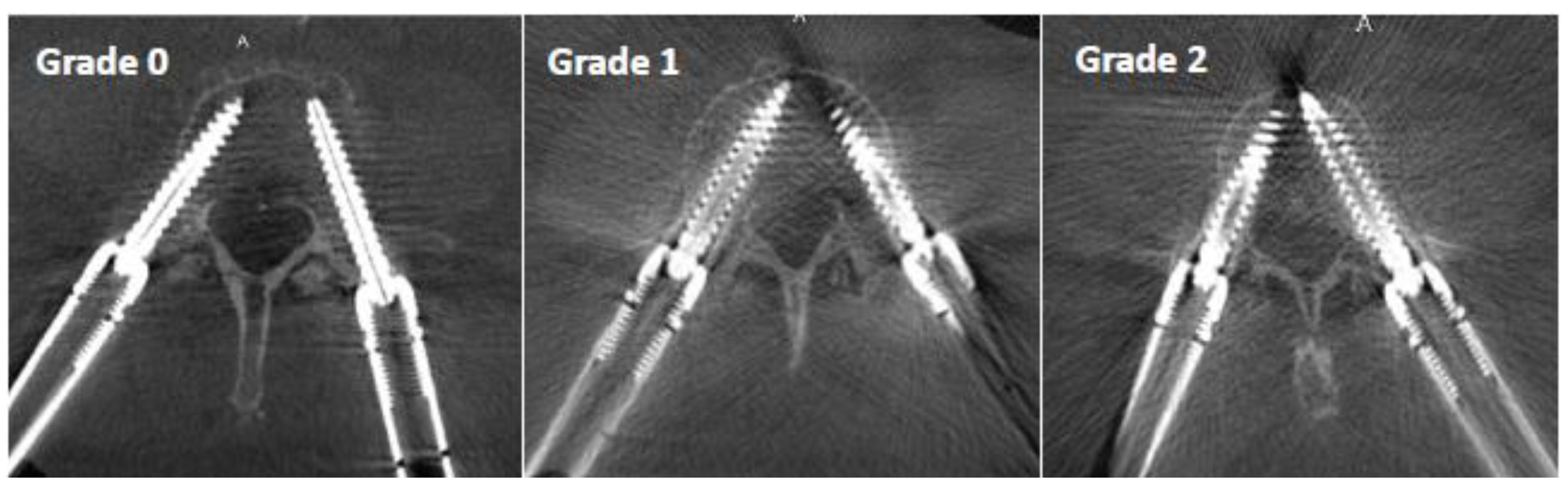
2.3. Image Analysis
- Grade 0: screw within the pedicle without cortical breach;
- Grade 1: 0–2 mm breach, minor perforation, including cortical encroachment;
- Grade 2: 2–4 mm breach, moderate breach;
- Grade 3: >4 mm breach, severe displacement, which was not found in this cohort.
- Grade 0: mild artifact, screw thread clearly visible, cortical bone clearly visible, bone soft tissue interface clearly visible, clear interpretation possible;
- Grade 1: moderate artifact, screw thread visible, cortical bone with unclear portions, bone soft tissue interface distinguishable, interpretation possible;
- Grade 2: strong artifact, screw thread unclear, cortical bone contours unclear, bone soft tissue not distinguishable, interpretation difficult.
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Gertzbein and Robins Classification
3.3. Image Quality Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldstein, C.L.; Macwan, K.; Sundararajan, K.; Rampersaud, Y.R. Comparative outcomes of minimally invasive surgery for posterior lumbar fusion: A systematic review. Clin. Orthop. Relat. Res. 2014, 472, 1727–1737. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, C.L.; Phillips, F.M.; Rampersaud, Y.R. Comparative Effectiveness and Economic Evaluations of Open Versus Minimally Invasive Posterior or Transforaminal Lumbar Interbody Fusion: A Systematic Review. Spine 2016, 41 (Suppl. 8), S74–S89. [Google Scholar] [CrossRef] [PubMed]
- Hohenhaus, M.; Watzlawick, R.; Masalha, W.; Volz, F.; Scholz, C.; Hubbe, U.; Klingler, J.H. Cranial facet joint injuries in percutaneous lumbar pedicle screw placement: A matched-pair analysis comparing intraoperative 3D navigation and conventional fluoroscopy. Eur. Spine J. 2021, 30, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Chen, W.; Liu, H.; Yang, H.; Liu, T. Does Pedicle Screw Fixation Assisted by O-Arm Navigation Perform Better Than Fluoroscopy-guided Technique in Thoracolumbar Fractures in Percutaneous Surgery? A Retrospective Cohort Study. Clin. Spine Surg. 2020, 33, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Elmi-Terander, A.; Nachabe, R.; Skulason, H.; Pedersen, K.; Söderman, M.; Racadio, J.; Babic, D.; Gerdhem, P.; Edström, E. Feasibility and Accuracy of Thoracolumbar Minimally Invasive Pedicle Screw Placement with Augmented Reality Navigation Technology. Spine 2018, 43, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Peh, S.; Chatterjea, A.; Pfarr, J.; Schäfer, J.P.; Weuster, M.; Klüter, T.; Seekamp, A.; Lippross, S. Accuracy of augmented reality surgical navigation for minimally invasive pedicle screw insertion in the thoracic and lumbar spine with a new tracking device. Spine J. 2020, 20, 629–637. [Google Scholar] [CrossRef]
- Charles, Y.P.; Cazzato, R.L.; Nachabe, R.; Chatterjea, A.; Steib, J.P.; Gangi, A. Minimally Invasive Transforaminal Lumbar Interbody Fusion Using Augmented Reality Surgical Navigation for Percutaneous Pedicle Screw Placement. Clin. Spine Surg. 2021, 34, E415–E424. [Google Scholar] [CrossRef]
- Edström, E.; Burström, G.; Omar, A.; Nachabe, R.; Söderman, M.; Persson, O.; Gerdhem, P.; Elmi-Terander, A. Augmented Reality Surgical Navigation in Spine Surgery to Minimize Staff Radiation Exposure. Spine 2020, 45, E45–E53. [Google Scholar] [CrossRef]
- Klingler, J.H.; Sircar, R.; Scheiwe, C.; Kogias, E.; Volz, F.; Krüger, M.T.; Hubbe, U. Comparative Study of C-arms for Intraoperative 3-dimensional Imaging and Navigation in Minimally Invasive Spine Surgery Part I: Applicability and Image Quality. Clin. Spine Surg. 2017, 30, 276–284. [Google Scholar] [CrossRef]
- Meyer, E.; Raupach, R.; Lell, M.; Schmidt, B.; Kachelriess, M. Normalized metal artifact reduction (NMAR) in computed tomography. Med. Phys. 2010, 37, 5482–5493. [Google Scholar] [CrossRef]
- Huber, F.A.; Sprengel, K.; Müller, L.; Graf, L.C.; Osterhoff, G.; Guggenberger, R. Comparison of different CT metal artifact reduction strategies for standard titanium and carbon-fiber reinforced polymer implants in sheep cadavers. BMC Med. Imaging 2021, 21, 29. [Google Scholar] [CrossRef] [PubMed]
- Privalov, M.; Mohr, M.; Swartman, B.; Beisemann, N.; Keil, H.; Franke, J.; Grützner, P.A.; Vetter, S.Y. Evaluation of Software-Based Metal Artifact Reduction in Intraoperative 3D Imaging of the Spine Using a Mobile Cone Beam CT. J. Digit. Imaging 2020, 33, 1136–1143. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Uneri, A.; Webster Stayman, J.; Zygourakis, C.C.; Lo, S.L.; Theodore, N.; Siewerdsen, J.H. Known-component 3D image reconstruction for improved intraoperative imaging in spine surgery: A clinical pilot study. Med. Phys. 2019, 46, 3483–3495. [Google Scholar] [CrossRef] [PubMed]
- Uneri, A.; Zhang, X.; Yi, T.; Stayman, J.W.; Helm, P.A.; Osgood, G.M.; Theodore, N.; Siewerdsen, J.H. Known-component metal artifact reduction (KC-MAR) for cone-beam CT. Phys. Med. Biol. 2019, 64, 165021. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Sheth, N.; Sisniega, A.; Uneri, A.; Han, R.; Vijayan, R.; Vagdargi, P.; Kreher, B.; Kunze, H.; Kleinszig, G.; et al. C-arm orbits for metal artifact avoidance (MAA) in cone-beam CT. Phys. Med. Biol. 2020, 65, 165012. [Google Scholar] [CrossRef]
- Thies, M.; Zäch, J.N.; Gao, C.; Taylor, R.; Navab, N.; Maier, A.; Unberath, M. A learning-based method for online adjustment of C-arm Cone-beam CT source trajectories for artifact avoidance. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 1787–1796. [Google Scholar] [CrossRef]
- Gertzbein, S.D.; Robbins, S.E. Accuracy of pedicular screw placement in vivo. Spine 1990, 15, 11–14. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Wiesner, L.; Kothe, R.; Rüther, W. Anatomic evaluation of two different techniques for the percutaneous insertion of pedicle screws in the lumbar spine. Spine 1999, 24, 1599–1603. [Google Scholar] [CrossRef]
- Charles, Y.P.; Ntilikina, Y.; Collinet, A.; Schuller, S.; Garnon, J.; Godet, J.; Clavert, P. Accuracy and technical limits of percutaneous pedicle screw placement in the thoracolumbar spine. Surg. Radiol. Anat. 2021, 43, 843–853. [Google Scholar] [CrossRef]
- Bodon, G.; Degreif, J. Fluoroscopy-based percutaneous posterior screw placement in the lateral position using the tunnel view technique: Technical note. Eur. Spine J. 2022, 1–8, epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Scarone, P.; Vincenzo, G.; Distefano, D.; Del Grande, F.; Cianfoni, A.; Presilla, S.; Reinert, M. Use of the Airo mobile intraoperative CT system versus the O-arm for transpedicular screw fixation in the thoracic and lumbar spine: A retrospective cohort study of 263 patients. J. Neurosurg. Spine 2018, 29, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Hecht, N.; Kamphuis, M.; Czabanka, M.; Hamm, B.; König, S.; Woitzik, J.; Synowitz, M.; Vajkoczy, P. Accuracy and workflow of navigated spinal instrumentation with the mobile AIRO® CT scanner. Eur. Spine J. 2016, 25, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.J.; Slakey, J.B. CT provides precise size assessment of implanted titanium alloy pedicle screws. Clin. Orthop. Relat. Res. 2014, 472, 1605–1609. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NoMAR | MAR | |
|---|---|---|
| Intra-Observer Correlation | ICC [95% CI] | ICC [95% CI] |
| Observer 1—surgeon | 0.63 [0.45–0.77] | 0.67 [0.50–0.79] |
| Observer 2—surgeon | 0.84 [0.74–0.90] | 0.78 [0.65–0.86] |
| Observer 3—surgeon | 0.77 [0.63–0.86] | 0.58 [0.37–0.73] |
| Observer 4—radiologist | 0.90 [0.83–0.94] | 0.85 [0.75–0.91] |
| Observer 5—radiologist | 0.79 [0.67–0.87] | 0.82 [0.71–0.89] |
| Observer 6—radiologist | 0.85 [0.75–0.91] | 0.90 [0.84–0.94] |
| Inter-observer Correlation | ||
| Between 3 surgeons | 0.89 [0.83–0.93] | 0.91 [0.86–0.95] |
| Between 3 radiologists | 0.74 [0.59–0.84] | 0.61 [0.39–0.75] |
| Between all 6 observers | 0.88 [0.82–0.92] | 0.85 [0.78–0.90] |
| NoMAR | MAR | |
|---|---|---|
| Intra-observer Correlation | ICC [95% CI] | ICC [95% CI] |
| Observer 1—surgeon | 0.73 [0.58–0.83] | 0.58 [0.38–0.73] |
| Observer 2—surgeon | 0.79 [0.66–0.87] | 0.69 [0.53–0.81] |
| Observer 3—surgeon | 0.64 [0.38–0.85] | 0.53 [0.23–0.75] |
| Observer 4—radiologist | 0.95 [0.91–0.97] | 0.87 [0.79–0.92] |
| Observer 5—radiologist | 0.63 [0.43–0.76] | 0.69 [0.53–0.81] |
| Observer 6—radiologist | 0.51 [0.29–0.68] | 0.58 [0.34–0.69] |
| Inter-observer Correlation | ||
| Between 3 surgeons | 0.81 [0.70–0.88] | 0.70 [0.38–0.84] |
| Between 3 radiologists | 0.62 [0.35–0.78] | 0.54 [0.28–0.71] |
| Between all 6 observers | 0.72 [0.55–0.80] | 0.63 [0.48–0.79] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charles, Y.P.; Al Ansari, R.; Collinet, A.; De Marini, P.; Schwartz, J.; Nachabe, R.; Schäfer, D.; Brendel, B.; Gangi, A.; Cazzato, R.L. Accuracy Assessment of Percutaneous Pedicle Screw Placement Using Cone Beam Computed Tomography with Metal Artifact Reduction. Sensors 2022, 22, 4615. https://doi.org/10.3390/s22124615
Charles YP, Al Ansari R, Collinet A, De Marini P, Schwartz J, Nachabe R, Schäfer D, Brendel B, Gangi A, Cazzato RL. Accuracy Assessment of Percutaneous Pedicle Screw Placement Using Cone Beam Computed Tomography with Metal Artifact Reduction. Sensors. 2022; 22(12):4615. https://doi.org/10.3390/s22124615
Chicago/Turabian StyleCharles, Yann Philippe, Rawan Al Ansari, Arnaud Collinet, Pierre De Marini, Jean Schwartz, Rami Nachabe, Dirk Schäfer, Bernhard Brendel, Afshin Gangi, and Roberto Luigi Cazzato. 2022. "Accuracy Assessment of Percutaneous Pedicle Screw Placement Using Cone Beam Computed Tomography with Metal Artifact Reduction" Sensors 22, no. 12: 4615. https://doi.org/10.3390/s22124615