
Electromyographic Assessment of the Efficacy of Deep Dry Needling versus the Ischemic Compression Technique in Gastrocnemius of Medium-Distance Triathletes


 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Design
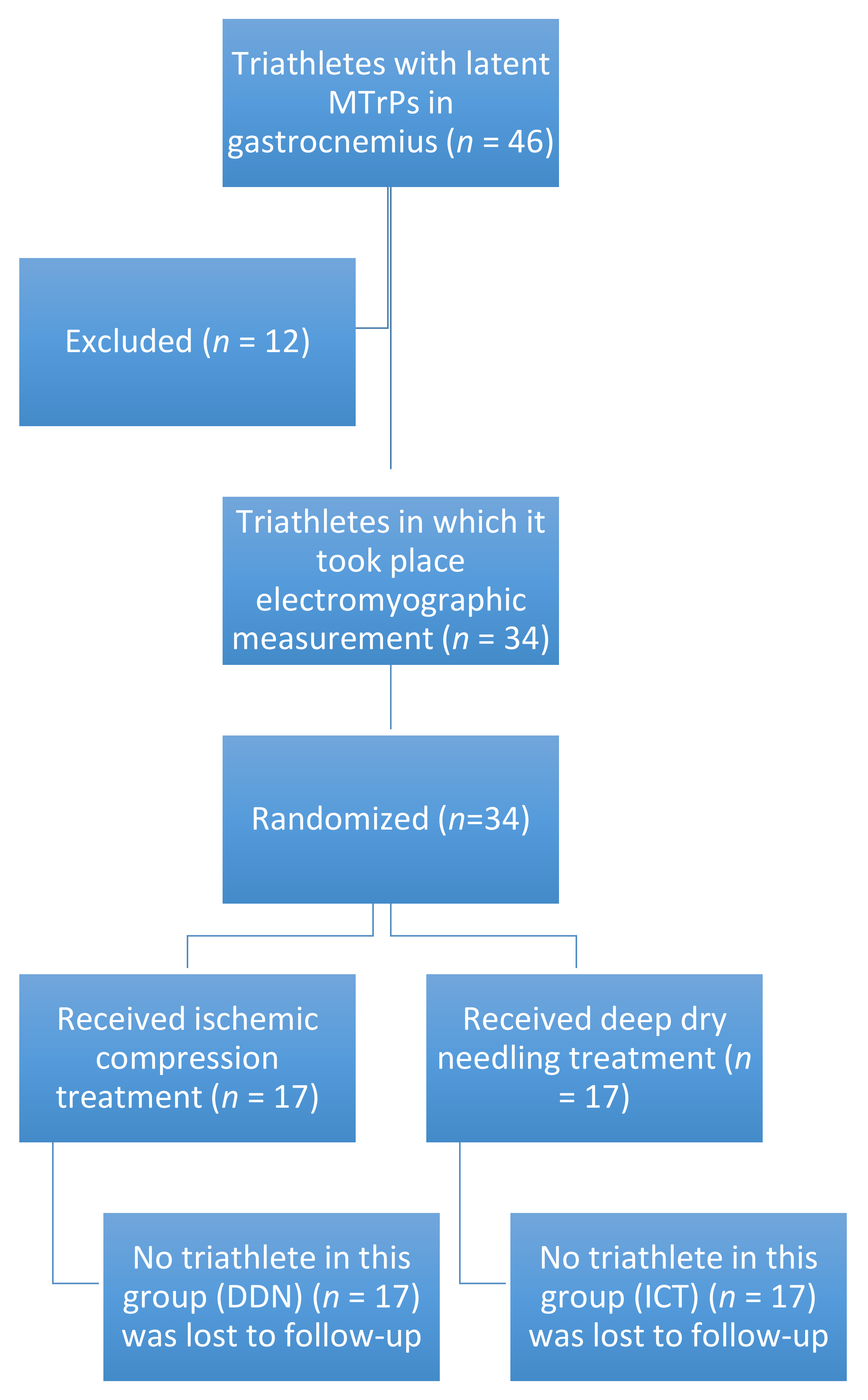
2.2. Participants
2.3. Simple Size Calculation
2.4. Principal Outcome: Electromyographic Measurement
2.5. Treatment Allocation
2.6. Experimental Group: DDN
2.7. Intervention Group: ICT
2.8. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristic by Treatment Groups.
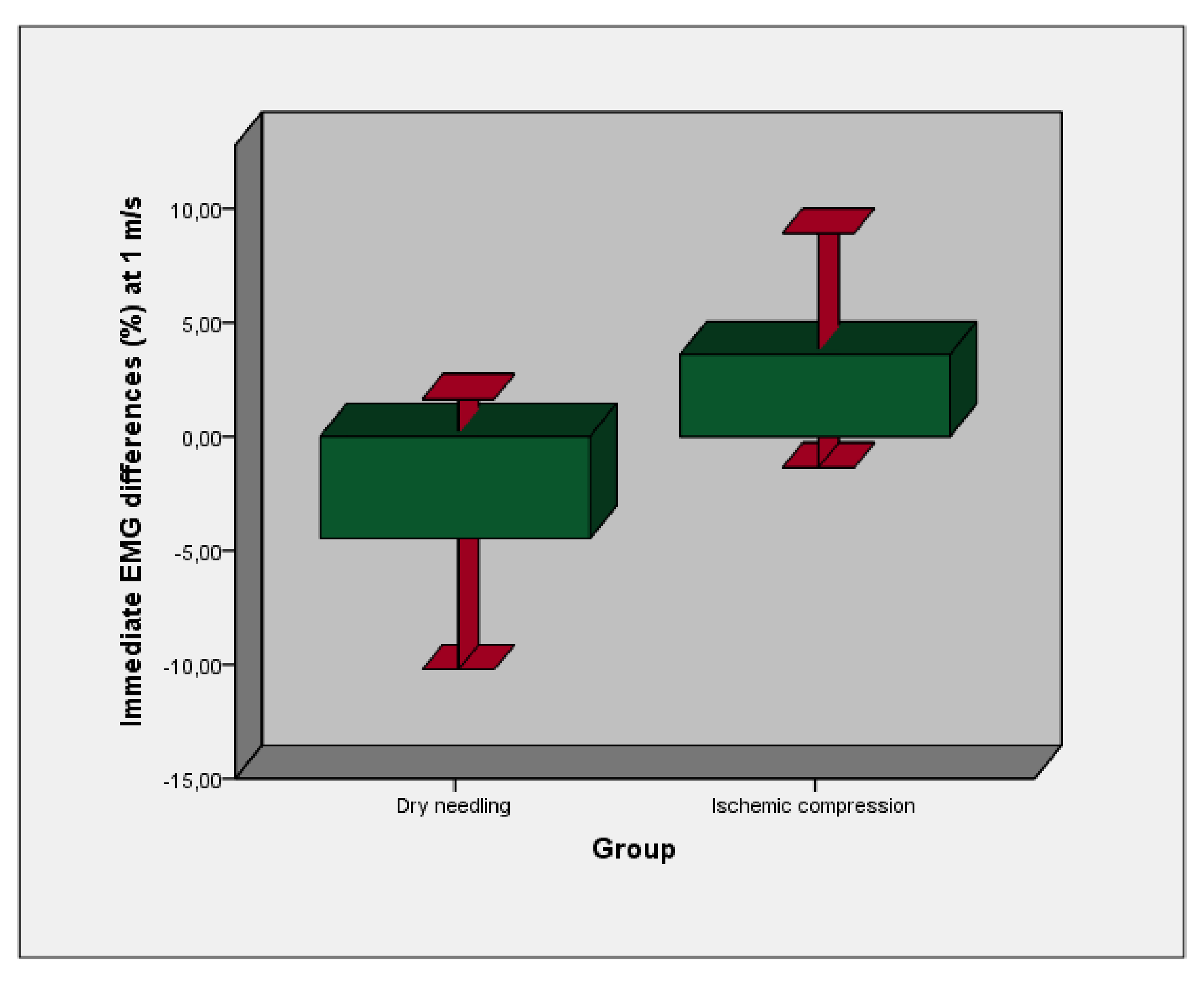
3.2. Electromyographic Measurement
3.3. Reliability Analysis
3.4. Multivariate Prediction Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdulmassih, S.; Phisitkul, P.; Femino, J.E.; Amendola, A. Triceps surae contracture: Implications for foot and ankle surgery. J. Am. Acad. Orthop. Surg. 2013, 21, 398–407. Available online: http://www.jaaos.org/cgi/doi/10.5435/JAAOS-21-07-398 (accessed on 16 April 2021). [CrossRef] [PubMed]
- Mokhtarzadeh, H.; Yeow, C.H.; Hong Goh, J.C.; Oetomo, D.; Malekipour, F.; Lee, P.V.-S. Contributions of the soleus and gastrocnemius muscles to the anterior cruciate ligament loading during single-leg landing. J. Biomech. 2013, 46, 1913–1920. [Google Scholar] [CrossRef] [PubMed]
- Kuitunen, S.; Kyröläinen, H.; Avela, J.; Komi, P.V. Leg stiffness modulation during exhaustive stretch-shortening cycle exercise. Scand. J. Med. Sci. Sports 2007, 17, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Getzin, A.R.; Milner, C.; Harkins, M. Fueling the Triathlete: Evidence-Based Practical Advice for Athletes of All Levels. Curr. Sports. Med. Rep. 2017, 16, 240–246. [Google Scholar] [CrossRef]
- Consejo Superior de Deportes. Licencias—Portal del Consejo Superior de Deportes. 2016. Available online: http://www.csd.gob.es/csd/asociaciones/1fedagclub/03Lic/ (accessed on 16 April 2021).
- Andersen, C.A.; Clarsen, B.; Johansen, T.V.; Engebretsen, L. High prevalence of overuse injury among iron-distance triathletes. Br. J. Sports Med. 2013, 47, 857–861. [Google Scholar] [CrossRef] [Green Version]
- Bertola, I.P.; Sartori, R.P.; Corrêa, D.G.; Zotz, T.G.G.; Gomes, A.R.S. Profile of injures prevalence in athletes who participated in SESC Triathlon Caiobá-2011. Acta Ortop. Bras. 2014, 22, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Bron, C.; Dommerholt, J.D. Etiology of myofascial trigger points. Curr. Pain Headache Rep. 2012, 16, 439–444. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22836591 (accessed on 16 April 2021). [CrossRef] [Green Version]
- Ge, H.-Y.; Fernández-de-Las-Peñas, C.; Yue, S.-W. Myofascial trigger points: Spontaneous electrical activity and its consequences for pain induction and propagation. Chin. Med. 2011, 6, 13. Available online: http://cmjournal.biomedcentral.com/articles/10.1186/1749-8546-6-13 (accessed on 16 April 2021). [CrossRef] [Green Version]
- Borg-Stein, J.; Simons, D.G. Focused review: Myofascial pain. Arch. Phys. Med. Rehabil. 2002, 83, S40–S47. Available online: http://www.ncbi.nlm.nih.gov/pubmed/11973695 (accessed on 16 April 2021). [CrossRef]
- Shah, J.P.; Thaker, N.; Heimur, J.; Aredo, J.V.; Sikdar, S.; Gerber, L. Myofascial Trigger Points Then and Now: A Historical and Scientific Perspective. PM&R 2015, 7, 746–761. [Google Scholar]
- Simons, D.G. Understanding effective treatments of myofascial trigger points. J. Bodyw. Mov. Ther. 2002, 6, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Travell, J.G.; Simons, D.G. Dolor y Disfunción Miofascial. el Manual de Los Puntos Gatillo; Mitad Inferior del Cuerpo: Baltimore, MD, USA, 2004. [Google Scholar]
- Zwingenberger, S.; Valladares, R.D.; Walther, A.; Beck, H.; Stiehler, M.; Kirschner, S.; Engelhardt, M.; Kasten, P. An epidemiological investigation of training and injury patterns in triathletes. J. Sports Sci. 2014, 32, 583–590. [Google Scholar] [CrossRef]
- Dommerholt, J. Dry needling—Peripheral and central considerations. J. Man. Manip. Ther. 2011, 19, 223–227. [Google Scholar] [CrossRef] [Green Version]
- Hong, C.Z. Lidocaine injection versus dry needling to myofascial trigger point. The importance of the local twitch response. Am. J. Phys. Med. Rehabil. 1994, 73, 256–263. [Google Scholar] [CrossRef]
- Kuan, T.-S.; Hsieh, Y.-L.; Chen, S.-M.; Chen, J.-T.; Yen, W.-C.; Hong, C.-Z. The myofascial trigger point region: Correlation between the degree of irritability and the prevalence of endplate noise. Am. J. Phys. Med. Rehabil. 2007, 86, 183–189. [Google Scholar] [CrossRef]
- Chou, L.-W.; Kao, M.-J.; Lin, J.-G. Probable mechanisms of needling therapies for myofascial pain control. Evid. Based Complement. Altern. Med. 2012, 2012, 705327. [Google Scholar] [CrossRef]
- Gattie, E.; Cleland, J.A.; Snodgrass, S. The effectiveness of trigger point dry needling for musculoskeletal conditions by physical therapists: A systematic review and meta-analysis. J. Orthop. Sports Phys. Ther. Mov. Sci. Media 2017, 47, 133–149. [Google Scholar] [CrossRef]
- Hains, G.; Descarreaux, M.; Hains, F. Chronic shoulder pain of myofascial origin: A randomized clinical trial using ischemic compression therapy. J. Manip. Physiol. Ther. 2010, 33, 362–369. [Google Scholar] [CrossRef]
- Apropos of a muscles. In Myofascial Pain and Dysfunction; Travell, J.G.; Simons, D.G. (Eds.) Williams & Wilkins: Baltimore, MD, USA, 2002. [Google Scholar]
- Cagnie, B.; Castelein, B.; Pollie, F.; Steelant, L.; Verhoeyen, H.; Cools, A. Evidence for the Use of Ischemic Compression and Dry Needling in the Management of Trigger Points of the Upper Trapezius in Patients with Neck Pain: A Systematic Review. Am. J. Phys. Med. Rehabil. 2015, 94, 573–583. [Google Scholar] [CrossRef]
- Miota Ibarra, J.; You Ge, H.; Wang, W.; Martínez Vizcaíno, V.; Graven.Nielsen, T.; Arendt-Nielsen, L. Latent myofascial trigger points are associated with an increased antagonistic muscle activity during agonist muscle contraction. J. Pain 2011, 12, 1282–1288. [Google Scholar] [CrossRef]
- Ge, H.-Y.; Monterde, S.; Graven-Nielsen, T.; Arendt-Nielsen, L. Latent Myofascial Trigger Points Are Associated with an Increased Intramuscular Electromyographic Activity During Synergistic Muscle Activation. J. Pain 2014, 15, 181–187. [Google Scholar] [CrossRef]
- Ge, H.-Y.; Arendt-Nielsen, L.; Madeleine, P. Accelerated muscle fatigability of latent myofascial trigger points in humans. Pain Med. 2012, 13, 957–964. [Google Scholar] [CrossRef] [Green Version]
- Ge, H.-Y.; Arendt-Nielsen, L. Latent Myofascial Trigger Points. Curr. Pain Headache Rep. 2011, 15, 386–392. [Google Scholar] [CrossRef]
- Gerwin, R.D.; Dommerholt, J.; Shah, J.P. An expansion of Simons’ integrated hypothesis of trigger point formation. Curr. Pain Headache Rep. 2004, 8, 468–475. [Google Scholar] [CrossRef]
- Simons, D.G.; Hong, C.-Z.; Simons, L.S. Endplate potentials are common to midfiber myofacial trigger points. Am. J. Phys. Med. Rehabil. 2002, 81, 212–222. [Google Scholar] [CrossRef]
- Abbaszadeh-Amirdehi, M.; Ansari, N.N.; Naghdi, S.; Olyaei, G.; Nourbakhsh, M.R. Therapeutic effects of dry needling in patients with upper trapezius myofascial trigger points. Acupunct. Med. 2017, 35, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Cagnie, B.; Dewitte, V.; Barbe, T.; Timmermans, F.; Delrue, N.; Meeus, M. Physiologic effects of dry needling. Curr. Pain Headache Rep. 2013, 17, 348. [Google Scholar] [CrossRef]
- Kalichman, L.; Vulfsons, S. Dry Needling in the Management of Musculoskeletal Pain. J. Am. Board Fam. Med. 2010, 23, 640–646. [Google Scholar] [CrossRef] [Green Version]
- Simons, D.G.; Travell, J.G.S.L. Travell and Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual Upper Half of Body, 2nd ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 1999. [Google Scholar]
- Kubo, K.; Yajima, H.; Takayama, M.; Ikebukuro, T.; Mizoguchi, H.; Takakura, N. Effects of acupuncture and heating on blood volume and oxygen saturation of human Achilles tendon in vivo. Eur. J. Appl. Physiol. 2010, 109, 545–550. [Google Scholar] [CrossRef]
- Ohkubo, M.; Hamaoka, T.; Niwayama, M.; Murase, N.; Osada, T.; Kime, R.; Kurosawa, Y.; Sakamoto, A.; Katsumura, T. Local increase in trapezius muscle oxygenation during and after acupuncture. Dyn. Med. 2009, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- Sato, A.; Sato, Y.; Shimura, M.; Uchida, S. Calcitonin gene-related peptide produces skeletal muscle vasodilation following antidromic stimulation of unmyelinated afferents in the dorsal root in rats. Neurosci. Lett. 2000, 283, 137–140. [Google Scholar] [CrossRef]
- Benito-de-Pedro, M.; Becerro-de-Bengoa-Vallejo, R.; Elena Losa-Iglesias, M.; Rodríguez-Sanz, D.; López-López, D.; Palomo-López, P.; Mazoteras-Pardo, V.; Calvo-Lobo, C. Effectiveness of Deep Dry Needling vs Ischemic Compression in the Latent Myofascial Trigger Points of the Shortened Triceps Surae from Triathletes on Ankle Dorsiflexion, Dynamic, and Static Plantar Pressure Distribution: A Clinical Trial. Pain Med. 2020, 21, e172–e181. [Google Scholar] [CrossRef] [PubMed]
- Travell, J.G.; Simons, D.G. Myofascial Pain and Dysfunction: The Trigger Point Manual; Williams & Wilkins: Baltimore, MD, USA, 1992. [Google Scholar]
- Myburgh, C.; Larsen, A.H.; Hartvigsen, J. A Systematic, Critical Review of Manual Palpation for Identifying Myofascial Trigger Points: Evidence and Clinical Significance. Arch. Phys. Med. Rehabil. 2008, 89, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Llamas-Ramos, R.; Pecos-Martín, D.; Gallego-Izquierdo, T.; Llamas-Ramos, I.; Plaza-Manzano, G.; Ortega-Santiago, R.; Joshua Cleland, J.; Fernández-de-las-Peñas, C. Comparison of the Short-Term Outcomes between Trigger Point Dry Needling and Trigger Point Manual Therapy for the Management of Chronic Mechanical Neck Pain: A Randomized Clinical Trial. J. Orthop. Sports Phys. Ther. 2014, 44, 852–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez de la Iglesia, J.; Dueñas Herrero, R.; Onís Vilches, M.C.; Aguado Taberné, C.; Albert Colomer, C.; Luque Luque, R. Spanish language adaptation and validation of the Pfeiffer’s questionnaire (SPMSQ) to detect cognitive deterioration in people over 65 years of age. Med. Clin. 2001, 117, 129–134. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- De Vito, G.; McHugh, D.; Macaluso, A.; Riches, P.E. Is the coactivation of biceps femoris during isometric knee extension affected by adiposity in healthy young humans? J. Electromyogr. Kinesiol. 2003, 13, 425–431. [Google Scholar] [CrossRef]
- Murley, G.S.; Bird, A.R. The effect of three levels of foot orthotic wedging on the surface electromyographic activity of selected lower limb muscles during gait. Clin. Biomech. 2006, 21, 1074–1080. [Google Scholar] [CrossRef]
- Cram, J.R.; Kasman, E.S.; Holtz, J. Introduction to Surface Electromyography; Aspen Publishers: New York, NY, USA, 1998. [Google Scholar]
- Pfeifer, K.; Banzer, W. Motor performance in different dynamic tests in knee rehabilitation. Scand. J. Med. Sci. Sports. 1999, 9, 19–27. [Google Scholar] [CrossRef]
- Fernández-Carner, J.; Ge, H.-Y.; Kimura, Y.; Fernández-de-Las-Peñas, C.; Arendt-Nielsen, L. Increased spontaneous electrical activity at a latent myofascial trigger point after nociceptive stimulation of another latent trigger point. Clin. J. Pain 2010, 26, 138–143. [Google Scholar] [CrossRef]
- Huang, S.; Ferris, D.P. Muscle activation patterns during walking from transtibial amputees recorded within the residual limb-prosthetic interface. J. Neuroeng. Rehabil. 2012, 9, 55. [Google Scholar] [CrossRef] [Green Version]
- Hermens, H.J.; Merletti, R.; Rix, H.F.B. The State of the Art on Signal Processing Methods for Surface Elektromyographie; SENIAM-deliverable 7; Roessingh Research and Development b.v.: Enschede, The Netherlands, 1999. [Google Scholar]
- Mayoral, O. Dry needling treatments for myofascial trigger points. J. Musculoskelet. Pain 2010, 18, 411–416. [Google Scholar] [CrossRef]
- Baldry, P. Superficial versus deep dry needling. Acupunct. Med. 2002, 20, 78–81. [Google Scholar] [CrossRef]
- Aguilera, F.J.M.; Martín, D.P.; Masanet, R.A.; Botella, A.C.; Soler, L.B.; Morell, F.B. Immediate effect of ultrasound and ischemic compression techniques for the treatment of trapezius latent myofascial trigger points in healthy subjects: A randomized controlled study. J. Manip. Physiol. Ther. 2009, 32, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Cagnie, B.; Dewitte, V.; Coppieters, I.; Van Oosterwijck, J.; Cools, A.; Danneels, L. Effect of Ischemic Compression on Trigger Points in the Neck and Shoulder Muscles in Office Workers: A Cohort Study. J. Manip. Physiol. Ther. 2013, 36, 482–489. [Google Scholar] [CrossRef]
- Benito-de-Pedro, M.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodríguez-Sanz, D.; López-López, D.; Cosín-Matamoros, J.; Martínez-Jiménez, E.M.; Calvo-Lobo, C. Effectiveness between Dry Needling and Ischemic Compression in the Triceps Surae Latent Myofascial Trigger Points of Triathletes on Pressure Pain Threshold and Thermography: A Single Blinded Randomized Clinical Trial. J. Clin. Med. 2019, 8, 1632. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.-C.; Lai, C.-H.; Chang, W.-H.; Tu, L.-W.; Lin, J.-C.; Chou, S.-W. Immediate effects of ischemic compression on neck function in patients with cervicogenic cephalic syndrome. J. Manip. Physiol. Ther. 2012, 35, 301–307. [Google Scholar] [CrossRef]
- Halle, J.S.; Halle, R.J. Pertinent dry needling considerations for minimizing adverse effects—Part two. Int. J. Sports Phys. Ther. 2016, 11, 810. [Google Scholar]
- Steentjes, K.; de Vries, L.M.A.; Ridwan, B.U.; Wijgman, A.J.J. Infection of a hip prosthesis after dry needling. Ned. Tijdschr. Geneeskd. 2016, 160, A9364. [Google Scholar]
- Baraja-Vegas, L.; Martín-Rodríguez, S.; Piqueras-Sanchiz, F.; Faundez-Aguilera, J.; Bautista, I.J.; Barrios, C.; Garcia-Escudero, M.; Fernández-de-las-Peñas, C. Localization of Muscle Edema and Changes on Muscle Contractility After Dry Needling of Latent Trigger Points in the Gastrocnemius Muscle. Pain Med. 2019, 20, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Cummings, M.; Ross-Marrs, R.; Gerwin, R. Pneumothorax complication of deep dry needling demonstration. Acupunct. Med. 2014, 32, 517–519. [Google Scholar] [CrossRef] [PubMed]
- Callan, A.K.; Bauer, J.M.; Martus, J.E. Deep Spine Infection after Acupuncture in the Setting of Spinal Instrumentation. Spine Deform. 2016, 4, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Lee, H.; Jo, D.-J. An Acute Cervical Epidural Hematoma as a Complication of Dry Needling. Spine 2011, 36, E891–E893. [Google Scholar] [CrossRef]
- Trigger Point Dry Needling: An Evidence and Clinical-Based Approach, 2nd ed.; Fernández-de-las-Peñas, C. (Ed.) Churchill Livingstone,: London, UK, 2019. [Google Scholar]
- Grieve, R.; Barnett, S.; Coghill, N.; Cramp, F. Myofascial trigger point therapy for triceps surae dysfunction: A case series. Man Ther. 2013, 18, 519–525. [Google Scholar] [CrossRef]
- Grieve, R.; Barnett, S.; Coghill, N.; Cramp, F. The prevalence of latent myofascial trigger points and diagnostic criteria of the triceps surae and upper trapezius: A cross sectional study. Physiotherapy 2013, 99, 278–284. [Google Scholar] [CrossRef]
- Simons, D.G. Review of enigmatic MTrPs as a common cause of enigmatic musculoskeletal pain and dysfunction. J. Electromyogr. Kinesiol. 2004, 14, 95–107. [Google Scholar] [CrossRef]
- Jafari, M.; Bahrpeyma, F.; Togha, M. Effect of ischemic compression for cervicogenic headache and elastic behavior of active trigger point in the sternocleidomastoid muscle using ultrasound imaging. J. Bodyw. Mov. Ther. 2017, 21, 933–939. [Google Scholar] [CrossRef]
- Takamoto, K.; Sakai, S.; Hori, E.; Urakawa, S.; Umeno, K.; Ono, T.; Nishijo, H. Compression on trigger points in the leg muscle increases parasympathetic nervous activity based on heart rate variability. J. Physiol. Sci. 2009, 59, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Ishii, H.; Niioka, T.; Watanabe, H.; Izumi, H. Inhibitory effects of excess sympathetic activity on parasympathetic vasodilation in the rat masseter muscle. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 293, R729–R736. [Google Scholar] [CrossRef]
- Hsieh, Y.-L.; Yang, S.-A.; Yang, C.-C.; Chou, L.-W. Dry needling at myofascial trigger spots of rabbit skeletal muscles modulates the biochemicals associated with pain, inflammation, and hypoxia. Evid. Based Complement. Altern. Med. 2012, 2012, 342165. [Google Scholar] [CrossRef]
- Baraja-Vegas, L.; Martín-Rodríguez, S.; Piqueras-Sanchiz, F.; Martín-Ruiz, J.; Yeste Fabregat, M.; Florencio, L.L.; Fernández-de-las-Peñas, C. Electromyographic Activity Evolution of Local Twitch Responses During Dry Needling of Latent Trigger Points in the Gastrocnemius Muscle: A Cross-Sectional Study. Pain Med. 2019, 21, 1224–1229. [Google Scholar] [CrossRef]
- De Meulemeester, K.E.; Castelein, B.; Coppieters, I.; Barbe, T.; Cools, A.; Cagnie, B. Comparing Trigger Point Dry Needling and Manual Pressure Technique for the Management of Myofascial Neck/Shoulder Pain: A Randomized Clinical Trial. J. Manip. Physiol. Ther. 2017, 40, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Behrangrad, S.; Abbaszadeh-Amirdehi, M.; Kordi Yoosefinejad, A.; Mokhtar Esmaeilnejadganji, S. Comparison of dry needling and ischaemic compression techniques on pain and function in patients with patellofemoral pain syndrome: A randomised clinical trial. Acupunct Med. 2020, 38, 371–379. [Google Scholar] [CrossRef]
- Vernon, H.; Schneider, M. Chiropractic management of myofascial trigger points and myofascial pain syndrome: A systematic review of the literature. J. Manip. Physiol. Ther. 2009, 32, 14–24. [Google Scholar] [CrossRef]
- Hong, C.Z. Myofascial pain therapy. J. Musculoskelet. Pain 2004, 12, 37–43. [Google Scholar] [CrossRef]
- Hsieh, Y.-L.; Chou, L.-W.; Joe, Y.-S.; Hong, C.-Z. Spinal cord mechanism involving the remote effects of dry needling on the irritability of myofascial trigger spots in rabbit skeletal muscle. Arch. Phys. Med. Rehabil. 2011, 92, 1098–1105. [Google Scholar] [CrossRef]
- Shah, J.P.; Gilliams, E.A. Uncovering the biochemical milieu of myofascial trigger points using in vivo microdialysis: An application of muscle pain concepts to myofascial pain syndrome. J. Bodyw. Mov. Ther. 2008, 12, 371–384. [Google Scholar] [CrossRef]
- Chen, J.T.; Chung, K.C.; Hou, C.R.; Kuan, T.S.; Chen, S.M.; Hong, C.Z. Inhibitory effect of dry needling on the spontaneous electrical activity recorded from myofascial trigger spots of rabbit skeletal muscle. Am. J. Phys. Med. Rehabil. 2001, 80, 729–735. [Google Scholar] [CrossRef] [Green Version]
- Abbaszadeh-Amirdehi, M.; Ansari, N.N.; Naghdi, S.; Olyaei, G.; Nourbakhsh, M.R. The neurophysiological effects of dry needling in patients with upper trapezius myofascial trigger points: Study protocol of a controlled clinical trial. BMJ Open. 2013, 3, e002825. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Experimental Group (DDN) (n = 17) | Control Group (ICT) (n = 17) | p Value | |
|---|---|---|---|
| Age (years) | 35.29 ± 5.39 (32.73–37.85) | 33.76 ± 5.76 (31.02–36.50) | 0.215 |
| Weight (kg) | 65.17 ± 10.71(60.08–70.27) | 69.17 ± 10.66 (64.10–74.24) | 0.141 |
| Height (cm) | 170.35 ± 12.94 (164.19–176.50) | 174.94 ± 6.96 (171.62–178.25) | 0.103 |
| BMI (kg/m2) | 22.37 ± 1.92 (21.46–23.29) | 22.48 ± 2.35 (21.36–23.6) | 0.443 |
| Foot length (cm) | 41.55 ± 3.26 (40.00–43.11) | 41.35 ± 2.73 (40.05–42.65) | 0.421 |
| Before Treatment | After Treatment | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Experimental Group (DDN) | Intervention Group (ICT) | p Value | Experimental Group (DDN) | Intervention Group (ICT) | Mean Difference (95% CI) | p Value |
| EMG FPM (µV). V1 (%) | 33.75 ± 14.84 (26.69–40.81) | 26.79 ± 9.40 (22.32–31.26) | 0.056 ** | −4.46 ± 11.53 (−30.74–11.08) | 3.59 ± 10.00 (−9.29–30.33) | −8.05 (−15.60; −0.51) | 0.037 * (t = −2.176) |
| EMG FPM (µV). V2 (%) | 34.84 ± 14.43 (27.98–41.70) | 30.36 ± 11.34 (24.97–35.76) | 0.160 ** | −1.00 ± 9.63 (−16.56–19.67) | 4.45 ± 10.62 (−13.86–35.56) | −5.45 (−12.53; 1.63) | 0.127 * (t = −1.167) |
| EMG FPM (µV). V3 (%) | 38.69 ± 15.19 (31.46–45.91) | 34.68 ± 11.69 (29.12–40.24) | 0.197 ** | 2.13 ± 7.42 (−8.07–24.15) | 3.23 ± 11.46 (−22.83–31.29) | −1.10 (−7.85; 5.84) | 0.734 † (U = 155.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benito-de-Pedro, M.; Calvo-Lobo, C.; López-López, D.; Benito-de-Pedro, A.I.; Romero-Morales, C.; San-Antolín, M.; Vicente-Campos, D.; Rodríguez-Sanz, D. Electromyographic Assessment of the Efficacy of Deep Dry Needling versus the Ischemic Compression Technique in Gastrocnemius of Medium-Distance Triathletes. Sensors 2021, 21, 2906. https://doi.org/10.3390/s21092906
Benito-de-Pedro M, Calvo-Lobo C, López-López D, Benito-de-Pedro AI, Romero-Morales C, San-Antolín M, Vicente-Campos D, Rodríguez-Sanz D. Electromyographic Assessment of the Efficacy of Deep Dry Needling versus the Ischemic Compression Technique in Gastrocnemius of Medium-Distance Triathletes. Sensors. 2021; 21(9):2906. https://doi.org/10.3390/s21092906
Chicago/Turabian StyleBenito-de-Pedro, María, César Calvo-Lobo, Daniel López-López, Ana Isabel Benito-de-Pedro, Carlos Romero-Morales, Marta San-Antolín, Davinia Vicente-Campos, and David Rodríguez-Sanz. 2021. "Electromyographic Assessment of the Efficacy of Deep Dry Needling versus the Ischemic Compression Technique in Gastrocnemius of Medium-Distance Triathletes" Sensors 21, no. 9: 2906. https://doi.org/10.3390/s21092906