
Marker Placement Reliability and Objectivity for Biomechanical Cohort Study: Healthy Aging in Industrial Environment (HAIE—Program 4)


 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Experimental Set-Up
2.3. Protocol
3. Data Analysis
4. Statistical Analysis
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sànchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. Gerontologist 2016, 56, S243–S255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshipura, M.; Mock, C.; Gosselin, R.A. Global burden of musculoskeletal conditions. Glob. Orthop. Caring Musculoskelet. Cond. Inj. Austere Settings 2014, 9–11. [Google Scholar]
- Hetsroni, I.; Finestone, A.; Milgrom, C.; Ben Sira, D.; Nyska, M.; Radeva-Petrova, D.; Ayalon, M. A prospective biomechanical study of the association between foot pronation and the incidence of anterior knee pain among military recruits. J. Bone Jt. Surg.-Ser. B 2006, 88, 905–908. [Google Scholar] [CrossRef] [Green Version]
- Sancho, I.; Malliaras, P.; Barton, C.; Willy, R.W.; Morrissey, D. Biomechanical alterations in individuals with Achilles tendinopathy during running and hopping: A systematic review with meta-analysis. Gait Posture 2019, 73, 189–201. [Google Scholar] [CrossRef]
- Ceyssens, L.; Vanelderen, R.; Barton, C.; Malliaras, P.; Dingenen, B. Biomechanical Risk Factors Associated with Running-Related Injuries: A Systematic Review. Sport. Med. 2019, 49, 1095–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahl, J.S.; Nelson, M.J.; Taylor, M.; Solomon, L.B.; Arnold, J.B.; Thewlis, D. Biomechanical changes and recovery of gait function after total hip arthroplasty for osteoarthritis: A systematic review and meta-analysis. Osteoarthr. Cartil. 2018, 26, 847–863. [Google Scholar] [CrossRef] [Green Version]
- Buldt, A.K.; Murley, G.S.; Butterworth, P.; Levinger, P.; Menz, H.B.; Landorf, K.B. The relationship between foot posture and lower limb kinematics during walking: A systematic review. Gait Posture 2013, 38, 363–372. [Google Scholar] [CrossRef]
- Cheung, A.S.; Gray, H.; Schache, A.G.; Hoermann, R.; Lim Joon, D.; Zajac, J.D.; Pandy, M.G.; Grossmann, M. Androgen deprivation causes selective deficits in the biomechanical leg muscle function of men during walking: A prospective case–control study. J. Cachexia Sarcopenia Muscle 2017, 8, 102–112. [Google Scholar] [CrossRef]
- Schwartz, M.H.; Trost, J.P.; Wervey, R.A. Measurement and management of errors in quantitative gait data. Gait Posture 2004, 20, 196–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jandacka, D.; Uchytil, J.; Zahradnik, D.; Farana, R.; Vilimek, D.; Skypala, J.; Urbaczka, J.; Plesek, J.; Motyka, A.; Blaschova, D.; et al. Running and Physical Activity in an Air-Polluted Environment: The Biomechanical and Musculoskeletal Protocol for a Prospective Cohort Study 4HAIE (Healthy Aging in Industrial Environment—Program 4). Int. J. Environ. Res. Public Health 2020, 17, 9142. [Google Scholar] [CrossRef]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef]
- Gorton, G.E.; Hebert, D.A.; Gannotti, M.E. Assessment of the kinematic variability among 12 motion analysis laboratories. Gait Posture 2009, 29, 398–402. [Google Scholar] [CrossRef]
- Wilken, J.M.; Rodriguez, K.M.; Brawner, M.; Darter, B.J. Reliability and minimal detectible change values for gait kinematics and kinetics in healthy adults. Gait Posture 2012, 35, 301–307. [Google Scholar] [CrossRef]
- Hamill, J.; Selbie, W.; Kepple, T. Three-dimensional Kinematics. In Research Methods in Biomechanics; Robertson, D., Caldwell, G., Hamill, J., Kamen, G., Whittlesey, S., Eds.; Human Kinetics: Champaign, IL, USA, 2013; pp. 35–60. [Google Scholar]
- Robertson, D.G.E.; Caldwell, G.E.; Hamill, J.; Kamen, G.; Whittlesey, S.N. Research Methods in Biomechanics; Human Kinetics: Champaign, IL, USA, 2014; ISBN 9781492595809. [Google Scholar]
- Maynard, V.; Bakheit, A.M.O.; Oldham, J.; Freeman, J. Intra-rater and inter-rater reliability of gait measurements with CODA mpx30 motion analysis system. Gait Posture 2003, 17, 59–67. [Google Scholar] [CrossRef]
- McGinley, J.; Baker, R.; Wolfe, R. Quantification of kinematic measurement variability in gait analysis. Gait Posture 2006, 24, S55–S56. [Google Scholar] [CrossRef]
- Kadaba, M.; Ramakrishnan, H.; Wooten, M.; Gainey, J.; Gorton, G.; Cochran, G.V.B. Repeatability of kinematic, kinetic, and electromyographic data in normal adult gait. J. Orthop. Res. 1989, 7, 849–860. [Google Scholar] [CrossRef] [PubMed]
- Ferber, R.; McClay-Davis, I.; Williams, D.; Laughton, C. A comparison of within- and between-day reliability of discrete 3D lower extremity variables in runners. J. Orthop. Res. 1989, 20, 1139–1145. [Google Scholar] [CrossRef]
- Ford, K.; Myer, G.; Hewett, T. Reliability of landing 3D motion analysis: Implications for longitudinal analyses. Med. Sci. Sport. Exerc. 2007, 39, 2021–2028. [Google Scholar] [CrossRef]
- Besier, T.; Sturnicks, D.; Alderson, J.A.; Lloyd, D.G. Repeatability of gait data using a functional hip joint centre and a mean helical knee axis. J. Biomech. 2003, 36, 1159–1168. [Google Scholar] [CrossRef]
- Rast, F.M.; Graf, E.S.; Meichtry, A.; Kool, J.; Bauer, C.M. Between-day reliability of three-dimensional motion analysis of the trunk: A comparison of marker based protocols. J. Biomech. 2016, 49, 807–811. [Google Scholar] [CrossRef]
- Noehren, B.; Manal, K.; Davis, I. Improving between-day kinematic reliability using a marker placement device. J. Orthop. Res. 2010, 28, 1405–1410. [Google Scholar] [CrossRef]
- Kainz, H.; Hoang, H.; Stockton, C.; Boyd, R.N.; Lloyd, D.G.; Carty, C.P. Accuracy and reliability of marker based approaches to scale the pelvis, thigh and shank segments in musculoskeletal models. J. Appl. Biomech. 2017, in press. [Google Scholar] [CrossRef]
- Bishop, C.; Thewlis, D.; Uden, H.; Ogilvie, D.; Paul, G. A radiological method to determine the accuracy of motion capture marker placement on palpable anatomical landmarks through a shoe. Footwear Sci. 2011, 3, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Mcclay, I.; Manal, K. Three-dimensional kinetic analysis of running: Significance of secondary planes of motion. Med. Sci. Sport. Exerc. 1999, 31, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Benedetti, M.G.; Berti, L.; Bettinelli, D.; Nativo, R.; Giannini, S. Rear-foot, mid-foot and fore-foot motion during the stance phase of gait. Gait Posture 2007, 25, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Portinaro, N.; Leardini, A.; Panou, A.; Monzani, V.; Caravaggi, P. Modifying the Rizzoli foot model to improve the diagnosis of pes-planus: Application to kinematics of feet in teenagers. J. Foot Ankle Res. 2014, 7, 754. [Google Scholar] [CrossRef] [Green Version]
- Hanavan, E.P.J. A mathematical model of the human body. Aerosp. Med. Res. Lab. 1964, 1–149. [Google Scholar]
- C-motion Tutorial: IOR Gait Full-Body Model. Available online: https://www.c-motion.com/v3dwiki/index.php?title=Tutorial%3A_IOR_Gait_Full-Body_Model&fbclid=IwAR0fv2MbKy1KaYVL99ShLc061bZtKIt6W7zZnPnl5mGtfJ6WwGwG0ywwVRc (accessed on 10 December 2020).
- C-motion Tutorial: Building a Model. Available online: https://www.c-motion.com/v3dwiki/index.php?title=Tutorial:_Building_a_Model (accessed on 10 December 2020).
- C-motion Tutorial: IOR Foot Model. Available online: https://www.c-motion.com/v3dwiki/index.php?title=Tutorial:_IOR_Foot_Model (accessed on 10 December 2020).
- Weir, J.P. Quantifying Test-Retest Reliability Using the Intraclass Correlation Coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231. [Google Scholar] [CrossRef] [PubMed]
- Richard, L. Computing Intraclass Correlations (ICC) as Estimates of Interrater Reliability in SPSS. Winnower 2015, 8, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Prentice Hall: Upper Saddle River, NJ, USA, 2000. [Google Scholar]
- Pourahmadi, M.R.; Takamjani, I.E.; Jaberzadeh, S.; Sarrafzadeh, J.; Sanjari, M.A.; Bagheri, R.; Taghipour, M. Kinematics of the spine during sit-to-stand movement using motion analysis systems: A systematic review of literature. J. Sport Rehabil. 2019, 28, 77–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lempereur, M.; Brochard, S.; Leboeuf, F.; Rémy-Néris, O. Validity and reliability of 3D marker based scapular motion analysis: A systematic review. J. Biomech. 2014, 47, 2219–2230. [Google Scholar] [CrossRef] [PubMed]
- Topley, M.; Richards, J.G. A comparison of currently available optoelectronic motion capture systems. J. Biomech. 2020, 106, 109820. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.G. The measurement of human motion: A comparison of commercially available systems. Hum. Mov. Sci. 1999, 18, 589–602. [Google Scholar] [CrossRef]
- Valevicius, A.M.; Jun, P.Y.; Hebert, J.S.; Vette, A.H. Use of optical motion capture for the analysis of normative upper body kinematics during functional upper limb tasks: A systematic review. J. Electromyogr. Kinesiol. 2018, 40, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Hamill, J.; van Emmerik, R.E.; Heiderscheit, B.C.; Li, L. A dynamical systems approach to lower extremity running injuries. Clin. Biomech. 1999, 14, 297–308. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
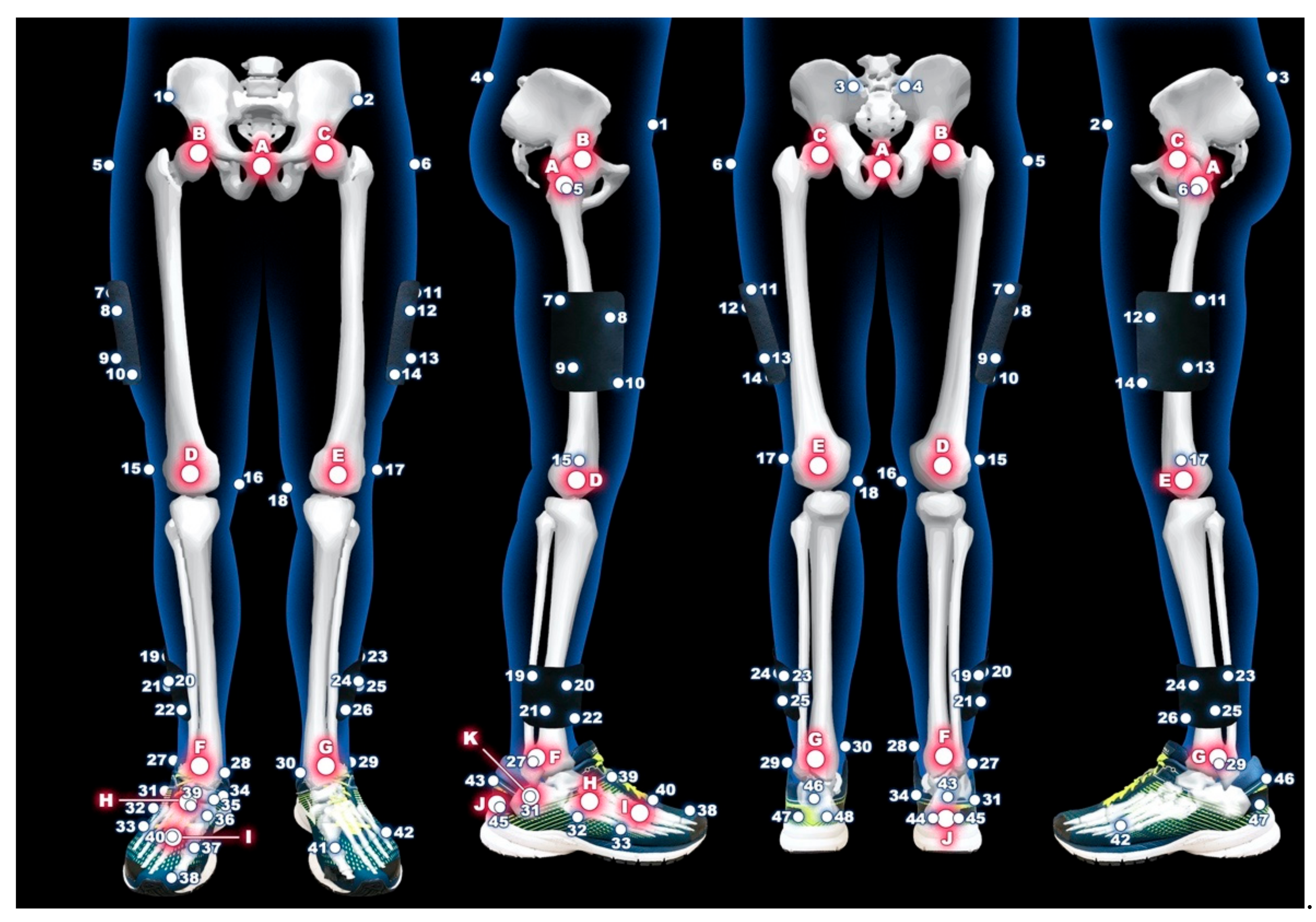
| Number | Anatomical Location | Number | Anatomical Location |
| 1 | right anterior superior iliac spine | 29 | left lateral malleoli of ankle |
| 2 | left anterior superior iliac spine | 30 | left medial malleoli of ankle |
| 3 | left posterior superior iliac spine | 31 | right lateral apex of the peroneal tubercle |
| 4 | right posterior superior iliac spine | 32 | right base of the fifth metatarsal |
| 5 | right great trochanter of the femur | 33 | right head of the fifth metatarsal |
| 6 | left great trochanter of the femur | 34 | right most medial apex of the sustentaculum tali |
| 7–10 | right marker cluster plate on the thigh | 35 | right most medial apex of the tuberosity of the navicular |
| 11–14 | left marker cluster plate on the thigh | 36 | right base of the first metatarsal |
| 15 | right lateral femoral condyle of knee | 37 | right head of the first metatarsal |
| 16 | right medial femoral condyle of knee | 38 | head of the proximal phalanx of the hallux |
| 17 | left lateral femoral condyle of knee | 39 | right base of the second metatarsal |
| 18 | left medial femoral condyle of knee | 40 | right head of the second metatarsal |
| 19–22 | right marker cluster plate on the shank | 41 | left head of the first metatarsal |
| 23–26 | left marker cluster plate on the shank | 42 | left head of the fifth metatarsal |
| 27 | right lateral malleoli of ankle | 43–45 | triad markers on the right heel |
| 28 | right medial malleoli of ankle | 46–48 | triad markers on the left heel |
| Letter | Landmark | Letter | Landmark |
| A | center between no.5 and no.6 | G | left ankle joint center |
| B | right hip joint center | H | center between no.32 and no.35 |
| C | left hip joint center | I | center between no.33 and no.37 |
| D | right knee joint center | J | center between no.44 and no.45 |
| E | left knee joint center | K | center between no.31 and no.34 |
| F | right ankle joint center |
| p-Values of the Shapiro-Wilk Test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PEL | RTH | LTH | RSK | LSK | RF | LF | RC | RMF | RM | |
| M1 | 0.277 | 0.820 | 0.122 | 0.009 | 0.302 | 0.446 | 0.335 | 0.107 | 0.582 | 0.274 |
| M2 | 0.095 | 0.485 | 0.074 | 0.013 | 0.034 | 0.691 | 0.305 | 0.619 | 0.039 | 0.054 |
| M3 | 0.027 | 0.079 | 0.101 | 0.031 | 0.025 | 0.527 | 0.606 | 0.873 | 0.675 | 0.459 |
| M4 | 0.093 | 0.259 | 0.126 | 0.085 | 0.028 | 0.286 | 0.681 | 0.813 | 0.044 | 0.525 |
| M5 | 0.025 | 0.109 | 0.320 | 0.032 | 0.009 | 0.347 | 0.512 | 0.356 | 0.607 | 0.271 |
| M6 | 0.080 | 0.380 | 0.308 | 0.001 | 0.004 | 0.928 | 0.359 | 0.108 | 0.891 | 0.832 |
| M7 | 0.010 | 0.288 | 0.098 | 0.011 | 0.132 | 0.244 | 0.446 | 0.654 | 0.666 | 0.568 |
| M8 | 0.067 | 0.222 | 0.125 | 0.005 | 0.051 | 0.613 | 0.202 | 0.097 | 0.128 | 0.420 |
| Segment | M1_ICC | M2_ICC | M3_ICC | M4_ICC | M5_ICC | M6_ICC | M7_ICC | M8_ICC | ICC_Mean |
|---|---|---|---|---|---|---|---|---|---|
| PEL | 0.972 | 0.968 | 0.994 | 0.982 | 0.986 | 0.985 | 0.988 | 0.956 | 0.979 |
| RTH | 0.931 | 0.959 | 0.983 | 0.856 | 0.991 | 0.972 | 0.815 | 0.983 | 0.936 |
| LTH | 0.620 | 0.954 | 0.975 | 0.958 | 0.974 | 0.967 | 0.890 | 0.978 | 0.915 |
| RSK | 0.982 | 0.995 | 0.985 | 0.971 | 0.986 | 0.989 | 0.989 | 0.992 | 0.986 |
| LSK | 0.979 | 0.977 | 0.986 | 0.977 | 0.986 | 0.975 | 0.992 | 0.984 | 0.982 |
| RF | 0.957 | 0.982 | 0.988 | 0.986 | 0.995 | 0.980 | 0.995 | 0.982 | 0.983 |
| LF | 0.982 | 0.980 | 0.981 | 0.985 | 0.993 | 0.986 | 0.984 | 0.987 | 0.985 |
| RC | 0.851 | 0.882 | 0.897 | 0.322 | 0.914 | 0.855 | 0.936 | 0.771 | 0.804 |
| RM | 0.402 | 0.818 | 0.541 | 0.848 | 0.318 | 0.924 | 0.839 | 0.770 | 0.683 |
| RMF | 0.913 | 0.884 | 0.931 | 0.697 | 0.924 | 0.947 | 0.862 | 0.960 | 0.890 |
| Segment | X (cm) | SD (cm) | SEM (cm) | MDC (cm) | %SEM | %MDC |
|---|---|---|---|---|---|---|
| PEL | 13.52 | 1.39 | 0.19 | 0.54 | 1.43 | 3.95 |
| RTH | 43.21 | 2.53 | 0.54 | 1.50 | 1.25 | 3.46 |
| LTH | 43.11 | 2.55 | 0.65 | 1.79 | 1.49 | 4.12 |
| RSK | 40.93 | 2.76 | 0.31 | 0.87 | 0.77 | 2.13 |
| LSK | 40.74 | 2.77 | 0.36 | 1.01 | 0.90 | 2.48 |
| RF | 13.80 | 1.26 | 0.16 | 0.43 | 1.13 | 3.12 |
| LF | 13.94 | 1.26 | 0.15 | 0.43 | 1.10 | 3.05 |
| RC | 6.08 | 0.91 | 0.36 | 1.01 | 6.08 | 16.85 |
| RM | 5.78 | 0.71 | 0.36 | 1.00 | 6.26 | 17.35 |
| RMF | 5.91 | 0.59 | 0.18 | 0.51 | 3.14 | 8.69 |
| Segment | ICC1 | ICC2 | ICC3 | ICC | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| PEL | 0.990 | 0.990 | 0.990 | 0.995 | 0.984 | 0.999 |
| RTH | 0.943 | 0.965 | 0.988 | 0.981 | 0.938 | 0.998 |
| LTH | 0.979 | 0.968 | 0.989 | 0.990 | 0.968 | 0.999 |
| RSK | 0.994 | 0.991 | 0.991 | 0.996 | 0.987 | 1.000 |
| LSK | 0.993 | 0.991 | 0.988 | 0.995 | 0.985 | 0.999 |
| RF | 0.990 | 0.997 | 0.995 | 0.998 | 0.993 | 1.000 |
| LF | 0.993 | 0.992 | 0.994 | 0.997 | 0.989 | 1.000 |
| RC | 0.948 | 0.951 | 0.935 | 0.975 | 0.917 | 0.997 |
| RM | 0.805 | 0.798 | 0.694 | 0.860 | 0.541 | 0.984 |
| RMF | 0.942 | 0.937 | 0.943 | 0.971 | 0.903 | 0.997 |
| Segment | X (cm) | SD (cm) | SEM (cm) | MDC (cm) | %SEM | %MDC |
|---|---|---|---|---|---|---|
| PEL | 13.52 | 0.39 | 0.03 | 0.08 | 0.20 | 0.57 |
| RTH | 43.21 | 1.19 | 0.16 | 0.45 | 0.38 | 1.05 |
| LTH | 43.11 | 0.92 | 0.09 | 0.26 | 0.21 | 0.59 |
| RSK | 40.93 | 1.07 | 0.07 | 0.19 | 0.16 | 0.46 |
| LSK | 40.74 | 0.87 | 0.06 | 0.17 | 0.15 | 0.42 |
| RF | 13.80 | 0.23 | 0.01 | 0.03 | 0.08 | 0.21 |
| LF | 13.94 | 0.22 | 0.01 | 0.03 | 0.09 | 0.24 |
| RC | 6.08 | 0.64 | 0.10 | 0.28 | 1.67 | 4.62 |
| RM | 5.78 | 0.47 | 0.18 | 0.49 | 3.03 | 8.40 |
| RMF | 5.91 | 0.53 | 0.09 | 0.25 | 1.54 | 4.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malus, J.; Skypala, J.; Silvernail, J.F.; Uchytil, J.; Hamill, J.; Barot, T.; Jandacka, D. Marker Placement Reliability and Objectivity for Biomechanical Cohort Study: Healthy Aging in Industrial Environment (HAIE—Program 4). Sensors 2021, 21, 1830. https://doi.org/10.3390/s21051830
Malus J, Skypala J, Silvernail JF, Uchytil J, Hamill J, Barot T, Jandacka D. Marker Placement Reliability and Objectivity for Biomechanical Cohort Study: Healthy Aging in Industrial Environment (HAIE—Program 4). Sensors. 2021; 21(5):1830. https://doi.org/10.3390/s21051830
Chicago/Turabian StyleMalus, Jan, Jiri Skypala, Julia Freedman Silvernail, Jaroslav Uchytil, Joseph Hamill, Tomas Barot, and Daniel Jandacka. 2021. "Marker Placement Reliability and Objectivity for Biomechanical Cohort Study: Healthy Aging in Industrial Environment (HAIE—Program 4)" Sensors 21, no. 5: 1830. https://doi.org/10.3390/s21051830