
Elderly Perception on the Internet of Things-Based Integrated Smart-Home System


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Literature Review
2.1. Necessity of Smart Home System for the Elderly
2.2. Sensor Application in Smart Home System for the Elderly
2.3. Elderly Perception on Smart Home Systems
3. Method
3.1. Study Design
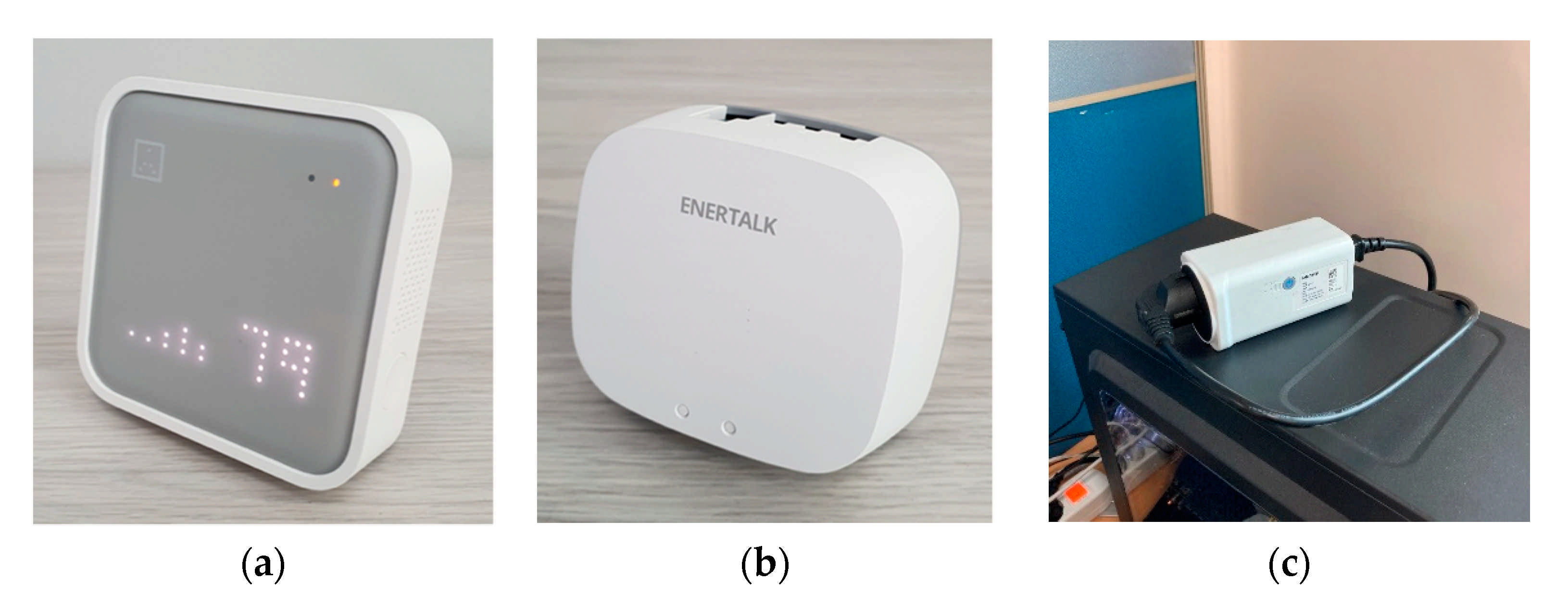
3.1.1. Sensor-Set Selection
- (1)
- In this study, we defined a smart home system that provides comprehensive benefits essential for improving the QoL of the elderly as an ISHS. Based on a literature review, essential benefits that are commonly considered as important benefits of smart home systems for the elderly are as follows: fall detection [7], healthcare monitoring [1,8], ADL recognition [48], iAQ monitoring, and energy consumption monitoring [10,11]. Thus, the sensor-set for the ISHS were to provide the essential benefits of a smart home system.
- (2)
- (3)
- By minimizing the applied sensors for our ISHS, the cost factor of our sensor-set application can be efficiently minimized; we assured the sensor-set selection provided the collection of the necessary data that can be analyzed to provide the aforementioned essential benefits for the elderly in an ISHS environment, despite minimizing the number of applied smart home sensors.
- (4)
- To minimize the privacy invasion of the ISHS user, the sensor-set selection excludes the application of sensors which can record real-time visualizations. For instance, indoor location information can be easily acquired through sensors integrated with cameras, however, due to the nature of privacy invasion using cameras, BLE beacons were chosen as our sensor for acquiring indoor location information.
3.1.2. Technological Trial
3.2. Focus Group Interview Design
3.2.1. Interview Design
3.2.2. Participants
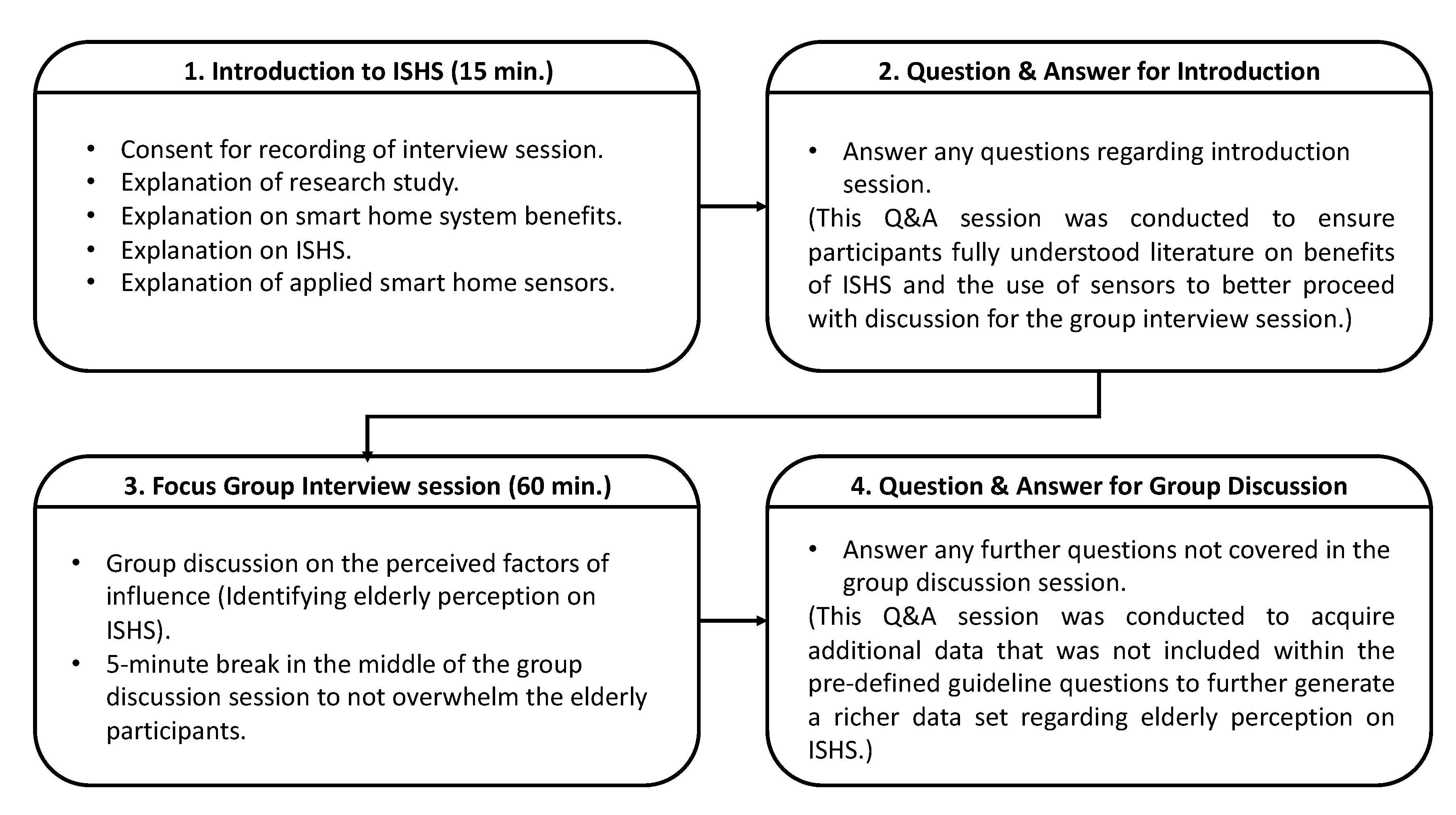
3.2.3. Focus Group Interview & Procedure
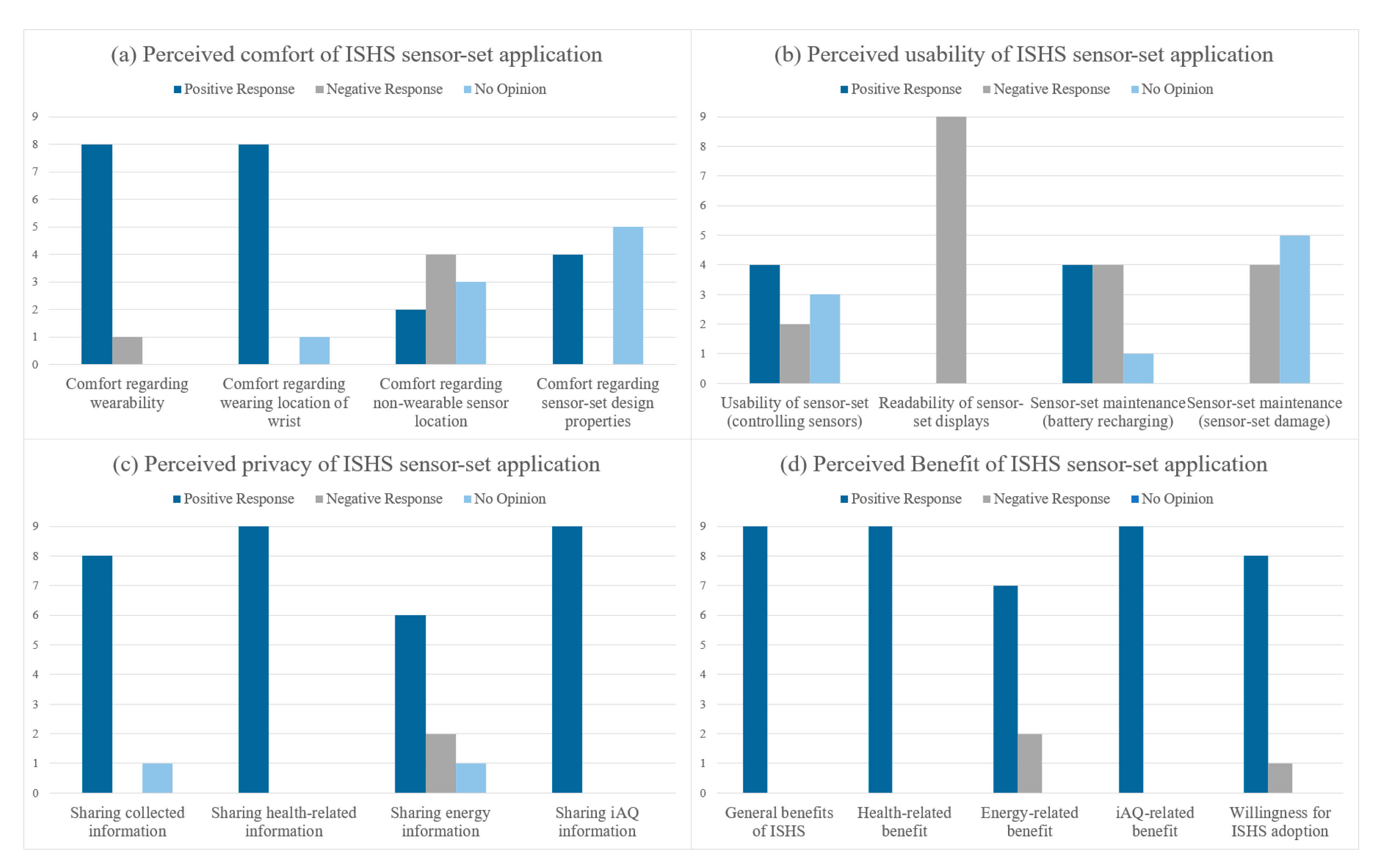
4. Results
5. Discussion
5.1. Perceived Comfort
5.2. Perceived Usability
5.3. Perceived Privacy
5.4. Perceived Benefits
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- How do you perceive the comfort in using the sensors?
- Did you experience any physical discomfort from wearing the wearable BLE beacon?
- Did the design properties of the sensors generate any discomfort? (cues: weight, size, color, and form).
- How would you perceive the comfort of wearable sensors at different wearing locations? (cues: head, neck, arm, waist, leg, and ankle)
- Did you experience any interruptions to your daily activities from using the sensors?
- Do you think changing the installation location of non-wearable sensors/wearing location of the wearable BLE beacon might solve the issues of interruption to daily activities?
- How do you perceive the usability of the sensors?
- Did you experience any difficulties interacting (control) with the sensors?
- Do you experience any difficulties with the readability of the sensors? (cues: display size, color, and font)
- Did you have any worries about damaging the sensors?
- Did you experience any difficulties with having to charge the batteries of the sensors?
- How would you prefer using replaceable battery cells instead of recharging via charging cable?
- Did you experience any issues with forgetting to put the sensor back on after taking it off?
- Do you have any suggestions for future implementations regarding the usability of sensors?
- How do you perceive the privacy of the ISHS?
- Do you have any privacy concerns regarding sharing information about your activity levels?
- What information collected from monitoring do you feel neglected to share? (cues: healthcare, iAQ, and energy information).
- To which entities do you feel neglected to share information with? (cues: family, friends, doctors, and caretakers)
- If the monitoring information was required to be a long-term collection, how would you feel about it?
- How do you perceive the benefit of the integrated smart home system?
- What monitoring information do you think would be most helpful to the elderly population?
- How might you like to receive the information? (cues: sensor display, professional feedback, immediate action, when necessary).
- What are the benefits of ISHS that you think is most helpful?
- Do you think living in an ISHS environment will help improve QoL for the independently aging elderly population?
- Would you be willing to adopt ISHS?
- Do you have any other suggestions for the future implications of ISHS?
References
- Majumder, S.; Aghayi, E.; Noferesti, M.; Memarzadeh-Tehran, H.; Mondal, T.; Pang, Z.; Deen, M.J. Smart homes for elderly healthcare—Recent advances and research challenges. Sensors 2017, 17, 2496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deen, M.J. Information and communications technologies for elderly ubiquitous healthcare in a smart home. Pers. Ubiquitous Comput. 2015, 19, 573–599. [Google Scholar] [CrossRef]
- Habjanič, A.; Saarnio, R.; Elo, S.; Turk, D.M.; Isola, A. Challenges for institutional elder care in Slovenian nursing homes. J. Clin. Nurs. 2012, 21, 2579–2589. [Google Scholar] [CrossRef] [PubMed]
- Canjuga, I.; Železnik, D.; Neuberg, M.; Božicevic, M.; Cikac, T. Does an impaired capacity for self-care impact the prevalence of social and emotional loneliness among elderly people? Work Older People 2018, 22, 211–223. [Google Scholar] [CrossRef]
- Jacobzone, S.; Cambois, E.; Robine, J.-M.C.N.-C. Is the health of older persons in OECD countries improving fast enough to compensate for population ageing? In Labour Market and Social Policy—Occasional Papers; OECD: Paris, France, 2000; pp. 1–35. [Google Scholar] [CrossRef]
- Wiles, J.L.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E.S. The meaning of “aging in place” to older people. Gerontologist 2012, 52, 357–366. [Google Scholar] [CrossRef]
- Lim, D.; Park, C.; Kim, N.H.; Kim, S.-H.; Yu, Y.S. Fall-Detection Algorithm Using 3-Axis Acceleration: Combination with Simple Threshold and Hidden Markov Model. J. Appl. Math. 2014, 2014, 1–8. [Google Scholar] [CrossRef]
- Pantelopoulos, A.; Bourbakis, N.G. A Survey on Wearable Sensor-Based Systems for Health Monitoring and Prognosis. IEEE Trans. Syst. Man Cybern. Part C Appl. Rev. 2010, 40, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Wei, W.; Ramalho, O.; Mandin, C. Indoor air quality requirements in green building certifications. Build. Environ. 2015, 92, 10–19. [Google Scholar] [CrossRef]
- Sanchez, V.G. A Review of Smart House Analysis Methods for Assisting Older People Living Alone. J. Sens. Actuator Netw. 2017, 6, 11. [Google Scholar] [CrossRef] [Green Version]
- Jaouhari, S.E.L.; Palacios-Garcia, E.J.; Anvari-Moghaddam, A.; Bouabdallah, A. Integrated management of energy, wellbeing and health in the next generation of smart homes. Sensors 2019, 19, 481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, W.; Cui, H.; Rao, H.; Li, Z.; Yao, L. Detection of Human Falls on Furniture Using Scene Analysis Based on Deep Learning and Activity Characteristics. IEEE Access 2018, 6, 9324–9335. [Google Scholar] [CrossRef]
- Sehairi, K.; Chouireb, F.; Meunier, J. Elderly fall detection system based on multiple shape features and motion analysis. In Proceedings of the 2018 IEEE International Conference on Intelligent Systems and Computer Vision (ISCV), Fez, Morocco, 2–4 April 2018; pp. 1–8. [Google Scholar] [CrossRef]
- Daher, M.; Diab, A.; El Badaoui El Najjar, M.; Ali Khalil, M.; Charpillet, F. Elder Tracking and Fall Detection System Using Smart Tiles. IEEE Sens. J. 2017, 17, 469–479. [Google Scholar] [CrossRef]
- Yacchirema, D.; De Puga, J.S.; Palau, C.; Esteve, M. Fall detection system for elderly people using IoT and ensemble machine learning algorithm. Procedia Comput. Sci. 2018, 130, 603–610. [Google Scholar] [CrossRef]
- Sucerquia, A.; López, J.D.; Vargas-Bonilla, J.F. Real-life/real-time elderly fall detection with a triaxial accelerometer. Sensors 2018, 18, 1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, A.M.; Selvaraj, N.; Ferdosi, N.; Narasimhan, R. Wireless patch sensor for remote monitoring of heart rate, respiration, activity, and falls. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 6115–6118. [Google Scholar] [CrossRef]
- Perego, P.; Standoli, C.; Andreoni, G. Wearable monitoring of elderly in an ecologic setting: The SMARTA project. In Proceedings of the 2nd International Electronic Conference on Sensors and Applications, MDPI, Basel, Switzerland, 5 November 2015; p. S3001. [Google Scholar] [CrossRef]
- Milici, S.; Amendola, S.; Bianco, A.; Marrocco, G. Epidermal RFID passive sensor for body temperature measurements. In Proceedings of the 2014 IEEE RFID Technology and Applications Conference (RFID-TA), Tampere, Finland, 8–9 September 2014; pp. 140–144. [Google Scholar] [CrossRef]
- Boano, C.A.; Lasagni, M.; Romer, K.; Lange, T. Accurate Temperature Measurements for Medical Research Using Body Sensor Networks. In Proceedings of the 2011 14th IEEE International Symposium on Object/Component/Service-Oriented Real-Time Distributed Computing Workshops, Newport Beach, CA, USA, 28 –31 March 2011; pp. 189–198. [Google Scholar] [CrossRef]
- Kim, J.; Kwon, S.; Seo, S.; Park, K. Highly wearable galvanic skin response sensor using flexible and conductive polymer foam. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 6631–6634. [Google Scholar] [CrossRef]
- Guo, R.; Li, S.; He, L.; Gao, W.; Qi, H.; Owens, G. Pervasive and Unobtrusive Emotion Sensing for Human Mental Health. In Proceedings of the Proceedings of the ICTs for improving Patients Rehabilitation Research Techniques, Venice, Italy, 5–8 May 2013; pp. 436–439. [Google Scholar]
- Basit, A.; Sidhu, G.A.S.; Mahmood, A.; Gao, F. Efficient and Autonomous Energy Management Techniques for the Future Smart Homes. IEEE Trans. Smart Grid 2017, 8, 917–926. [Google Scholar] [CrossRef]
- Ford, R.; Pritoni, M.; Sanguinetti, A.; Karlin, B. Categories and functionality of smart home technology for energy management. Build. Environ. 2017, 123, 543–554. [Google Scholar] [CrossRef] [Green Version]
- Filho, G.; Ueyama, J.; Villas, L.; Pinto, A.; Gonçalves, V.; Pessin, G.; Pazzi, R.; Braun, T. NodePM: A Remote Monitoring Alert System for Energy Consumption Using Probabilistic Techniques. Sensors 2014, 14, 848–867. [Google Scholar] [CrossRef]
- Schieweck, A.; Uhde, E.; Salthammer, T.; Salthammer, L.C.; Morawska, L.; Mazaheri, M.; Kumar, P. Smart homes and the control of indoor air quality. Renew. Sustain. Energy Rev. 2018, 94, 705–718. [Google Scholar] [CrossRef]
- Yu, T.-C.; Lin, C.-C. An Intelligent Wireless Sensing and Control System to Improve Indoor Air Quality: Monitoring, Prediction, and Preaction. Int. J. Distrib. Sens. Netw. 2015, 11, 140978. [Google Scholar] [CrossRef] [Green Version]
- Marikyan, D.; Papagiannidis, S.; Alamanos, E. A systematic review of the smart home literature: A user perspective. Technol. Forecast. Soc. Chang. 2019, 138, 139–154. [Google Scholar] [CrossRef]
- Courtney, K.L.; Demiris, G.; Rantz, M.; Skubic, M. Needing smart home technologies: The perspectives of older adults in continuing care retirement communities. Inform. Prim. Care 2008, 16, 195–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.K.; Choi, M. Older adults’ willingness to share their personal and health information when adopting healthcare technology and services. Int. J. Med. Inform. 2019, 126, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Wild, K.; Boise, L.; Lundell, J.; Foucek, A. Unobtrusive in-home monitoring of cognitive and physical health: Reactions and perceptions of older adults. J. Appl. Gerontol. 2008, 27, 181–200. [Google Scholar] [CrossRef] [PubMed]
- Reeder, B.; Chung, J.; Lyden, K.; Winters, J.; Jankowski, C.M. Older women’s perceptions of wearable and smart home activity sensors. Inform. Health Soc. Care 2020, 45, 96–109. [Google Scholar] [CrossRef] [PubMed]
- Peng, G.; Garcia, L.M.S.; Nunes, M.; Zhang, N. Identifying user requirements of wearable healthcare technologies for Chinese ageing population. In Proceedings of the IEEE 2nd International Smart Cities Conference Improving the Citizens Quality of Life, Trento, Italy, 12–15 September 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Parag, Y.; Butbul, G. Flexiwatts and seamless technology: Public perceptions of demand flexibility through smart home technology. Energy Res. Soc. Sci. 2018, 39, 177–191. [Google Scholar] [CrossRef]
- Barnicoat, G.; Danson, M. The ageing population and smart metering: A field study of householders’ attitudes and behaviours towards energy use in Scotland. Energy Res. Soc. Sci. 2015, 9, 107–115. [Google Scholar] [CrossRef]
- Brown, C.J.; Markusson, N. The responses of older adults to smart energy monitors. Energy Policy 2019, 130, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Coughlin, J.F.; D’Ambrosio, L.A.; Reimer, B.; Pratt, M.R. Older adult perceptions of smart home technologies: Implications for research, policy & market innovations in healthcare. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 1810–1815. [Google Scholar] [CrossRef]
- Kekade, S.; Hseieh, C.H.; Islam, M.M.; Atique, S.; Mohammed Khalfan, A.; Li, Y.C.; Abdul, S.S. The usefulness and actual use of wearable devices among the elderly population. Comput. Methods Progr. Biomed. 2018, 153, 137–159. [Google Scholar] [CrossRef]
- Farina, N.; Sherlock, G.; Thomas, S.; Lowry, R.G.; Banerjee, S. Acceptability and feasibility of wearing activity monitors in community-dwelling older adults with dementia. Int. J. Geriatr. Psychiatry 2019, 34, 617–624. [Google Scholar] [CrossRef]
- Pal, D.; Funilkul, S.; Charoenkitkarn, N.; Kanthamanon, P. Internet-of-Things and Smart Homes for Elderly Healthcare: An End User Perspective. IEEE Access 2018, 6, 10483–10496. [Google Scholar] [CrossRef]
- Kim, M.J.; Oh, M.W.; Cho, M.E.; Lee, H.; Kim, J.T. A critical review of user studies on healthy smart homes. Indoor Built Environ. 2013, 22, 260–270. [Google Scholar] [CrossRef]
- Alsulami, M.H.; Atkins, A.S. Factors Influencing Ageing Population for Adopting Ambient Assisted Living Technologies in the Kingdom of Saudi Arabia. Ageing Int. 2016, 41, 227–239. [Google Scholar] [CrossRef]
- Kok, L.; Berden, C.; Sadiraj, K. Costs and benefits of home care for the elderly versus residential care: A comparison using propensity scores. Eur. J. Health Econ. 2015, 16, 119–131. [Google Scholar] [CrossRef]
- Borg, C.; Hallberg, I.R.; Blomqvist, K. Life satisfaction among older people (65+) with reduced self-care capacity: The relationship to social, health and financial aspects. J. Clin. Nurs. 2006, 15, 607–618. [Google Scholar] [CrossRef]
- Kahya, N.C.; Zorlu, T.; Ozgen, S.; Sari, R.M.; Sen, D.E.; Sagsoz, A. Psychological effects of physical deficiencies in the residences on elderly persons: A case study in Trabzon Old Person’s Home in Turkey. Appl. Ergon. 2009, 40, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Houben, P.P.J. Changing housing for elderly people and co-ordination issues in Europe. Hous. Stud. 2001, 16, 651–673. [Google Scholar] [CrossRef] [Green Version]
- Brookes, N.; Palmer, S.; Callaghan, L. I live with other people and not alone: A survey of the views and experiences of older people using Shared Lives (adult placement). Work Older People 2016, 20, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Diethe, T.; Camplani, M.; Tao, L.; Burrows, A.; Twomey, N.; Kaleshi, D.; Mirmehdi, M.; Flach, P.; Craddock, I. Bridging e-Health and the Internet of Things: The SPHERE Project. IEEE Intell. Syst. 2015, 30, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Balta-Ozkan, N.; Davidson, R.; Bicket, M.; Whitmarsh, L. Social barriers to the adoption of smart homes. Energy Policy 2013, 63, 363–374. [Google Scholar] [CrossRef]
- De Silva, L.C.; Morikawa, C.; Petra, I.M. State of the art of smart homes. Eng. Appl. Artif. Intell. 2012, 25, 1313–1321. [Google Scholar] [CrossRef]
- Lutolf, R. Smart Home Concept and the Integration of Energy Meters into a Home Based System. In Proceedings of the Seventh International Conference on Metering Apparatus and Tariffs for Electricity Supply, Glasgow, UK, 17–19 November 1992; pp. 277–278. [Google Scholar]
- Aldrich, F.K. Smart Homes: Past, Present and Future. Insid. Smart Home 2006, 17–39. [Google Scholar] [CrossRef]
- Schulz, R.; Wahl, H.W.; Matthews, J.T.; De Vito Dabbs, A.; Beach, S.R.; Czaja, S.J. Advancing the aging and technology agenda in gerontology. Gerontologist 2015, 55, 724–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, M.; Estève, D.; Fourniols, J.Y.; Escriba, C.; Campo, E. Smart wearable systems: Current status and future challenges. Artif. Intell. Med. 2012, 56, 137–156. [Google Scholar] [CrossRef] [PubMed]
- Peek, S.T.M.; Wouters, E.J.M.; van Hoof, J.; Luijkx, K.G.; Boeije, H.R.; Vrijhoef, H.J.M. Factors influencing acceptance of technology for aging in place: A systematic review. Int. J. Med. Inform. 2014, 83, 235–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, X.; Wang, H.; Xue, B.; Zhou, M.; Ji, B.; Li, Y. Depth-based human fall detection via shape features and improved extreme learning machine. IEEE J. Biomed. Health Inform. 2014, 18, 1915–1922. [Google Scholar] [CrossRef]
- Daher, M.; El Najjar, M.E.B.; Khalil, M. Automatic Fall Detection System using Sensing Floors. Int. J. Comput. Inf. Sci. 2016, 12, 75–82. [Google Scholar] [CrossRef]
- Yang, L.; Ren, Y.; Zhang, W. 3D depth image analysis for indoor fall detection of elderly people. Digit. Commun. Netw. 2016, 2, 24–34. [Google Scholar] [CrossRef] [Green Version]
- Minvielle, L.; Atiq, M.; Serra, R.; Mougeot, M.; Vayatis, N. Fall detection using smart floor sensor and supervised learning. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 3445–3448. [Google Scholar] [CrossRef]
- Shinmoto Torres, R.L.; Ranasinghe, D.C.; Shi, Q.; Sample, A.P. Sensor enabled wearable RFID technology for mitigating the risk of falls near beds. In Proceedings of the 2013 IEEE International Conference on RFID (RFID), Penang, Malaysia, 30 April–2 May 2013; pp. 191–198. [Google Scholar] [CrossRef]
- Pierleoni, P.; Belli, A.; Palma, L.; Pellegrini, M.; Pernini, L.; Valenti, S. A High Reliability Wearable Device for Elderly Fall Detection. IEEE Sens. J. 2015, 15, 4544–4553. [Google Scholar] [CrossRef]
- Shahzad, A.; Kim, K. FallDroid: An Automated Smart Phone based Fall Detection System using Multiple Kernel Learning. IEEE Trans. Ind. Inform. 2018, 15, 35–44. [Google Scholar] [CrossRef]
- Santos, G.L.; Endo, P.T.; Monteiro, K.H.d.C.; Rocha, E.d.S.; Silva, I.; Lynn, T. Accelerometer-based human fall detection using convolutional neural networks. Sensors 2019, 19, 1644. [Google Scholar] [CrossRef] [Green Version]
- Nemati, E.; Deen, M.; Mondal, T. A wireless wearable ECG sensor for long-term applications. IEEE Commun. Mag. 2012, 50, 36–43. [Google Scholar] [CrossRef]
- Van Dooren, M.; De Vries, J.J.G.G.; Janssen, J.H. Physiology & Behavior Emotional sweating across the body: Comparing 16 different skin conductance measurement locations. Physiol. Behav. 2012, 106, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Sugathan, A.; Roy, G.G.; Kirthyvijay, G.J.; Thomson, J. Application of arduino based platform for wearable health monitoring system. In Proceedings of the 2013 IEEE 1st International Conference on Condition Assessment Techniques in Electrical Systems (CATCON), Kolkata, India, 6–8 December 2013; pp. 1–5. [Google Scholar] [CrossRef]
- Lee, J.; Heo, J.; Lee, W.; Lim, Y.; Kim, Y.; Park, K. Flexible Capacitive Electrodes for Minimizing Motion Artifacts in Ambulatory Electrocardiograms. Sensors 2014, 14, 14732–14743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Y.J.; Kim, I.J.; Ahn, S.C.; Kim, H.G. Mobile health monitoring system based on activity recognition using accelerometer. Simul. Model. Pract. Theory 2010, 18, 446–455. [Google Scholar] [CrossRef]
- Lee, H.; Park, J.; Helal, A. Estimation of Indoor Physical Activity Level Based on Footstep Vibration Signal Measured by MEMS Accelerometer for Personal Health Care Under Smart. Control Instrum. 2009, 5801 LNCS, 148–162. [Google Scholar] [CrossRef]
- Zambrano-montenegro, D.; García-bermúdez, R.; Member, S. An approach to beacons-based location for AAL systems in broadband communication constrained scenarios. In Proceedings of the 2018 IEEE 8th International Conference on Consumer Electronics-Berlin (ICCE-Berlin), Berlin, Germany, 2–5 September 2018; pp. 3–6. [Google Scholar] [CrossRef]
- Nath, R.K.; Bajpai, R.; Thapliyal, H. IoT Based Indoor Location Detection System for Smart Home Environment. In Proceedings of the 2018 IEEE International Conference on Consumer Electronics (ICCE), Las Vegas, NV, USA, 12–14 January 2018; pp. 2018–2020. [Google Scholar]
- Fernández-Llatas, C.; Benedi, J.-M.; García-Gómez, J.; Traver, V. Process Mining for Individualized Behavior Modeling Using Wireless Tracking in Nursing Homes. Sensors 2013, 13, 15434–15451. [Google Scholar] [CrossRef] [Green Version]
- Belmonte-Fernández, Ó.; Puertas-Cabedo, A.; Torres-Sospedra, J.; Montoliu-Colás, R.; Trilles-Oliver, S. An Indoor Positioning System Based on Wearables for Ambient-Assisted Living. Sensors 2016, 17, 36. [Google Scholar] [CrossRef]
- Ni, B.; Wang, G.; Moulin, P. RGBD-HuDaAct: A color-depth video database for human daily activity recognition. In Proceedings of the 2011 IEEE International Conference on Computer Vision Workshops (ICCV Workshops), Barcelona, Spain, 6–13 November 2011; pp. 1147–1153. [Google Scholar] [CrossRef]
- Awais, M.; Chiari, L.; Ihlen, E.A.F.; Helbostad, J.L.; Palmerini, L. Physical Activity Classification for Elderly People in Free-Living Conditions. IEEE J. Biomed. Health Inform. 2019, 23, 197–207. [Google Scholar] [CrossRef]
- Morita, T.; Taki, K.; Fujimoto, M.; Suwa, H.; Arakawa, Y.; Yasumoto, K. BLE Beacon-based Activity Monitoring System toward Automatic Generation of Daily Report. In Proceedings of the 2018 IEEE International Conference on Pervasive Computing and Communications Workshops (PerCom Workshops), Athens, Greece, 19–23 March 2018; Volume 26, pp. 788–793. [Google Scholar] [CrossRef]
- Kim, J.Y.; Liu, N.; Tan, H.X.; Chu, C.H. Unobtrusive Monitoring to Detect Depression for Elderly with Chronic Illnesses. IEEE Sens. J. 2017, 17, 5694–5704. [Google Scholar] [CrossRef]
- Chen, S.; Liu, T.; Gao, F.; Ji, J.; Xu, Z.; Qian, B.; Wu, H.; Guan, X. Butler, Not Servant: A Human-Centric Smart Home Energy Management System. IEEE Commun. Mag. 2017, 55, 27–33. [Google Scholar] [CrossRef]
- Siano, P.; Graditi, G.; Atrigna, M.; Piccolo, A. Designing and testing decision support and energy management systems for smart homes. J. Ambient Intell. Humaniz. Comput. 2013, 4, 651–661. [Google Scholar] [CrossRef]
- Marques, G.; Pitarma, R. An Indoor Monitoring System for Ambient Assisted Living Based on Internet of Things Architecture. Int. J. Environ. Res. Public Health 2016, 13, 1152. [Google Scholar] [CrossRef] [Green Version]
- Preethichandra, D.M.G. Design of a smart indoor air quality monitoring wireless sensor network for assisted living. In Proceedings of the 2013 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Minneapolis, MN, USA, 6–9 May 2013; pp. 1306–1310. [Google Scholar] [CrossRef]
- Ranasinghe, S.; Al MacHot, F.; Mayr, H.C. A review on applications of activity recognition systems with regard to performance and evaluation. Int. J. Distrib. Sens. Netw. 2016, 12. [Google Scholar] [CrossRef] [Green Version]
- Balta-Ozkan, N.; Amerighi, O.; Boteler, B. A comparison of consumer perceptions towards smart homes in the UK, Germany and Italy: Reflections for policy and future research. Technol. Anal. Strateg. Manag. 2014, 26, 1176–1195. [Google Scholar] [CrossRef]
- Agbakoba, R.; McGee-Lennon, M.; Bouamrane, M.M.; Watson, N.; Mair, F.S. Implementation factors affecting the large-scale deployment of digital health and well-being technologies: A qualitative study of the initial phases of the “Living-It-Up” programme. Health Inform. J. 2016, 22, 867–877. [Google Scholar] [CrossRef] [Green Version]
- Leonard, K.J. Critical Success Factors Realting to Healthcare’s Adoption of New Technology: A guide to increasing the likelihood of successful implementation. Electron. Healthc. 2004, 2, 72–81. [Google Scholar]
- Sponselee, A.; Schouten, B.; Bouwhuis, D.; Willems, C. Smart Home Technology for the Elderly: Perceptions of Multidisciplinary Stakeholders. In Proceedings of the Constructing Ambient Intelligence; Mühlhäuser, M., Ferscha, A., Aitenbichler, E., Eds.; Springer: Berlin/Heidelberg, Germany, 2008; pp. 314–326. [Google Scholar] [CrossRef] [Green Version]
- Jacelon, C.S.; Hanson, A. Older adults’ participation in the development of smart environments: An integrated review of the literature. Geriatr. Nurs. (Minneap) 2013, 34, 116–121. [Google Scholar] [CrossRef]
- Lee, L.N.; Kim, M.J. A Critical Review of Smart Residential Environments for Older Adults with a Focus on Pleasurable Experience. Front. Psychol. 2020, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Visutsak, P.; Daoudi, M. The smart home for the elderly: Perceptions, technologies and psychological accessibilities: The requirements analysis for the elderly in Thailand. In Proceedings of the 2017 XXVI International Conference on Information, Communication and Automation Technologies (ICAT), Sarajevo, Bosnia-Herzegovina, 1–6 December 2017. [Google Scholar] [CrossRef] [Green Version]
- Hargreaves, T.; Nye, M.; Burgess, J. Making energy visible: A qualitative field study of how householders interact with feedback from smart energy monitors. Energy Policy 2010, 38, 6111–6119. [Google Scholar] [CrossRef]
- Hargreaves, T.; Nye, M.; Burgess, J. Keeping energy visible? Exploring how householders interact with feedback from smart energy monitors in the longer term. Energy Policy 2013, 52, 126–134. [Google Scholar] [CrossRef]
- Fang, Y.M.; Chang, C.C. Users’ psychological perception and perceived readability of wearable devices for elderly people. Behav. Inf. Technol. 2016, 35, 225–232. [Google Scholar] [CrossRef]
- Hall, A.; Boulton, E.; Stanmore, E. Older adults’ perceptions of wearable technology hip protectors: Implications for further research and development strategies. Disabil. Rehabil. Assist. Technol. 2019, 14, 663–668. [Google Scholar] [CrossRef] [Green Version]
- Qi, W.; Zhou, L. A User Study of Wearable Product for Elderly Care—Taking Community Nursing Service as Example. In Proceedings of the 2018 11th International Congress on Image and Signal Processing, BioMedical Engineering and Informatics (CISP-BMEI), Beijing, China, 13–15 October 2019; pp. 1–5. [Google Scholar] [CrossRef]
- Vincent, C.; Vincent, C.; Routhier, F.; Drouin, G.; Routhier, F. Examination of New Environmental Control Applications. Assist. Technol. 2002, 14, 98–111. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Tilke, D.; Adams, T.; Crandall, A.S.; Cook, D.J.; Schmitter-Edgecombe, M. Smart home in a box: Usability study for a large scale self-installation of smart home technologies. J. Reliab. Intell. Environ. 2016, 2, 93–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuchiya, L.D.; Braga, L.F.; de Faria Oliveira, O.; de Bettio, R.W.; Greghi, J.G.; Freire, A.P. Design and evaluation of a mobile smart home interactive system with elderly users in Brazil. Pers. Ubiquitous Comput. 2020. [Google Scholar] [CrossRef]
- Ashraf, A.; Liu, J.H.; Rauf, Q. Aging population perception and post adoption behavior about the usability of smart home technology of pakistani culture. In Proceedings of the 2020 6th International Conference on Computing and Data Engineering, Sanya, China, 4–6 January 2020; pp. 179–188. [Google Scholar] [CrossRef]
- Dou, J.; Qin, J.; Wang, Q.; Zhao, Q. Identification of usability problems and requirements of elderly Chinese users for smart TV interactions. Behav. Inf. Technol. 2019, 38, 664–677. [Google Scholar] [CrossRef]
- Ehrenhard, M.; Kijl, B.; Nieuwenhuis, L. Market adoption barriers of multi-stakeholder technology: Smart homes for the aging population. Technol. Forecast. Soc. Chang. 2014, 89, 306–315. [Google Scholar] [CrossRef]
- Bregman, D.; Korman, A. A universal implementation model for the smart home. Int. J. Smart Home 2009, 3, 15–30. [Google Scholar]
- Lee, H.; Kobsa, A. Privacy preference modeling and prediction in a simulated campuswide IoT environment. In Proceedings of the 2017 IEEE International Conference on Pervasive Computing and Communications (PerCom), Kona, HI, USA, 13–17 March 2017; pp. 276–285. [Google Scholar] [CrossRef]
- Suo, H.; Wan, J.; Zou, C.; Liu, J. Security in the internet of things: A review. In Proceedings of the 2012 International Conference on Computer Science and Electronics Engineering, Hangzhou, China, 23–25 March 2012; Volume 3, pp. 648–651. [Google Scholar] [CrossRef]
- Chau, K.Y.; Lam, M.H.S.; Cheung, M.L.; Tso, E.K.H.; Flint, S.W.; Broom, D.R.; Tse, G.; Lee, K.Y. Smart technology for healthcare: Exploring the antecedents of adoption intention of healthcare wearable technology. Health Psychol. Res. 2019, 7, 33–39. [Google Scholar] [CrossRef]
- Rashid, H.; Singh, P.; Stankovic, V.; Stankovic, L. Can non-intrusive load monitoring be used for identifying an appliance’s anomalous behaviour? Appl. Energy 2019, 238, 796–805. [Google Scholar] [CrossRef] [Green Version]
- Davis, F.D. A technology acceptance model for empirically testing new end-user information systems: Theory and results. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 1985; p. 291. [Google Scholar]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. Manag. Inf. Syst. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Thong, J.Y.L.; Xu, X. Consumer Acceptance and Use of Information Technology: Extending the Unified Theory of Acceptance and Use of Technology. MIS Q. 2012, 36, 157–178. [Google Scholar] [CrossRef] [Green Version]
- Park, E. User acceptance of smart wearable devices: An expectation-confirmation model approach. Telemat. Inform. 2020, 47. [Google Scholar] [CrossRef]
- Baudier, P.; Ammi, C.; Deboeuf-Rouchon, M. Smart home: Highly-educated students’ acceptance. Technol. Forecast. Soc. Chang. 2020, 153, 119355. [Google Scholar] [CrossRef]
- Gill, P.; Stewart, K.; Treasure, E.; Chadwick, B. Methods of data collection in qualitative research: Interviews and focus groups. Br. Dent. J. 2008, 204, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, A. What are focus groups? Why use focus groups and not other methods? Soc. Res. Updat. 1997, 19, 1–8. [Google Scholar]
- Nielsen, J.; Molich, R. Heuristic evaluation of user interfaces. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Austin, TX, USA, 30 April–4 June 1990; pp. 249–256. [Google Scholar] [CrossRef]
- Ni, H.; Wu, S.; Abdulrazak, B.; Zhang, D.; Ma, X.; Zhou, X. Non-intrusive sleep pattern recognition with ubiquitous sensing in elderly assistive environment. Front. Comput. Sci. 2015, 9, 966–979. [Google Scholar] [CrossRef]
- Mihailidis, A.; Cockburn, A.; Longley, C.; Boger, J. The acceptability of home monitoring technology among community-dwelling older adults and baby boomers. Assist. Technol. 2008, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Jang, I.Y.; Kim, H.R.; Lee, E.; Jung, H.W.; Park, H.; Cheon, S.H.; Lee, Y.S.; Park, Y.R. Impact of a wearable device-based walking programs in rural older adults on physical activity and health outcomes: Cohort study. JMIR mHealth uHealth 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.; Thompson, H.J.; Joe, J.; Hall, A.; Demiris, G. Examining Korean and Korean American older adults’ perceived acceptability of home-based monitoring technologies in the context of culture. Inform. Health Soc. Care 2017, 42, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.; Demiris, G.; Thompson, H.J.; Chen, K.Y.; Burr, R.; Patel, S.; Fogarty, J. Feasibility testing of a home-based sensor system to monitor mobility and daily activities in Korean American older adults. Int. J. Older People Nurs. 2017, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Abbate, S.; Avvenuti, M.; Light, J. Usability Study of a Wireless Monitoring System among Alzheimer’s Disease Elderly Population. Int. J. Telemed. Appl. 2014, 2014. [Google Scholar] [CrossRef]
- Demiris, G.; Hensel, B.K.; Skubic, M.; Rantz, M. Senior residents’ perceived need of and preferences for “smart home” sensor technologies. Int. J. Technol. Assess. Health Care 2008, 24, 120–124. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare the Results of the 2017 National Survey of Living Conditions and Welfare Needs of Korean Older Persons. Available online: http://www.prism.go.kr/homepage/entire/retrieveEntireDetail.do?research_id=1351000-201800182 (accessed on 10 October 2020).
- Singh, D.; Psychoula, I.; Kropf, J.; Hanke, S.; Holzinger, A. Users’ Perceptions and Attitudes Towards Smart Home Technologies. In Smart Homes and Health Telematics, Designing a Better Future: Urban Assisted Living; ICOST Lecture Notes in Computer, Science; Mokhtari, M., Abdulrazak, B., Aloulou, H., Eds.; Springer: Cham, Switzerland, 2018; Volume 10898. [Google Scholar] [CrossRef]
- Mahmood, A.; Yamamoto, T.; Lee, M.; Steggell, C. Perceptions and use of gerotechnology: Implications for aging in place. J. Hous. Elderly 2008, 22, 104–126. [Google Scholar] [CrossRef]
- Rasyidah, Z.A.; Hariati, A.H.; Rosadah, M.; Maryanti, M.R. Perceptions on smart home concept among the millennials in Johor. IOP Conf. Ser. Mater. Sci. Eng. 2020, 849. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, T.H.; Ma, J.H.; Cha, S.H. Elderly Perception on the Internet of Things-Based Integrated Smart-Home System. Sensors 2021, 21, 1284. https://doi.org/10.3390/s21041284
Jo TH, Ma JH, Cha SH. Elderly Perception on the Internet of Things-Based Integrated Smart-Home System. Sensors. 2021; 21(4):1284. https://doi.org/10.3390/s21041284
Chicago/Turabian StyleJo, Tae Hee, Jae Hoon Ma, and Seung Hyun Cha. 2021. "Elderly Perception on the Internet of Things-Based Integrated Smart-Home System" Sensors 21, no. 4: 1284. https://doi.org/10.3390/s21041284