
Assessment of the Shank-to-Vertical Angle While Changing Heel Heights Using a Single Inertial Measurement Unit in Individuals with Incomplete Spinal Cord Injury Wearing an Ankle-Foot-Orthosis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
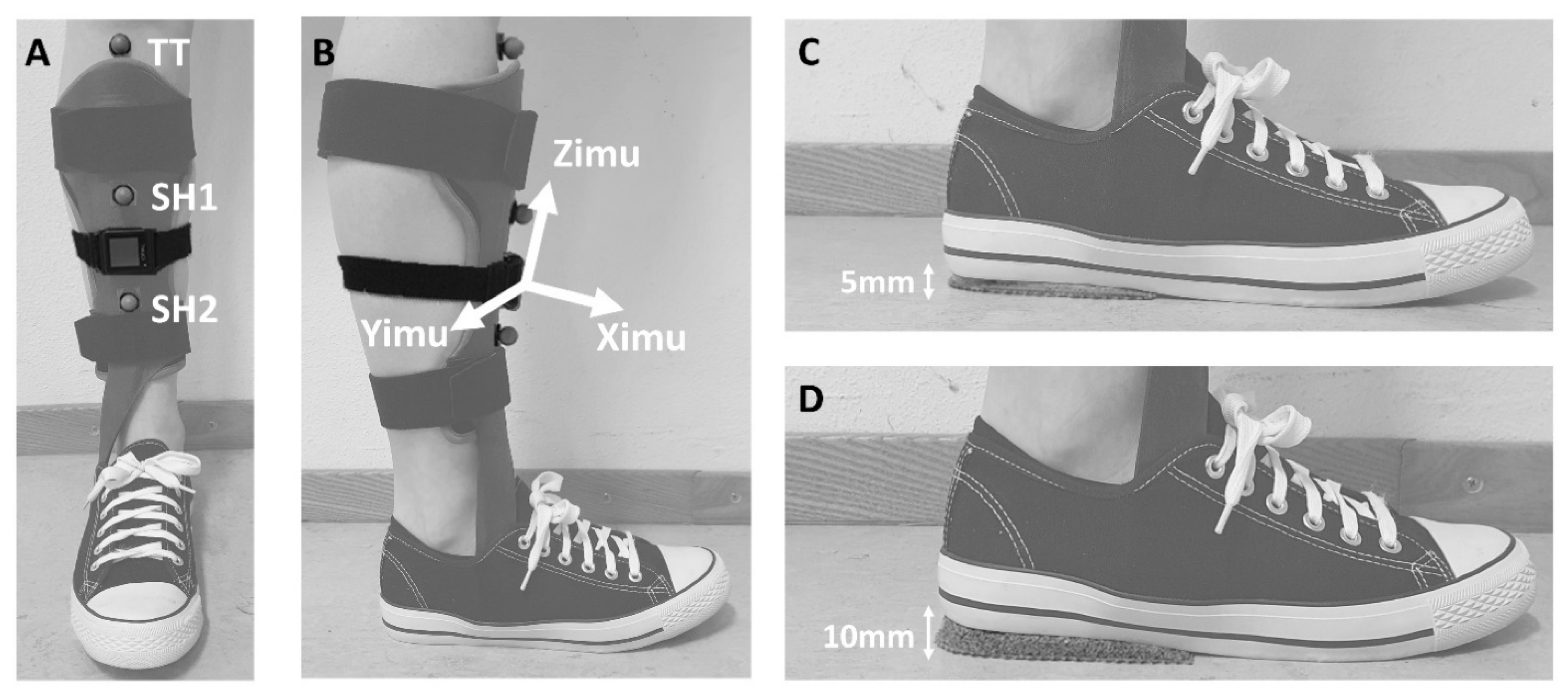
2.2. Equipment
2.3. Measurement Procedure
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
3.1. Participants
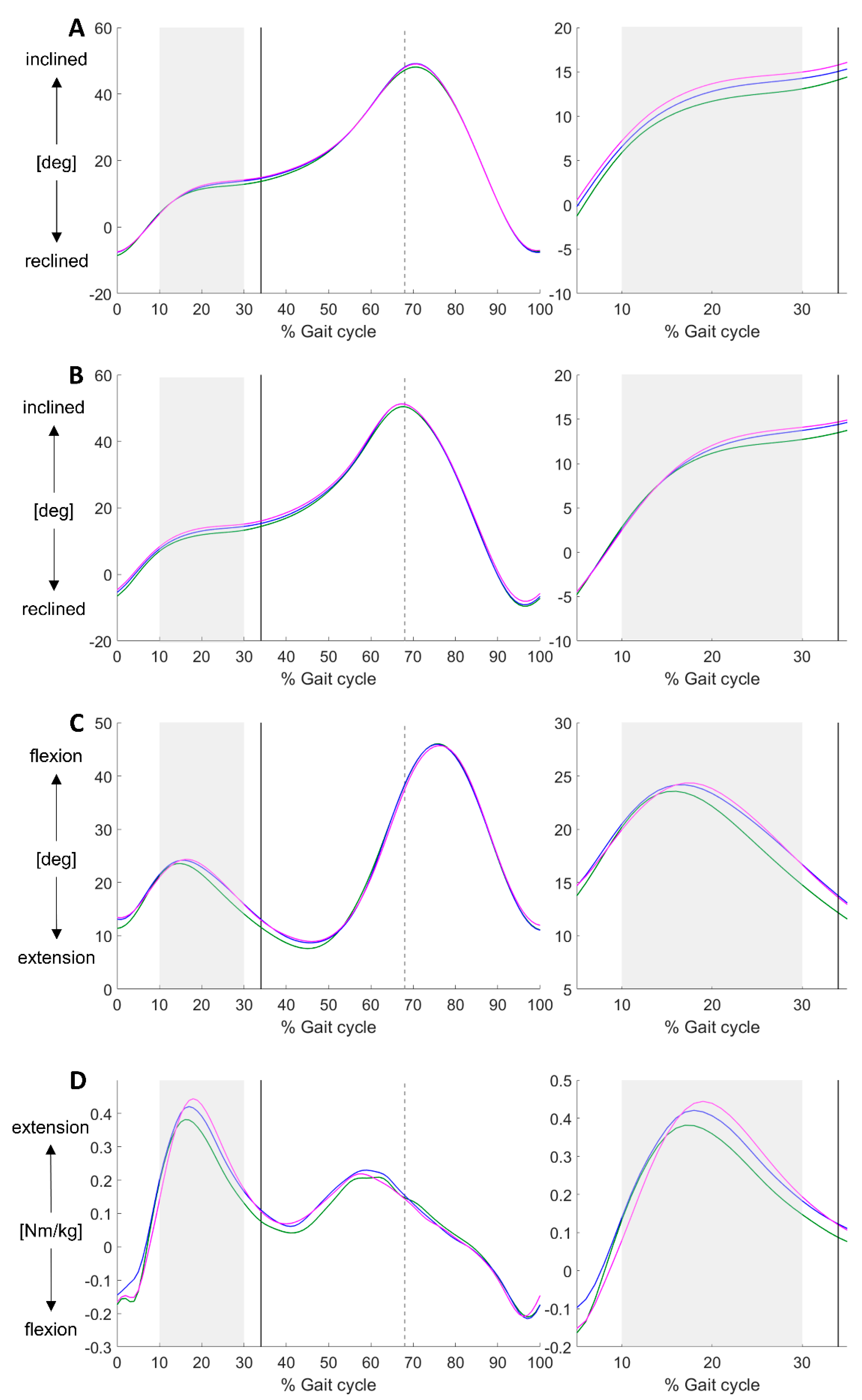
3.2. Validity
3.3. Heel Height Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pépin, A.; Norman, K.E.; Barbeau, H. Treadmill walking in incomplete spinal-cord-injured subjects: 1. Adaptation to changes in speed. Spinal Cord 2003, 41, 257–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, H.B.; Chvatal, S.A.; French, M.A.; Ting, L.H.; Trumbower, R.D. Neuromuscular constraints on muscle coordination during overground walking in persons with chronic incomplete spinal cord injury. Clin. Neurophysiol 2014, 125, 2024–2035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waters, R.; Yakura, J.; Adkins, R. Gait performance after spinal cord injury. Clin. Orthop. Relat. Res. 1993, 288, 87–96. [Google Scholar] [CrossRef]
- Barbeau, H.; Ladouceur, M.; Norman, K.E.; Pepin, A.; Leroux, A. Walking after spinal cord injury: Evaluation, treatment, and functional recovery. Arch. Phys. Med. Rehabil 1999, 80, 225–235. [Google Scholar] [CrossRef]
- Wirz, M.; van Hedel, H.J.A. Balance, gait, and falls in spinal cord injury. Handb. Clin. Neurol. 2018, 159, 367–384. [Google Scholar]
- Atrice, M.B. Lower extremity orthotic management for the spinal-cord-injured client. Top. Spinal Cord Inj. Rehabil. 2000, 5, 1–10. [Google Scholar] [CrossRef]
- Arazpour, M.; Tajik, H.R.; Aminian, G.; Bani, M.A.; Ghomshe, F.T.; Hutchins, S.W. Comparison of the effects of solid versus hinged ankle foot orthoses on select temporal gait parameters in patients with incomplete spinal cord injury during treadmill walking. Prosthet. Orthot. Int. 2013, 37, 70–75. [Google Scholar] [CrossRef]
- Kim, C.M.; Eng, J.J.; Whittaker, M.W. Effects of a simple functional electric system and/or a hinged ankle-foot orthosis on walking in persons with incomplete spinal cord injury. Arch. Phys. Med. Rehabil. 2004, 85, 1718–1723. [Google Scholar] [CrossRef]
- Beekman, C.; Perry, J.; Boyd, L.A.; Newsam, C.J.; Mulroy, S.J. The effects of a dorsiflexion-stopped ankle-foot orthosis on walking in individuals with incomplete spinal cord injury. Top. Spinal Cord Inj. Rehabil. 2000, 5, 54–62. [Google Scholar] [CrossRef]
- Brehm, M.A.; Harlaar, J.; Schwartz, M. Effect of ankle-foot orthoses on walking efficiency and gait in children with cerebral palsy. J. Rehabil. Med. 2008, 40, 529–534. [Google Scholar] [CrossRef] [Green Version]
- Eddison, N.; Chockalingam, N. The effect of tuning ankle foot orthoses-footwear combination on the gait parameters of children with cerebral palsy. Prosthet. Orthot. Int. 2013, 37, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Jagadamma, K.C.; Coutts, F.J.; Mercer, T.H.; Herman, J.; Yirrel, J.; Forbes, L.; Van Der Linden, M.L. Effects of tuning of ankle foot orthoses-footwear combination using wedges on stance phase knee hyperextension in children with cerebral palsy Preliminary results. Disabil. Rehabil. Assist. Technol. 2009, 4, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Owen, E. The Importance of Being Earnest about Shank and Thigh Kinematics Especially When Using Ankle-Foot Orthoses. Prosthet. Orthot. Int. 2010, 34, 254–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerkum, Y.L.; Houdijk, H.; Brehm, M.-A.; Buizer, A.I.; Kessels, M.L.C.; Sterk, A.; van den Noort, J.C.; Harlaar, J. The Shank-to-Vertical-Angle as a parameter to evaluate tuning of Ankle-Foot Orthoses. Gait Posture 2015, 42, 269–274. [Google Scholar] [CrossRef] [PubMed]
- de Jong, L.A.F.; Kerkum, Y.L.; van Oorschot, W.; Keijsers, N.L.W. A single Inertial Measurement Unit on the shank to assess the Shank-to-Vertical Angle. J. Biomech. 2020, 108, 109895. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.T.; Baicoianu, N.A.; Howell, D.B.; Peters, K.M.; Steele, K.M. Accuracy and repeatability of smartphone sensors for measuring shank-to-vertical angle. Prosthet. Orthot. Int. 2020, 44, 172–179. [Google Scholar] [CrossRef]
- Kirshblum, S.C.; Waring, W.; Biering-Sorensen, F.; Burns, S.P.; Johansen, M.; Schmidt-Read, M.; Donovan, W.; Graves, D.; Jha, A.; Jones, L.; et al. Reference for the 2011 revision of the International Standards for Neurological Classification of Spinal Cord Injury. J. Spinal Cord Med. 2011, 34, 547–554. [Google Scholar] [CrossRef] [Green Version]
- Riddoch, G.; Medical Research Council. Aids to the Examination of the Peripheral Nervous System. Available online: https://mrc.ukri.org/documents/pdf/aids-to-the-examination-of-the-peripheral-nervous-system-mrc-memorandum-no-45-superseding-war-memorandum-no-7/ (accessed on 25 January 2021).
- Woltring, H.J. A Fortran package for generalized, cross-validatory spline smoothing and differentiation. Adv. Eng. Softw. 1986, 8, 104–113. [Google Scholar] [CrossRef]
- Aminian, K.; Najafi, B.; Büla, C.; Leyvraz, P.F.; Robert, P. Spatio-temporal parameters of gait measured by an ambulatory system using miniature gyroscopes. J. Biomech. 2002, 35, 689–699. [Google Scholar] [CrossRef]
- Perry, J. Gait Analysis: Normal and Pathological Function. SLACK Inc. 1992, 12, 815. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power for the Behavioral Sciences, 2nd ed.; Laurence Erlbaum and Associates: Hillsdale, NJ, USA, 1988; ISBN 0-8058-0283-5. [Google Scholar]
- Jagadamma, K.C.; Owen, E.; Coutts, F.J.; Herman, J.; Yirrell, J.; Mercer, T.H.; Van Der Linden, M.L. The effects of tuning an ankle-foot orthosis footwear combination on kinematics and kinetics of the knee joint of an adult with hemiplegia. Prosthet. Orthot. Int. 2010, 34, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Eddison, N.; Healy, A.; Needham, R.; Chockalingam, N. The effect of tuning ankle foot orthoses-footwear combinations on gait kinematics of children with cerebral palsy: A case series. Foot 2020, 43, 101660. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Mean ± SD |
|---|---|
| Age (years) | 55.0 ± 14.1 |
| Gender, male/female | 10/2 |
| Height (cm) | 182.4 ± 8.7 |
| Weight (kg) | 90.0 ± 19.9 |
| ASIA Impairment Scale, grade C/D | 1/11 |
| Level of the lesion, C1-8/T1-12/L1-5 | 4/4/4 |
| Time since injury | 161 ± 212 |
| Affected leg, left/right | 6/6 |
| MRC plantar flexors, 0/1/2/3/4/5 | 3/1/2/4/1/1 |
| MRC dorsal flexors, 0/1/2/3/4/5 | 1/2/0/5/3/1 |
| AFO type, dynamic */hinged ** | 11/1 |
| Conditions | RefHH | LowHH | HighHH | F | p |
|---|---|---|---|---|---|
| Midstance phase | |||||
| SVAIMU (°) | 11.3 ± 4.3 | 12.4 ± 4.8 | 13.2 ± 4.3 | 3.87 a | 0.036 |
| SVA3DGA (°) | 10.6 ± 4.2 | 10.9 ± 4.3 | 11.2 ± 4.2 | 2.51 a | 0.104 |
| Knee angle (°) | 20.2 ± 4.3 | 21.5 ± 3.8 | 21.6 ± 3.1 | 3.56 b | 0.053 |
| Knee moment (Nm/kg) | 0.28 ± 0.12 | 0.31 ± 0.12 | 0.33 ± 0.12 | 5.03 b | 0.020 |
| Instant of midstance | |||||
| SVAIMU (°) | 13.4 ± 4.2 | 14.6 ± 4.5 | 15.3 ± 3.5 | 3.68 a | 0.042 |
| SVA3DGA (°) | 13.6 ± 4.6 | 14.5 ± 4.3 | 14.8 ± 4.3 | 6.51 a | 0.006 |
| Knee angle (°) | 11.4 ± 6.3 | 12.7 ± 5.3 | 12.8 ± 5.2 | 3.03 b | 0.077 |
| Knee moment (Nm/kg) | 0.07 ± 0.16 | 0.11 ± 0.13 | 0.12 ± 0.14 | 3.27 b | 0.065 |
| Terminal stance phase | |||||
| Knee moment (Nm/kg) | 0.07 ± 0.16 | 0.10 ± 0.16 | 0.11 ± 0.15 | 2.24 b | 0.139 |
| Gait characteristics | |||||
| Walking speed (m/s) | 0.85 ± 0.18 | 0.84 ± 0.17 | 0.83 ± 0.17 | 1.66 a | 0.214 |
| Conditions | Ref–Low | Low–High | Ref–High | |||
|---|---|---|---|---|---|---|
| Mean ± SD | ES | Mean ± SD | ES | Mean ± SD | ES | |
| Midstance phase | ||||||
| SVAimu (°) | 1.1 ± 2.6 | 0.40 | 0.80 ± 2.4 | 0.33 | 1.9 ± 1.8 * | 1.03 |
| SVA3DGA (°) | 0.32 ± 1.1 | 0.28 | 0.27 ± 0.6 | 0.44 | 0.59 ± 0.9 | 0.65 |
| Knee angle (°) | 1.3 ± 1.8 | 0.69 | 0.16 ± 1.6 | 0.10 | 1.4 ± 1.9 | 0.76 |
| Knee moment (Nm/kg) | 0.04 ±0.07 | 0.54 | 0.02 ± 0.05 | 0.39 | 0.05 ± 0.04 * | 1.43 |
| Instant of midstance | ||||||
| SVAimu (°) | 1.2 ± 2.7 | 0.44 | 0.6 ± 2.3 | 0.28 | 1.8 ± 2.0 * | 0.89 |
| SVA3DGA (°) | 0.9 ± 1.4 | 0.69 | 0.3 ± 1.0 | 0.26 | 1.2 ± 1.2 * | 0.98 |
| Knee angle (°) | 1.3 ± 1.9 | 0.70 | 0.04 ± 1.5 | 0.03 | 1.4 ± 2.3 | 0.61 |
| Knee moment (Nm/kg) | 0.04 ± 0.08 | 0.50 | 0.01 ± 0.04 | 0.23 | 0.05 ± 0.06 | 0.84 |
| Terminal stance phase | ||||||
| Knee moment (Nm/kg) | 0.03 ± 0.07 | 0.13 | 0.01 ± 0.04 | 0.08 | 0.04 ± 0.05 | 0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Jong, L.A.F.; Kerkum, Y.L.; de Groot, T.; Vos-van der Hulst, M.; van Nes, I.J.W.; Keijsers, N.L.W. Assessment of the Shank-to-Vertical Angle While Changing Heel Heights Using a Single Inertial Measurement Unit in Individuals with Incomplete Spinal Cord Injury Wearing an Ankle-Foot-Orthosis. Sensors 2021, 21, 985. https://doi.org/10.3390/s21030985
de Jong LAF, Kerkum YL, de Groot T, Vos-van der Hulst M, van Nes IJW, Keijsers NLW. Assessment of the Shank-to-Vertical Angle While Changing Heel Heights Using a Single Inertial Measurement Unit in Individuals with Incomplete Spinal Cord Injury Wearing an Ankle-Foot-Orthosis. Sensors. 2021; 21(3):985. https://doi.org/10.3390/s21030985
Chicago/Turabian Stylede Jong, Lysanne A. F., Yvette L. Kerkum, Tom de Groot, Marije Vos-van der Hulst, Ilse J. W. van Nes, and Noel L. W. Keijsers. 2021. "Assessment of the Shank-to-Vertical Angle While Changing Heel Heights Using a Single Inertial Measurement Unit in Individuals with Incomplete Spinal Cord Injury Wearing an Ankle-Foot-Orthosis" Sensors 21, no. 3: 985. https://doi.org/10.3390/s21030985