
Combining Action Observation Treatment with a Brain–Computer Interface System: Perspectives on Neurorehabilitation

 ,
, 
 ,
,  , and
, and {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Towards Translational, Evidence-Based Approaches in Neurorehabilitation
- Firstly, it should be evidence based. The efficacy of any rehabilitation practice should be supported by the results merging from randomized controlled studies or clinical trials, comparing a specific approach with a control condition.
- A neurorehabilitation approach needs to be grounded in neurophysiology: every approach should have its theoretical background in physiology principles and mechanisms. For example, when speaking about motor recovery, the terrific advance of knowledge regarding the organization and functions of the motor system coming from basic neuroscience should be taken into account. All approaches should consider neuroscientific studies to transfer knowledge in clinical practice.
- Any approach in neurorehabilitation should also aim at the recovery of functions and, as a consequence, of the capacity of patients to interact with the environment and other people, as assumed when considering health not only as the condition in which individuals are free from diseases [3]. It is worth stressing that in many cases, physiotherapists focus on ways to circumvent functional deficits, suggesting alternative strategies in order to allow patients to face daily activities. This attitude leads to a compensation or a reeducation of functions, rather than a cure for them through remediation. In contrast with this rather diffuse attitude, we believe rehabilitative tools should aim at restoring the neural structures whose damage caused the impaired functions, or activating supplementary or related pathways that may perform the original functions.
2. Action Observation Treatment and Its Efficacy in Clinical Practice
3. Combining AOT with a Brain–Computer Interface to Improve the Actual Motor Execution of Patients
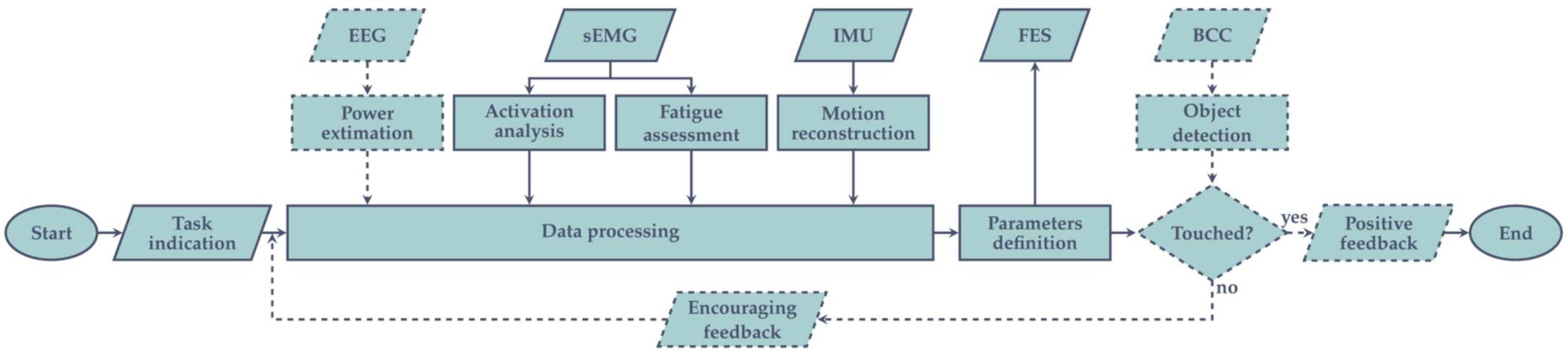
- EEG activity is analyzed considering its power density in the beta and mu bands, aiming to detect whether an ERD occurs and to define its magnitude;
- Muscles activity is monitored by the sEMG sensors, distinguishing between each acquisition channel (i.e., different muscular fiber recruitment) and evaluating if the relation among them reflects the physiological behavior;
- From sEMG, muscular fatigue assessment is performed too, analyzing the M-waves from the different muscles, and considering its degradation over time;
- Position, angular velocity, and linear acceleration from the different employed IMUs are combined to reconstruct the limb kinematic across space, evaluating if they are consistent with physiological movements.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taub, E.; Uswatte, G.; Elbert, T. New treatments in neurorehabilitation founded on basic research. Nat. Rev. Neurosci. 2002, 3, 228–236. [Google Scholar] [CrossRef] [Green Version]
- Small, S.L.; Buccino, G.; Solodkin, A. Brain repair after stroke—a novel neurological model. Nat. Rev. Neurol. 2013, 9, 698–707. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001; ISBN 978-92-4-154542-6. [Google Scholar]
- Shi, Y.X.; Tian, J.H.; Yang, K.H.; Zhao, Y. Modified constraint-induced movement therapy versus traditional rehabilitation in patients with upper-extremity dysfunction after stroke: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2011, 92, 972–982. [Google Scholar] [CrossRef] [PubMed]
- Corbetta, D.; Sirtori, V.; Castellini, G.; Moja, L.; Gatti, R. Constraint-induced movement therapy for upper extremities in people with stroke. Cochrane Database Syst. Rev. 2015, CD004433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakzewski, L.; Gordon, A.; Eliasson, A.-C. The state of the evidence for intensive upper limb therapy approaches for children with unilateral cerebral palsy. J. Child Neurol. 2014, 29, 1077–1090. [Google Scholar] [CrossRef] [PubMed]
- Nudo, R.J. Mechanisms for recovery of motor function following cortical damage. Curr. Opin. Neurobiol. 2006, 16, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, V.S.; Altschuler, E.L. The use of visual feedback, in particular mirror visual feedback, in restoring brain function. Brain J. Neurol. 2009, 132, 1693–1710. [Google Scholar] [CrossRef] [Green Version]
- Thieme, H.; Mehrholz, J.; Pohl, M.; Behrens, J.; Dohle, C. Mirror therapy for improving motor function after stroke. Stroke 2013, 44, e1–e2. [Google Scholar] [CrossRef] [Green Version]
- Bruchez, R.; Jequier Gygax, M.; Roches, S.; Fluss, J.; Jacquier, D.; Ballabeni, P.; Grunt, S.; Newman, C.J. Mirror therapy in children with hemiparesis: A randomized observer-blinded trial. Dev. Med. Child Neurol. 2016, 58, 970–978. [Google Scholar] [CrossRef]
- Jeannerod, M. The representing brain: Neural correlates of motor intention and imagery. Behav. Brain Sci. 1994, 17, 187–202. [Google Scholar] [CrossRef] [Green Version]
- Linden, C.A.; Uhley, J.E.; Smith, D.; Bush, M.A. The effects of mental practice on walking balance in an elderly population. Occup. Ther. J. Res. 1989, 9, 155–169. [Google Scholar] [CrossRef]
- Butler, A.J.; Page, S.J. Mental practice with motor imagery: Evidence for motor recovery and cortical reorganization after stroke. Arch. Phys. Med. Rehabil. 2006, 87, S2–S11. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.P.; Chan, C.C.; Lee, T.M.; Hui-Chan, C.W. Mental imagery for promoting relearning for people after stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2004, 85, 1403–1408. [Google Scholar] [CrossRef]
- Tamir, R.; Dickstein, R.; Huberman, M. Integration of Motor Imagery and Physical Practice in Group Treatment Applied to Subjects With Parkinson’s Disease. Neurorehabil. Neural Repair 2007, 21, 68–75. [Google Scholar] [CrossRef]
- Jeannerod, M. Neural simulation of action: A unifying mechanism for motor cognition. NeuroImage 2001, 14, S103–S109. [Google Scholar] [CrossRef]
- Hardwick, R.M.; Caspers, S.; Eickhoff, S.B.; Swinnen, S.P. Neural correlates of action: Comparing meta-analyses of imagery, observation, and execution. Neurosci. Biobehav. Rev. 2018, 94, 31–44. [Google Scholar] [CrossRef]
- McInnes, K.; Friesen, C.; Boe, S. Specific Brain Lesions Impair Explicit Motor Imagery Ability: A Systematic Review of the Evidence. Arch. Phys. Med. Rehabil. 2016, 97, 478–489.e1. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Craighero, L. The mirror-neuron system. Annu. Rev. Neurosci. 2004, 27, 169–192. [Google Scholar] [CrossRef] [Green Version]
- di Pellegrino, G.; Fadiga, L.; Fogassi, L.; Gallese, V.; Rizzolatti, G. Understanding motor events: A neurophysiological study. Exp. Brain Res. 1992, 91, 176–180. [Google Scholar] [CrossRef]
- Vogt, S.; Thomaschke, R. From visuo-motor interactions to imitation learning: Behavioural and brain imaging studies. J. Sports Sci. 2007, 25, 497–517. [Google Scholar] [CrossRef] [Green Version]
- Mattar, A.A.G.; Gribble, P.L. Motor learning by observing. Neuron 2005, 46, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefan, K.; Cohen, L.G.; Duque, J.; Mazzocchio, R.; Celnik, P.; Sawaki, L.; Ungerleider, L.; Classen, J. Formation of a motor memory by action observation. J. Neurosci. Off. J. Soc. Neurosci. 2005, 25, 9339–9346. [Google Scholar] [CrossRef] [PubMed]
- Porro, C.A.; Facchin, P.; Fusi, S.; Dri, G.; Fadiga, L. Enhancement of force after action observation: Behavioural and neurophysiological studies. Neuropsychologia 2007, 45, 3114–3121. [Google Scholar] [CrossRef] [PubMed]
- Gatti, R.; Tettamanti, A.; Gough, P.M.; Riboldi, E.; Marinoni, L.; Buccino, G. Action observation versus motor imagery in learning a complex motor task: A short review of literature and a kinematics study. Neurosci. Lett. 2013, 540, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Bassolino, M.; Campanella, M.; Bove, M.; Pozzo, T.; Fadiga, L. Training the motor cortex by observing the actions of others during immobilization. Cereb. Cortex 2014, 24, 3268–3276. [Google Scholar] [CrossRef]
- Buccino, G. Action observation treatment: A novel tool in neurorehabilitation. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 2014, 369, 20130185. [Google Scholar] [CrossRef]
- Caggiano, V.; Fogassi, L.; Rizzolatti, G.; Pomper, J.K.; Thier, P.; Giese, M.A.; Casile, A. View-based encoding of actions in mirror neurons of area f5 in macaque premotor cortex. Curr. Biol. CB 2011, 21, 144–148. [Google Scholar] [CrossRef] [Green Version]
- Scott, M.W.; Wood, G.; Holmes, P.S.; Williams, J.; Marshall, B.; Wright, D.J. Combined action observation and motor imagery: An intervention to combat the neural and behavioural deficits associated with developmental coordination disorder. Neurosci. Biobehav. Rev. 2021, 127, 638–646. [Google Scholar] [CrossRef]
- Gibson, J.J. The Theory of Affordances. In Perceiving, Acting, and Knowing: Toward an Ecological Psychology; Robert E Shaw, J.B., Ed.; Lawrence Erlbaum Associates: Hillsdale, MI, USA , 1977; pp. 67–82. [Google Scholar]
- Grafton, S.T.; Fadiga, L.; Arbib, M.A.; Rizzolatti, G. Premotor cortex activation during observation and naming of familiar tools. NeuroImage 1997, 6, 231–236. [Google Scholar] [CrossRef] [Green Version]
- Grèzes, J.; Tucker, M.; Armony, J.; Ellis, R.; Passingham, R.E. Objects automatically potentiate action: An fMRI study of implicit processing. Eur. J. Neurosci. 2003, 17, 2735–2740. [Google Scholar] [CrossRef]
- Buccino, G.; Sato, M.; Cattaneo, L.; Rodà, F.; Riggio, L. Broken affordances, broken objects: A TMS study. Neuropsychologia 2009, 47, 3074–3078. [Google Scholar] [CrossRef]
- Ryan, D.; Fullen, B.; Rio, E.; Segurado, R.; Stokes, D.; O’Sullivan, C. Effect of Action Observation Therapy in the Rehabilitation of Neurologic and Musculoskeletal Conditions: A Systematic Review. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100106. [Google Scholar] [CrossRef]
- Ertelt, D.; Small, S.; Solodkin, A.; Dettmers, C.; McNamara, A.; Binkofski, F.; Buccino, G. Action observation has a positive impact on rehabilitation of motor deficits after stroke. NeuroImage 2007, 36 (Suppl. 2), T164–T173. [Google Scholar] [CrossRef]
- Buccino, G.; Gatti, R.; Giusti, M.C.; Negrotti, A.; Rossi, A.; Calzetti, S.; Cappa, S.F. Action observation treatment improves autonomy in daily activities in Parkinson’s disease patients: Results from a pilot study. Mov. Disord. Off. J. Mov. Disord. Soc. 2011, 26, 1963–1964. [Google Scholar] [CrossRef]
- Pelosin, E.; Avanzino, L.; Bove, M.; Stramesi, P.; Nieuwboer, A.; Abbruzzese, G. Action observation improves freezing of gait in patients with Parkinson’s disease. Neurorehabil. Neural Repair 2010, 24, 746–752. [Google Scholar] [CrossRef]
- Doyon, J.; Bellec, P.; Amsel, R.; Penhune, V.; Monchi, O.; Carrier, J.; Lehéricy, S.; Benali, H. Contributions of the basal ganglia and functionally related brain structures to motor learning. Behav. Brain Res. 2009, 199, 61–75. [Google Scholar] [CrossRef]
- Obeso, J.A.; Rodríguez-Oroz, M.C.; Benitez-Temino, B.; Blesa, F.J.; Guridi, J.; Marin, C.; Rodriguez, M. Functional organization of the basal ganglia: Therapeutic implications for Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2008, 23 (Suppl. 3), S548–S559. [Google Scholar] [CrossRef]
- Alegre, M.; Rodríguez-Oroz, M.C.; Valencia, M.; Pérez-Alcázar, M.; Guridi, J.; Iriarte, J.; Obeso, J.A.; Artieda, J. Changes in subthalamic activity during movement observation in Parkinson’s disease: Is the mirror system mirrored in the basal ganglia. Clin. Neurophysiol. 2010, 121, 414–425. [Google Scholar] [CrossRef]
- Jahanshahi, M.; Jenkins, I.H.; Brown, R.G.; Marsden, C.D.; Passingham, R.E.; Brooks, D.J. Self-initiated versus externally triggered movements. I. An investigation using measurement of regional cerebral blood flow with PET and movement-related potentials in normal and Parkinson’s disease subjects. Brain J. Neurol. 1995, 118 Pt 4, 913–933. [Google Scholar] [CrossRef]
- Rowe, J.; Stephan, K.E.; Friston, K.; Frackowiak, R.; Lees, A.; Passingham, R. Attention to action in Parkinson’s disease: Impaired effective connectivity among frontal cortical regions. Brain J. Neurol. 2002, 125, 276–289. [Google Scholar] [CrossRef] [Green Version]
- Buccino, G.; Arisi, D.; Gough, P.; Aprile, D.; Ferri, C.; Serotti, L.; Tiberti, A.; Fazzi, E. Improving upper limb motor functions through action observation treatment: A pilot study in children with cerebral palsy. Dev. Med. Child Neurol. 2012, 54, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Sgandurra, G.; Ferrari, A.; Cossu, G.; Guzzetta, A.; Fogassi, L.; Cioni, G. Randomized Trial of Observation and Execution of Upper Extremity Actions Versus Action Alone in Children With Unilateral Cerebral Palsy. Neurorehabil. Neural Repair 2013, 27, 808–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.-Y.; Kim, J.-M.; Ko, E.-Y. The effect of the action observation physical training on the upper extremity function in children with cerebral palsy. J. Exerc. Rehabil. 2014, 10, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Buccino, G.; Molinaro, A.; Ambrosi, C.; Arisi, D.; Mascaro, L.; Pinardi, C.; Rossi, A.; Gasparotti, R.; Fazzi, E.; Galli, J. Action Observation Treatment Improves Upper Limb Motor Functions in Children with Cerebral Palsy: A Combined Clinical and Brain Imaging Study. Neural Plast. 2018, 2018, 4843985. [Google Scholar] [CrossRef]
- Bellelli, G.; Buccino, G.; Bernardini, B.; Padovani, A.; Trabucchi, M. Action observation treatment improves recovery of postsurgical orthopedic patients: Evidence for a top-down effect? Arch. Phys. Med. Rehabil. 2010, 91, 1489–1494. [Google Scholar] [CrossRef]
- Marangolo, P.; Bonifazi, S.; Tomaiuolo, F.; Craighero, L.; Coccia, M.; Altoè, G.; Provinciali, L.; Cantagallo, A. Improving language without words: First evidence from aphasia. Neuropsychologia 2010, 48, 3824–3833. [Google Scholar] [CrossRef]
- Chen, J.; Jin, W.; Zhang, X.X.; Xu, W.; Liu, X.N.; Ren, C.C. Telerehabilitation Approaches for Stroke Patients: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Stroke Cerebrovasc. Dis. 2015, 24, 2660–2668. [Google Scholar] [CrossRef]
- Sarfo, F.S.; Ulasavets, U.; Opare-Sem, O.K.; Ovbiagele, B. Tele-Rehabilitation after Stroke: An Updated Systematic Review of the Literature. J. Stroke Cerebrovasc. Dis. 2018, 27, 2306–2318. [Google Scholar] [CrossRef]
- Laver, K.E.; Adey-Wakeling, Z.; Crotty, M.; Lannin, N.A.; George, S.; Sherrington, C. Telerehabilitation services for stroke. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Khan, F.; Amatya, B.; Kesselring, J.; Galea, M. Telerehabilitation for persons with multiple sclerosis. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Cox, N.S.; Corso, S.D.; Hansen, H.; McDonald, C.F.; Hill, C.J.; Zanaboni, P.; Alison, J.A.; O’Halloran, P.; Macdonald, H.; Holland, A.E. Telerehabilitation for chronic respiratory disease. Cochrane Database Syst. Rev. 2021. [Google Scholar] [CrossRef]
- Nuara, A.; Avanzini, P.; Rizzolatti, G.; Fabbri-Destro, M. Efficacy of a home-based platform for child-to-child interaction on hand motor function in unilateral cerebral palsy. Dev. Med. Child Neurol. 2019, 61, 1314–1322. [Google Scholar] [CrossRef]
- Molinaro, A.; Micheletti, S.; Pagani, F.; Garofalo, G.; Galli, J.; Rossi, A.; Fazzi, E.; Buccino, G. Action Observation Treatment in a tele-rehabilitation setting: A pilot study in children with cerebral palsy. Disabil. Rehabil. 2020, 1–6. [Google Scholar] [CrossRef]
- LYNCH, C.L.; POPOVIC, M.R. Functional Electrical Stimulation. IEEE Control Syst. Mag. 2008, 28, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Marquez-Chin, C.; Popovic, M.R. Functional electrical stimulation therapy for restoration of motor function after spinal cord injury and stroke: A review. Biomed. Eng. OnLine 2020, 19, 34. [Google Scholar] [CrossRef]
- Kapadia, N.; Moineau, B.; Popovic, M.R. Functional Electrical Stimulation Therapy for Retraining Reaching and Grasping After Spinal Cord Injury and Stroke. Front. Neurosci. 2020, 14, 718. [Google Scholar] [CrossRef]
- Eraifej, J.; Clark, W.; France, B.; Desando, S.; Moore, D. Effectiveness of upper limb functional electrical stimulation after stroke for the improvement of activities of daily living and motor function: A systematic review and meta-analysis. Syst. Rev. 2017, 6, 40. [Google Scholar] [CrossRef] [Green Version]
- Jiang, S.; Chen, L.; Wang, Z.; Xu, J.; Qi, C.; Qi, H.; He, F.; Ming, D. Application of BCI-FES system on stroke rehabilitation. In Proceedings of the 2015 7th International IEEE/EMBS Conference on Neural Engineering (NER), Montpellier, France, 22–24 April 2015; pp. 1112–1115. [Google Scholar]
- Broniera Junior, P.; Campos, D.P.; Lazzaretti, A.E.; Nohama, P.; Carvalho, A.A.; Krueger, E.; Minhoto Teixeira, M.C. EEG-FES-Force-MMG closed-loop control systems of a volunteer with paraplegia considering motor imagery with fatigue recognition and automatic shut-off. Biomed. Signal Process. Control 2021, 68, 102662. [Google Scholar] [CrossRef]
- Rossi, F.; Motto Ros, P.; Rosales, R.M.; Demarchi, D. Embedded Bio-Mimetic System for Functional Electrical Stimulation Controlled by Event-Driven sEMG. Sensors 2020, 20, 1535. [Google Scholar] [CrossRef] [Green Version]
- Kuk, E.-J.; Kim, J.-M.; Oh, D.-W.; Hwang, H.-J. Effects of action observation therapy on hand dexterity and EEG-based cortical activation patterns in patients with post-stroke hemiparesis. Top. Stroke Rehabil. 2016, 23, 318–325. [Google Scholar] [CrossRef]
- Kim, S.-H.; Cho, J.-S. Action Observation and Cortical Connectivity: Evidence from EEG Analysis. J. Korean Phys. Ther. 2016, 28, 398–407. [Google Scholar] [CrossRef] [Green Version]
- Ge, S.; Wang, P.; Liu, H.; Lin, P.; Gao, J.; Wang, R.; Iramina, K.; Zhang, Q.; Zheng, W. Neural Activity and Decoding of Action Observation Using Combined EEG and fNIRS Measurement. Front. Hum. Neurosci. 2019, 13, 357. [Google Scholar] [CrossRef] [Green Version]
- Marquez-Chin, C.; Marquis, A.; Popovic, M.R. EEG-Triggered Functional Electrical Stimulation Therapy for Restoring Upper Limb Function in Chronic Stroke with Severe Hemiplegia. Case Rep. Neurol. Med. 2016, 2016, e9146213. [Google Scholar] [CrossRef] [Green Version]
- Likitlersuang, J.; Koh, R.; Gong, X.; Jovanovic, L.; Bolivar-Tellería, I.; Myers, M.; Zariffa, J.; Márquez-Chin, C. EEG-Controlled Functional Electrical Stimulation Therapy With Automated Grasp Selection: A Proof-of-Concept Study. Top. Spinal Cord Inj. Rehabil. 2018, 24, 265–274. [Google Scholar] [CrossRef]
- Fumanal-Idocin, J.; Wang, Y.-K.; Lin, C.-T.; Fernández, J.; Sanz, J.A.; Bustince, H. Motor-Imagery-Based Brain Computer Interface using Signal Derivation and Aggregation Functions. IEEE Trans. Cybern. 2021, 1–12. [Google Scholar] [CrossRef]
- Lotze, M.; Halsband, U. Motor imagery. J. Physiol. Paris 2006, 99, 386–395. [Google Scholar] [CrossRef]
- Chaisaen, R.; Autthasan, P.; Mingchinda, N.; Leelaarporn, P.; Kunaseth, N.; Tammajarung, S.; Manoonpong, P.; Mukhopadhyay, S.C.; Wilaiprasitporn, T. Decoding EEG Rhythms During Action Observation, Motor Imagery, and Execution for Standing and Sitting. IEEE Sens. J. 2020, 20, 13776–13786. [Google Scholar] [CrossRef]
- Alimardani, M.; Nishio, S.; Ishiguro, H. Brain-Computer Interface and Motor Imagery Training: The Role of Visual Feedback and Embodiment; IntechOpen: London, UK, 2018; ISBN 978-1-78984-070-4. [Google Scholar]
- Ruiz-Olaya, A.F.; Antelis, J.M.; Cerquera, A. Decoding Steady-State Visual Evoked Potentials From EEG Signals: Towards an EEG-Triggered FES System to Restore Hand Grasp Function. In Proceedings of the 2019 IEEE 10th Annual Ubiquitous Computing, Electronics Mobile Communication Conference (UEMCON), New York, NY, USA, 10–12 October 2019; pp. 1152–1157. [Google Scholar]
- McGie, S.C.; Zariffa, J.; Popovic, M.R.; Nagai, M.K. Short-term neuroplastic effects of brain-controlled and muscle-controlled electrical stimulation. Neuromodulation Technol. Neural Interface 2015, 18, 233–240, discussion 240. [Google Scholar] [CrossRef]
- Biasiucci, A.; Leeb, R.; Iturrate, I.; Perdikis, S.; Al-Khodairy, A.; Corbet, T.; Schnider, A.; Schmidlin, T.; Zhang, H.; Bassolino, M.; et al. Brain-actuated functional electrical stimulation elicits lasting arm motor recovery after stroke. Nat. Commun. 2018, 9, 2421. [Google Scholar] [CrossRef]
- Padfield, N.; Zabalza, J.; Zhao, H.; Masero, V.; Ren, J. EEG-Based Brain-Computer Interfaces Using Motor-Imagery: Techniques and Challenges. Sensors 2019, 19, 1423. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; McIntosh, J.; Shadli, S.M.; Neo, P.S.-H.; Huang, Z.; McNaughton, N. Removing eye blink artefacts from EEG—A single-channel physiology-based method. J. Neurosci. Methods 2017, 291, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Bian, G.-B.; Tian, Z. Removal of Artifacts from EEG Signals: A Review. Sensors 2019, 19, 987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gant, K.; Guerra, S.; Zimmerman, L.; Parks, B.A.; Prins, N.W.; Prasad, A. EEG-controlled functional electrical stimulation for hand opening and closing in chronic complete cervical spinal cord injury. Biomed. Phys. Eng. Express 2018, 4, 065005. [Google Scholar] [CrossRef]
- De Luca, C.J. Surface Electromyography: Detection and Recording. Available online: https://www.delsys.com/downloads/TUTORIAL/semg-detection-and-recording.pdf (accessed on 30 November 2021).
- De Luca, G. Fundamental Concepts in EMG Signal Acquisition. Available online: https://www.delsys.com/downloads/TUTORIAL/fundamental-concepts-in-emg-signal-acquisition.pdf (accessed on 30 November 2021).
- Prakash, A.; Kumari, B.; Sharma, S. A low-cost, wearable sEMG sensor for upper limb prosthetic application. J. Med. Eng. Technol. 2019, 43, 235–247. [Google Scholar] [CrossRef]
- Liang, S.; Wu, Y.; Chen, J.; Zhang, L.; Chen, P.; Chai, Z.; Cao, C. Identification of Gesture Based on Combination of Raw sEMG and sEMG Envelope Using Supervised Learning and Univariate Feature Selection. J. Bionic Eng. 2019, 16, 647–662. [Google Scholar] [CrossRef]
- Sapienza, S.; Crepaldi, M.; Motto Ros, P.; Bonanno, A.; Demarchi, D. On Integration and Validation of a Very Low Complexity ATC UWB System for Muscle Force Transmission. IEEE Trans. Biomed. Circuits Syst. 2016, 10, 497–506. [Google Scholar] [CrossRef]
- Rossi, F.; Motto Ros, P.; Sapienza, S.; Bonato, P.; Bizzi, E.; Demarchi, D. Wireless Low Energy System Architecture for Event-Driven Surface Electromyography. In Applications in Electronics Pervading Industry, Environment and Society; Saponara, S., De Gloria, A., Eds.; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Mongardi, A.; Motto Ros, P.; Rossi, F.; Ruo Roch, M.; Martina, M.; Demarchi, D. A Low-Power Embedded System for Real-Time sEMG based Event-Driven Gesture Recognition. In Proceedings of the 2019 26th IEEE International Conference on Electronics, Circuits and Systems (ICECS); Genova, Italy, 27–29 November 2019; pp. 65–68. [Google Scholar]
- Masani, K.; Popovic, M.R. Functional Electrical Stimulation in Rehabilitation and Neurorehabilitation. In Springer Handbook of Medical Technology; Kramme, R., Hoffmann, K.-P., Pozos, R.S., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 877–896. ISBN 978-3-540-74658-4. [Google Scholar]
- Henneman, E. Relation between size of neurons and their susceptibility to discharge. Science 1957, 126, 1345–1347. [Google Scholar] [CrossRef]
- De Luca, C.J. The Use of Surface Electromyography in Biomechanics. J. Appl. Biomech. 1997, 13, 135–163. [Google Scholar] [CrossRef] [Green Version]
- Schauer, T.; Vrontos, A. Modeling of Mixed Artificially and Voluntary Induced Muscle Contractions for Controlled Functional Electrical Stimulation of Shoulder Abduction. IFAC-Pap. 2019, 51, 284–289. [Google Scholar] [CrossRef]
- Li, Y.; Chen, J.; Yang, Y. A Method for Suppressing Electrical Stimulation Artifacts from Electromyography. Int. J. Neural Syst. 2019, 29, 1850054. [Google Scholar] [CrossRef]
- de Sousa, A.C.C.; Valtin, M.; Bó, A.P.L.; Schauer, T. Automatic Detection of Stimulation Artifacts to Isolate Volitional from Evoked EMG Activity. IFAC-PapersOnLine 2018, 51, 282–287. [Google Scholar] [CrossRef]
- Li, Z.; Guiraud, D.; Andreu, D.; Gelis, A.; Fattal, C.; Hayashibe, M. Real-Time Closed-Loop Functional Electrical Stimulation Control of Muscle Activation with Evoked Electromyography Feedback for Spinal Cord Injured Patients. Int. J. Neural Syst. 2018, 28, 1750063. [Google Scholar] [CrossRef]
- Bi, Z.-Y.; Xie, C.-X.; Zhou, Y.-X.; Wang, H.-P.; Lu, X.-Y.; Wang, Z.-G. An Anti Stimulation Artifacts and M-waves Surface Electromyography Detector with a Short Blanking Time. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020. [Google Scholar] [CrossRef]
- Sa-E, S.; Freeman, C.; Yang, K. Model-Based Control of FES Embedding Simultaneous Volitional EMG Measurement; IEEE: Piscataway, NJ, USA, 2018; pp. 480–485. [Google Scholar]
- Pérez, R.; Costa, Ú.; Torrent, M.; Solana, J.; Opisso, E.; Cáceres, C.; Tormos, J.M.; Medina, J.; Gómez, E.J. Upper limb portable motion analysis system based on inertial technology for neurorehabilitation purposes. Sensors 2010, 10, 10733–10751. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Liu, X.; Gummeson, J.; Lee, S. A Wearable RFID System to Monitor Hand Use for Individuals with Upper Limb Paresis. In Proceedings of the 2019 IEEE 16th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Chicago, IL, USA, 19-22 May 2019. [Google Scholar] [CrossRef]
- Kang, M.; Kim, J.; Jang, B.; Chae, Y.; Kim, J.-H.; Ahn, J.-H. Graphene-Based Three-Dimensional Capacitive Touch Sensor for Wearable Electronics. ACS Nano 2017, 11, 7950–7957. [Google Scholar] [CrossRef]
- Varga, V.; Vakulya, G.; Sample, A.; Gross, T. Enabling Interactive Infrastructure with Body Channel Communication. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2017, 1, 169. [Google Scholar] [CrossRef]
- Crepaldi, M.; Barcellona, A.; Zini, G.; Ansaldo, A.; Motto Ros, P.; Sanginario, A.; Cuccu, C.; De Marchi, D.; Brayda, L. Live Wire—A Low-Complexity Body Channel Communication System for Landmark Identification. IEEE Trans. Emerg. Top. Comput. 2020, 9, 1248–1264. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, F.; Savi, F.; Prestia, A.; Mongardi, A.; Demarchi, D.; Buccino, G. Combining Action Observation Treatment with a Brain–Computer Interface System: Perspectives on Neurorehabilitation. Sensors 2021, 21, 8504. https://doi.org/10.3390/s21248504
Rossi F, Savi F, Prestia A, Mongardi A, Demarchi D, Buccino G. Combining Action Observation Treatment with a Brain–Computer Interface System: Perspectives on Neurorehabilitation. Sensors. 2021; 21(24):8504. https://doi.org/10.3390/s21248504
Chicago/Turabian StyleRossi, Fabio, Federica Savi, Andrea Prestia, Andrea Mongardi, Danilo Demarchi, and Giovanni Buccino. 2021. "Combining Action Observation Treatment with a Brain–Computer Interface System: Perspectives on Neurorehabilitation" Sensors 21, no. 24: 8504. https://doi.org/10.3390/s21248504