
Sagittal and Vertical Growth of the Maxillo–Mandibular Complex in Untreated Children: A Longitudinal Study on Lateral Cephalograms Derived from Cone Beam Computed Tomography


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Orientation
- Roll: The cranium was oriented such that a midline could be drawn through the midpoint of the frontonasal suture and the base of the nose, and was parallel to the true vertical, which is perpendicular to a true horizontal line (Figure 1A). A true horizontal line goes through the most inferior aspect of the orbits;
- Yaw: The cranium was oriented to achieve the best symmetry of the cranial base, zygomatic, and maxillary structures on either side of the midline (Figure 1A);
- Pitch: The cranium was oriented such that the Frankfurt horizontal plane was parallel to the true horizontal plane (Figure 1B).
2.3. Lateral Cephalograms Superimpositions and Construction of the “Core Lines”
2.4. Linear and Angular Measurements
- Nasion (N): the most anterior point of the frontonasal suture;
- Orbitale (Or): the most inferior point of the orbital rim;
- Porion (Po): the most superior point of the external auditory meatus;
- Condylion (Co): the midpoint between the most posterior and superior points of the condyle;
- Gonion (Go): the midpoint between the best fit lines tangent to the posterior and the inferior border of the mandible;
- Gnathion (Gn): the midpoint between the most anterior and inferior points of the symphysis;
- A-point (A): the most concave point along the maxillary dentoalveolus between the anterior nasal spine and the crestal bone;
- B-point (B): the most concave point along the mandibular dentoalveolus between the crestal bone and the pogonion;
- Maxillary first molar (U6): the furcation between the mesiobuccal and distobuccal roots of the maxillary first molar;
- Maxillary central incisor (U1): the incisal edge of the maxillary central incisor;
- Mandibular first molar (L6): the furcation of the mandibular first molar roots;
- Mandibular central incisor (L1): the incisal edge of the mandibular central incisor.
- SN: the millimeter distance between the sella and the nasion, representing the length of the anterior cranial base;
- Co-Gn: the millimeter distance between the condylion and the gnathion, representing the mandibular length;
- SNA: the angle between a line through the sella to the nasion and a line through the nasion to the A point;
- SNB: the angle between a line through the sella to the nasion and a line through the nasion to the B point;
- ANB: SNA minus SNB, representing the maxilla–mandibular sagittal relationship;
- SN-GoGn: the angle between a line through the sella to the nasion, and a line through the gonion and the gnathion;
- CB line-A: the angle between the cranial base core line and a line through the CB core point (anterior point of the CB core line) and the A point, representing the maxillary sagittal position relative to the cranial base, instead of the SN, and eliminating the influence of the remodeling of the nasion (Figure 3A);
- CB line-B: the angle between the cranial base core line and a line through the CB core point (anterior point of the CB core line) and the B point, representing the mandibular sagittal position relative to the cranial base, instead of the SN, and eliminating the influence of the remodeling of the nasion (Figure 3A);
- A-CB point-B: the difference between CB line-A and CB line-B, representing the maxilla–mandibular sagittal relationship. It is analogous to the ANB, but uses the CB point instead of the nasion, eliminating the influence of the remodeling of the nasion (Figure 3A);
- CB line-GoGn: the angle between the cranial base core line and a line through the gonion and the gnathion. The T2–T1 difference represents the mandibular plane rotation relative to the cranial base (Figure 3B);
- CB line-Mx point: the angle between the cranial base core line and a line through the cranial base and the maxillary core points. The cranial base core point is the anterior point of the cranial base core line. The maxillary core point is the anterior point of the maxillary core line. The T2–T1 difference represents the changes in the maxillary sagittal position (Figure 3C);
- CB line-Md point: the angle between the cranial base core line and a line through the cranial base and the mandibular core points. The mandibular core point is the anterior point of the mandibular core line. The T2–T1 difference represents the changes in the mandibular sagittal position (Figure 3C);
- Mx point-CB line-Md point: the difference between the CB line-Mx point and the CB line-Md point, representing the maxillomandibular relationship (Figure 3C);
- CB line-Mx line: the angle between the cranial base core line and the maxillary core line. The T2–T1 difference represents the maxillary rotation relative to the cranial base (Figure 3D);
- CB line-Md line: the angle between the cranial base core line and the mandibular core line. The T2–T1 difference represents the true mandibular rotation relative to the cranial base (Figure 3D);
- Co-Md line: the angle between the mandibular core line and a line through the posterior end of the mandibular core line and the condylion. The T2–T1 difference represents the direction of the condylar growth relative to the mandibular body (Figure 3E);
- Md line-Md Border: the angle between the mandibular core line and the best fit line to the inferior border of the mandible. The T2–T1 difference represents the degree of remodeling that occurs on the mandibular inferior border (Figure 3F);
- Gonial angle: the angle formed by the junction at the gonion of the posterior border of the ramus and the inferior border of the body of the mandibles.
2.5. Statistical Analysis
3. Results
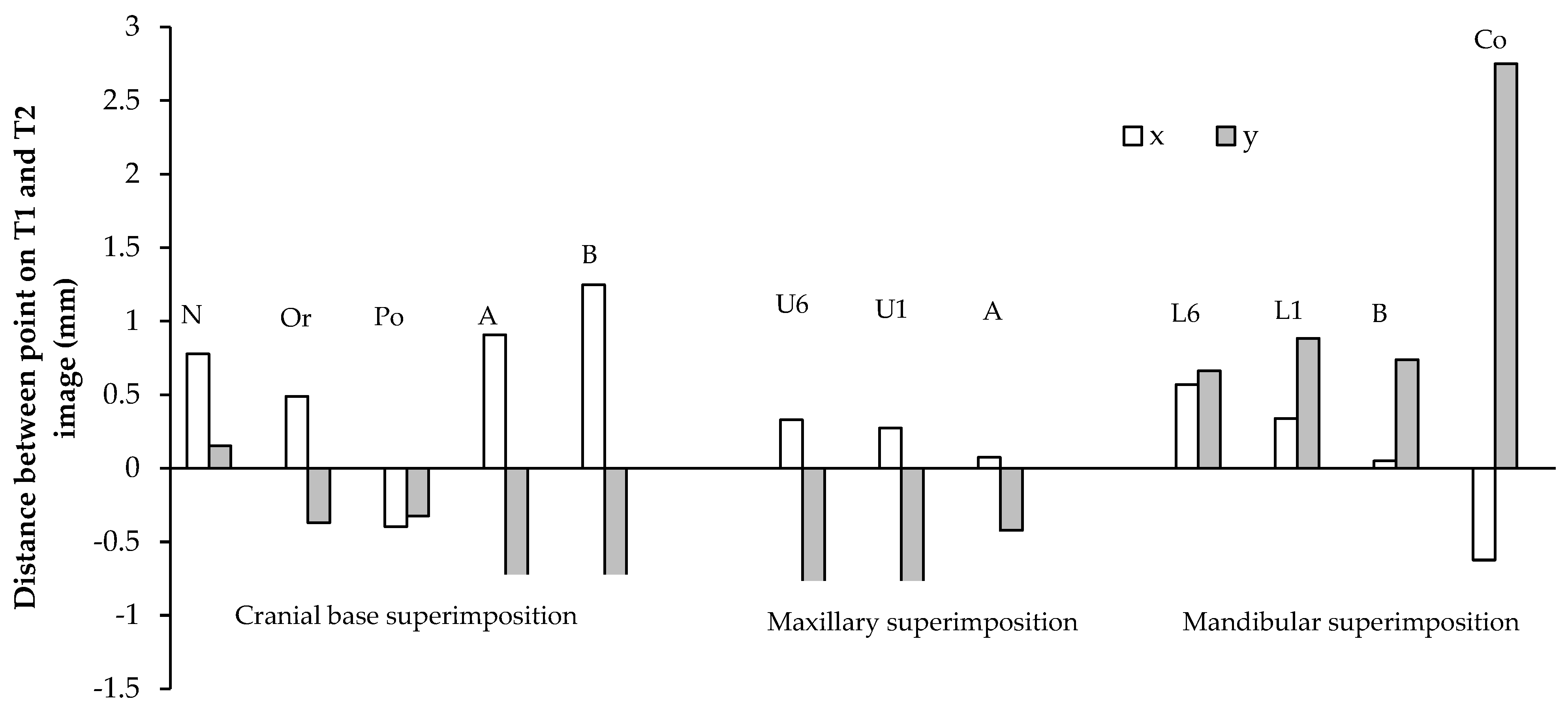
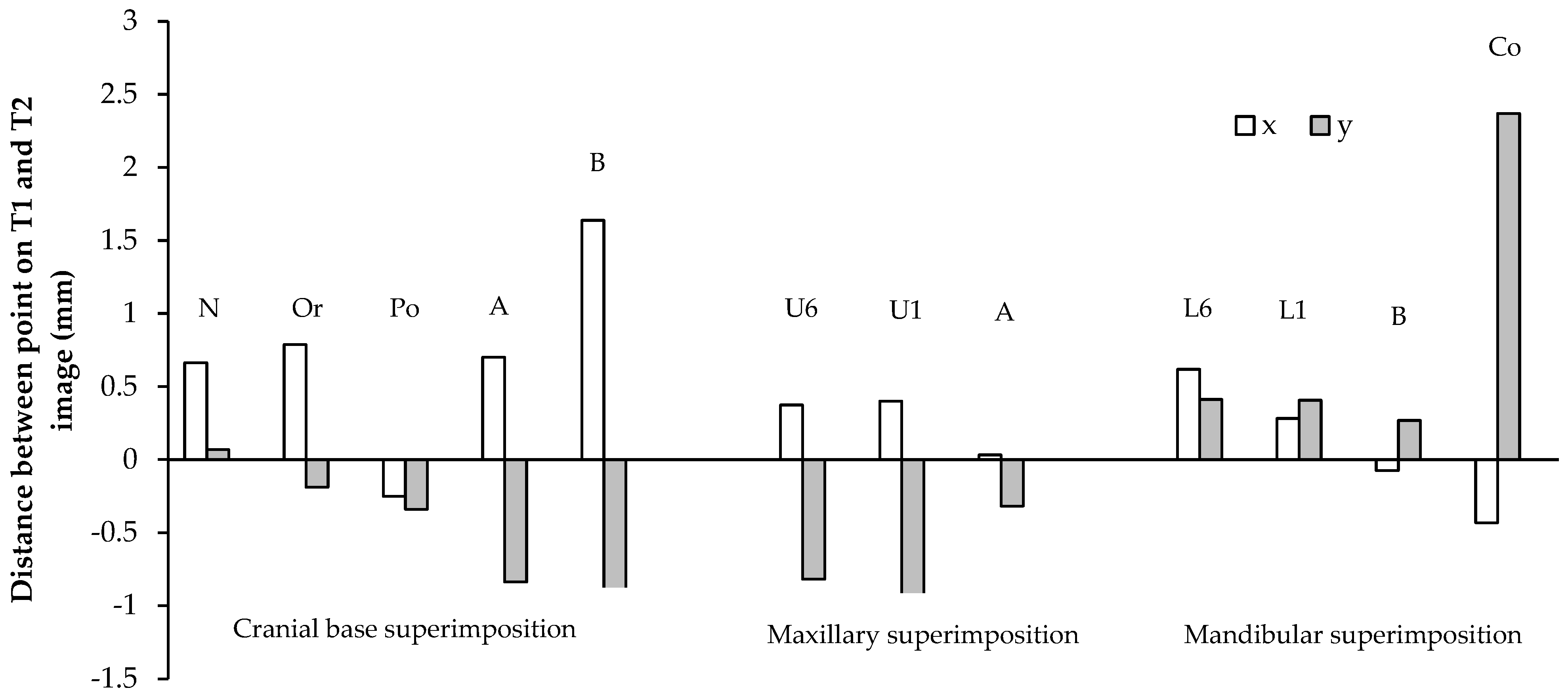
3.1. Cephalometric Point Distance
3.2. Linear and Angular Changes
3.3. Intraexaminer Reliability
4. Discussion
5. Conclusions
- On a cranial base superimposition, the orbitale, the A-point, and the B-point moved anteriorly and inferiorly. The porion moved posteriorly and inferiorly. The nasion moved inferiorly, and showed a large variation in vertical displacement. The SN and Frankfurt horizontal planes might not be reliable as the reference planes for the longitudinal evaluation of growth;
- The A-point displayed the inferior movement that is only statistically significant in males, and variable sagittal movement on a maxillary superimposition. The B-point displayed the superior movement that was only statistically significant in males, and variable sagittal movement on a mandibular superimposition. Sagittally, the anterior surfaces of the maxillary and mandibular corpora were stable;
- Most subjects displayed the forward rotation of the jaws and correlated processes, such as the forward growth of the condyle, the compensatory remodeling of the inferior mandibular border, and the reduction in the gonial angle. These correlated processes occured in the opposite direction for the individual who had backward rotation of the jaws;
- Males had greater increases in the mandibular length than females. Increases in the mandibular length and the vertical growth of the condyle were correlated with vertical dentoalveolar eruption;
- The maxillary and mandibular molars and incisors erupted at similar rates. The maxillary molars erupted more than the mandibular molars. The mandibular molar mesialized more than the maxillary molar because of the greater leeway space. The maxillary and mandibular incisors proclined only slightly on maxillary and mandibular superimpositions, respectively;
- Our limitations of this study are the inclusion of multiple facial types and a small sample size. Future studies with a larger sample size would be beneficial in order to examine the differential growth patterns according to different face types.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bjork, A.; Skieller, V. Facial development and tooth eruption. An implant study at the age of puberty. Am. J. Orthod. 1972, 62, 339–383. [Google Scholar] [CrossRef]
- Bjork, A.; Skieller, V. Growth of the maxilla in three dimensions as revealed radiographically by the implant method. Br. J. Orthod. 1977, 4, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Bjork, A.; Skieller, V. Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur. J. Orthod. 1983, 5, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.H. The cranial base. Am. J. Phys. Anthropol. 1958, 16, 319–348. [Google Scholar] [CrossRef]
- Steuer, I. The cranial base for superimposition of lateral cephalometric radiographs. Am. J. Orthod. 1972, 61, 493–500. [Google Scholar] [CrossRef]
- Melsen, B. The Cranial Base: The Postnatal Development of the Cranial Base Studied Histologically on Human Autopsy Material; Arhus: Aarhus, Denmark, 1974; Volume 66. [Google Scholar]
- Afrand, M.; Ling, C.P.; Khosrotehrani, S.; Flores-Mir, C.; Lagravere-Vich, M.O. Anterior cranial-base time-related changes: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 21–32. [Google Scholar] [CrossRef]
- Afrand, M.; Oh, H.; Flores-Mir, C.; Lagravere-Vich, M.O. Growth changes in the anterior and middle cranial bases assessed with cone-beam computed tomography in adolescents. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 342–350. [Google Scholar] [CrossRef]
- Buschang, P.H.; Martins, J. Childhood and adolescent changes of skeletal relationships. Angle Orthod. 1998, 68, 199–206, discussion 207–198. [Google Scholar] [CrossRef]
- Nielsen, I.L. Maxillary superimposition: A comparison of three methods for cephalometric evaluation of growth and treatment change. Am. J. Orthod. Dentofac. Orthop. 1989, 95, 422–431. [Google Scholar] [CrossRef]
- Doppel, D.M.; Damon, W.M.; Joondeph, D.R.; Little, R.M. An investigation of maxillary superimposition techniques using metallic implants. Am. J. Orthod. Dentofac. Orthop. 1994, 105, 161–168. [Google Scholar] [CrossRef]
- Ruellas, A.C.; Ghislanzoni, L.T.H.; Gomes, M.R.; Danesi, C.; Lione, R.; Nguyen, T.; McNamara, J.A., Jr.; Cozza, P.; Franchi, L.; Cevidanes, L.H. Comparison and reproducibility of 2 regions of reference for maxillary regional registration with cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 533–542. [Google Scholar] [CrossRef] [Green Version]
- Springate, S.D.; Jones, A.G. The validity of two methods of mandibular superimposition: A comparison with tantalum implants. Am. J. Orthod. Dentofac. Orthop. 1998, 113, 263–270. [Google Scholar] [CrossRef]
- Krarup, S.; Darvann, T.A.; Larsen, P.; Marsh, J.L.; Kreiborg, S. Three-dimensional analysis of mandibular growth and tooth eruption. J. Anat. 2005, 207, 669–682. [Google Scholar] [CrossRef]
- Buschang, P.H.; LaPalme, L.; Tanguay, R.; Demirjian, A. The technical reliability of superimposition on cranial base and mandibular structures. Eur. J. Orthod. 1986, 8, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Araujo, A.M.; Buschang, P.H.; Melo, A.C. Adaptive condylar growth and mandibular remodelling changes with bionator therapy—An implant study. Eur. J. Orthod. 2004, 26, 515–522. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.K.; Buschang, P.H.; Behrents, R. Mandibular rotation and remodeling changes during early childhood. Angle Orthod. 2009, 79, 271–275. [Google Scholar] [CrossRef]
- Ueno, H.; Behrents, R.G.; Oliver, D.R.; Buschang, P.H. Mandibular rotation during the transitional dentition. Angle Orthod. 2013, 83, 29–35. [Google Scholar] [CrossRef]
- West, K.S.; McNamara, J.A., Jr. Changes in the craniofacial complex from adolescence to midadulthood: A cephalometric study. Am. J. Orthod. Dentofac. Orthop. 1999, 115, 521–532. [Google Scholar] [CrossRef]
- Buschang, P.H.; Santos-Pinto, A. Condylar growth and glenoid fossa displacement during childhood and adolescence. Am. J. Orthod. Dentofac. Orthop. 1998, 113, 437–442. [Google Scholar] [CrossRef]
- Baumrind, S.; Ben-Bassat, Y.; Korn, E.L.; Bravo, L.A.; Curry, S. Mandibular remodeling measured on cephalograms. 1. Osseous changes relative to superimposition on metallic implants. Am. J. Orthod. Dentofac. Orthop. 1992, 102, 134–142. [Google Scholar] [CrossRef]
- Kumar, V.; Ludlow, J.B.; Mol, A.; Cevidanes, L. Comparison of conventional and cone beam CT synthesized cephalograms. Dentomaxillofac. Radiol. 2007, 36, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Lamichane, M.; Anderson, N.K.; Rigali, P.H.; Seldin, E.B.; Will, L.A. Accuracy of reconstructed images from cone-beam computed tomography scans. Am. J. Orthod. Dentofac. Orthop. 2009, 136, e151–e156, discussion 156–157. [Google Scholar] [CrossRef]
- Habeeb, M.; Boucher, N.; Chung, C.H. Effects of rapid palatal expansion on the sagittal and vertical dimensions of the maxilla: A study on cephalograms derived from cone-beam co.omputed tomography. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Yi, L.; Jeon, H.H.; Li, C.; Boucher, N.; Chung, C.H. Transverse Growth of the Maxillo-Mandibular Complex in Untreated Children: A Longitudinal Cone Beam Computed Tomography Study. Sensors 2021, 21, 6378. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.S.; Chung, C.H. Comparison of craniofacial growth of untreated Class I and Class II girls from ages 9 to 18 years: A longitudinal study. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.H.; Wong, W.W. Craniofacial growth in untreated skeletal Class II subjects: A longitudinal study. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 619–626. [Google Scholar] [CrossRef]
- English, J.D.; Akyalcin, S.; Peltomaki, T.; Litschel, K. Mosby’s Orthodontic Review, 2nd ed.; Mosby: Maryland Heights, MO, USA, 2014. [Google Scholar]
- Knott, V.B. Change in cranial base measures of human males and females from age 6 years to early adulthood. Growth 1971, 35, 145–158. [Google Scholar]
- Ranly, D.M. Craniofacial growth. Dent. Clin. North. Am. 2000, 44, 457–470. [Google Scholar]
- Baumrind, S.; Korn, E.L.; Isaacson, R.J.; West, E.E.; Molthen, R. Superimpositional assessment of treatment-associated changes in the temporomandibular joint and the mandibular symphysis. Am. J. Orthod. 1983, 84, 443–465. [Google Scholar] [CrossRef]
- Spady, M.; Buschang, P.H.; Demirjian, A.; Lapalme, L. Mandibular rotation and angular remodeling during childhood and adolescence. Am. J. Hum. Biol. 1992, 4, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Bjork, A. Sutural growth of the upper face studied by the implant method. Acta Odontol. Scand. 1966, 24, 109–127. [Google Scholar] [CrossRef] [PubMed]
- Enlow, D.H. The Human Face: An Account of the Postnatal Growth and Development of the Craniofacial Skeleton; Hoeber Medical Division, Harper & Row: New York, NY, USA, 1968. [Google Scholar]
- Donald, H.; Enlow, M.G.H. Essentials of Facial Growth; W. B. Saunders Company: Philadelphia, PA, USA, 1996. [Google Scholar]
- Lavergne, J.; Gasson, N. Direction and intensity of mandibular rotation in the sagittal adjustment during growth of the jaws. Scand. J. Dent. Res. 1977, 85, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Nielsen, I.L. A longitudinal study of condylar growth and mandibular rotation in untreated subjects with class II malocclusion. Angle Orthod. 2002, 72, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Riolo, M.L. An Atlas of Craniofacial Growth; Center for Human Growth and Development, The University of Michigan.: Ann Arbor, Michigan, 1974. [Google Scholar]
- Lux, C.J.; Burden, D.; Conradt, C.; Komposch, G. Age-related changes in sagittal relationship between the maxilla and mandible. Eur. J. Orthod. 2005, 27, 568–578. [Google Scholar] [CrossRef] [PubMed]
- Sassouni, V. A classification of skeletal facial types. Am. J. Orthod. 1969, 55, 109–123. [Google Scholar] [CrossRef]
- Buschang, P.H.; Santos-Pinto, A.; Demirjian, A. Incremental growth charts for condylar growth between 6 and 16 years of age. Eur. J. Orthod. 1999, 21, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.S.; Buschang, P.H. How does tooth eruption relate to vertical mandibular growth displacement? Am. J. Orthod. Dentofacial Orthop. 2011, 139, 745–751. [Google Scholar] [CrossRef]
- Buschang, P.H.; Roldan, S.I.; Tadlock, L.P. Guidelines for assessing the growth and development of orthodontic patients. Semin. Orthod. 2017, 321–335. [Google Scholar] [CrossRef]
- Buschang, P.H.; Tanguay, R.; Demirjian, A.; LaPalme, L.; Goldstein, H. Pubertal growth of the cephalometric point gnathion: Multilevel models for boys and girls. Am. J. Phys. Anthropol. 1988, 77, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Buschang, P.H.; Gandini Junior, L.G. Mandibular skeletal growth and modelling between 10 and 15 years of age. Eur. J. Orthod. 2002, 24, 69–79. [Google Scholar] [CrossRef] [Green Version]
- Buschang, P.H. Class I malocclusions—the development and etiology of mandibular malalignments. Semin. Orthod. 2014, 20, 3–15. [Google Scholar] [CrossRef]
- Iseri, H.; Solow, B. Continued eruption of maxillary incisors and first molars in girls from 9 to 25 years, studied by the implant method. Eur. J. Orthod. 1996, 18, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Stahl, F.; Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. Longitudinal growth changes in untreated subjects with Class II Division 1 malocclusion. Am. J. Orthod. Dentofacial Orthop. 2008, 134, 125–137. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Female | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Average | S.D. | Min | Max | p−Value | N | Average | S.D. | Min | Max | p−Value | ||
| Cranial Base | |||||||||||||
| N | x | 11 | 0.78 | 0.48 | 0.00 | 1.60 | * | 18 | 0.66 | 0.60 | 0.00 | 1.87 | * |
| y | 11 | 0.15 | 0.46 | −0.60 | 1.26 | NS | 18 | 0.07 | 0.73 | −2.23 | 1.35 | NS | |
| Or | x | 11 | 0.49 | 0.47 | 0.00 | 1.54 | * | 19 | 0.79 | 0.54 | −0.21 | 1.76 | * |
| y | 11 | −0.37 | 0.41 | −1.37 | 0.00 | * | 19 | −0.19 | 0.53 | −1.12 | 0.81 | NS | |
| Po | x | 11 | −0.40 | 0.33 | −0.93 | 0.16 | * | 19 | −0.25 | 0.51 | −1.33 | 0.73 | * |
| y | 11 | −0.33 | 0.44 | −1.52 | 0.00 | * | 19 | −0.34 | 0.46 | −1.17 | 0.49 | * | |
| A | x | 11 | 0.91 | 0.68 | −0.56 | 1.74 | * | 19 | 0.70 | 0.91 | −0.95 | 1.88 | * |
| y | 11 | −0.98 | 0.34 | −1.74 | −0.49 | * | 19 | −0.84 | 0.68 | −2.29 | 0.56 | * | |
| B | x | 7 | 1.25 | 1.15 | −0.81 | 2.90 | * | 13 | 1.64 | 0.96 | 0.00 | 3.12 | * |
| y | 7 | −0.80 | 1.08 | −2.26 | 0.90 | NS | 13 | −0.90 | 1.36 | −3.03 | 1.07 | * | |
| Maxilla | |||||||||||||
| U6 | x | 9 | 0.33 | 0.21 | 0.00 | 0.54 | * | 18 | 0.37 | 0.37 | 0.00 | 1.13 | * |
| y | 9 | −0.94 | 0.61 | −1.87 | 0.00 | * | 18 | −0.82 | 0.61 | −1.74 | 0.00 | * | |
| U1 | x | 9 | 0.27 | 0.24 | 0.00 | 0.77 | * | 18 | 0.40 | 0.89 | −0.79 | 2.06 | NS |
| y | 9 | −1.01 | 0.66 | −2.44 | 0.00 | * | 18 | −0.95 | 1.21 | −5.03 | 0.00 | * | |
| A | x | 11 | 0.07 | 0.43 | −0.73 | 0.77 | NS | 19 | 0.03 | 0.43 | −1.28 | 0.78 | NS |
| y | 11 | −0.42 | 0.47 | −1.36 | 0.00 | * | 19 | −0.32 | 0.67 | −2.36 | 0.62 | NS | |
| Mandible | |||||||||||||
| L6 | x | 8 | 0.57 | 0.42 | 0.00 | 1.16 | * | 19 | 0.62 | 0.49 | 0.00 | 1.39 | * |
| y | 8 | 0.66 | 0.35 | 0.00 | 1.04 | * | 19 | 0.41 | 0.40 | 0.00 | 1.40 | * | |
| L1 | x | 8 | 0.34 | 0.27 | 0.00 | 0.86 | * | 18 | 0.28 | 0.56 | −0.85 | 1.84 | * |
| y | 8 | 0.88 | 0.50 | 0.16 | 1.54 | * | 18 | 0.41 | 0.45 | 0.00 | 1.71 | * | |
| B | x | 10 | 0.05 | 0.11 | 0.00 | 0.26 | NS | 19 | −0.08 | 0.29 | −0.79 | 0.46 | NS |
| y | 10 | 0.74 | 0.81 | −0.49 | 1.96 | * | 19 | 0.27 | 1.06 | −2.43 | 2.23 | NS | |
| Co | x | 11 | −0.62 | 0.51 | −1.72 | 0.00 | * | 19 | −0.43 | 0.99 | −2.47 | 1.67 | NS |
| y | 11 | 2.75 | 0.80 | 0.73 | 3.89 | * | 19 | 2.37 | 1.13 | 0.19 | 5.15 | * | |
| Males | Females | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Average | SD | Min | Max | p−Value | N | Average | SD | Min | Max | p−Value | |
| SN (mm) | 11 | 0.90 | 0.49 | 0.00 | 1.82 | * | 18 | 0.98 | 0.77 | 0.00 | 3.34 | * |
| Co−Gn (mm) | 11 | 2.51 | 0.51 | 1.51 | 3.18 | * | 19 | 2.06 | 0.92 | 0.50 | 3.80 | * |
| SNA (°) | 11 | −0.02 | 0.77 | −2.00 | 0.95 | NS | 18 | 0.15 | 0.94 | −2.12 | 1.30 | NS |
| SNB (°) | 8 | 0.23 | 0.49 | −0.49 | 0.84 | NS | 13 | 0.71 | 0.75 | −0.64 | 1.95 | * |
| ANB (°) | 8 | −0.37 | 0.53 | −1.57 | 0.11 | NS | 13 | −0.66 | 0.64 | −2.35 | 0.00 | * |
| SN−GoGn (°) | 8 | −0.54 | 0.37 | −1.20 | 0.08 | * | 13 | −0.35 | 0.86 | −1.85 | 0.57 | NS |
| CB line−A (°) | 11 | 0.16 | 0.59 | −0.85 | 1.06 | NS | 19 | 0.15 | 0.89 | −1.75 | 1.25 | NS |
| CB line−B (°) | 8 | 0.48 | 0.61 | −0.35 | 1.48 | NS | 13 | 0.91 | 0.63 | −0.29 | 2.01 | * |
| A−CB point−B (°) | 8 | −0.43 | 0.35 | −1.13 | −0.07 | * | 13 | −0.67 | 0.69 | −2.27 | 0.03 | * |
| CB line−GoGn (°) | 8 | −0.67 | 0.69 | −2.17 | 0.08 | * | 13 | −0.49 | 0.69 | −2.45 | 0.31 | * |
| CB line−Mx point (°) | 11 | 0.47 | 0.64 | −0.33 | 1.65 | * | 19 | 0.48 | 0.81 | −1.30 | 1.61 | * |
| CB line−Md point (°) | 8 | 0.69 | 0.58 | 0.00 | 1.65 | * | 13 | 1.08 | 0.73 | 0.00 | 2.46 | * |
| Md point−CB point−Mx point (°) | 8 | −0.19 | 0.22 | −0.65 | 0.00 | * | 13 | −0.48 | 0.59 | −1.64 | 0.08 | * |
| CB line−Mx line (°) | 11 | −0.53 | 0.47 | −1.43 | 0.10 | * | 19 | −0.57 | 1.05 | −2.87 | 2.63 | NS |
| CB line−Md line (°) | 8 | −1.26 | 0.66 | −2.52 | −0.47 | * | 13 | −1.24 | 1.27 | −3.90 | 0.39 | * |
| Co−Md line (°) | 11 | −0.94 | 0.68 | −1.90 | 0.10 | * | 19 | −0.99 | 1.18 | −4.41 | 0.00 | * |
| Md line−Md border (°) | 11 | −0.41 | 0.39 | −0.84 | 0.58 | * | 19 | −0.43 | 0.68 | −1.41 | 1.26 | * |
| Gonial Angle (°) | 11 | −0.63 | 0.54 | −1.33 | 0.20 | * | 19 | −0.43 | 0.77 | −2.15 | 1.02 | * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, L.; Jeon, H.H.; Li, C.; Boucher, N.; Chung, C.-H. Sagittal and Vertical Growth of the Maxillo–Mandibular Complex in Untreated Children: A Longitudinal Study on Lateral Cephalograms Derived from Cone Beam Computed Tomography. Sensors 2021, 21, 8484. https://doi.org/10.3390/s21248484
Yi L, Jeon HH, Li C, Boucher N, Chung C-H. Sagittal and Vertical Growth of the Maxillo–Mandibular Complex in Untreated Children: A Longitudinal Study on Lateral Cephalograms Derived from Cone Beam Computed Tomography. Sensors. 2021; 21(24):8484. https://doi.org/10.3390/s21248484
Chicago/Turabian StyleYi, Leah, Hyeran Helen Jeon, Chenshuang Li, Normand Boucher, and Chun-Hsi Chung. 2021. "Sagittal and Vertical Growth of the Maxillo–Mandibular Complex in Untreated Children: A Longitudinal Study on Lateral Cephalograms Derived from Cone Beam Computed Tomography" Sensors 21, no. 24: 8484. https://doi.org/10.3390/s21248484