
Role of Artificial Intelligence in COVID-19 Detection

 , , , , , ,
, , , , , ,  ,
,  ,
,
Abstract
:1. Introduction
- The state-of-the-art AI techniques (deep neural network (DNN) and hand-crafted feature learning (HCFL) based models) used to detect COVID-19.
- Analysis of the results of AI techniques with various imaging modalities.
- The key challenges and future direction in the detection of COVID-19.
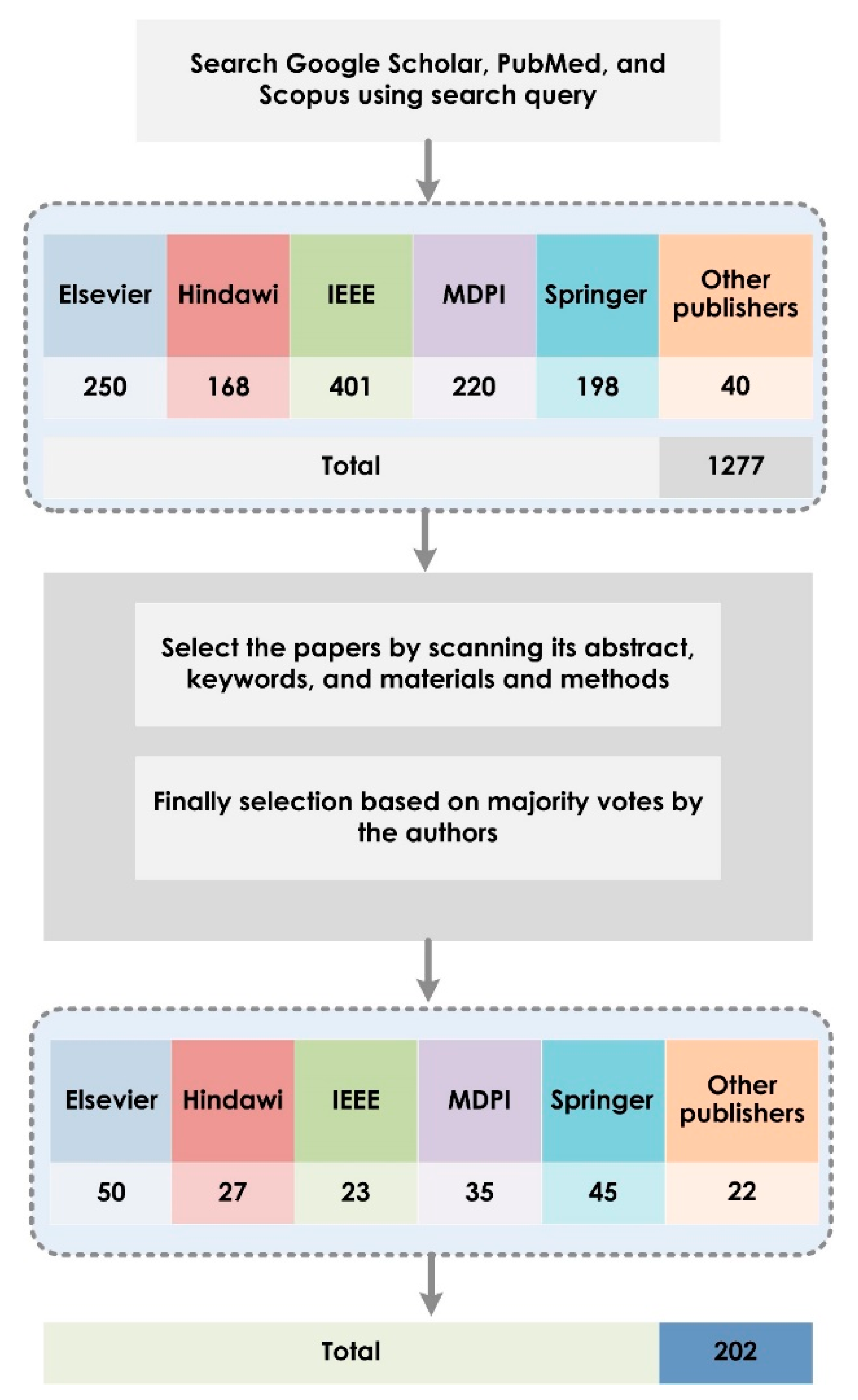
2. Search Criteria and Selection Process
3. AI Techniques for COVID-19 Detection
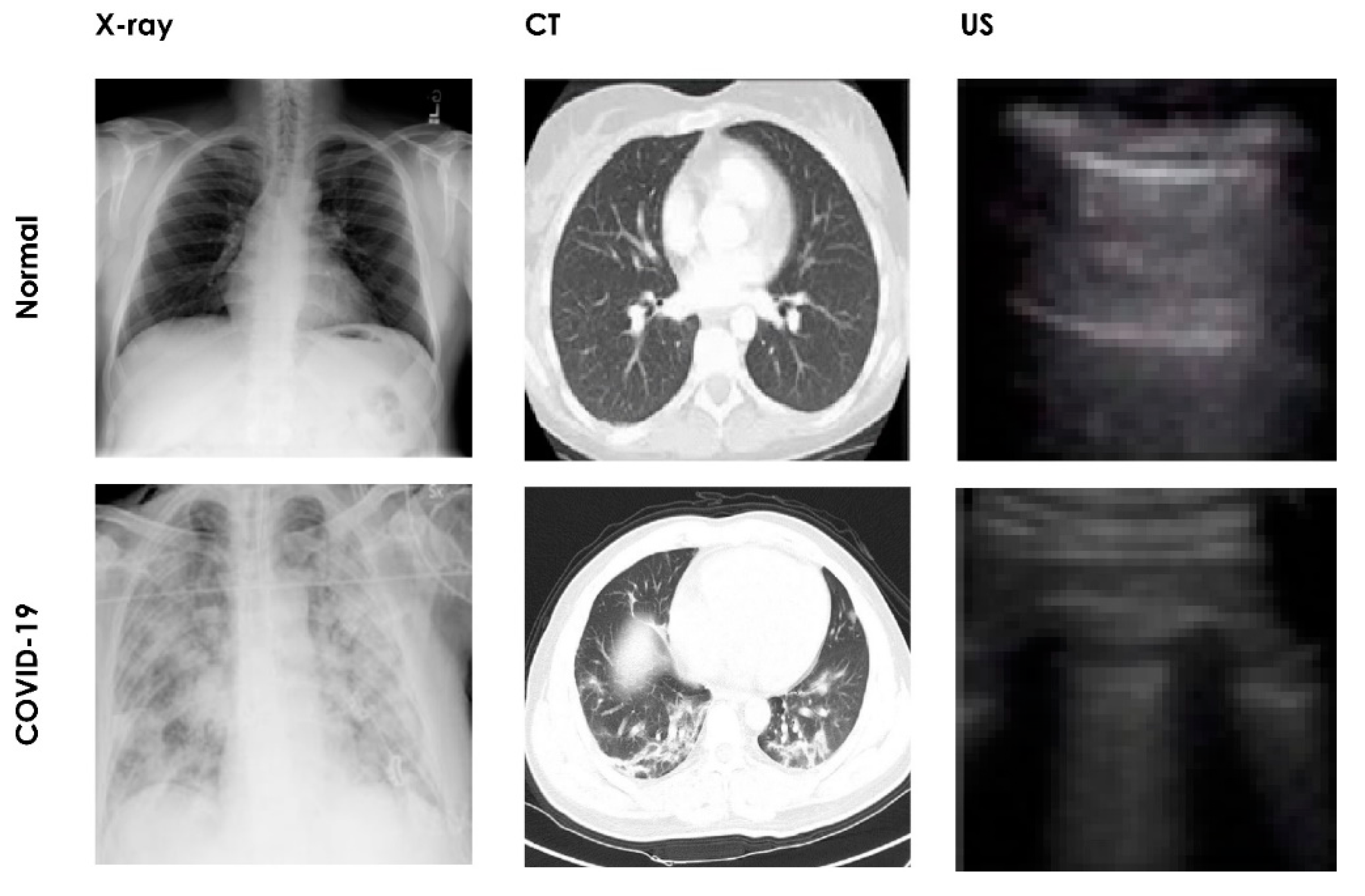
3.1. COVID-19 Dataset: Medical Image
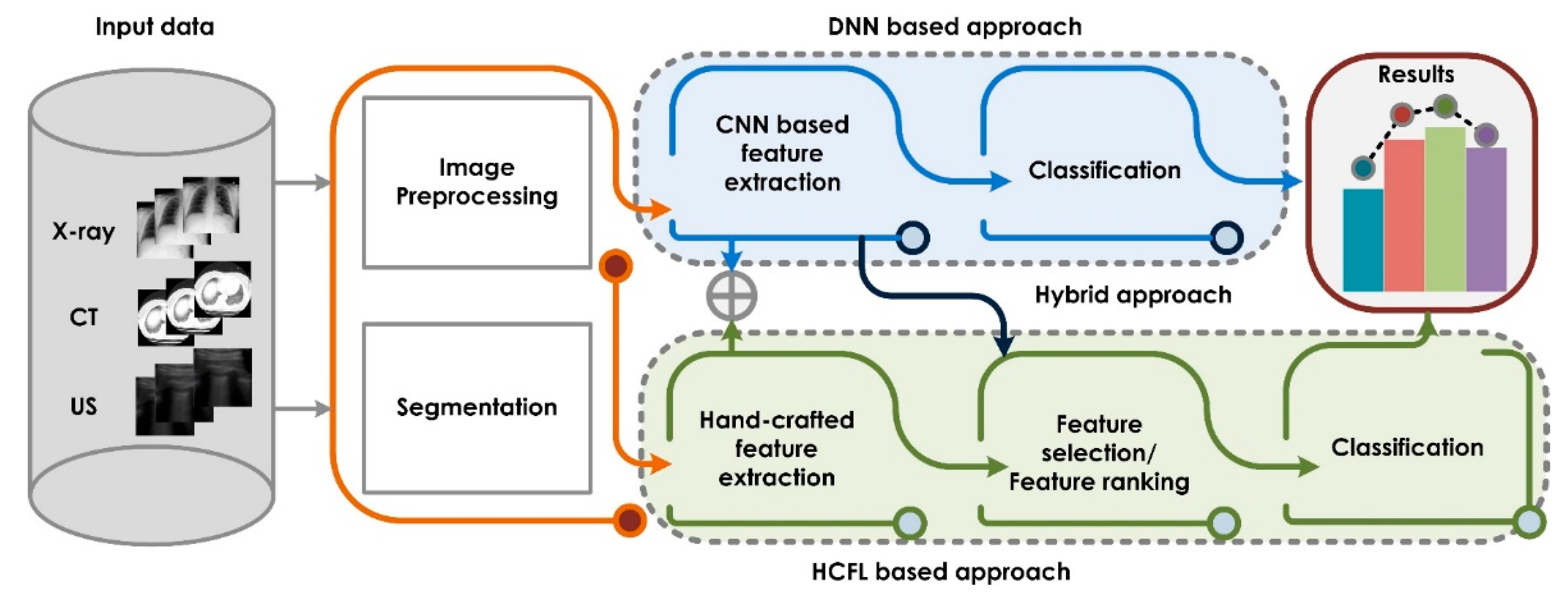
3.2. Methodology
3.2.1. Preprocessing/Segmentation
3.2.2. Feature Extraction
3.2.3. Feature Selection/Optimization
3.2.4. Classification
4. Results
5. Discussion
5.1. Future Trends
5.2. Limitations of the Review
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Zheng, M.; Gao, Y.; Wang, G.; Song, G.; Liu, S.; Sun, D.; Xu, Y.; Tian, Z. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 533–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Litvinova, M.; Wang, W.; Wang, Y.; Deng, X.; Chen, X.; Li, M.; Zheng, W.; Yi, L.; Chen, X.; et al. Evolving epidemiology and transmission dynamics of coronavirus disease 2019 outside Hubei province, China: A descriptive and modelling study. Lancet Infect. Dis. 2020, 20, 793–802. [Google Scholar] [CrossRef]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation and Treatment Coronavirus (COVID-19); Stat Pearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor recognition by novel coronavirus from Wuhan: An analysis based on decade-long structural studies of SARS. J. Virol. 2020, 94, e00127-20. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef]
- Sims, A.C.; Baric, R.S.; Yount, B.; Burkett, S.E.; Collins, P.L.; Pickles, R.J. Severe acute respiratory syndrome coronavirus infection of human ciliated airway epithelia: Role of ciliated cells in viral spread in the conducting airways of the lungs. J. Virol. 2005, 79, 15511–15524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, N.L.-S.; Chan, P.K.-S.; Wong, C.-K.; To, K.-F.; Wu, A.K.-L.; Sung, Y.-M.; Hui, D.S.-C.; Sung, J.J.-Y.; Lam, C.W.-K. Early Enhanced Expression of Interferon-Inducible Protein-10 (CXCL-10) and Other Chemokines Predicts Adverse Outcome in Severe Acute Respiratory Syndrome. Clin. Chem. 2005, 51, 2333–2340. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef]
- Donnelly, C.A.; Ghani, A.C.; Leung, G.M.; Hedley, A.J.; Fraser, C.; Riley, S.; Abu-Raddad, L.J.; Ho, L.M.; Thach, T.Q.; Chau, P.; et al. Epidemiological determinants of spread of causal agent of severe acute respiratory syndrome in hong kong. Lancet 2003, 361, 1761–1766. [Google Scholar] [CrossRef] [Green Version]
- Goyal, P.; Choi, J.J.; Pinheiro, L.C.; Schenck, E.J.; Chen, R.; Jabri, A.; Satlin, M.J.; Campion, T.R., Jr.; Nahid, M.; Ringel, J.B.; et al. Clinical Characteristics of Covid-19 in New York City. N. Engl. J. Med. 2020, 382, 2372–2374. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Young, B.E.; Ong, S.; Kalimuddin, S.; Low, J.G.; Tan, S.Y.; Loh, J.; Ng, O.T.; Marimuthu, K.; Ang, L.W.; Mak, T.M.; et al. Epidemiologic features and clinical course of patients infected with SARS-CoV-2 in Singapore. JAMA 2020, 323, 1488–1494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, K.S.; Hung, I.; Chan, P.; Lung, K.C.; Tso, E.; Liu, R.; Ng, Y.Y.; Chu, M.Y.; Chung, T.; Tam, A.R.; et al. Gastrointestinal manifestations of SARS-CoV-2 infection and virus load in fecal samples from the hong kong cohort and systematic review and meta-analysis. Gastroenterology 2020, 159, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.webmd.com/lung/COVID19-digestive-symptoms (accessed on 15 June 2020).
- Liu, R.; Han, H.; Liu, F.; Lv, Z.; Wu, K.; Liu, Y.; Feng, Y.; Zhu, C. Positive rate of RT–PCR detection of SARS-CoV-2 infection in 4880 cases from one hospital in Wuhan, China, from Jan to Feb 2020. Clin. Chim. Acta 2020, 505, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Kugunavar, S.; Prabhakar, C.J. Convolutional neural networks for the diagnosis and prognosis of the coronavirus disease pandemic. Vis. Comput. Ind. Biomed. Art 2021, 4, 12. [Google Scholar] [CrossRef]
- Shuja, J.; Alanazi, E.; Alasmary, W.; Alashaikh, A. COVID-19 open source data sets: A comprehensive survey. Appl. Intell. 2021, 51, 1296–1325. [Google Scholar] [CrossRef]
- Rehman, A.; Iqbal, M.; Xing, H.; Ahmed, I. COVID-19 Detection Empowered with Machine Learning and Deep Learning Techniques: A Systematic Review. Appl. Sci. 2021, 11, 3414. [Google Scholar] [CrossRef]
- Low, W.C.S.; Chuah, J.H.; Tee, C.A.T.H.; Anis, S.; Shoaib, M.A.; Faisal, A.; Khalil, A.; Lai, K.W. An Overview of Deep Learning Techniques on Chest X-ray and CT Scan Identification of COVID-19. Comput. Math. Methods Med. 2021, 2021, 5528144. [Google Scholar] [CrossRef]
- Ghaderzadeh, M.; Asadi, F. Deep Learning in the Detection and Diagnosis of COVID-19 Using Radiology Modalities: A Systematic Review. J. Health Eng. 2021, 2021, 6677314. [Google Scholar] [CrossRef]
- Ozsahin, I.; Sekeroglu, B.; Musa, M.S.; Mustapha, M.T.; Ozsahin, D.U. Review on Diagnosis of COVID-19 from Chest CT Images Using Artificial Intelligence. Comput. Math. Methods Med. 2020, 2020, 9756518. [Google Scholar] [CrossRef]
- Aishwarya, T.; Kumar, V.R. Machine Learning and Deep Learning Approaches to Analyze and Detect COVID-19: A Review. SN Comput. Sci. 2021, 2, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nayak, J.; Naik, B.; Dinesh, P.; Vakula, K.; Dash, P.B.; Pelusi, D. Significance of deep learning for Covid-19: State-of-the-art review. Res. Biomed. Eng. 2021, 1–24. [Google Scholar] [CrossRef]
- Alballa, N.; Al-Turaiki, I. Machine Learning Approaches in COVID-19 Diagnosis, Mortality, and Severity Risk Prediction: A Review. Inform. Med. Unlocked 2021, 24, 100564. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, S.; Maddikunta, P.K.R.; Pham, Q.-V.; Gadekallu, T.R.; Chowdhary, C.L.; Alazab, M.; Piran, J. Deep learning and medical image processing for coronavirus (COVID-19) pandemic: A survey. Sustain. Cities Soc. 2021, 65, 102589. [Google Scholar] [CrossRef]
- Tayarani, M.H. Applications of artificial intelligence in battling against covid-19: A literature review. Chaos Solitons Fractals 2021, 142, 110338. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Huang, P.; Liu, T.; Huang, L.; Liu, H.; Lei, M.; Xu, W.; Hu, X.; Chen, J.; Liu, B. Use of Chest CT in Combination with Negative RT-PCR Assay for the 2019 Novel Coronavirus but High Clinical Suspicion. Radiology 2020, 295, 22–23. [Google Scholar] [CrossRef]
- Cellina, M.; Martinenghi, C.; Marino, P.; Oliva, G. COVID-19 pneumonia—ultrasound, radiographic, and computed tomography findings: A comprehensive pictorial essay. Emerg. Radiol. 2021, 28, 519–526. [Google Scholar] [CrossRef]
- Yan, T. Ccap: A Chest Ct Dataset. 2020. Available online: https://ieee-dataport.org/authors/tao-yan (accessed on 29 November 2021).
- Available online: https://iclus-web.bluetensor.ai/ (accessed on 5 October 2020).
- Zhao, J.; Zhang, Y.; He, X.; Xie, P. COVID-CT-Dataset: A CT scan dataset about COVID-19. arXiv 2020, arXiv:2003.13865. [Google Scholar]
- Soares, E.; Angelov, P.; Biaso, S.; Froes, M.H.; Abe, D.K. SARSCov-2 CT-scan dataset: A large dataset of real patients CT scans for SARS-cov-2 identification. MedRxiv 2020, 20078584. [Google Scholar] [CrossRef]
- Morozov, S.P.; Andreychenko, A.E.; Pavlov, N.A.; Vladzymyrskyy, A.V.; Ledikhova, N.V.; Gombolevskiy, V.A.; Blokhin, I.A.; Gelezhe, P.B.; Gonchar, A.V.; Chernina, V.Y. Mosmeddata: Chest ct scans with covid-19 related findings dataset. arXiv 2020, arXiv:2005.06465. [Google Scholar]
- Ma, J.; Cheng, G.; Wang, Y.; An, X.; Gao, J.; Yu, Z.; Zhang, M.; Liu, X.; Deng, X.; Cao, S.; et al. COVID-19 CT Lung and Infection Segmentation Dataset. Zenodo 2020, 20, 3757476. [Google Scholar] [CrossRef]
- Born, J.; Wiedemann, N.; Cossio, M.; Buhre, C.; Brändle, G.; Leidermann, K.; Aujayeb, A.; Moor, M.; Rieck, B.; Borgwardt, K. Accelerating Detection of Lung Pathologies with Explainable Ultrasound Image Analysis. Appl. Sci. 2021, 11, 672. [Google Scholar] [CrossRef]
- Karel, Z. Contrast Limited Adaptive Histograph Equalization. Graphic Gems IV; Academic Press Professional: San Diego, CA, USA, 1994; pp. 474–485. [Google Scholar]
- Kirsch, R. Computer determination of the constituent structure of biological images. Comput. Biomed. Res. 1971, 4, 315–328. [Google Scholar] [CrossRef]
- Gonzales, R.C.; Richard, E. Woods. Digital Image Processing, 2nd ed.; Englewood Cliffs: Prentice Hall, NJ, USA, 2002. [Google Scholar]
- Charles, P. Digital Video and HDTV Algorithms and Interfaces; Morgan Kaufman Publishers: San Francisco, CA, USA, 2003. [Google Scholar]
- Haralick, R.M.; Shapiro, L.G. Image segmentation techniques. Comput. Vis. Graph. Image Process. 1985, 29, 100–132. [Google Scholar] [CrossRef]
- Meyer, F. Topographic distance and watershed lines. Signal Process. 1994, 38, 113–125. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: Berlin/Heidelberg, Germany, 2015; pp. 234–241. [Google Scholar]
- Chaurasia, A.; Culurciello, E. LinkNet: Exploiting encoder representations for efficient semantic segmentation. In Proceedings of the 2017 IEEE Visual Communications and Image Processing (VCIP), Saint Petersburg, FL, USA, 10–13 December 2017; pp. 1–4. [Google Scholar]
- Selvan, R.; Dam, E.B.; Detlefsen, N.S.; Rischel, S.; Sheng, K.; Nielsen, M.; Pai, A. Lung segmentation from chest X-rays using variational data imputation. arXiv 2020, arXiv:2005.10052. [Google Scholar]
- Rahman, S.; Sarker, S.; Al Miraj, A.; Nihal, R.A.; Haque, A.K.M.N.; Al Noman, A. Deep Learning–Driven Automated Detection of COVID-19 from Radiography Images: A Comparative Analysis. Cogn. Comput. 2021, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Chandra, T.B.; Verma, K.; Singh, B.K.; Jain, D.; Netam, S.S. Coronavirus disease (COVID-19) detection in Chest X-ray images using majority voting based classifier ensemble. Expert Syst. Appl. 2021, 165, 113909. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Radford, A.; Metz, L.; Chintala, S. Unsupervised representation learning with deep convolutional generative adversarial networks. In Proceedings of the 4th International Conference on Learning Representations, ICLR 2016—Conference Track Proceedings, San Juan, PR, USA, 2–4 May 2016. [Google Scholar]
- Mehdi, M.; Osindero, S. Conditional generative adversarial nets. arXiv 2014, arXiv:1411.1784. [Google Scholar]
- Waheed, A.; Goyal, M.; Gupta, D.; Khanna, A.; Al-Turjman, F.; Pinheiro, P.R. CovidGAN: Data Augmentation Using Auxiliary Classifier GAN for Improved Covid-19 Detection. IEEE Access 2020, 8, 91916–91923. [Google Scholar] [CrossRef]
- Mallat, S.G. A theory for multiresolution signal decomposition: The wavelet representation. IEEE Trans. Pattern Anal. Mach. Intell. 1989, 11, 674–693. [Google Scholar] [CrossRef] [Green Version]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I. Textural Features for Image Classification. IEEE Trans. Syst. Man Cybern 1973, SMC-3, 610–621. [Google Scholar] [CrossRef] [Green Version]
- Górszczyk, A.; Malinowski, M.; Bellefleur, G. Enhancing 3D post-stack seismic data acquired in hardrock environment using 2D curvelet transform. Geophys Prospect. 2015, 63, 903–918. [Google Scholar] [CrossRef]
- Tuncer, T.; Dogan, S.; Ozyurt, F. An automated Residual Exemplar Local Binary Pattern and iterative ReliefF based COVID-19 detection method using chest X-ray image. Chemom. Intell. Lab. Syst. 2020, 203, 104054. [Google Scholar] [CrossRef]
- Dalal, N.; Triggs, B. Histograms of Oriented Gradients for Human Detection. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR’05), San Diego, CA, USA, 20–25 June 2005. [Google Scholar] [CrossRef] [Green Version]
- Yin, M.; Liu, W.; Zhao, X.; Guo, Q.-W.; Bai, R.-F. Image denoising using trivariate prior model in nonsubsampled dual-tree complex contourlet transform domain and non-local means filter in spatial domain. Optik 2013, 124, 6896–6904. [Google Scholar] [CrossRef]
- Ranjbarzadeh, R.; Ghoushchi, S.J.; Bendechache, M.; Amirabadi, A.; Ab Rahman, M.N.; Saadi, S.B.; Aghamohammadi, A.; Forooshani, M.K. Lung Infection Segmentation for COVID-19 Pneumonia Based on a Cascade Convolutional Network from CT Images. BioMed Res. Int. 2021, 2021, 5544742. [Google Scholar] [CrossRef]
- Available online: https://pillow.readthedocs.io/en/3.1.x/reference/Image.html (accessed on 20 May 2020).
- Elaziz, M.A.; Hosny, K.M.; Salah, A.; Darwish, M.M.; Lu, S.; Sahlol, A.T. New machine learning method for image-based diagnosis of COVID-19. PLoS ONE 2020, 15, e0235187. [Google Scholar] [CrossRef]
- Ojala, T.; Pietikainen, M.; Maenpaa, T. Multiresolution gray-scale and rotation invariant texture classification with local binary patterns. IEEE Trans. Pattern Anal. Mach. Intell. 2002, 24, 971–987. [Google Scholar] [CrossRef]
- Hosny, K.M.; Darwish, M.M.; Li, K.; Salah, A. COVID-19 diagnosis from CT scans and chest X-ray images using low-cost Raspberry Pi. PLoS ONE 2021, 16, e0250688. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef] [Green Version]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Net Works. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; van der Maaten, L.; Kilian, Q. Weinberger. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Zhou, B.; Lapedriza, A.; Torralba, A.; Oliva, A. Places: An Image Database for Deep Scene Understanding. arXiv 2016, arXiv:1610.02055. [Google Scholar] [CrossRef]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.C. MobileNetV2: Inverted Residuals and Linear Bottlenecks. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Iandola, F.N.; Han, S.; Moskewicz, M.W.; Ashraf, K.; Dally, W.J.; Keutzer, K. SqueezeNet: AlexNet-level accuracy with 50x fewer parameters and <0.5 MB model size. arXiv 2016, arXiv:1602.07360. [Google Scholar]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. ImageNet Large Scale Visual Recognition Challenge. arXiv 2015, arXiv:1409.0575. [Google Scholar] [CrossRef] [Green Version]
- Chollet, F. Xception: Deep Learning with Depthwise Separable Convolutions. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 1800–1807. [Google Scholar] [CrossRef] [Green Version]
- Ahsan, M.; Alam, T.E.; Trafalis, T.; Huebner, P. Deep MLP-CNN Model Using Mixed-Data to Distinguish between COVID-19 and Non-COVID-19 Patients. Symmetry 2020, 12, 1526. [Google Scholar] [CrossRef]
- Ahmed, S.; Hossain, T.; Hoque, O.B.; Sarker, S.; Rahman, S.; Shah, F.M. Automated COVID-19 Detection from Chest X-ray Images: A High-Resolution Network (HRNet) Approach. SN Comput. Sci. 2021, 2, 1–17. [Google Scholar] [CrossRef]
- Guyon, I.; Elisseeff, A. An introduction to variable and feature selection. J. Mach. Learn. Res. 2003, 3, 1157–1182. [Google Scholar]
- Mirjalili, S.; Gandomi, A.H.; Mirjalili, S.Z.; Saremi, S.; Faris, H.; Mirjalili, S.M. Salp Swarm Algorithm: A bio-inspired optimizer for engineering design problems. Adv. Eng Softw. 2017, 114, 163–191. [Google Scholar] [CrossRef]
- El-Kenawy, E.-S.M.; Mirjalili, S.; Ibrahim, A.; Alrahmawy, M.; El-Said, M.; Zaki, R.M.; Eid, M.M. Advanced Meta-Heuristics, Convolutional Neural Networks, and Feature Selectors for Efficient COVID-19 X-ray Chest Image Classification. IEEE Access 2021, 9, 36019–36037. [Google Scholar] [CrossRef]
- Geem, Z.W.; Kim, J.H.; Loganathan, G. A new heuristic optimization algorithm: Harmony search. Simulation 2001, 76, 60–68. [Google Scholar] [CrossRef]
- Tuncer, T.; Akbal, E.; Dogan, S. An automated snoring sound classification method based on local dual octal pattern and iterative hybrid feature selector, Biomed. Signal Process Contr. 2021, 63, 102173. [Google Scholar] [CrossRef] [PubMed]
- Mirjalili, S.; Mirjalili, S.M.; Lewis, A. Grey Wolf Optimizer. Adv. Eng. Softw. 2014, 69, 46–61. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.K.; Kumar, A.; Mahmud, M.; Kaiser, M.S.; Kishore, A. COVID-19 Infection Detection from Chest X-ray Images Using Hybrid Social Group Optimization and Support Vector Classifier. Cogn. Comput. 2021, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Sahlol, A.T.; Yousri, D.; Ewees, A.A.; Al-Qaness, M.A.A.; Damasevicius, R.; Elaziz, M.A. COVID-19 image classification using deep features and fractional-order marine predators algorithm. Sci. Rep. 2020, 10, 1–15. [Google Scholar] [CrossRef]
- Peng, H.; Long, F.; Ding, C. Feature selection based on mutual information criteria of max-dependency, max-relevance, and min-redundancy. IEEE Trans. Pattern Anal. Mach. Intell. 2005, 27, 1226–1238. [Google Scholar] [CrossRef] [PubMed]
- van der Maaten, L.; Hinton, G. Visualizing data using t-SNE. J. Mach. Learn. Res. 2008, 9, 2579–2605. [Google Scholar]
- Krzanowski, W.J. Principles of Multivariate Analysis; Oxford University Press: Oxford, UK, 1988. [Google Scholar]
- Kojadinovic, I. Relevance measures for subset variable selection in regression problems based on k-additive mutual information. Comput. Stat. Data Anal. 2005, 49, 1205–1227. [Google Scholar] [CrossRef]
- Spolaor, N.; Cherman, E.A.; Monard, M.C.; Lee, H.D. ReliefF for Multi-label Feature Selection. In Proceedings of the 2013 Brazilian Conference on Intelligent Systems, Fortaleza, Brazil, 19–24 October 2013; pp. 6–11. [Google Scholar]
- Mirjalili, S. Dragonfly algorithm: A new meta-heuristic optimization technique for solving single-objective, discrete, and multi-objective problems. Neural Comput. Appl. 2016, 27, 1053–1073. [Google Scholar] [CrossRef]
- El-Kenawy, E.-S.M.; Ibrahim, A.; Mirjalili, S.; Eid, M.M.; Hussein, S.E. Novel Feature Selection and Voting Classifier Algorithms for COVID-19 Classification in CT Images. IEEE Access 2020, 8, 179317–179335. [Google Scholar] [CrossRef]
- Hasan, A.M.; Al-Jawad, M.M.; Jalab, H.A.; Shaiba, H.; Ibrahim, R.W.; Al-Shamasneh, A.R. Classification of Covid-19 Coronavirus, Pneumonia and Healthy Lungs in CT Scans Using Q-Deformed Entropy and Deep Learning Features. Entropy 2020, 22, 517. [Google Scholar] [CrossRef]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. In Proceedings of the International Conference Learn Represent (ICLR), San Diego, CA, USA, 5–8 May 2015. [Google Scholar]
- Tieleman, T.; Hinton, G. Divide the gradient by a running average of its recent magnitude. coursera: Neural Networks Machine Learning. Tech. Rep. 2012, 4, 26–31. [Google Scholar]
- Mirjalili, S.; Lewis, A. The whale optimization algorithm. Adv. Eng. Softw. 2016, 95, 51–67. [Google Scholar] [CrossRef]
- Pathan, S.; Siddalingaswamy, P.; Ali, T. Automated Detection of Covid-19 from Chest X-ray scans using an optimized CNN architecture. Appl. Soft Comput. 2021, 104, 107238. [Google Scholar] [CrossRef]
- Simon, D. Biogeography-Based Optimization. IEEE Trans. Evol. Comput. 2008, 12, 702–713. [Google Scholar] [CrossRef] [Green Version]
- Singh, D.; Kumar, V.; Kaur, M. Classification of COVID-19 patients from chest CT images using multi-objective differential evolution–based convolutional neural networks. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1379–1389. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.K. The random subspace method for constructing decision forests. IEEE Trans. Pattern Anal. Mach. Intell. 1998, 20, 832–844. [Google Scholar] [CrossRef] [Green Version]
- Sain, S.R.; Vapnik, V.N. The Nature of Statistical Learning Theory. Technometrics 1996, 38, 409. [Google Scholar] [CrossRef]
- Breiman, L. Bagging predictors. Mach. Learn. 1996, 24, 123–140. [Google Scholar] [CrossRef] [Green Version]
- Larose, D.T. Data Mining Methods and Models; Wiley: Hoboken, NJ, USA, 2005. [Google Scholar]
- Breiman, L.; Friedman, J.H.; Olshen, R.A.; Stone, C.J. Classification and Regression Trees; Chapman & Hall: Boca Raton, FL, USA, 1984. [Google Scholar]
- Schutze, H.; Manning, C.D.; Raghavan, P. Introduction to Information Retrieval; Cambridge University Press: Cambridge, UK, 2008. [Google Scholar]
- Hopfield, J.J. Artificial neural networks. IEEE Circuits Devices Mag. 1988, 4, 3–10. [Google Scholar] [CrossRef]
- Wasserman, P.D. Advanced Methods in Neural Computing; Van Nostrand Reinhold: New York, NY, USA, 1993. [Google Scholar]
- Trevor, T.; Robert, T.; Jerome, F. The Elements of Statistical Learning: Data Mining, Inference, and Prediction; Springer: New York, NY, USA, 2009. [Google Scholar]
- Donald, F. Probabilistic neural networks. Neural Netw. 1990, 3, 109–118. [Google Scholar]
- Huang, G.-B.; Zhou, H.; Ding, X.; Zhang, R. Extreme Learning Machine for Regression and Multiclass Classification. IEEE Trans. Syst Man Cybern B Cybern 2012, 42, 513–529. [Google Scholar] [CrossRef] [Green Version]
- Freund, Y.; Schapire, R.E. A decision-theoretic generalization of on-line learning and an application to boosting. J. Comput. Syst. Sci. 1997, 55, 119–139. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the 22nd Acm Sigkdd International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Wright, R. Logistic regression. In Reading & Understanding Multivariate Statistics; Grimm, L.C., Yarnold, P.R., Eds.; American Psychological Association: Washington, DC, USA, 1995. [Google Scholar]
- Mostafiz, R.; Uddin, M.S.; Nur-A-Alam, R.M.; Rahman, M.M. Covid-19 detection in chest X-ray through random forest classifier using a hybridization of deep CNN and DWT optimized features. J. King Saud Univ.-Comput. Inf. Sci. 2020. [Google Scholar] [CrossRef]
- Brunese, L.; Martinelli, F.; Mercaldo, F.; Santone, A. Machine learning for coronavirus covid-19 detection from chest X-rays. Procedia Comput. Sci. 2020, 176, 2212–2221. [Google Scholar] [CrossRef] [PubMed]
- Islam, Z.; Islam, M.; Asraf, A. A combined deep CNN-LSTM network for the detection of novel coronavirus (COVID-19) using X-ray images. Inform. Med. Unlocked 2020, 20, 100412. [Google Scholar] [CrossRef]
- Rahimzadeh, M.; Attar, A. A modified deep convolutional neural network for detecting COVID-19 and pneumonia from chest X-ray images based on the concatenation of Xception and ResNet50V2. Inform. Med. Unlocked 2020, 19, 100360. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.I.; Shah, J.L.; Bhat, M.M. CoroNet: A deep neural network for detection and diagnosis of COVID-19 from chest X-ray images. Comput. Methods Programs Biomed. 2020, 196, 105581. [Google Scholar] [CrossRef] [PubMed]
- Dorr, F.; Chaves, H.; Serra, M.M.; Ramirez, A.; Costa, M.E.; Seia, J.; Cejas, C.; Castro, M.; Eyheremendy, E.; Slezak, D.F.; et al. COVID-19 pneumonia accurately detected on chest radiographs with artificial intelligence. Intell. Med. 2020, 3, 100014. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Acharya, U.R. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput. Biol. Med. 2020, 121, 103792. [Google Scholar] [CrossRef] [PubMed]
- Altan, A.; Karasu, S. Recognition of COVID-19 disease from X-ray images by hybrid model consisting of 2D curvelet transform, chaotic salp swarm algorithm and deep learning technique. Chaos Solitons Fractals 2020, 140, 110071. [Google Scholar] [CrossRef]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Explainable Deep Learning for Pulmonary Disease and Coronavirus COVID-19 Detection from X-rays. Comput. Methods Programs Biomed. 2020, 196, 105608. [Google Scholar] [CrossRef] [PubMed]
- Jain, G.; Mittal, D.; Thakur, D.; Mittal, M.K. A deep learning approach to detect Covid-19 coronavirus with X-ray images. Biocybern. Biomed. Eng. 2020, 40, 1391–1405. [Google Scholar] [CrossRef]
- Heidari, M.; Mirniaharikandehei, S.; Khuzani, A.Z.; Danala, G.; Qiu, Y.; Zheng, B. Improving the performance of CNN to predict the likelihood of COVID-19 using chest X-ray images with preprocessing algorithms. Int. J. Med. Inform. 2020, 144, 104284. [Google Scholar] [CrossRef]
- Minaee, S.; Kafieh, R.; Sonka, M.; Yazdani, S.; Soufi, G.J. Deep-COVID: Predicting COVID-19 from chest X-ray images using deep transfer learning. Med. Image Anal. 2020, 65, 101794. [Google Scholar] [CrossRef]
- Afshar, P.; Heidarian, S.; Naderkhani, F.; Oikonomou, A.; Plataniotis, K.N.; Mohammadi, A. COVID-CAPS: A capsule network-based framework for identification of COVID-19 cases from X-ray images. Pattern Recognit. Lett. 2020, 138, 638–643. [Google Scholar] [CrossRef]
- Panwar, H.; Gupta, P.; Siddiqui, M.K.; Morales-Menendez, R.; Singh, V. Application of deep learning for fast detection of COVID-19 in X-rays using nCOVnet. Chaos Solitons Fractals 2020, 138, 109944. [Google Scholar] [CrossRef]
- Azemin, M.Z.C.; Hassan, R.; Tamrin, M.I.M.; Ali, M.A.M. COVID-19 Deep Learning Prediction Model Using Publicly Available Radiologist-Adjudicated Chest X-ray Images as Training Data: Preliminary Findings. Int. J. Biomed. Imaging 2020, 2020, 8828855. [Google Scholar] [CrossRef]
- Sharma, A.; Rani, S.; Gupta, D. Artificial Intelligence-Based Classification of Chest X-ray Images into COVID-19 and Other Infectious Diseases. Int. J. Biomed. Imaging 2020, 2020, 8889023. [Google Scholar] [CrossRef]
- Haque, K.F.; Abdelgawad, A. A Deep Learning Approach to Detect COVID-19 Patients from Chest X-ray Images. AI 2020, 1, 418–435. [Google Scholar] [CrossRef]
- Civit-Masot, J.; Luna-Perejón, F.; Morales, M.D.; Civit, A. Deep Learning System for COVID-19 Diagnosis Aid Using X-ray Pulmonary Images. Appl. Sci. 2020, 10, 4640. [Google Scholar] [CrossRef]
- Duran-Lopez, L.; Dominguez-Morales, J.; Corral-Jaime, J.; Vicente-Diaz, S.; Linares-Barranco, A. COVID-XNet: A Custom Deep Learning System to Diagnose and Locate COVID-19 in Chest X-ray Images. Appl. Sci. 2020, 10, 5683. [Google Scholar] [CrossRef]
- Misra, S.; Jeon, S.; Lee, S.; Managuli, R.; Jang, I.-S.; Kim, C. Multi-Channel Transfer Learning of Chest X-ray Images for Screening of COVID-19. Electronics 2020, 9, 1388. [Google Scholar] [CrossRef]
- Tartaglione, E.; Barbano, C.; Berzovini, C.; Calandri, M.; Grangetto, M. Unveiling COVID-19 from CHEST X-ray with Deep Learning: A Hurdles Race with Small Data. Int. J. Environ. Res. Public Health 2020, 17, 6933. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Aslam, N. A Deep-Learning-Based Framework for Automated Diagnosis of COVID-19 Using X-ray Images. Information 2020, 11, 419. [Google Scholar] [CrossRef]
- Lee, K.-S.; Kim, J.; Jeon, E.-T.; Choi, W.; Kim, N.; Lee, K. Evaluation of Scalability and Degree of Fine-Tuning of Deep Convolutional Neural Networks for COVID-19 Screening on Chest X-ray Images Using Explainable Deep-Learning Algorithm. J. Pers. Med. 2020, 10, 213. [Google Scholar] [CrossRef]
- De Moura, J.; Ramos, J.J.D.M.; Vidal, P.L.; Novo, J.; Ortega, A.M. Analysis of Separability of COVID-19 and Pneumonia in Chest X-ray Images by Means of Convolutional Neural Networks. Proceedings 2020, 54, 31. [Google Scholar] [CrossRef]
- Loey, M.; Smarandache, F.; Khalifa, N.E.M. Within the Lack of Chest COVID-19 X-ray Dataset: A Novel Detection Model Based on GAN and Deep Transfer Learning. Symmetry 2020, 12, 651. [Google Scholar] [CrossRef] [Green Version]
- Zulkifley, M.A.; Abdani, S.R.; Zulkifley, N.H. COVID-19 Screening Using a Lightweight Convolutional Neural Network with Generative Adversarial Network Data Augmentation. Symmetry 2020, 12, 1530. [Google Scholar] [CrossRef]
- Apostolopoulos, I.D.; Mpesiana, T.A. Covid-19: Automatic detection from X-ray images utilizing transfer learning with convolutional neural networks. Phys. Eng. Sci. Med. 2020, 43, 635–640. [Google Scholar] [CrossRef] [Green Version]
- Das, D.; Santosh, K.C.; Pal, U. Truncated inception net: COVID-19 outbreak screening using chest X-rays. Phys. Eng. Sci. Med. 2020, 43, 915–925. [Google Scholar] [CrossRef]
- Pratiwi, N.C.; Ibrahim, N.; Fu’Adah, Y.N.; Masykuroh, K. Computer-Aided Detection (CAD) for COVID-19 based on Chest X-ray Images using Convolutional Neural Network. IOP Conf. Ser. Mater. Sci. Eng. 2020, 982, 012004. [Google Scholar] [CrossRef]
- Hirano, H.; Koga, K.; Takemoto, K. Vulnerability of deep neural networks for detecting COVID-19 cases from chest X-ray images to universal adversarial attacks. PLoS ONE 2020, 15, e0243963. [Google Scholar] [CrossRef]
- Wang, L.; Wong, A. COVID-Net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. arXiv 2020, arXiv:2003.09871. [Google Scholar] [CrossRef]
- Wang, D.; Mo, J.; Zhou, G.; Xu, L.; Liu, Y. An efficient mixture of deep and machine learning models for COVID-19 diagnosis in chest X-ray images. PLoS ONE 2020, 15, e0242535. [Google Scholar] [CrossRef]
- Li, T.; Han, Z.; Wei, B.; Zheng, Y.; Hong, Y.; Cong, J. Robust screening of covid-19 from chest X-ray via discriminative cost-sensitive learning. arXiv 2020, arXiv:2004.12592. [Google Scholar]
- Sekeroglu, B.; Ozsahin, I. Detection of COVID-19 from Chest X-ray Images Using Convolutional Neural Networks. SLAS Technol. Transl. Life Sci. Innov. 2020, 25, 553–565. [Google Scholar] [CrossRef]
- Oh, Y.; Park, S.; Ye, J.C. Deep Learning COVID-19 Features on CXR Using Limited Training Data Sets. IEEE Trans. Med. Imaging 2020, 39, 2688–2700. [Google Scholar] [CrossRef] [PubMed]
- Sahinbas, K.; Catak, F.O. Transfer learning-based convolutional neural network for COVID-19 detection with X-ray images. In Data Science for COVID-19; Elsevier: Amsterdam, The Netherlands, 2021; pp. 451–466. [Google Scholar]
- Chowdhury, M.E.H.; Rahman, T.; Khandakar, A.; Mazhar, R.; Kadir, M.A.; Bin Mahbub, Z.; Islam, K.R.; Khan, M.S.; Iqbal, A.; Al Emadi, N.; et al. Can AI Help in Screening Viral and COVID-19 Pneumonia? IEEE Access 2020, 8, 132665–132676. [Google Scholar] [CrossRef]
- Sakib, S.; Tazrin, T.; Fouda, M.M.; Fadlullah, Z.M.; Guizani, M. DL-CRC: Deep Learning-Based Chest Radiograph Classification for COVID-19 Detection: A Novel Approach. IEEE Access 2020, 8, 171575–171589. [Google Scholar] [CrossRef]
- Shah, P.M.; Ullah, F.; Shah, D.; Gani, A.; Maple, C.; Wang, Y.; Shahid, A.; Abrar, M.; Islam, S.U. Deep GRU-CNN model for COVID-19 detection from chest X-rays data. IEEE Access 2021. [Google Scholar] [CrossRef]
- Iskanderani, A.I.; Mehedi, I.M.; Aljohani, A.J.; Shorfuzzaman, M.; Akther, F.; Palaniswamy, T.; Latif, S.A.; Latif, A.; Alam, A. Artificial Intelligence and Medical Internet of Things Framework for Diagnosis of Coronavirus Suspected Cases. J. Health Eng. 2021, 2021, 3277988. [Google Scholar] [CrossRef]
- Wang, W.; Li, Y.; Li, J.; Zhang, P.; Wang, X. Detecting COVID-19 in Chest X-ray Images via MCFF-Net. Comput. Intell. Neurosci. 2021, 2021, 3604900. [Google Scholar] [CrossRef]
- Shorfuzzaman, M.; Masud, M.; Alhumyani, H.; Anand, D.; Singh, A. Artificial Neural Network-Based Deep Learning Model for COVID-19 Patient Detection Using X-ray Chest Images. J. Health Eng. 2021, 2021, 5513679. [Google Scholar] [CrossRef] [PubMed]
- Reshi, A.A.; Rustam, F.; Mehmood, A.; Alhossan, A.; Alrabiah, Z.; Ahmad, A.; Alsuwailem, H.; Choi, G.S. An Efficient CNN Model for COVID-19 Disease Detection Based on X-ray Image Classification. Complex 2021, 2021, 6621607. [Google Scholar] [CrossRef]
- Alruwaili, M.; Shehab, A.; El-Ghany, S.A. COVID-19 Diagnosis Using an Enhanced Inception-ResNetV2 Deep Learning Model in CXR Images. J. Health Eng. 2021, 2021, 6658058. [Google Scholar] [CrossRef] [PubMed]
- Shukla, P.K.; Sandhu, J.K.; Ahirwar, A.; Ghai, D.; Maheshwary, P.; Shukla, P.K. Multiobjective Genetic Algorithm and Convolutional Neural Network Based COVID-19 Identification in Chest X-ray Images. Math. Probl. Eng. 2021, 2021, 7804540. [Google Scholar] [CrossRef]
- Taresh, M.M.; Zhu, N.; Ali, T.A.A.; Hameed, A.S.; Mutar, M.L. Transfer Learning to Detect COVID-19 Automatically from X-ray Images Using Convolutional Neural Networks. Int. J. Biomed. Imaging 2021, 2021, 8828404. [Google Scholar] [CrossRef]
- Kaur, M.; Kumar, V.; Yadav, V.; Singh, D.; Kumar, N.; Das, N.N. Metaheuristic-based Deep COVID-19 Screening Model from Chest X-ray Images. J. Health Eng. 2021, 2021, 8829829. [Google Scholar] [CrossRef]
- Ahmad, F.; Farooq, A.; Ghani, M.U. Deep Ensemble Model for Classification of Novel Coronavirus in Chest X-ray Images. Comput. Intell. Neurosci. 2021, 2021, 8890226. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.D.K.; Ahmed, S.; Abdullah, Z.M.E.; Khan, M.M.; Anand, D.; Singh, A.; AlZain, M.; Masud, M. Deep Learning Approaches for Detecting Pneumonia in COVID-19 Patients by Analyzing Chest X-ray Images. Math. Probl. Eng. 2021, 2021, 9929274. [Google Scholar] [CrossRef]
- Muhammad, Y.; Alshehri, M.D.; Alenazy, W.M.; Hoang, T.V.; Alturki, R. Identification of Pneumonia Disease Applying an Intelligent Computational Framework Based on Deep Learning and Machine Learning Techniques. Mob. Inf. Syst. 2021, 2021, 9989237. [Google Scholar] [CrossRef]
- Pandit, M.; Banday, S.; Naaz, R.; Chishti, M. Automatic detection of COVID-19 from chest radiographs using deep learning. Radiography 2021, 27, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Kedia, P.; Katarya, R. CoVNet-19: A Deep Learning model for the detection and analysis of COVID-19 patients. Appl. Soft Comput. 2021, 104, 107184. [Google Scholar] [CrossRef]
- Saha, P.; Sadi, M.S.; Islam, M. EMCNet: Automated COVID-19 diagnosis from X-ray images using convolutional neural network and ensemble of machine learning classifiers. Inform. Med. Unlocked 2021, 22, 100505. [Google Scholar] [CrossRef] [PubMed]
- Panahi, A.H.; Rafiei, A.; Rezaee, A. FCOD: Fast COVID-19 Detector based on deep learning techniques. Inform. Med. Unlocked 2021, 22, 100506. [Google Scholar] [CrossRef]
- Xu, Y.; Lam, H.-K.; Jia, G. MANet: A two-stage deep learning method for classification of COVID-19 from Chest X-ray images. Neurocomputing 2021, 443, 96–105. [Google Scholar] [CrossRef]
- Karakanis, S.; Leontidis, G. Lightweight deep learning models for detecting COVID-19 from chest X-ray images. Comput. Biol. Med. 2021, 130, 104181. [Google Scholar] [CrossRef] [PubMed]
- Alorf, A. The Practicality of Deep Learning Algorithms in COVID-19 Detection: Application to Chest X-ray Images. Algorithms 2021, 14, 183. [Google Scholar] [CrossRef]
- Ben Jabra, M.; Koubaa, A.; Benjdira, B.; Ammar, A.; Hamam, H. COVID-19 Diagnosis in Chest X-rays Using Deep Learning and Majority Voting. Appl. Sci. 2021, 11, 2884. [Google Scholar] [CrossRef]
- Ahrabi, S.S.; Scarpiniti, M.; Baccarelli, E.; Momenzadeh, A. An Accuracy vs. Complexity Comparison of Deep Learning Architectures for the Detection of COVID-19 Disease. Computation 2021, 9, 3. [Google Scholar] [CrossRef]
- Luján-García, J.; Villuendas-Rey, Y.; López-Yáñez, I.; Camacho-Nieto, O.; Yáñez-Márquez, C. NanoChest-Net: A Simple Convolutional Network for Radiological Studies Classification. Diagnostics 2021, 11, 775. [Google Scholar] [CrossRef]
- Karbhari, Y.; Basu, A.; Geem, Z.W.; Han, G.-T.; Sarkar, R. Generation of Synthetic Chest X-ray Images and Detection of COVID-19: A Deep Learning Based Approach. Diagnostics 2021, 11, 895. [Google Scholar] [CrossRef] [PubMed]
- Khishe, M.; Caraffini, F.; Kuhn, S. Evolving Deep Learning Convolutional Neural Networks for Early COVID-19 Detection in Chest X-ray Images. Mathematics 2021, 9, 1002. [Google Scholar] [CrossRef]
- Alam, N.A.; Ahsan, M.; Based, A.; Haider, J.; Kowalski, M. COVID-19 Detection from Chest X-ray Images Using Feature Fusion and Deep Learning. Sensors 2021, 21, 1480. [Google Scholar] [CrossRef]
- Vantaggiato, E.; Paladini, E.; Bougourzi, F.; Distante, C.; Hadid, A.; Taleb-Ahmed, A. COVID-19 Recognition Using Ensemble-CNNs in Two New Chest X-ray Databases. Sensors 2021, 21, 1742. [Google Scholar] [CrossRef]
- Muñoz-Saavedra, L.; Civit-Masot, J.; Luna-Perejón, F.; Domínguez-Morales, M.; Civit, A. Does Two-Class Training Extract Real Features? A COVID-19 Case Study. Appl. Sci. 2021, 11, 1424. [Google Scholar] [CrossRef]
- Barua, P.; Gowdh, N.M.; Rahmat, K.; Ramli, N.; Ng, W.; Chan, W.; Kuluozturk, M.; Dogan, S.; Baygin, M.; Yaman, O.; et al. Automatic COVID-19 Detection Using Exemplar Hybrid Deep Features with X-ray Images. Int. J. Environ. Res. Public Health 2021, 18, 8052. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.; Abdelsamea, M.M.; Gaber, M.M. Classification of COVID-19 in chest X-ray images using DeTraC deep convolutional neural network. Appl. Intell. 2021, 51, 854–864. [Google Scholar] [CrossRef]
- Gaur, L.; Bhatia, U.; Jhanjhi, N.Z.; Muhammad, G.; Masud, M. Medical image-based detection of COVID-19 using Deep Convolution Neural Networks. Multimed. Syst. 2021, 1–10. [Google Scholar] [CrossRef]
- Luz, E.; Silva, P.; Silva, R.; Silva, L.; Guimarães, J.; Miozzo, G.; Moreira, G.; Menotti, D. Towards an effective and efficient deep learning model for COVID-19 patterns detection in X-ray images. Res. Biomed. Eng. 2021, 1–14. [Google Scholar] [CrossRef]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic detection of coronavirus disease (COVID-19) using X-ray images and deep convolutional neural networks. Pattern Anal. Appl. 2021, 24, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Rajagopal, R. Comparative Analysis of COVID-19 X-ray Images Classification Using Convolutional Neural Network, Transfer Learning, and Machine Learning Classifiers Using Deep Features. Pattern Recognit. Image Anal. 2021, 31, 313–322. [Google Scholar] [CrossRef]
- Castiglioni, I.; Ippolito, D.; Interlenghi, M.; Monti, C.B.; Salvatore, C.; Schiaffino, S.; Polidori, A.; Gandola, D.; Messa, C.; Sardanelli, F. Machine learning applied on chest X-ray can aid in the diagnosis of COVID-19: A first experience from Lombardy, Italy. Eur. Radiol. Exp. 2021, 5, 1–10. [Google Scholar] [CrossRef]
- Sarkar, A.; Vandenhirtz, J.; Nagy, J.; Bacsa, D.; Riley, M. Identification of Images of COVID-19 from Chest X-rays Using Deep Learning: Comparing COGNEX VisionPro Deep Learning 1.0™ Software with Open Source Convolutional Neural Networks. SN Comput. Sci. 2021, 2, 1–16. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, P.M.; Carneiro, P.C.; Oliveira, M.M.; Pereira, G.M.; Junior, C.A.D.C.; De Moura, L.V.; Mattjie, C.; Da Silva, A.M.M.; Patrocinio, A.C. COVID-19 classification in X-ray chest images using a new convolutional neural network: CNN-COVID. Res. Biomed. Eng. 2021, 1–11. [Google Scholar] [CrossRef]
- Turkoglu, M. COVIDetectioNet: COVID-19 diagnosis system based on X-ray images using features selected from pre-learned deep features ensemble. Appl. Intell. 2021, 51, 1213–1226. [Google Scholar] [CrossRef] [PubMed]
- Umer, M.; Ashraf, I.; Ullah, S.; Mehmood, A.; Choi, G.S. COVINet: A convolutional neural network approach for predicting COVID-19 from chest X-ray images. J. Ambient. Intell. Humaniz. Comput. 2021, 1–13. [Google Scholar] [CrossRef]
- Madaan, V.; Roy, A.; Gupta, C.; Agrawal, P.; Sharma, A.; Bologa, C.; Prodan, R. XCOVNet: Chest X-ray Image Classification for COVID-19 Early Detection Using Convolutional Neural Networks. New Gener. Comput. 2021, 39, 583–597. [Google Scholar] [CrossRef] [PubMed]
- Das, A.K.; Ghosh, S.; Thunder, S.; Dutta, R.; Agarwal, S.; Chakrabarti, A. Automatic COVID-19 detection from X-ray images using ensemble learning with convolutional neural network. Pattern Anal. Appl. 2021, 24, 1111–1124. [Google Scholar] [CrossRef]
- Agrawal, T.; Choudhary, P. FocusCovid: Automated COVID-19 detection using deep learning with chest X-ray images. Evol. Syst. 2021, 1–15. [Google Scholar] [CrossRef]
- Swapnarekha, H.; Behera, H.S.; Roy, D.; Das, S.; Nayak, J. Competitive Deep Learning Methods for COVID-19 Detection using X-ray Images. J. Inst. Eng. Ser. B 2021, 102, 1177–1190. [Google Scholar] [CrossRef]
- Aradhya, V.N.M.; Mahmud, M.; Guru, D.S.; Agarwal, B.; Kaiser, M.S. One-shot Cluster-Based Approach for the Detection of COVID–19 from Chest X–ray Images. Cogn. Comput. 2021, 13, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Gupta, M.; Taneja, S.; Hemanth, D.J. Deep learning based detection and analysis of COVID-19 on chest X-ray images. Appl. Intell. 2021, 51, 1690–1700. [Google Scholar] [CrossRef]
- Maior, C.B.S.; Santana, J.M.M.; Lins, I.D.; Moura, M.J.C. Convolutional neural network model based on radiological images to support COVID-19 diagnosis: Evaluating database biases. PLoS ONE 2021, 16, e0247839. [Google Scholar] [CrossRef] [PubMed]
- Salam, M.A.; Taha, S.; Ramadan, M. COVID-19 detection using federated machine learning. PLoS ONE 2021, 16, e0252573. [Google Scholar] [CrossRef]
- Ahsan, M.; Ahad, T.; Soma, F.A.; Paul, S.; Chowdhury, A.; Luna, S.A.; Yazdan, M.M.S.; Rahman, A.; Siddique, Z.; Huebner, P. Detecting SARS-CoV-2 From Chest X-ray Using Artificial Intelligence. IEEE Access 2021, 9, 35501–35513. [Google Scholar] [CrossRef]
- Zhou, J.; Jing, B.; Wang, Z.; Xin, H.; Tong, H. SODA: Detecting COVID-19 in Chest X-rays with Semi-supervised Open Set Domain Adaptation. IEEE/ACM Trans. Comput. Biol. Bioinform. 2021, 1. [Google Scholar] [CrossRef]
- Mohagheghi, S.; Alizadeh, M.; Safavi, S.M.; Foruzan, A.H.; Chen, Y.-W. Integration of CNN, CBMIR, and Visualization Techniques for Diagnosis and Quantification of Covid-19 Disease. IEEE J. Biomed. Health Inform. 2021, 25, 1873–1880. [Google Scholar] [CrossRef]
- Oyelade, O.N.; Ezugwu, A.E.-S.; Chiroma, H. CovFrameNet: An Enhanced Deep Learning Framework for COVID-19 Detection. IEEE Access 2021, 9, 77905–77919. [Google Scholar] [CrossRef]
- Abbas, A.; Abdelsamea, M.M.; Gaber, M.M. 4S-DT: Self-Supervised Super Sample Decomposition for Transfer Learning With Application to COVID-19 Detection. IEEE Trans. Neural Netw. Learn. Syst. 2021, 32, 2798–2808. [Google Scholar] [CrossRef]
- Zhou, C.; Song, J.; Zhou, S.; Zhang, Z.; Xing, J. COVID-19 Detection Based on Image Regrouping and Resnet-SVM Using Chest X-ray Images. IEEE Access 2021, 9, 81902–81912. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.; Yang, Q.; Fu, Y.; Tian, M.; Zhuo, C. RCoNet: Deformable Mutual Information Maximization and High-Order Uncertainty-Aware Learning for Robust COVID-19 Detection. IEEE Trans. Neural Netw. Learn. Syst. 2021, 32, 3401–3411. [Google Scholar] [CrossRef] [PubMed]
- Ardakani, A.A.; Kanafi, A.R.; Acharya, U.R.; Khadem, N.; Mohammadi, A. Application of deep learning technique to manage COVID-19 in routine clinical practice using CT images: Results of 10 convolutional neural networks. Comput. Biol. Med. 2020, 121, 103795. [Google Scholar] [CrossRef]
- Silva, P.; Luz, E.; Silva, G.; Moreira, G.; Silva, R.; Lucio, D.; Menotti, D. COVID-19 detection in CT images with deep learning: A voting-based scheme and cross-datasets analysis. Inform. Med. Unlocked 2020, 20, 100427. [Google Scholar] [CrossRef]
- Li, T.; Wei, W.; Cheng, L.; Zhao, S.; Xu, C.; Zhang, X.; Zeng, Y.; Gu, J. Computer-Aided Diagnosis of COVID-19 CT Scans Based on Spatiotemporal Information Fusion. J. Health Eng. 2021, 2021, 6649591. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zhong, Y.; Deng, Y.; Tang, X.; Li, X. CoSinGAN: Learning COVID-19 Infection Segmentation from a Single Radiological Image. Diagnostics 2020, 10, 901. [Google Scholar] [CrossRef]
- Wan, Y.; Zhou, H.; Zhang, X. An Interpretation Architecture for Deep Learning Models with the Application of COVID-19 Diagnosis. Entropy 2021, 23, 204. [Google Scholar] [CrossRef] [PubMed]
- Gifani, P.; Shalbaf, A.; Vafaeezadeh, M. Automated detection of COVID-19 using ensemble of transfer learning with deep convolutional neural network based on CT scans. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 115–123. [Google Scholar] [CrossRef]
- Loey, M.; Manogaran, G.; Khalifa, N.E.M. A deep transfer learning model with classical data augmentation and CGAN to detect COVID-19 from chest CT radiography digital images. Neural Comput. Appl. 2020, 1–13. [Google Scholar] [CrossRef]
- Singh, D.; Kumar, V.; Kaur, M. Densely connected convolutional networks-based COVID-19 screening model. Appl. Intell. 2021, 51, 3044–3051. [Google Scholar] [CrossRef]
- Fan, D.-P.; Zhou, T.; Ji, G.-P.; Zhou, Y.; Chen, G.; Fu, H.; Shen, J.; Shao, L. Inf-Net: Automatic COVID-19 Lung Infection Segmentation From CT Images. IEEE Trans. Med. Imaging 2020, 39, 2626–2637. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, X.; Huo, J.; Xia, L.; Shan, F.; Liu, J.; Mo, Z.; Yan, F.; Ding, Z.; Yang, Q.; Song, B.; et al. Dual-Sampling Attention Network for Diagnosis of COVID-19 From Community Acquired Pneumonia. IEEE Trans. Med. Imaging 2020, 39, 2595–2605. [Google Scholar] [CrossRef]
- Zhang, Y.-D.; Satapathy, S.C.; Zhu, L.-Y.; Gorriz, J.M.; Wang, S.-H. A seven-layer convolutional neural network for chest CT based COVID-19 diagnosis using stochastic pooling. IEEE Sensors J. 2020, 1. [Google Scholar] [CrossRef]
- Qian, X.; Fu, H.; Shi, W.; Chen, T.; Fu, Y.; Shan, F.; Xue, X. M3Lung-Sys: A Deep Learning System for Multi-Class Lung Pneumonia Screening From CT Imaging. IEEE J. Biomed. Health Inform. 2020, 24, 3539–3550. [Google Scholar] [CrossRef]
- Ozyurt, F.; Tuncer, T.; Subasi, A. An automated COVID-19 detection based on fused dynamic exemplar pyramid feature extraction and hybrid feature selection using deep learning. Comput. Biol. Med. 2021, 132, 104356. [Google Scholar] [CrossRef]
- Rohila, V.S.; Gupta, N.; Kaul, A.; Sharma, D.K. Deep learning assisted COVID-19 detection using full CT-scans. Internet Things 2021, 14, 100377. [Google Scholar] [CrossRef]
- Shiri, I.; Sorouri, M.; Geramifar, P.; Nazari, M.; Abdollahi, M.; Salimi, Y.; Khosravi, B.; Askari, D.; Aghaghazvini, L.; Hajianfar, G.; et al. Machine learning-based prognostic modeling using clinical data and quantitative radiomic features from chest CT images in COVID-19 patients. Comput. Biol. Med. 2021, 132, 104304. [Google Scholar] [CrossRef]
- Priya, C.; Fathima, S.S.S.; Kirubanandasarathy, N.; Valanarasid, A.; Begam, M.S.; Aiswarya, N. Automatic Optimized CNN Based COVID-19 Lung Infection Segmentation from CT Image; Elsevier BV: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Wu, Z.; Li, L.; Jin, R.; Liang, L.; Hu, Z.; Tao, L.; Han, Y.; Feng, W.; Zhou, D.; Li, W.; et al. Texture feature-based machine learning classifier could assist in the diagnosis of COVID-19. Eur. J. Radiol. 2021, 137, 109602. [Google Scholar] [CrossRef]
- Yu, X.; Lu, S.; Guo, L.; Wang, S.-H.; Zhang, Y.-D. ResGNet-C: A graph convolutional neural network for detection of COVID-19. Neurocomputing 2021, 452, 592–605. [Google Scholar] [CrossRef]
- Turkoglu, M. COVID-19 Detection System Using Chest CT Images and Multiple Kernels-Extreme Learning Machine Based on Deep Neural Network. IRBM 2021, 42, 207–214. [Google Scholar] [CrossRef]
- He, K.; Zhao, W.; Xie, X.; Ji, W.; Liu, M.; Tang, Z.; Shi, Y.; Shi, F.; Gao, Y.; Liu, J.; et al. Synergistic learning of lung lobe segmentation and hierarchical multi-instance classification for automated severity assessment of COVID-19 in CT images. Pattern Recognit. 2021, 113, 107828. [Google Scholar] [CrossRef]
- Gao, K.; Su, J.; Jiang, Z.; Zeng, L.-L.; Feng, Z.; Shen, H.; Rong, P.; Xu, X.; Qin, J.; Yang, Y.; et al. Dual-branch combination network (DCN): Towards accurate diagnosis and lesion segmentation of COVID-19 using CT images. Med. Image Anal. 2021, 67, 101836. [Google Scholar] [CrossRef]
- Serte, S.; Demirel, H. Deep learning for diagnosis of COVID-19 using 3D CT scans. Comput. Biol. Med. 2021, 132, 104306. [Google Scholar] [CrossRef] [PubMed]
- Perumal, V.; Narayanan, V.; Rajasekar, S.J.S. Prediction of COVID-19 with Computed Tomography Images using Hybrid Learning Techniques. Dis. Markers 2021, 2021, 5522729. [Google Scholar] [CrossRef] [PubMed]
- Helwan, A.; Ma’Aitah, M.K.S.; Hamdan, H.; Ozsahin, D.U.; Tuncyurek, O. Radiologists versus Deep Convolutional Neural Networks: A Comparative Study for Diagnosing COVID-19. Comput. Math. Methods Med. 2021, 2021, 5527271. [Google Scholar] [CrossRef]
- Lawton, S.; Viriri, S. Detection of COVID-19 from CT Lung Scans Using Transfer Learning. Comput. Intell. Neurosci. 2021, 2021, 5527923. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Tan, W.; Liu, P.; Zhou, Q.; Yang, J. Classification of COVID-19 Chest CT Images Based on Ensemble Deep Learning. J. Health Eng. 2021, 2021, 5528441. [Google Scholar] [CrossRef] [PubMed]
- Salamh, A.B.S.; Salamah, A.A.; Akyüz, H.I. A Study of a New Technique of the CT Scan View and Disease Classification Protocol Based on Level Challenges in Cases of Coronavirus Disease. Radiol. Res. Pract. 2021, 2021, 5554408. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.-H.; Zhang, Y.; Cheng, X.; Zhang, X.; Zhang, Y.-D. PSSPNN: PatchShuffle Stochastic Pooling Neural Network for an Explainable Diagnosis of COVID-19 with Multiple-Way Data Augmentation. Comput. Math. Methods Med. 2021, 2021, 6633755. [Google Scholar] [CrossRef]
- Zheng, B.; Cai, Y.; Zeng, F.; Lin, M.; Zheng, J.; Chen, W.; Qin, G.; Guo, Y. An Interpretable Model-Based Prediction of Severity and Crucial Factors in Patients with COVID-19. BioMed Res. Int. 2021, 2021, 8840835. [Google Scholar] [CrossRef]
- Zheng, R.; Zheng, Y.; Dong-Ye, C. Improved 3D U-Net for COVID-19 Chest CT Image Segmentation. Sci. Program. 2021, 2021, 9999368. [Google Scholar] [CrossRef]
- Oluwasanmi, A.; Aftab, M.U.; Qin, Z.; Ngo, S.T.; Van Doan, T.; Nguyen, S.B. Transfer Learning and Semisupervised Adversarial Detection and Classification of COVID-19 in CT Images. Complexity 2021, 2021, 6680455. [Google Scholar] [CrossRef]
- Manzo, M.; Pellino, S. Fighting Together against the Pandemic: Learning Multiple Models on Tomography Images for COVID-19 Diagnosis. AI 2021, 2, 261–273. [Google Scholar] [CrossRef]
- Singh, V.K.; Abdel-Nasser, M.; Pandey, N.; Puig, D. LungINFseg: Segmenting COVID-19 Infected Regions in Lung CT Images Based on a Receptive-Field-Aware Deep Learning Framework. Diagnostics 2021, 11, 158. [Google Scholar] [CrossRef]
- Qiblawey, Y.; Tahir, A.; Chowdhury, M.; Khandakar, A.; Kiranyaz, S.; Rahman, T.; Ibtehaz, N.; Mahmud, S.; Maadeed, S.; Musharavati, F.; et al. Detection and Severity Classification of COVID-19 in CT Images Using Deep Learning. Diagnostics 2021, 11, 893. [Google Scholar] [CrossRef]
- Chatzitofis, A.; Cancian, P.; Gkitsas, V.; Carlucci, A.; Stalidis, P.; Albanis, G.; Karakottas, A.; Semertzidis, T.; Daras, P.; Giannitto, C.; et al. Volume-of-Interest Aware Deep Neural Networks for Rapid Chest CT-Based COVID-19 Patient Risk Assessment. Int. J. Environ. Res. Public Health 2021, 18, 2842. [Google Scholar] [CrossRef]
- Alshazly, H.; Linse, C.; Barth, E.; Martinetz, T. Explainable COVID-19 Detection Using Chest CT Scans and Deep Learning. Sensors 2021, 21, 455. [Google Scholar] [CrossRef]
- Voulodimos, A.; Protopapadakis, E.; Katsamenis, I.; Doulamis, A.; Doulamis, N. A Few-Shot U-Net Deep Learning Model for COVID-19 Infected Area Segmentation in CT Images. Sensors 2021, 21, 2215. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, S.; Panigrahi, B.K.; Dey, N.; Rajinikanth, V.; Gandhi, T.K. Deep transfer learning-based automated detection of COVID-19 from lung CT scan slices. Appl. Intell. 2021, 51, 571–585. [Google Scholar] [CrossRef]
- Garain, A.; Basu, A.; Giampaolo, F.; Velasquez, J.D.; Sarkar, R. Detection of COVID-19 from CT scan images: A spiking neural network-based approach. Neural Comput. Appl. 2021, 33, 12591–12604. [Google Scholar] [CrossRef]
- Li, D.; Fu, Z.; Xu, J. Stacked-autoencoder-based model for COVID-19 diagnosis on CT images. Appl. Intell. 2021, 51, 2805–2817. [Google Scholar] [CrossRef]
- Rezaeijo, S.M.; Ghorvei, M.; Abedi-Firouzjah, R.; Mojtahedi, H.; Zarch, H.E. Detecting COVID-19 in chest images based on deep transfer learning and machine learning algorithms. Egypt. J. Radiol. Nucl. Med. 2021, 52, 1–12. [Google Scholar] [CrossRef]
- Sen, S.; Saha, S.; Chatterjee, S.; Mirjalili, S.; Sarkar, R. A bi-stage feature selection approach for COVID-19 prediction using chest CT images. Appl. Intell. 2021, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.; Keniya, R.; Shridharani, A.; Punjabi, M.; Shah, J.; Mehendale, N. Diagnosis of COVID-19 using CT scan images and deep learning techniques. Emerg. Radiology 2021, 28, 497–505. [Google Scholar] [CrossRef]
- Tan, W.; Liu, P.; Li, X.; Liu, Y.; Zhou, Q.; Chen, C.; Gong, Z.; Yin, X.; Zhang, Y. Classification of COVID-19 pneumonia from chest CT images based on reconstructed super-resolution images and VGG neural network. Health Inf. Sci. Syst. 2021, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ardakani, A.A.; Acharya, U.R.; Habibollahi, S.; Mohammadi, A. COVIDiag: A clinical CAD system to diagnose COVID-19 pneumonia based on CT findings. Eur. Radiol. 2021, 31, 121–130. [Google Scholar] [CrossRef]
- Yasar, H.; Ceylan, M. A novel comparative study for detection of Covid-19 on CT lung images using texture analysis, machine learning, and deep learning methods. Multimed. Tools Appl. 2021, 80, 5423–5447. [Google Scholar] [CrossRef] [PubMed]
- Elmuogy, S.; Hikal, N.A.; Hassan, E. An efficient technique for CT scan images classification of COVID-19. J. Intell. Fuzzy Syst. 2021, 40, 5225–5238. [Google Scholar] [CrossRef]
- Elaziz, M.A.; Al-Qaness, M.A.A.; Zaid, E.O.A.; Lu, S.; Ibrahim, R.A.; Ewees, A.A. Automatic clustering method to segment COVID-19 CT images. PLoS ONE 2021, 16, e0244416. [Google Scholar] [CrossRef]
- Han, C.H.; Kim, M.; Kwak, J.T. Semi-supervised learning for an improved diagnosis of COVID-19 in CT images. PLoS ONE 2021, 16, e0249450. [Google Scholar] [CrossRef]
- Yousefzadeh, M.; Esfahanian, P.; Movahed, S.M.S.; Gorgin, S.; Rahmati, D.; Abedini, A.; Nadji, S.A.; Haseli, S.; Karam, M.B.; Kiani, A.; et al. ai-corona: Radiologist-assistant deep learning framework for COVID-19 diagnosis in chest CT scans. PLoS ONE 2021, 16, e0250952. [Google Scholar] [CrossRef]
- Yan, Q.; Wang, B.; Gong, D.; Luo, C.; Zhao, W.; Shen, J.; Ai, J.; Shi, Q.; Zhang, Y.; Jin, S.; et al. COVID-19 Chest CT Image Segmentation Network by Multi-Scale Fusion and Enhancement Operations. IEEE Trans. Big Data 2021, 7, 13–24. [Google Scholar] [CrossRef]
- Paluru, N.; Dayal, A.; Jenssen, H.B.; Sakinis, T.; Cenkeramaddi, L.R.; Prakash, J.; Yalavarthy, P.K. Anam-Net: Anamorphic Depth Embedding-Based Lightweight CNN for Segmentation of Anomalies in COVID-19 Chest CT Images. IEEE Trans. Neural Netw. Learn. Syst. 2021, 32, 932–946. [Google Scholar] [CrossRef]
- Muhammad, G.; Hossain, M.S. COVID-19 and Non-COVID-19 Classification using Multi-layers Fusion From Lung Ultrasound Images. Inf. Fusion 2021, 72, 80–88. [Google Scholar] [CrossRef]
- Dastider, A.G.; Sadik, F.; Fattah, S.A. An integrated autoencoder-based hybrid CNN-LSTM model for COVID-19 severity prediction from lung ultrasound. Comput. Biol. Med. 2021, 132, 104296. [Google Scholar] [CrossRef]
- Panwar, H.; Gupta, P.; Siddiqui, M.K.; Morales-Menendez, R.; Bhardwaj, P.; Singh, V. A deep learning and grad-CAM based color visualization approach for fast detection of COVID-19 cases using chest X-ray and CT-Scan images. Chaos Solitons Fractals 2020, 140, 110190. [Google Scholar] [CrossRef]
- Ibrahim, D.M.; Elshennawy, N.M.; Sarhan, A.M. Deep-chest: Multi-classification deep learning model for diagnosing COVID-19, pneumonia, and lung cancer chest diseases. Comput. Biol. Med. 2021, 132, 104348. [Google Scholar] [CrossRef] [PubMed]
- Elpeltagy, M.; Sallam, H. Automatic prediction of COVID− 19 from chest images using modified ResNet50. Multimed. Tools Appl. 2021, 1–13. [Google Scholar] [CrossRef]
- Gilanie, G.; Bajwa, U.I.; Waraich, M.M.; Asghar, M.; Kousar, R.; Kashif, A.; Aslam, R.S.; Qasim, M.M.; Rafique, H. Coronavirus (COVID-19) detection from chest radiology images using convolutional neural networks. Biomed. Signal Process. Control. 2021, 66, 102490. [Google Scholar] [CrossRef] [PubMed]
- Saha, P.; Mukherjee, D.; Singh, P.K.; Ahmadian, A.; Ferrara, M.; Sarkar, R. GraphCovidNet: A graph neural network based model for detecting COVID-19 from CT scans and X-rays of chest. Sci. Rep. 2021, 11, 1–16. [Google Scholar] [CrossRef]
- Perumal, V.; Narayanan, V.; Rajasekar, S.J.S. Detection of COVID-19 using CXR and CT images using Transfer Learning and Haralick features. Appl. Intell. 2021, 51, 341–358. [Google Scholar] [CrossRef]
- Lascu, M.-R. Deep Learning in Classification of Covid-19 Coronavirus, Pneumonia and Healthy Lungs on CXR and CT Images. J. Med. Biol. Eng. 2021, 10, 1–9. [Google Scholar] [CrossRef]
- Kassania, S.H.; Kassanib, P.H.; Wesolowskic, M.J.; Schneidera, K.A.; Detersa, R. Automatic Detection of Coronavirus Disease (COVID-19) in X-ray and CT Images: A Machine Learning Based Approach. Biocybern. Biomed. Eng. 2021, 41, 867–879. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhao, G.; Tao, Y.; Zhai, P.; Chen, H.; He, H.; Cai, T. Multi-task contrastive learning for automatic CT and X-ray diagnosis of COVID-19. Pattern Recognit. 2021, 114, 107848. [Google Scholar] [CrossRef]
- Imani, M. Automatic diagnosis of coronavirus (COVID-19) using shape and texture characteristics extracted from X-ray and CT-Scan images. Biomed. Signal Process. Control. 2021, 68, 102602. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, H.; Ghosh, S.; Dhar, A.; Obaidullah, S.M.; Santosh, K.C.; Roy, K. Deep neural network to detect COVID-19: One architecture for both CT Scans and Chest X-rays. Appl. Intell. 2021, 51, 2777–2789. [Google Scholar] [CrossRef] [PubMed]
- Pal, B.; Gupta, D.; Rashed-Al-Mahfuz, M.; Alyami, S.; Moni, M. Vulnerability in Deep Transfer Learning Models to Adversarial Fast Gradient Sign Attack for COVID-19 Prediction from Chest Radiography Images. Appl. Sci. 2021, 11, 4233. [Google Scholar] [CrossRef]
- Aminu, M.; Ahmad, N.A.; Noor, M.H.M. Covid-19 detection via deep neural network and occlusion sensitivity maps. Alex. Eng. J. 2021, 60, 4829–4855. [Google Scholar] [CrossRef]
- Mittal, H.; Pandey, A.C.; Pal, R.; Tripathi, A. A new clustering method for the diagnosis of CoVID19 using medical images. Appl. Intell. 2021, 51, 2988–3011. [Google Scholar] [CrossRef]
- Horry, M.J.; Chakraborty, S.; Paul, M.; Ulhaq, A.; Pradhan, B.; Saha, M.; Shukla, N. COVID-19 Detection Through Transfer Learning Using Multimodal Imaging Data. IEEE Access 2020, 8, 149808–149824. [Google Scholar] [CrossRef]
- Gudigar, A.; Raghavendra, U.; Hegde, A.; Menon, G.; Molinari, F.; Ciaccio, E.; Acharya, U. Automated Detection and Screening of Traumatic Brain Injury (TBI) Using Computed Tomography Images: A Comprehensive Review and Future Perspectives. Int. J. Environ. Res. Public Health 2021, 18, 6499. [Google Scholar] [CrossRef]
- Raghavendra, U.; Gudigar, A.; Rao, N.; Ciaccio, J.; Ng, E.Y.K. Rajendra Acharya, Computer-aided di-agnosis for the identification of breast cancer using thermogram images: A comprehensive review. Infrared Phys. Technol. 2019, 102, 103041. [Google Scholar] [CrossRef]
- Gudigar, A.; Raghavendra, U.; Hegde, A.; Kalyani, M.; Ciaccio, E.J.; Rajendra, A.U. Brain pathology identi-fication using computer aided diagnostic tool: A systematic review. Comput. Methods Programs Biomed. 2020, 187, 105205. [Google Scholar] [CrossRef] [PubMed]
- Abilash, V.; Geoffrey, V.; Krishna, S.B.R. Coronavirus Pandemic Analysis Using Deep Learning Techniques A Study. In Proceedings of the 2021 5th International Conference on Trends in Electronics and Informatics (ICOEI), Tirunelveli, India, 3–5 June 2021; pp. 875–880. [Google Scholar]
- Sri, R.S.; Pushpa, A.M. Systematic Study on Diagnosis of Lung Disorders using Machine Learning and Deep Learning Algorithms. In Proceedings of the 2021 Seventh International conference on Bio Signals, Images, and Instrumentation (ICBSII), Kalavakkam, Tamil Nadu, India, 25–27 March 2021; pp. 1–8. [Google Scholar]
- Mohammad-Rahimi, H.; Nadimi, M.; Ghalyanchi-Langeroudi, A.; Taheri, M.; Ghafouri-Fard, S. Application of Machine Learning in Diagnosis of COVID-19 Through X-ray and CT Images: A Scoping Review. Front. Cardiovasc. Med. 2021, 8, 185. [Google Scholar] [CrossRef] [PubMed]
- Desai, S.B.; Pareek, A.; Lungren, M.P. Deep learning and its role in COVID-19 medical imaging. Intell. Med. 2020, 3, 100013. [Google Scholar] [CrossRef]
- Gazzah, S.; Bencharef, O. A Survey on how computer vision can response to urgent need to contribute in COVID-19 pandemics. In Proceedings of the 2020 International Conference on Intelligent Systems and Computer Vision (ISCV), Fez, Morocco, 9–11 June 2020; pp. 1–5. [Google Scholar]
- Signoroni, A.; Savardi, M.; Benini, S.; Adami, N.; Leonardi, R.; Gibellini, P.; Vaccher, F.; Ravanelli, M.; Borghesi, A.; Maroldi, R.; et al. BS-Net: Learning COVID-19 pneumonia severity on a large chest X-ray dataset. Med. Image Anal. 2021, 71, 102046. [Google Scholar] [CrossRef]
- Zhang, H.-T.; Zhang, J.-S.; Nan, Y.-D.; Zhao, Y.; Fu, E.-Q.; Xie, Y.-H.; Liu, W.; Li, W.-P.; Zhang, H.-J.; Jiang, H.; et al. Automated detection and quantification of COVID-19 pneumonia: CT imaging analysis by a deep learning-based software. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2525–2532. [Google Scholar] [CrossRef]
- Goncharov, M.; Pisov, M.; Shevtsov, A.; Shirokikh, B.; Kurmukov, A.; Blokhin, I.; Chernina, V.; Solovev, A.; Gombolevskiy, V.; Morozov, S.; et al. CT-Based COVID-19 triage: Deep multitask learning improves joint identification and severity quantification. Med. Image Anal. 2021, 71, 102054. [Google Scholar] [CrossRef] [PubMed]
- Oulefki, A.; Agaian, S.; Trongtirakul, T.; Laouar, A.K. Automatic COVID-19 lung infected region segmentation and measurement using CT-scans images. Pattern Recognit. 2021, 114, 107747. [Google Scholar] [CrossRef]
- Giordano, F.; Ippolito, E.; Quattrocchi, C.; Greco, C.; Mallio, C.; Santo, B.; D’Alessio, P.; Crucitti, P.; Fiore, M.; Zobel, B.; et al. Radiation-Induced Pneumonitis in the Era of the COVID-19 Pandemic: Artificial Intelligence for Differential Diagnosis. Cancers 2021, 13, 1960. [Google Scholar] [CrossRef]
- Shoeibi, A.; Khodatars, M.; Alizadehsani, R.; Ghassemi, N.; Jafari, M.; Moridian, P.; Khadem, A.; Sadeghi, D.; Hussain, S.; Zare, A.; et al. Automated detection and forecasting of covid-19 using deep learning techniques: A review. arXiv 2020, arXiv:2007.10785. [Google Scholar]
- Sharifrazi, D.; Alizadehsani, R.; Roshanzamir, M.; Joloudari, J.H.; Shoeibi, A.; Jafari, M.; Hussain, S.; Sani, Z.A.; Hasanzadeh, F.; Khozeimeh, F.; et al. Fusion of convolution neural network, support vector machine and Sobel filter for accurate detection of COVID-19 patients using X-ray images. Biomed. Signal Process. Control. 2021, 68, 102622. [Google Scholar] [CrossRef]
- Jahmunah, V.; Sudarshan, V.K.; Oh, S.L.; Gururajan, R.; Gururajan, R.; Zhou, X.; Tao, X.; Faust, O.; Ciaccio, E.J.; Ng, K.H.; et al. Future IoT tools for COVID-19 contact tracing and prediction: A review of the state-of-the-science. Int. J. Imaging Syst. Technol. 2021, 31, 455–471. [Google Scholar] [CrossRef] [PubMed]
- Basiri, M.E.; Nemati, S.; Abdar, M.; Asadi, S.; Acharrya, U.R. A novel fusion-based deep learning model for sentiment analysis of COVID-19 tweets. Knowl.-Based Syst. 2021, 228, 107242. [Google Scholar] [CrossRef]
- Alizadehsani, R.; Sani, Z.A.; Behjati, M.; Roshanzamir, Z.; Hussain, S.; Abedini, N.; Hasanzadeh, F.; Khosravi, A.; Shoeibi, A.; Roshanzamir, M.; et al. Risk factors prediction, clinical outcomes, and mortality in COVID-19 patients. J. Med. Virol. 2021, 93, 2307–2320. [Google Scholar] [CrossRef]
- Taiwo, O.; Ezugwu, A.E. Smart healthcare support for remote patient monitoring during covid-19 quarantine. Inform. Med. Unlocked 2020, 20, 100428. [Google Scholar] [CrossRef]
- Ardakani, A.A.; Kwee, R.M.; Mirza-Aghazadeh-Attari, M.; Castro, H.M.; Kuzan, T.Y.; Altintoprak, K.M.; Besutti, G.; Monelli, F.; Faeghi, F.; Acharya, U.R.; et al. A practical artificial intelligence system to diagnose COVID-19 using computed tomography: A multinational external validation study. Pattern Recognit. Lett. 2021, 152, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef]
- Lin, E.C. Radiation Risk from Medical Imaging. Mayo Clin. Proc. 2010, 85, 1142–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, Q.-Y.; Wang, X.-T.; Zhang, L.-N.; Chinese Critical Care Ultrasound Study Group (CCUSG). Findings of lung ultrasonography of novel corona virus pneumonia during the 2019–2020 epidemic. Intensiv. Care Med. 2020, 46, 849–850. [Google Scholar] [CrossRef] [Green Version]
- Despotovic, V.; Ismael, M.; Cornil, M.; Mc Call, R.; Fagherazzi, G. Detection of COVID-19 from voice, cough and breathing patterns: Dataset and preliminary results. Comput. Biol. Med. 2021, 138, 104944. [Google Scholar] [CrossRef]
- Kobat, M.A.; Kivrak, T.; Barua, P.D.; Tuncer, T.; Dogan, S.; Tan, R.-S.; Ciaccio, E.J.; Acharya, U.R. Automated COVID-19 and Heart Failure Detection Using DNA Pattern Technique with Cough Sounds. Diagnostics 2021, 11, 1962. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S.No. | Paper/Source | Imaging Modality | Total Number of Images |
|---|---|---|---|
| 1 | Available in: https://www.kaggle.com/tawsifurrahman/covid19-radiography-database (accessed on 21 August 2021) | X-ray | Normal: 10,192 COVID: 3616 Viral Pneumonia:1345 Lung opacity: 6012 |
| 2 | Available in: https://www.kaggle.com/prashant268/chest-xray-covid19-pneumonia (accessed on 21 August 2021) | X-ray | Normal: 1583 COVID: 576 Pneumonia: 4273 |
| 3 | [35]/Available in: https://github.com/UCSD-AI4H/COVID-CT (accessed on 21 August 2021) | CT | COVID:349 NonCovid: 397 |
| 4 | [36] Available in: https://www.kaggle.com/plameneduardo/sarscov2-ctscan-dataset (accessed on 21 August 2021) | CT | COVID:1252 Noncovid:1230 |
| 5 | [37]/Available in: https://mosmed.ai/datasets/covid19_1110 (accessed on 21 August 2021) | CT | 1110 patients with severity grading (CT-0 to CT-4) |
| 6 | [38]/Available in: https://zenodo.org/record/3757476#.YPUTnugzbIU (accessed on 21 August 2021) | CT | 20 labeled COVID-19 CT scans (1800 + annotated slices) |
| 7 | [39]/Available in: https://github.com/BorgwardtLab/covid19_ultrasound (accessed on 21 August 2021) | US | Videos and images Healthy: 90 COVID-19: 92 Bacterial Pneumonia: 73 Viral Pneumonia: 6 |
| Paper | Method Used: Preprocessing + Segmentation + Feature Extraction + Feature Selection + Classification or CNN + Classification | Result Obtained | Dataset Used (Most Are Public) | No. of Classes | |
|---|---|---|---|---|---|
| [114] | Image enhancement + WS +deep CNN (ResNet50) and DWT and GLCM+ mRMR+ RF | Cvd.Acc: 99.45, Cvd.Sen:.99.17, Cvd.Pre: 97.51,F1-Score: 0.9833 | N:1500,C-19: 790,BP: 1304,VP: 1215 (after data augmentation) | 2 (C-19, NC) | |
| Cvd.Acc: 98.48, Cvd.Sen: 98.72, Cvd.Pre: 97.89,F1-Score: 0.9829 | 4 | ||||
| [115] | Color layout descriptor + k-NN | Cvd.Sen: 96.5, Cvd.Pre: 96.5 | Total:86 | ||
| [116] | CNN model + Long short-term memory (LSTM) | Cvd.Acc: 99.4, Cvd.Sen: 99.3, Cvd.Spe: 99.2, F1-Score: 98.9, AUC: 99.9 | N: 1525, C-19: 1525,P: 1525 | 3 | |
| [117] | Concatenation of the Xception and ResNet50V2 | Cvd.Acc (avg.): 91.4 | N: 8851,C-19: 180,P: 6054 | 3 | |
| [118] | CNN model | Cvd.Acc: 95, Cvd.Sen: 96.9, Cvd.Spe: 97.5, Cvd.Pre: 95, F-measure: 95.6 | N: 310,C-19: 284,BP: 330,VP: 327 | 3(N, C-19, P) | |
| Cvd.Acc: 89.6, Cvd.Sen: 89.92, Cvd.Spe: 96.4, Cvd.Pre: 90,F-measure: 96.4 | 4 | ||||
| [119] | CNN model | AUROC: 0.96 | Pvt. + Public Dataset | 3 | |
| [120] | DarkNet based CNN model | Cvd.Acc(avg.): 98.08, Cvd.Sen(avg.): 95.13, Cvd.Spe(avg.): 95.3, Cvd.Pre (avg.): 98.03,F1-Score (avg.): 96.51 | N: 500,C-19: 127,P: 500 | 2 (N, C-19) | |
| Cvd.Acc(avg.): 87.02, Cvd.Sen(avg.): 85.35, Cvd.Spe(avg.): 92.18, Cvd.Pre (avg.): 89.96,F1-Score (avg.): 87.37 | 3 | ||||
| [121] | 2D-CTf + CSSA+ EfficientNet-B0 | Cvd.Acc: 99.69, Cvd.Sen: 99.44, Cvd.Spe: 99.81, Cvd.Pre: 99.62, F-measure: 99.53 | N: 1281,C-19: 159,VP: 1285 | 3 | |
| [122] | VGG-16 model | Cvd.Acc(avg.): 97 | N: 3520,C-19: 250,P: 2753 | 3 | |
| [123] | ResNet50 + ResNet101 | Cvd.Acc: 97.77, Cvd.Sen: 97.14, Cvd.Pre: 97.14 | N: 315,C-19: 250, BP: 300,VP: 350 | 2(C-19,O) | |
| [58] | ResExLBP + Relief-F+ SVM | Cvd.Acc: 99.69, Cvd.Sen: 98.85, Cvd.Spe: 100 | N: 234, C-19: 87 | 2 | |
| [124] | VGG16 model | Cvd.Acc: 98.1 | N: 2880, C-19: 415, P: 5179 | 2(C-19,NC) | |
| Cvd.Acc: 94.5 | 3 | ||||
| [125] | ResNet18, ResNet50, SqueezeNet,& DenseNet121 | Cvd.Sen: 98, Cvd.Spe(avg.): 90 | C-19: 200, NC:5000 | 2 | |
| [126] | Capsule Network-based architecture | Cvd.Acc: 95.7, Cvd.Sen: 90, Cvd.Spe: 95.8, AUC: 0.97 | 2(C-19,O) | ||
| [127] | VGG16 model | Cvd.Sen: 97.62, Cvd.Spe: 78.57 | N:142, C-19: 142 | 2 | |
| [128] | ResNet101 | Cvd.Acc: 71.9, Cvd.Sen: 77.3, Cvd.Spe: 71.8 | C-19: 154, NC: 5828 (test data) | 2 | |
| [129] | Deep learning model | Cvd. Acc C-19: 100,P: 93.75,N: 100 | N: 66, C-19: 51,NC: 21,P: 160,TB: 54 | 5 | |
| [130] | Sequential CNN model | Cvd.Acc: 98.3, Cvd.Sen: 100, Cvd.Pre: 96.72, F1-Score: 98.3,ROC area: 0.983 | N: 659, C-19: 295 | 2 | |
| [131] | HE +VGG16-based model | Cvd.Acc (avg.): 86, Cvd.Sen (avg.): 86, Cvd.Spe(avg.): 93, Cvd.Pre(avg.):86,F1-Score: 86 | N: 132, C-19: 132,P: 132 | 3 | |
| [132] | Histogram matching and autoencoder and CLAHE + Custom CNN model | Cvd.Acc (avg.):94.43, Cvd.Sen (avg.): 92.53, Cvd.Spe: 96.33, Cvd.Pre(avg.): 93.76, F1-Score (avg.): 93.14,AUC (avg): 0.988 | N: 4337,C-19: 2589 | 2 | |
| [133] | Ensemble of ResNet-18 Model | Cvd.Acc: 95.5, Cvd.Sen: 100, Cvd.Pre: 94 | N: 1579,C-19: 184,P: 4245 | 3 | |
| [134] | HE+ lung segmentation using UNet + Various deep model are analyzed. | ||||
| [135] | 4 models analyzed (Best: VGG16 and VGG19) | Cvd.Acc: 99.38, Cvd.Sen: 100, Cvd.Spe: 99.33 | N: 802, C-19: 790 | 2 | |
| [136] | CLAHE+VGG16 and VGG19 used (Best: VGG16) | Cvd.Acc: 95.9, Cvd.Sen: 92.5, Cvd.Spe: 97.5,AUC: 0.950 (max. only for C-19) | N: 607,C-19: 607,P: 607 | 3 | |
| [137] | CNN model to separate COVID-19 and pneumonia | ||||
| [138] | Alexnet, Googlenet, and Restnet18 is used (Googlenet best for 4 classes) | Cvd.Acc: 80.56, Cvd.Sen: 80.56, Cvd.Pre: 84.17, F1-Score: 82.32 | N: 79,C-19: 69, BP: 79, VP: 79 | 4 | |
| [76] | MLP-CNN | Cvd.Acc: 95.4, Cvd.Sen: 95, Cvd.Pre: 92.5, F1-Score: 93.6 | C-19: 112, NC: 30 | 2 | |
| [139] | LightCovidNet | Cvd.Acc (avg.): 96.97 | N: 1341,C-19: 446,P: 1345 | 3 | |
| [140] | MobileNet v2 | Cvd.Acc: 96.78, Cvd.Sen: 98.66, Cvd.Spe: 96.46 | N: 504, C-19: 224, P: 714 | 2(C-19,O) | |
| Cvd.Acc: 94.72 | 3(N,C-19,P) | ||||
| [141] | Truncated InceptionNet | Cvd.Acc (avg.): 98.77, Cvd.Sen(avg.): 95, Cvd.Spe(avg.): 99, Cvd. Pre(avg.): 99 F1 score(avg.): 0.97, AUC (avg.):0.99 | N:2003, C-19:162,P: 4280, TB:400 | 4 | |
| [142] | CNN model | Cvd. Prec (avg.), Cvd. Sen (avg.), F1-score (avg.): 100 | C-19: 500, P: 500 | 2 | |
| [143] | CNN model | Cvd.Acc (testing): 94.4 | N:8066, C-19:183,P: 5551 | 3 | |
| [144] | COVID-Net model | Cvd.Acc: 93.3 | Total: 13,975 from 13,870 patients | 3(N,C-19,P) | |
| [85] | CNN model (Inception) + FO-MPA + k-NN | Cvd.Acc: 98.7, F-score: 98.2 | DS1: C-19 +ve: 200, C-19 -ve: 1675 | 2 | |
| Cvd.Acc: 99.6, F-score: 99 | DS2: C-19 +ve: 219, C-19 -ve: 1341 | ||||
| [63] | FrMEMs + MRFO + k-NN | Cvd.Acc: 96.09, Cvd.Sen: 98.75, Cvd.Pre: 98.75 | DS1: C-19 +ve: 216,C-19 -ve: 1675 | 2 | |
| Cvd.Acc: 98.09, Cvd.Sen: 98.91, Cvd.Pre: 98.91 | DS2: C-19 +ve: 219,C-19 -ve: 1341 | ||||
| [145] | Xception model + SVM | Cvd.Acc: 99.33, Cvd.Sen: 99.27, Cvd.Spe: 99.38, Cvd.Pre: 99.27, F1-score:99.27,AUC: 99.32 | N: 565,C-19: 537 | 2 | |
| [146] | Discriminative cost sensitive learning approach | Cvd.Acc: 97.01, Cvd.Pre: 97, Cvd.Sen: 97.09,F1-score: 96.98 | N: 1000,C-19: 239,P: 1000 | 3 | |
| [147] | CNN model | Cvd.Sen (avg.): 91.05, Cvd.Spe(avg.): 99.61, Cvd.Acc(avg.): 98.34,ROC-AUC(avg.): 95.33 | N: 1583,C-19: 225 | 2 | |
| Cvd.Sen (avg.): 92.88, Cvd.Spe(avg.): 99.79, Cvd.Acc(avg.): 99.44,ROC-AUC(avg.): 96.33 | C-19: 225, P: 4292 | 2 | |||
| F1 score (avg.): 94.10 | N: 1583,C-19: 225,P: 4292 | 3 | |||
| [148] | HE and GC + DenseNet103 + ResNet18 | Cvd.Acc: 91.9 | N: 191, C-19: 180,BP: 54, VP: 20,TB: 57 | 4(N,BP,VP,TB) | |
| [149] | VGG16 model | Cvd.Acc, Cvd.Sen, Cvd. Prec, F-score: 80 | C-19: 70, NC: 70 | 2 | |
| [54] | ACGAN based model (CovidGAN) | Cvd.Acc: 95.00 | N: 403, C-19: 721 | 2(N, C-19) | |
| [150] | CNN model | Cvd.Acc: 99.70, Cvd.Pre: 99.70, Cvd.Sen: 99.70, Cvd.Spe: 99.55 | N: 1579, C-19: 423,VP:1485 | 2(N,C-19VP) | |
| [151] | Deep learning model | Cvd.Acc: 97.25, Cvd.Pre: 97.24,F1-score: 97.21 | N: 27,228, C-19: 209, P: 5794 | 3 | |
| [152] | CNN + gated recurrent unit (GRU) | Cvd.Sen: 96, Cvd.Pre: 96, F1-score: 95 | N: 141, C-19: 142, P: 141 | 3 | |
| [153] | Ensemble of deep CNN model (InceptionResNetV2 + ResNet152V2 + VGG16+ DenseNet201) | Cvd.Acc: 99.2, Cvd.Sen: 99.12, Cvd.Spe: 99.07, F-score: 99.17,AUC: 99.21 | N:2039, C-19:1663,P: 401,TB:394 | 4 | |
| [154] | MCFF-Net66-Conv1-GAP | Cvd.Acc: 94.66 | N:1500,C-19:942, BP:1802,VP:1797 | 4 | |
| [155] | ResNet50V2 + t-SNE | Cvd.Acc: 95.49, Cvd.Sen: 99.19, Cvd.Pre:96.19, F1-score: 98.0, AUC: 95.49 | N: 616, C-19: 616,P: 616 | 3 | |
| [156] | CNN model | Cvd.Acc:100, Cvd.Sen:100, Cvd.Spe:100, Cvd.Prec:100, F1-score:100, AUC:100 | N:42, C-19:136 | 2 | |
| [157] | Enhanced Inception-ResNetV2 model | Cvd.Acc(avg.): 98.80, Cvd.Sen(avg.): 99.11, Cvd.Prec(avg.): 98.61,F1 score(avg.): 98.86 | N:1341,C-19:219,VP: 1345 | 3 | |
| [158] | CNN model and GoogLeNet | Cvd.Acc: 97.62, Cvd.Sen: 98.29, Cvd.Spe: 97.64, F-score: 98.30,AUC: 97.96 | N: 1421,C-19: 1332 | 2 | |
| [159] | VGG16 Model | Cvd.Acc: 98.72, Cvd.Sen: 98.78, Cvd.Spe: 98.70, Cvd.Prec: 96.43, F1-score: 97.59 | N:1341,C-19:1200,VP:1345 | 3 | |
| [160] | AlexNet | Cvd.Acc: 99.13, Cvd.Sen: 99.4, Cvd.Spe: 99.15,F-score: 99.49,AUC: 99.31 | Consists: N,C-19,P,TB | 4 | |
| [161] | Ensemble of MobileNet and InceptionV3 | Cvd.Acc: 96.49, Cvd.Prec: 93.01, Cvd.Sen: 92.97,F-score: 92.97 | N:1050,C-19:1050,BP:1050,VP:1050 | 4 | |
| [162] | VGG16 model | Cvd.Acc(avg.): 91.69, Cvd.Sen(avg): 95.92, Cvd.Spe(avg.): 100 | Total: 7720 | 3(N, C-19,P) | |
| [163] | CLAHE + InceptionV3 + ANN | Cvd.Acc: 97.19 | N: 1583,P: 4273 | 2 | |
| [97] | CNN with various optimization algorithm | Cvd.Acc:96, Cvd.Sen:100, Cvd.Spe:99, Cvd.Pre:96, F1-Score:0.98 | N: 1583, C-19: 576, VP:4273 | 3 | |
| [164] | VGG16 model | Cvd.Acc: 96, Cvd.Sen: 92.64, Cvd.Spe: 97.27 | N: 504, C-19: 224 | 2 | |
| Cvd.Acc: 92.53, Cvd.Sen: 86.7, Cvd.Spe: 95.1 | N:504, C-19: 224, P: 700 | 3 | |||
| [50] | FOSF and GLCM and HOG + GWO + Ensemble of classifiers | Cvd.Acc: 98.06, Cvd.Sen: 98.83, Cvd.Spe: 96.51, Cvd.Pre: 98.26,F-measure: 98.55 AUC:0.97 | N: 782, C-19: 782, P: 782 | 2 (N,AB) | |
| Cvd.Acc: 91.32, Cvd.Sen: 96.51, Cvd.Spe: 86.2, Cvd.Pre:87.36,F-measure: 91.71,AUC: 0.91 | 2(C-19,P) | ||||
| [165] | Ensemble of deep CNN model (VGG19 + DenseNet121) + SVM | Cvd.Acc: 99.71 | N:2341, C-19: 798,P: 2345 | 2 (C-19,NC) | |
| Cvd.Acc: 98.28, Cvd.Sen (avg), Cvd.Pre(avg.),F1-Score (avg.): 98.33 | 3 | ||||
| [166] | CNN model + Ensemble of classifiers | Cvd.Acc: 98.91, Cvd.Sen: 97.82, Cvd.Pre: 100,F1-Score: 98.89 | N: 2300,C-19: 2300 | 2 | |
| [167] | Deep learning model (Inception architecture) | Cvd.Acc: 96, Cvd.Sen: 93, Cvd.Spe: 97, Cvd.Pre: 97, F1-Score: 0.96 | C-19: 435,NC: 505 | 2 | |
| [168] | UNet with ResNet + CNN model | Cvd.Acc (avg.): 96.32 | N:1840,C-19:433,BP:2780,VP:1345,TB: 394 | 5 | |
| [169] | Two separate CNN models for binary and ternary classification | Cvd.Acc: 98.7, Cvd.Sen: 100, Cvd.Spe: 98.3 | N:145,C-19: 145, BP: 145 | 2(N, C-19) | |
| Cvd.Acc: 98.3, Cvd.Sen: 99.3, Cvd.Spe: 98.1 | 3 | ||||
| [170] | VGG16 and Xception model (Best: Xception) | Cvd.Sen: 100, Cvd.Spe: 97.6, F1-Score: 97.7 | N: 400, C-19: 402,P:200,I: 35 | 2 | |
| [171] | Various DNN + Majority voting scheme | Cvd.Acc: 99.31 | N: 1338, C-19: 237, VP: 1336 | 3 | |
| [172] | Customized CNN Model | Cvd.Acc: 92.95, Cvd.Sen (avg.): 90.72, Cvd.Pre(avg.): 94.04,F1-Score(avg.): 0.9204 | N: 1341, C-19: 744 (Independent set) | 2 | |
| [173] | NanoChest-net model | Analyzed with various datasets. | |||
| [174] | VGG16+ HS + k-NN | Cvd.Acc, Cvd.Sen, Cvd.Pre,F1-Score, AUC:100 | N: 480,C-19: 280 | 2 | |
| [175] | OptiDCNN model | Cvd.Acc: 99.11 | N: 5000, C-19: 184 | 2 | |
| [176] | HOG and CNN(VGG19) + ME + CNN classifier + WS | Cvd.Acc: 99.49, Cvd.Sen: 93.65, Cvd.Spe: 95.7 | C-19 +ve: 1979, C-19 -ve: 3111 | 2 | |
| [177] | Ensemble-CNNs (based on ResNeXt-50, Inception-v3, and DenseNet-161) | Cvd.Acc: 75.23 ± 3.40, Cvd.Sen: 75.20, Cvd.Spe: 87.60, Cvd.Pre: 78.28, F1-Score: 73.43 AUC: 0.8140 | N: 711, C-19: 711,P:711,BP:711,VP:711 Lung Opacity not Pneumonia:711 (public+Pvt.) | 3(N,C-19,P) | |
| Cvd.Acc: 81.00 ± 2.39, Cvd.Sen: 82.96, Cvd.Spe: 85.24, Cvd.Pre: 82.99,F1-Score: 81.49, AUC: 0.8810 | 5 | ||||
| [178] | Showed that a system with 2-class model are not valid for the diseases with similar symptoms, by conducting various experiments | ||||
| [179] | Exemplar COVID-19FclNet9 + SVM | Cvd.Acc: 99.64 | N: 150,C-19:127 | 2 | |
| Cvd.Acc: 98.84 | N: 4000,C-19: 3616, P: 1345 | 3 | |||
| Cvd.Acc: 97.60 | N: 234,C-19:125,BP:242,VP:148 | 4 | |||
| [180] | Decompose, Transfer, and Compose (DeTraC)+PCA | Cvd.Acc: 93.1, Cvd.Sen:100 | N: 80, C-19:105,SARS: 11 | 3 | |
| [77] | UNet + HRNet | Cvd.Acc: 99.26, Cvd.Sen:98.53, Cvd.Spe: 98.82 | Total: 272 | 2 | |
| [181] | Various CNN model used (Best:EfficientNetB0) | Cvd.Acc:92.93, Cvd.Sen: 90, Cvd.Spe: 95, Cvd. Prec: 88.3,F1- score: 0.88 | N: 1341, C-19: 420, P: 1345 | 3 | |
| [182] | EfficientNet B3-X | Cvd.Acc: 93.9, Cvd.Sen: 96.8, Cvd.PPV: 100 | N:7966+100, C-19: 152+31 P: 5421+100 | 3 | |
| [183] | Various pre-trained CNN models (Best: ResNet50) | Cvd.Acc: 96.1 (N,C-19), Cvd.Acc: 99.5(C-19,VP), Cvd.Acc: 99.7(C-19,BP) | N: 2800, C-19: 341, BP: 2772, VP: 1493 | 2 | |
| [184] | CNN model + SVM | Cvd.Acc (avg.): 95.81, Cvd. Prec(avg.): 95.27, F1 score(avg.): 94.94 | N:1266 +317, C-19:460 + 116 P:3418 + 855 (Pvt.) | 3 | |
| [185] | ResNet50+ SVM | Cvd.Sen:80, Cvd.Spe: 81, AUC: 0.81 | Training and validation C-19:250, NC:250 | Testing independent set C-19:74,NC:36 (Pvt.) | 2 |
| [186] | VisionPro Deep Learning™ + COGNEX’s | F-score: 95.3 (for segmented lung) | N: 7966+100,C-19: 258+100 P: 5451+100 | 3 | |
| [84] | Pillow library + HSGO + SVM | Cvd.Acc:99.65 | C-19: 371, NC: 1341 | 2 | |
| [187] | CNN model | Cvd.Acc (avg.): 98.03, Cvd.Sen(avg.): 98.83, Cvd.Spe(avg.): 97 | DS1:C-19: 217, NC: 1126 DS2:C-19: 2025, NC: 2025 | 2 | |
| [188] | AlexNet + Relief + SVM | Cvd.Acc: 99.18 | N:1583, C-19: 219, P:4290 | 3 | |
| [189] | RGB to YUV and YUV to RGB + CNN | Cvd.Acc: 84.76, Cvd.Sen: 98.99, Cvd.Spe: 92.19, F-score: 0.9389,AUC: 0.5948 | N:28,C-19:78,P: 79(each for BP and VP) | 4 | |
| [190] | CNN model | Cvd.Acc: 98.44 | Total: 392, C-19: 196 | 2 | |
| [191] | Deep CNN model | Cvd.Acc(avg.): 91.62, AUC:91.71 | C-19 +ve: 538, C-19 –ve: 468 | 2 | |
| [192] | Deep CNN model | Cvd.Acc(avg.):99.2, Cvd.Sen(avg.):99.2,F1- score: 0.992 | N, C-19: 2484 (each) N, C-19,P: 3829 (each) | 2 | |
| Cvd.Acc(avg.):95.2, Cvd.Sen(avg.):95.2,F1-score: 0.952 | 3 | ||||
| [193] | MobileNetV2 | Cvd.Acc: 92.91, Cvd.Pre: 92 | N: 234, C-19: 390 | 2 | |
| [49] | DenseNet201 model+ Quadratic SVM | Cvd.Acc: 98.16, Cvd.Sen: 98.93, Cvd.Spe: 98.77 | N: 2924, C-19: 683,P: 4272 | 3 | |
| [194] | Cluster-based learning + Ensemble of classifiers | Cvd.Acc (avg.):100 | N:79,C-19: 69, BP:79, VP:79 | 2(N,C-19) | |
| Cvd.Acc(avg.): 85.23 | 3(N,C-19,BP) | ||||
| Cvd.Acc(avg.): 74.05 | 4 | ||||
| [195] | Various deep CNN models are compared (Best: XCeptionNet) | F1-score: 0.97 | N: 1345+238, C-19:490+ 86,P:3632+ 641 (Train + Test) | 3 | |
| [196] | CNN model | Cvd.Acc: 98.19 | N: 10,456, C-19: 573, P: 11,673 (Pvt.) | 2(C-19,P) | |
| Cvd.Acc: 91.21 | 3 | ||||
| [197] | Federated learning model | Cvd.Acc: 98.72 | N: 1266, C-19: 460,P: 3418 (Pvt.) | 2(C-19,P) | |
| Cvd.Acc: 95.96 | 3 | ||||
| [80] | ResNet50 + ASSOA + MLP | Cvd.Acc: 99.70 | Total: 5863 | 2(C-19+ve, C-19-ve) | |
| [198] | Several CNN models are analyzed (Best: VGG16) | Cvd.Acc: 91 | N:1341, C-19:219,P:1345 | 3 | |
| [199] | Semi-supervised open set domain adversarial network (SODA) | Avg. AUC-ROC Score: 0.9006(C-19), 0.9082(P) | With different domain target dataset | ||
| [200] | VGG16 model | Cvd.Acc: 97, Cvd.Sen: 99, Cvd.Spe: 99, Cvd.Pre: 97, F-score: 98 | N:1400, C-19: 210, P: 1400 | 3 | |
| [201] | CovFrameNet (deep learning architecture) | Cvd.Acc: 100, Cvd.Sen: 85, Cvd.Spe: 100, Cvd.Pre: 85, F-score: 90, AUC: 50 | Using two different dataset | ||
| [202] | Self-supervised super sample decomposition for transfer learning (4S-DT) model | Cvd.Acc: 97.54, Cvd.Sen: 97.88, Cvd.Spe: 97.15 | DS1: N: 296, C-19: 388, SARS: 41 | 3(N, C-19, SARS) | |
| Cvd.Acc: 99.80, Cvd.Sen: 99.70, Cvd.Spe: 100 | DS2: N: 1583,C-19: 576,P: 4273 | 3 (N,C-19,P) | |||
| [203] | VDI + Residual encoder + SVM | Cvd.Acc: 93.60, Cvd.Sen: 88, Cvd.Pre: 100, F1-score: 93.60 | C-19: 315, NC: 357 | 2 | |
| [204] | RCoNetks | Cvd.Acc (avg.):97.89, Cvd.Sen(avg.):97.76, Cvd.Spe(avg.):98.24, Cvd.PPV(avg.):97.93, F1-score(avg.):97.63 | N: 8851, C-19: 238, P: 6045 | 3 | |
| Paper | Method Used: Preprocessing + Segmentation + Feature Extraction + Feature Selection + Classification or CNN + Classification | Result Obtained | Dataset (Most Are Public) | No. of Classes | |
|---|---|---|---|---|---|
| [205] | Various deep models are analyzed (Best: ResNet101) | Cvd.Acc: 99.51, Cvd.Sen: 100, Cvd.Spe: 99.02, AUC: 0.994 | C-19: 108,NC: 86,Total: 1020 slice, (Pvt.) | 2 | |
| [206] | EfficientNet family based architecture | Cvd.Acc: 98.99, Cvd.Sen: 98.80, Cvd.PPV:99.20 | DS 1- NC: 1230, C-19: 1252 | 2 | |
| Cvd.Acc: 56.16, Cvd.Sen: 53.06, Cvd.PPV: 54.74 (Train DS 1 & Test DS2) | DS 2: NC: 463,C-19: 349 | ||||
| [207] | LinkNet + DenseNet + DT | Cvd.Acc(avg.): 94.4, Cvd.Pre(avg.): 96.7, Cvd.Rec(avg.): 95.2, F1-score(avg.): 96.0 | C-19:445,NC:233 | 2 | |
| [208] | novel conditional generative model, called CoSinGAN | Independent testing is done using 50 CT cases (for lung segmentation and infection learning) | |||
| [93] | Intensity normalization and segmentation + Q-deformed entropy + ANOVA+ LSTM | Cvd.Acc: 99.68 | N: 107,C-19: 118,P: 96 | 3 | |
| [209] | Modified Alexnet model | Cvd.Acc: 94.75, Cvd.Sen: 93.22, Cvd.Spe: 96.69, Cvd.PPV:97.27 | C-19:3482,NC:2751 (Pvt.) | 2 | |
| [210] | Ensemble various models using majority voting scheme | Cvd.Acc: 85.2, Cvd.Sen: 85.4, Cvd.Pre: 85.7,F-score: 0.852,AUC: 0.91 | C-19 + ve: 349,C-19 -ve: 397 | 2 | |
| [211] | ResNet50 | Cvd.Acc: 82.91, Cvd.Sen: 77.66, Cvd.Spe: 87.62 | C-19:345,NC:397 | 2 | |
| [99] | CNN model with MODE | Cvd.Acc: outperforms competitive models by 1.9789% | 2 | ||
| [212] | Ensemble is built using ResNet152V2, DenseNet201, and VGG16 | Cvd.Acc: 98.83, Cvd.Sen: 98.83, Cvd.Spe: 98.82,F-measure: 98.30,AUC: 98.28 | N:3038,C-19:2373,P: 2890 TB: 3193 | 4 | |
| [36] | eXplainable Deep Learning approach (xDNN) | F1-score: 97.31 | SARS-CoV-2: 1252 Non SARS-CoV-2: 1230 | 2 | |
| [35] | Multi-task and self-supervised learning | Cvd.Acc: 89, F1- score: 0.90, AUC: 0.98 | C-19:349,NC: 463 | 2 | |
| [213] | Semi-Inf-Net | Cvd.Sen: 0.725, Cvd.Spe: 0.960, Dice: 0.739 | 100 images from 19 patients (Pvt) | C-19 lung Seg. | |
| [214] | 3D CNN model | Cvd.Acc: 87.50, Cvd.Sen: 86.90, Cvd.Spe: 90.10,F1-score: 82,AUC: 94.40 | Train: 2186, Test: 2796 (Pvt.) | 2 (CAP,C-19) | |
| [215] | CNN model | Cvd.Acc (avg): 94.03, Cvd.Sen(avg.): 94.44, Cvd.Spe (avg.): 93.63 | N: 320, C-19: 320 (Pvt.) | 2 | |
| [92] | AlexNet + Guided WOA | Cvd.Acc: 87.50, AUC: 99.50 | C-19: 334, NC-19: 794 | 2 | |
| [216] | Multi-task multi-slice deep learning system | Cvd.Acc: 95.21 | N: 251,C-19: 245,H1N1: 105 CAP: 123 (Pvt.) | 4 | |
| [217] | LBP and statistical features + ReliefF and NCA + DNN | Cvd.Acc: 95.84 | N: 397,C-19: 349 | 2 | |
| [218] | Region growing + deep CNN model (ResNet101 as its backbone) | Cvd.Acc: 94.9 | Total: 1110 patients with 5 classes | 5 | |
| [219] | Radiomic features + mRMR + XGBoost | AUC: 0.95 ± 0.02 | Total: 152 Patients | ||
| [220] | Segmentation of infectious lung as ResNet50 backbone | ||||
| [221] | DTCT and GLCM + RF | Cvd.Acc (avg.): 72.2, Cvd.Sen(avg.): 77, Cvd.Spe(avg.): 68,AUROC (avg.): 0.8 | C-19: 291, P: 279 (Pvt.) | 2 | |
| [222] | ResGNet (Graphs are generated using ResNet101-C features) | Cvd.Acc (avg.): 96.62, Cvd.Sen(avg.): 97.33, Cvd.Spe(avg.): 95.91, Cvd.Pre(avg.): 96.21,F1-Score(avg.): 0.9665 | N:148,C-19: 148 (Pvt.) | 2 | |
| [223] | CNN model (DenseNet201) + ELM | Cvd.Acc: 98.36, Cvd.Sen: 98.28, Cvd.Spe: 98.44, Cvd.Pre: 98.22,F1-Score: 98.25, AUC: 98.36 | C-19: 349,NC: 397 | 2 | |
| [224] | M 2 UNet (Multi-task multi-instance deep network) | Cvd.Acc (avg.): 98.5, Cvd.Sen(avg.): 95.2, Cvd.Pre(avg.): 97.5,F1-Score(avg.): 0.963 AUC(avg.): 0.991 | S:51,NS: 191(Pvt.) | 2 | |
| [225] | Dual-branch combination network (using UNet + ResNet50) | Cvd.Acc: 96.74, Cvd.Sen: 97.91, Cvd.Spe: 96.00,AUC: 0.9864 | N: 75 scans, C-19: 48 scans (Pvt.) | 2 | |
| [226] | Majority voting scheme with ResNet50 | Cvd.Acc: 96, Cvd.Sen:100, Cvd.Spe: 96,AUC: 0.90 | Two public datasets are used | 2 | |
| [227] | HE + WF + AlexNet + SVM | Cvd.Acc: 96.69, Cvd.Sen: 96, Cvd.Spe: 98 | N:500,C-19:488, P:500 | 3 | |
| [228] | DenseNet-201 | Cvd.Acc: 97.8, Cvd.Sen: 98.1, Cvd.Spe: 97.3, Cvd.Pre: 98.4, F1-score: 98.25 | C-19: 1500, NC: 1500 | 2 | |
| [229] | CLAHE + VGG-19 model | Cvd.Acc: 95.75, Cvd.Sen: 97.13,F1- score: 95.75, ROC-AUC: 99.30 | C-19 +ve: 1252, C-19 -ve: 1230 | 2 | |
| [230] | VGG16 model and ensemble learning | Cvd.Acc: 93.57, Cvd.Sen: 94.21, Cvd.Spe: 93.93, Cvd.Pre: 89.4,F1-score: 91.74 | N: 243,C-19: 790,P: 384 | 3 | |
| [61] | Z-score normalization and KF+CNN + fuzzy c-means + LDN | Cvd.Pre: 96, Cvd.Sen: 97, F-score: 97 and volume overlap error (VOE) of 5.6 ± 1:2%. | |||
| [231] | Golden Key Tool + VGG model | Cvd.Acc: 100 | DS1- N: 55, C-19: 349 | 2 | |
| Cvd.Acc: 93.478, Cvd.Pre: 97.33, F1-score: 87.5 | DS2- N: 55, C-19: 349, NC: 20 | 3 | |||
| Cvd.Acc: 90.12, Cvd.Pre: 90.6 | DS3- C-19: 349, NC: 396 | 2 | |||
| [232] | PatchShuffle Stochastic Pooling Neural Network (PSSPNN) | F1-score(avg.): 95.79 | Total:521 | 4(N,C-19, P, TB) | |
| [233] | Clinical information and chest CT features + XGBoost | Cvd.Sen: 90.91, Cvd.Spec: 97.96, AUC: 0.924 | Total: 198 | 2 (M,S) | |
| [234] | 3D CU-Net | DSC: 0.960, 0.963, 0.771, Cvd.Sen: 0.969, 0.966, 0.837, Cvd.Spe: 0.998, 0.998, 0.998 | C-19: 70 for detecting C-19 infection | ||
| [235] | Tensor + COVID-19-Net (VGG16) + Transfer-Net (ResNet50) | Cvd.Acc: 94, Cvd.Sen: 96, Cvd.Spe: 92 | N: 700, C-19: 700 | 2 | |
| [236] | Ensemble model (using Resnet18, Densenet201, Mobilenetv2 and Shufflenet) | Cvd.Acc: 96.51, Cvd.Sen: 96.96, Cvd.Spe: 96.00,F1-Score: 0.97,AUC: 0.99 | C-19: 349,NC: 397 | 2 | |
| [237] | LungINFseg, model for segmentation | Cvd.Acc (avg.): 98.92, Cvd.Sen(avg.): 83.10, Cvd.Spe(avg.): 99.52, DSC(avg.):80.34 intersection over union (IoU) (avg.): 0.6877 | 20 labeled COVID-19 CT scans (1800 + annotated Slices) | ||
| [238] | Feature Pyramid Network(FPN) DenseNet201 for detection | Cvd.Sen: 98.3 (m), Cvd.Sen: 71.2(mod), Cvd.Sen: 77.8(s), Cvd.Sen: 100(cr) | 1110 subjects Severity classification | ||
| [239] | Volume of interest based DenseNet-201 | Cvd.Acc: 88.88, Cvd.Sen:89.77, Cvd.Spe: 94.73, F1-Score: 88.88 | C-19: -moderate risk:40 severe risk:40 extreme risk:40 | 3 | |
| [240] | Various deep network architectures are analyzed using publicly available two COVID-19 CT datasets | 2 | |||
| [241] | UNet | F1-Score, improvement of 5.394 ± 3.015%. | +ve:492. -ve: 447 | ||
| [242] | Stationary wavelets + CNN model (Best: ResNet18) | Cvd.Acc: 99.4, Cvd.Sen: 100, Cvd.Spe: 98.6,AUC: 0.9965 | C-19:349, NC:397 | 2 | |
| [243] | Gabor filter + convolution and pooling layers + RF | F1 score: 0.99 | C-19: 349,NC: 397 | 2 | |
| [244] | Stacked autoencoder detector model | Cvd.Acc(avg.):94.7, Cvd.Sen(avg.):94.1, Cvd.Pre(avg.):96.54, F1-score (avg.):94.8 | C-19: 275,NC: 195 | 2 | |
| [245] | DenseNet201 model + k-NN | Cvd.Acc, Cvd.Sen, Cvd.Pre, & F1-score:100 | C-19:2740,Suspected Cases: 2740 (Private) | 2 | |
| [246] | CNN model + MI and Relief-F and DA +SVM | Cvd.Acc: 98.39, Cvd.Sen: 97.78, Cvd.Pre: 98.21, F1-score: 0.98, AUC: 0.9952 | SARS-CoV-2: 1252 Non SARS-CoV-2: 1230 | 2 | |
| Cvd.Acc: 90.0, Cvd.Sen: 84.06, Cvd.Pre: 93.55,F1-score: 0.8855, AUC: 0.9414 | C-19:349, NC: 463 | ||||
| [247] | VGG19 model | Cvd.Acc: 94.52 | C-19: 349,NC: 463 | 2 | |
| [248] | VGG16 model | Cvd.Acc: 98.0, Cvd.Sen: 99.0, Cvd.Spe: 94.9 | N: 275, C-19: 195 | 2 | |
| [249] | Radiological features + Chi-square test + Ensemble classifier | Cvd.Acc: 91.94, Cvd.Sen: 93.54, Cvd.Spe: 90.32,AUC: 0.965 | C-19: 306,non-COVID-19 pneumonia: 306 (Pvt.) | 2 | |
| [250] | Various CNN and texture based approaches | Cvd.Acc (avg.): 95.99, Cvd.Sen(avg.): 94.04, Cvd.Spe(avg.): 99.01,F1-score(avg.): 0.9284, AUC (avg.): 0.9903 | COVID-19: 386, NC: 1010 | 2 | |
| [251] | Worried deep neural network + pre-trained models (InceptionV3, ResNet50, and VGG19) | Cvd.Acc: 99.04, Cvd.Prec: 98.68, Cvd.Rec: 99.11,F-score: 98.90 | Total: 2623 (Pvt.) | 2(I,NI) | |
| [252] | Density peak clustering approach | Structural similarity index (SSIM): 89 | Total images: 12 (Pvt.) | C-19 Seg. | |
| [253] | EfficientNet-b0 model | Cvd.Acc: 99.83, Cvd.Sen: 92.86, Cvd.Spe: 98.32, Cvd.PPV:91.92 | Total images: 107,675 (Pvt.) | 2(C-19,NC) | |
| Cvd.Acc: 97.32, Cvd.Sen: 99.71, Cvd.Spe: 95.98, Cvd.PPV: 93.26 | 2 (C-19,P) | ||||
| [254] | EfficientNetB3 | Cvd.Sen: 97.2, Cvd.Spe: 96.8,F1-score: 0.970, AUC: 0.997 | N:105,C-19:143,P:147 (Pvt.) | 3 | |
| Cvd.Sen: 92.4, Cvd.Spe: 98.3,F1-score: 0.953,AUC: 0.989 | N: 121,C-19: 119, P: 117(Pvt.) | 3 | |||
| Cvd.Sen: 93.9, Cvd.Spe: 83.1,AUC: 0.954 | C-19: 856,Non-P: 254 (Pvt.) | 2 | |||
| [255] | COVID Segnet | For COVID-19 segmentation: Dice Score: 0.726, Cvd.Sen.: 0.751, Cvd.Pre.: 0.726 | Train: 731 Test: 130 patients (Pvt.) | Lung and infected regions seg. | |
| For lung segmentation: Dice Score: 0.987, Cvd.Sen.: 0.986, Cvd.Pre.: 0.990 | |||||
| [256] | Anam-Net | Dice Score: 0.956, Cvd.Acc.: 98.5, Cvd.Sen.: 92.7, Cvd.Spe.: 99.8 | N:929, AB:880 | Anomalies seg. | |
| Paper | Method Used: Preprocessing + Segmentation + Feature Extraction + Feature Selection + Classification or CNN + Classification | Result Obtained | Dataset (Most Are Public) | No. of Classes |
|---|---|---|---|---|
| [257] | Features from various layers deep CNN model is fused | Cvd.Acc (avg.): 92.5, Cvd.Sen(avg.): 93.2, Cvd.Pre(avg.): 91.8 | N: 53 + 15,C-19: 45+18,BP: 23 + 7 | 3 |
| [258] | Autoencoder network and separable convolutional branches attached with a modified DenseNet201 | 17% more than the traditional DenseNet | Convex:38, Linear: 20 Score 0 (healthy) to Score 3 (worst-case) | 4 |
| [39] | Frame- and video-based CNN models (Best: VGG) | Cvd.Sen: 0.90 ± 0.08, Cvd.Spe: 0.96 ± 0.04 | N: 90,C-19:92, BP: 73,VP: 6 (It includes videos and images) | 3 |
| Paper | Method Used: Preprocessing + Segmentation + Feature Extraction + Feature Selection + Classification or CNN + Classification | Result Obtained | Dataset (Most Are Public) | No. of Classes |
|---|---|---|---|---|
| [259] | VGG19 model | Cvd.Acc: 89.47, Cvd.Sen: 76.19, Cvd.Spe: 97.22 | X-ray: 673 radiology images of 342 patients | 2(N,C-19) |
| Cvd.Acc: 95.61, Cvd.Sen: 96.55, Cvd.Spe: 95.29 | SARS-CoV-2 CT: C-19:1252, NC: 1230 | 2(C-19,P) | ||
| Cvd.Acc: 95, Cvd.Sen: 94.04, Cvd.Spe: 95.86 | X-ray: 5856 images | 2(C-19,NC) | ||
| [260] | VGG19 + CNN model | Cvd.Acc: 98.05, Cvd.Spe: 99.5, Cvd.Rec: 98.05, Cvd.Pre: 98.43, F1-Score: 98.24,AUC: 99.66 | Total images: 33,676 | 4(N,C-19,P,LC) |
| [65] | LBP and MFrLFM + SFS | Cvd.Acc: 99.3±0.2, F1-score: 93.1±0.2, AUC: 94.9±0.1 | Chest X-ray: 1926 | 2(C-19,NC) |
| Cvd.Acc: 93.2±0.3, F1- score: 92.1±0.3,AUC: 93.2±0.3 | CT scan: 2482 | |||
| [261] | COVID-ResNet53 | Cvd.Acc: 97.1, Cvd.Sen: 98.9, Cvd.Spe: 95.7, Cvd.Pre: 94.5 | X-ray: C-19: 4045, NC: 5500 | 2(C-19,NC) |
| Cvd.Acc: 97.7, Cvd.Sen: 98.7, Cvd.Spe: 95.6, Cvd.Pre: 97.9 | CT: C-19: 5427, NC: 2628 | |||
| [262] | CNN model | Cvd.Acc: 96.68, Cvd.Sen: 96.24, Cvd.Spe: 95.65 | N: 7021,C-19: 1066, P:7021 | 3(N,C-19, P) |
| [263] | PF+ GraphCovidNet | Cvd.Acc, Cvd.Pre, Cvd.Sen,F1- score:100 | SARS-CoV-2 CT N: 1229, C-19:1252 | 2 |
| Cvd.Acc, Cvd.Pre, Cvd.Sen,F1- score:100 | CT: N: 407, C-19: 349 | 2 | ||
| Cvd.Acc, Cvd.Pre, Cvd.Sen,F1- score: 99.84 | X-ray: N: 1592,C-19:504,P: 4343 | 3 | ||
| [264] | HE and WF + Haralick texture feature and VGG16 model | Cvd.Acc: 93, Cvd.Sen: 90, Cvd.Pre: 91 | N: 1349,C-19: 407,BP: 2538,VP: 1345 | 4 |
| [265] | HE and WF + DenseNet103 + Haralick texture feature and ResNet101 model | Cvd.Acc: 94.9, Cvd. Sen: 93, Cvd. Pre: 93 | Total images: 12,520, N: 4100, C-19: 220 P: 4100,Lung opacity: 4100 | 4 |
| [266] | DenseNet121 + Bagging tree classifier | Cvd.Acc: 99 | Total images: 274 | 2(N,C-19) |
| [267] | Contrastive multi-task convolutional neural network (CMT-CNN) CNN Model: EfficientNet | Cvd.Acc (avg.): 93.46, Cvd.Sen (avg.): 90.57, Cvd.Spe (avg.): 90.84 AUC (avg.): 89.33 (2-class) | CT scan: N: 1164,C-19: 1980,P:1614 | 2(C-19,O) 3(N,C-19,P) |
| Cvd.Acc (avg.): 91.45 (3-class) | ||||
| Cvd.Acc (avg.): 97.23, Cvd.Sen (avg.): 92.97, Cvd.Spe (avg.): 91.91 AUC (avg.): 92.13 (2-class) | X-ray: N: 1583, C-19: 231,P: 4007 | |||
| Cvd.Acc (avg.): 93.49 (3-class) | ||||
| [268] | Contextual features reduced by convolutional filters (CFRCF) | Cvd.Acc: 94.23 | CT: C-19: 349, NC: 397 | 2(C-19,NC) |
| X-ray: C-19: 187, NC: 73 | ||||
| [269] | CNN model | Cvd. Sen: 97.92, Cvd.Spe: 94.64, Cvd. Pre: 94.81,AUC: 0.9808 | Total images: 672 (X-ray:336 and CT:336) | 2(C-19,NC) |
| [270] | VGG16 + InceptionV3 models | Cvd.Sen: 100, Cvd.Pre: 0.97, F1: 0.98 | CT: 746 X-ray: 268 | 2(N,C-19) |
| [271] | CovidNet model | Cvd. Acc: 100, Cvd. Sen: 100 | CT: C-19: 1252, NC: 1230 | 2 |
| Cvd. Acc: 96.84, Cvd. Sen: 92.19 | X-ray: N: 445, C-19:321, P:500 | 3 | ||
| Using all X-ray, CT, and US imageries | ||||
| [272] | Pre-trained deep learning models: DenseNet-161, ResNet-34, VGG-16 and MobileNet-V2 are used | Cvd.Sen: 97.91, Cvd.Spe: 99.57, Cvd.Pre: 99.57,F1-score: 98.73 | X-ray: C-19: 234, NC:234 | 2 |
| Cvd.Acc: 64.41, Cvd.Sen: 66.28, Cvd.Spe: 62.93, Cvd.Pre:58.67,F1-Score: 0.6225 | CT: C-19: 392, NC:392 | |||
| Cvd.Acc: 99.36, Cvd.Sen: 98.74, Cvd.Spe: 100, Cvd.Pre:100,F1-Score: 0.9973 | US: C-19:19, NC:14 | |||
| [273] | VGG19 model | Cvd.Pre: 86 | X-ray: N: 60,361,C-19:140,P:322 | 3 |
| Cvd.Pre: 84 | CT: C-19: 349, NC: 397 | 2 | ||
| Cvd.Pre: 100 | US: N: 235,C-19: 399,P: 277 | 3 | ||
| X-ray | |||||
| Class | Cvd.Acc (%) | Cvd.Sen (%) | Cvd.Spe (%) | F1-score (%) | AUC (%) |
| 2 | 97.05 | 95.37,086 | 94.79 | 96.11 | 95.45 |
| 3 | 94.78 | 95.63,542 | 97.10 | 85.71 | 93.55 |
| 4 | 91.69 | 94.335 | 97.16 | 83.32 | 64.74 |
| 5 | 92.41 | 82.96 | 95.24 | 81.49 | 88.1 |
| CT | |||||
| Class | Cvd.Acc (%) | Cvd.Sen (%) | Cvd.Spe (%) | F1-score (%) | AUC (%) |
| 2 | 92.99 | 92.61,897 | 93.28 | 94.57 | 91.40 |
| 3 | 94.55 | 95.016 | 95.55 | 92.08 | 99.3 |
| 4 | 97.02 | 98.83 | 98.82 | 97.9 | 98.28 |
| 5 | -- | -- | -- | -- | 94.9 |
| X-ray and CT | |||||
| Class | Cvd.Acc (%) | Cvd.Sen (%) | Cvd.Spe (%) | F1-score (%) | AUC (%) |
| 2 | 96.54 | 94.35 | 95.81 | 97.38 | 93.87 |
| 3 | 94.99 | 94.21 | 95.65 | 99.84 | |
| 4 | 95.52 | 94.75 | -- | 98.24 | 99.66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gudigar, A.; Raghavendra, U.; Nayak, S.; Ooi, C.P.; Chan, W.Y.; Gangavarapu, M.R.; Dharmik, C.; Samanth, J.; Kadri, N.A.; Hasikin, K.; et al. Role of Artificial Intelligence in COVID-19 Detection. Sensors 2021, 21, 8045. https://doi.org/10.3390/s21238045
Gudigar A, Raghavendra U, Nayak S, Ooi CP, Chan WY, Gangavarapu MR, Dharmik C, Samanth J, Kadri NA, Hasikin K, et al. Role of Artificial Intelligence in COVID-19 Detection. Sensors. 2021; 21(23):8045. https://doi.org/10.3390/s21238045
Chicago/Turabian StyleGudigar, Anjan, U Raghavendra, Sneha Nayak, Chui Ping Ooi, Wai Yee Chan, Mokshagna Rohit Gangavarapu, Chinmay Dharmik, Jyothi Samanth, Nahrizul Adib Kadri, Khairunnisa Hasikin, and et al. 2021. "Role of Artificial Intelligence in COVID-19 Detection" Sensors 21, no. 23: 8045. https://doi.org/10.3390/s21238045