
Effect of Blue Light on Acne Vulgaris: A Systematic Review



 ,
,
Abstract
:1. Introduction
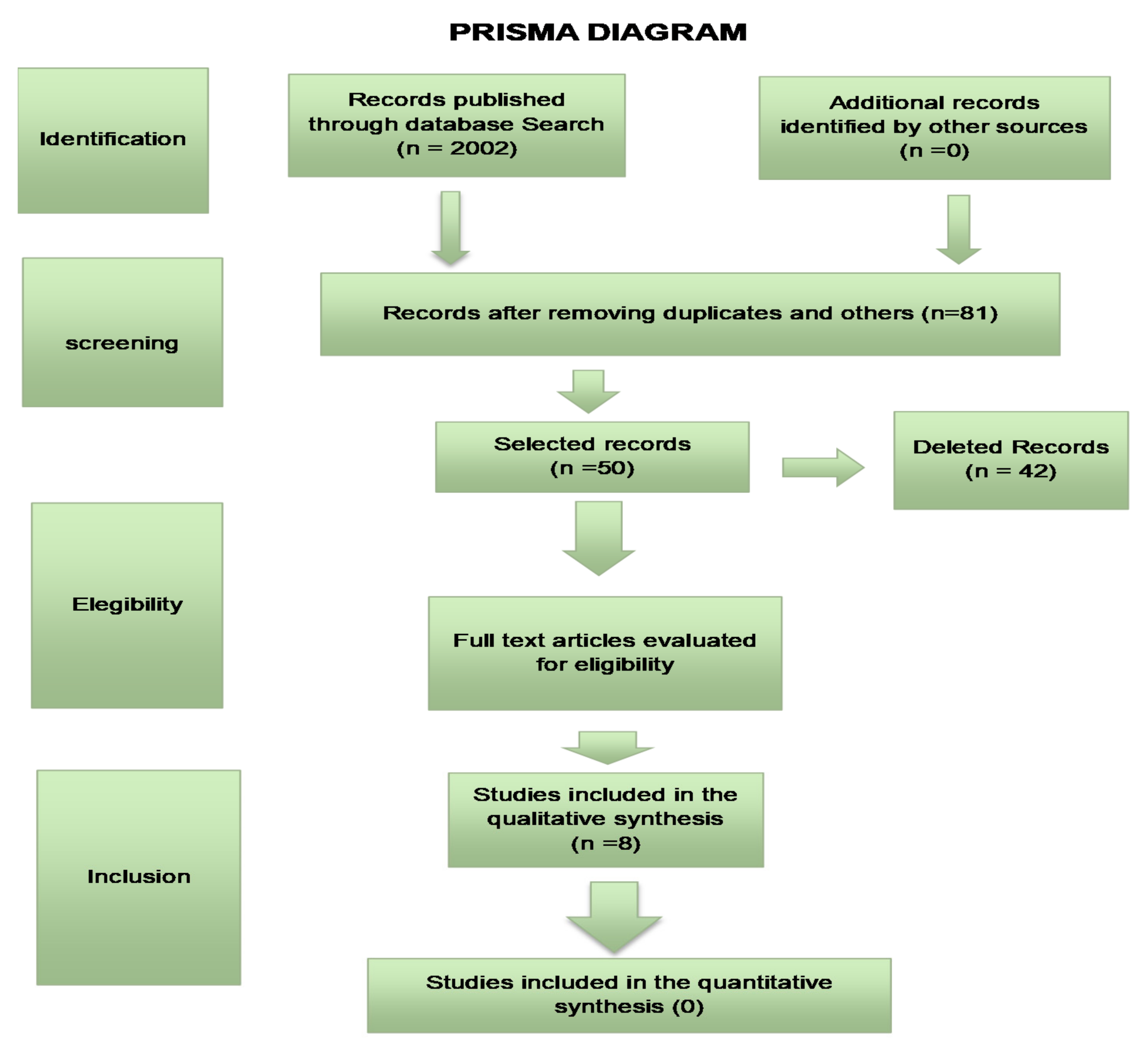
2. Materials and Methods
- Only randomized controlled trials from 1990 to 2021;
- Articles that presented control group.
- Duplicates or studies with the same number of ethical approval.
3. Results
Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Sociedade Brasileira de Dermatologia. Perfil nosológico das consultas dermatológicas no Brasil. An. Bras. Dermatol. 2006, 81, 549–558. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.; Bhate, K. A global perspective on the epidemiology of acne. Br. J. Dermatol. 2015, 172, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Bergler-Czop, B. The etiopathogenesis of acne vulgaris—What’s new? Int. J. Cosmet. Sci. 2014, 36, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Mooney, T. Preventing psychological distress in patients with acne. Nurs. Stand. 2014, 28, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Koo, J.Y.M.; Smith, L.L. Psychologic Aspects of Acne. Pediatr. Dermatol. 1991, 8, 185–188. [Google Scholar] [CrossRef]
- Saitta, P.; Keehan, P.; Yousif, J.; Way, B.V.; Grekin, S.; Brancaccio, R. Cutis. An update on the presence of psychiatric comorbidities in acne patients, Part 2: Depression, anxiety, and suicide. Cutis 2011, 88, 92–97. [Google Scholar]
- Dreno, B.; Bagatin, E.; Blume-Peytavi, U.; Rocha, M.; Gollnick, H. Female type of adult acne: Physiological and psychological considerations and management. J. Dtsch. Dermatol. Ges. 2018, 16, 1185–1194. [Google Scholar] [CrossRef] [Green Version]
- Makrantonaki, E.; Ganceviciene, R.; Zouboulis, C.C. An update on the role of the sebaceous gland in the pathogenesis of acne. Dermato-Endocrinology 2011, 3, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, A.; Massa, A.; Picoto, A.; Soares, A.; Basto, A.; Lopes, C.; Bello, R. Avaliação e tratamento do doente com acne—Parte I: Epidemiologia, etiopatogenia, clínica, classificação, impacto psicossocial, mitos e realidades, diagnóstico diferencial e estudos complementares. Rev. Soc. Port. Med. Interna 2011, 27, 59–65. [Google Scholar]
- Figueiredo, A.A.; Massa, A.; Picoto, A.P.; Soares, A.S.; Basto, C.; Lopes, C.; Resende, C.; Rebelo, F.M.; Brandão, G.M.; Pinto, H.S.d.; et al. Avaliação e tratamento do doente com acne–Parte II: Tratamento tópico, sistémico e cirúrgico, tratamento da acne na grávida, algoritmo terapêutico. Rev. Port. Clín. Geral 2011, 27, 66–76. [Google Scholar] [CrossRef]
- Thiboutot, D.; Gollnick, H.; Bettoli, V.; Dréno, B.; Kang, S.; Leyden, J.J.; Shalita, A.R.; Lozada, V.T.; Berson, D.; Finlay, A.Y.; et al. New insights into the management of acne: An update from the Global Alliance to Improve Outcomes in Acne Group. J. Am. Acad. Dermatol. 2009, 60, S1–S50. [Google Scholar] [CrossRef] [PubMed]
- Doshi, A.; Zaheer, A.; Stiller, M.J. A comparison of current acne grading systems and proposal of a novel system. Int. J. Dermatol. 1997, 36, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Know the problems of Skin, Hair and Nails. Available online: www.sbd.org.br (accessed on 14 April 2021).
- Fox, L.; Csongradi, C.; Aucamp, M.; Du Plessis, J.; Gerber, M. Treatment Modalities for Acne. Molecules 2016, 21, 1063. [Google Scholar] [CrossRef] [Green Version]
- Otlewska, A.; Baran, W.; Batycka-Baran, A. Adverse events related to topical drug treatments for acne vulgaris. Expert Opin. Drug Saf. 2020, 19, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Marson, J.W.; Baldwin, H.E. An Overview of Acne Therapy, Part 1. Dermatol. Clin. 2019, 37, 183–193. [Google Scholar] [CrossRef]
- Stangeland, K.Z.; Huldt-Nystrøm, T.; Li, X.; Danielsen, K. Behandling av akne. Tidsskr. Den Nor. legeforening 2019. [Google Scholar] [CrossRef]
- Farrah, G.; Tan, E. The use of oral antibiotics in treating acne vulgaris: A new approach. Dermatol. Ther. 2016, 29, 377–384. [Google Scholar] [CrossRef]
- Bagatin, E.; Costa, C.S. The use of isotretinoin for acne – an update on optimal dosing, surveillance, and adverse effects. Expert Rev. Clin. Pharmacol. 2020, 13, 885–897. [Google Scholar] [CrossRef]
- Hamblin, M. Introduction to experimental and clinical studies using low-level Laser (light) therapy (LLLT). Lasers Surg. Med. 2010, 42, 447–449. [Google Scholar] [CrossRef]
- Karu, T.I. Cellular and Molecular Mechanisms of Photobiomodulation (Low-Power Laser Therapy). IEEE J. Sel. Top. Quantum Electron. 2013, 20, 143–148. [Google Scholar] [CrossRef]
- Melø, T.B. Uptake of Protoporphyrin and Violet Light Photodestruction of Propionibacterium Acnes. Z. Nat. 1987, 42, 123–128. [Google Scholar] [CrossRef] [PubMed]
- McGinley, K.J.; Webster, G.F.; Leyden, J.J. Facial follicular porphyrin fluorescence: Correlation with age and density of Propionibacterium acnes. Br. J. Dermatol. 1980, 102, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, C.; Dessinioti, C.; Sotiriadis, D.; Kalokasidis, K.; Kontochristopoulos, G.; Petridis, A.; Nikolis, A. A multicenter, randomized, split-face clinical trial evaluating the efficacy and safety of chromophore gel-assisted blue light phototherapy for the treatment of acne. Int. J. Dermatol. 2016, 55, 1321–1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Arruda, L.H.F.; Kodani, V.; Filho, A.B.; Mazzaro, C.B. Estudo clínico, prospectivo, aberto, randomizado e comparativo para avaliar a segurança e a eficácia da luz azul versus peróxido de benzoíla 5% no tratamento da acne inflamatória graus II e III. An. Bras. Dermatol. 2009, 84, 463–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gold, M.H.; Sensing, W.; Biron, J.A. Clinical efficacy of home-use blue-light therapy for mild-to moderate acne. J. Cosmet. Laser Ther. 2011, 13, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.; Lee, J.; Yoon, J.; Park, S.; Ryu, H.; Park, B.; Kim, Y.; Suh, D. The clinical and histological effect of home-use, combination blue-red LED phototherapy for mild-to-moderate acne vulgaris in Korean patients: A double-blind, randomized controlled trial. Br. J. Dermatol. 2012, 168, 1088–1094. [Google Scholar] [CrossRef] [PubMed]
- Greaves, A.J. The effects of narrow bands of visible light upon some skin disorders: A review. Int. J. Cosmet. Sci. 2016, 38, 325–345. [Google Scholar] [CrossRef]
- Scott, A.M.; Stehlik, P.; Clark, J.; Zhang, D.; Yang, Z.; Hoffmann, T.; Del Mar, C.; Glasziou, P. Blue-Light Therapy for Acne Vulgaris: A Systematic Review and Meta-Analysis. Ann. Fam. Med. 2019, 17, 545–553. [Google Scholar] [CrossRef] [Green Version]
- Chernyshov, P.V.; Zouboulis, C.C.; Tomas-Aragones, L.; Jemec, G.B.; Manolache, L.; Tzellos, T.; Finlay, A.Y. Acne-Related Quality of Life Among Female Adults of Different Races/Ethnicities. J. Eur. Acad. Dermatol. Venereol. 2015, 7, 154–162. [Google Scholar]
- Cheema, A.N.; Ameen, U.; Javaid, R.; Bokhari, M.A. Efficacy and safety of blue light versus 4% topical benzoyl peroxide in mild to moderate acne. J. Pak. Assoc. Dermatol. 2018, 28, 79–84. [Google Scholar]
- Elman, M.; Slatkine, M.; Harth, Y. The effective treatment of acne vulgaris by a high-intensity, narrow band 405-420 nm light source. J. Cosmet. Laser Ther. 2003, 5, 111–117. [Google Scholar] [CrossRef]
- Kwon, H.H.; Choi, S.C.; Jung, J.Y.; Bae, Y.; Park, G.-H. A Novel Combined Light-Based Treatment of Acne Vulgaris with 1450-nm Diode Laser and 450-nm Blue Light. Dermatol. Surg. 2019, 45, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, P.; Katsambas, A.; Chu, A. Phototherapy with blue (415 nm) and red (660 nm) light in the treatment of acne vulgaris. Br. J. Dermatol. 2000, 142, 973–978. [Google Scholar] [CrossRef]
- Tzung, T.-Y.; Wu, K.-H.; Huang, M.-L. Blue light phototherapy in the treatment of acne. Photodermatol. Photoimmunol. Photomed. 2004, 20, 266–269. [Google Scholar] [CrossRef]
- Uebelhoer, N.S.; Bogle, M.A.; Dover, J.S.; Arndt, K.A.; Rohrer, T.E. Comparison of Stacked Pulses versus Double-Pass Treatments of Facial Acne with a 1450-nm Laser. Dermatol. Surg. 2007, 33, 552–559. [Google Scholar]
- Boyd, J.; Lewis, K.A.; Mohammed, N.; Desai, P.; Purdy, M.; Li, W.-H.; Fourre, T.; Miksa, D.; Crane, S.; Southall, M.; et al. Propionibacterium acnes susceptibility to low-level 449 nm blue light photobiomodulation. Lasers Surg. Med. 2019, 51, 727–734. [Google Scholar] [CrossRef]
- Rademaker, M. Adverse effects of isotretinoin: A retrospective review of 1743 patients started on isotretinoin. Australas. J. Dermatol. 2010, 51, 248–253. [Google Scholar] [CrossRef]
- Mariwalla, K.; Rohrer, T.E. Use of lasers and light-based therapies for treatment of acne vulgaris. Lasers Surg. Med. 2005, 37, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Pei, S.; Inamadar, A.C.; Adya, K.A.; Tsoukas, M.M. Light-based therapies in acne treatment. Indian Dermatol. Online J. 2015, 6, 145–157. [Google Scholar]
- Jagdeo, J.; Austin, E.; Mamalis, A.; Wong, C.; Ho, D.; Siegel, D.M. Light-emitting diodes in dermatology: A systematic review of randomized controlled trials. Lasers Surg. Med. 2018, 50, 613–628. [Google Scholar] [CrossRef] [PubMed]
- Hamblin, M.R. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophys. 2017, 4, 337–361. [Google Scholar] [CrossRef] [PubMed]
- Chapman, M.C.C. The first law of photochemistry. J. Chem. Soc. Trans. 1924, 125, 1521–1526. [Google Scholar] [CrossRef]
- Smith, K.C. The photobiological basis of low level laser radiation therapy. Laser Ther. 1991, 3, 19–24. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Patient | With Inflammatory Acne |
|---|---|
| Intervention | Photobiomodulation with blue light |
| Comparison | Medicines/other therapies |
| Outcomes | Reduction of lesions |
| Author, Year, Country | Randomization Unit | Groups | Follow-Ups (Weeks) | Average Age (in Years) | Acne Severity Degree | N Total | Light/Wavelength (Blue) | Total No. of Sessions | Duration of Exposure (Weeks) |
|---|---|---|---|---|---|---|---|---|---|
| Antoniou et al., 2016 (Greece) | Half-face | 2 groups: 44 Half-face L 45 Half-face D | 12 | 21 (16–30) | Moderate, severe | 98 | 415/446 nm | 12 | (6) Two weekly treatment sessions were performed for 6 weeks. |
| Arruda et al., 2009 (Brazil) | Individual | 2 groups: 24 blue light and 28 BPO | 6 | 17 (NR) | Moderate, severe | 60 | 407 a 420 nm | 8 | (4) eight sessions, applied twice a week. |
| Cheema et al., 2018 (Pakistan) | Individual | 2 groups: 62 blue light and 62 BPO | 12 | 23.02 ± 6.3 | Mild to moderate | 124 | 407 a 420 nm | 12 | twice a week, for 6 weeks |
| Elman et al., 2002 (Israel) | Face/Half-face | 3 groups: (1) 10 (Half-face) e (2) 13 (Full-face) (3) 23 (face Blinding) | 8 | 1.8 | inflammatory acne lesions | 23 | 405 a 420 nm | 8 | Goup 1—Not cited Group 2 twice a week for 4 weeks Group 3—twice a week for 4 weeks |
| Gold et al., 2011 (United States) | Lesion | 2 groups: Light and random simulator | After 2 treatments) | 30 (NR) | Mild, moderate | 30 | 414 nm | 4 | 4 treatments in 2 consecutive days (2 treatments a day with an interval between 2 and 12 h) for as long as 10 days |
| Kwon et al., 2019 (korea) | Individual | 2 groups: DL + BL/BL (nonspec ific) | 12 | 21.6 ± 7.8 | Mild, moderate | 24 | 450 nm | 3 | 3 sessions with an interval of 4 weeks |
| Papageorgiou et al., 2000 (United Kingdom) | Individual | 4: 27 (B) 30 (B + R) 25 (Whith light) 25 (BPO) | 12 | 23, 25, 27 d (NR) | Mild, moderate | 82 | 415 nm +20/−15 nm | 84 | 15 min daily for 12 weeks |
| Tzung et al., 2004 (Taiwan) | Half-face | 2 groups (treated face and control side) | 8 | 21 (15–32) | Moderate, severe | 31 | 420 ± 20 nm | 8 | 8 sessions, twice a week |
| Study | Types Light | Wavalengh | Application | Diameter Laser | Application Time | Radiant Exposure | Irradiance | Outcome Variable | Percentage of Treated Side Improvement | Control Side Improvement Percentage |
|---|---|---|---|---|---|---|---|---|---|---|
| Antoniou, 2016 | LED | 415/446 nm | 5 cm | - | 5 min | 33 a 35 J/cm2 | - | Lesions Count and Acne Severity | 40% | 18% |
| Arruda, 2009 | Light | 407 a 420 nm | - | 55 mm lighted área | - | - | - | Lesions count and % | 21.66% | 31.32% |
| Cheema, 2018 | Light | 407 a 420 nm | - | 55 mm circular area | 15 min | - | - | Lesions Count and Acne Severity | 76% | 60% |
| Elman, 2002 | Light | 405 a 420 nm | contact | - | 15 min | - | 50 a 200 mW/cm2 | Lesion count | G1 65.9% E, 67.6% D G2 80%; G3 60% | - - G3 30% |
| Gold, 2011 | Light | 414 nm | - | - | - | - | - | Lesions size and Erythema | Lesions size 76% Erythema 37% | Lesion size 41% Erythema 10% |
| Kwon, 2019 | Ligth | 450 nm | - | Spot size 6 mm | 3 min | 0.6 a 1.2 J/cm2 | 3.5 a 7 mW/cm2 | Inflammatory lesion count | 35.30% | 62.30% |
| Papageorgiou, 2000 | Lamp | 415 nm + −20/−15 nm | 25 cm | - | 15 min | 320 J/cm2 | 4.23 mW/cm2 | Inflamatory lesions | IL 63% comedones 45% | Red light: 76% IL 58% comedones |
| Tzung, 2004 | Light | 420 ± 20 nm | 15 cm | - | - | 40 J/cm2 per session | - | Number and size of lesions | 52% improvement in acne | 15% |
| Random Sequence Generation | Allocation Concealment | Blinding of Participants and Professionals | Blinding of Outcome Assessors | Incomplete Outcomes (Losses) | Selective Reporting of Outcome | Other Biases | |
|---|---|---|---|---|---|---|---|
| Antoniou, 2016 | LOW | UNCERTAIN | UNCERTAIN | UNCERTAIN | LOW | UNCERTAIN | UNCERTAIN |
| Arruda, 2009 | HIGH | UNCERTAIN | HIGH | HIGH | HIGH | UNCERTAIN | UNCERTAIN |
| Cheema, 2018 | UNCERTAIN | UNCERTAIN | UNCERTAIN | LOW | UNCERTAIN | UNCERTAIN | UNCERTAIN |
| Elman, 2002 | UNCERTAIN | UNCERTAIN | LOW | UNCERTAIN | UNCERTAIN | UNCERTAIN | UNCERTAIN |
| Gold, 2011 | UNCERTAIN | UNCERTAIN | UNCERTAIN | UNCERTAIN | UNCERTAIN | UNCERTAIN | UNCERTAIN |
| Kwon, 2019 | LOW | LOW | UNCERTAIN | LOW | LOW | UNCERTAIN | UNCERTAIN |
| Papagerorgiou, 2000 | LOW | UNCERTAIN | LOW | LOW | LOW | UNCERTAIN | UNCERTAIN |
| Tzung, 2004 | UNCERTAIN | UNCERTAIN | UNCERTAIN | UNCERTAIN | UNCERTAIN | UNCERTAIN | UNCERTAIN |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diogo, M.L.G.; Campos, T.M.; Fonseca, E.S.R.; Pavani, C.; Horliana, A.C.R.T.; Fernandes, K.P.S.; Bussadori, S.K.; Fantin, F.G.M.M.; Leite, D.P.V.; Yamamoto, Â.T.A.; et al. Effect of Blue Light on Acne Vulgaris: A Systematic Review. Sensors 2021, 21, 6943. https://doi.org/10.3390/s21206943
Diogo MLG, Campos TM, Fonseca ESR, Pavani C, Horliana ACRT, Fernandes KPS, Bussadori SK, Fantin FGMM, Leite DPV, Yamamoto ÂTA, et al. Effect of Blue Light on Acne Vulgaris: A Systematic Review. Sensors. 2021; 21(20):6943. https://doi.org/10.3390/s21206943
Chicago/Turabian StyleDiogo, Mara Lúcia Gonçalves, Thalita Molinos Campos, Elsa Susana Reis Fonseca, Christiane Pavani, Anna Carolina Ratto Tempestini Horliana, Kristianne Porta Santos Fernandes, Sandra Kalil Bussadori, Francisca Goreth Malheiro Moraes Fantin, Diego Portes Vieira Leite, Ângela Toshie Araki Yamamoto, and et al. 2021. "Effect of Blue Light on Acne Vulgaris: A Systematic Review" Sensors 21, no. 20: 6943. https://doi.org/10.3390/s21206943